RHEUMATOLOGY
1/115
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
116 Terms
important management considerations when starting on steroids
- Give patients a steroid card
- Advise never to stop steroids suddenly due to the risk of adrenal insufficiency
- If they are unable to take tablets (e.g. due to vomiting) they need to seek urgent medical advice
- Explain the risk of immunosuppression and check vaccination status
- bone protection with bisphosphonates +/- vitamin D and calcium supplementation; this should be continued for the duration of steroid treatment before reassessing fragility - fracture risk (osteoporosis)
- proton pump inhibitor for gastric protection
- Monitor blood pressure and glucose levels
when to avoid NSAIDs
Peptic ulcer disease / GI bleeding
Renal impairment (CKD, AKI)
Cardiovascular disease (IHD, HF, HTN)
what is the Beighton scale
evaluates joint hyper mobility
go through the whole antibody list
1. ANA (unspecific) - many conditions
2. anti-dsDNA - specific for lupus
3. ENA
Ro -
La - for sjogren
Smooth muscle - specific for lupus
RNP
Jo-1 = for myositis
Scl 70 = for limited systemic sclerosis
4. ANCA
5. RF
6. CCP - more specific for RA
ANTI-PHOSPHOLIPID SYNDROME definition
- you have anti-phospholipid antibodies
ANTI-PHOSPHOLIPID SYNDROME investigations
- anticardiolipin antibodies (aCL),
- anti-beta-2-glycoprotein I antibodies (anti-β2GPI),
- lupus anticoagulant (LA).
ANTI-PHOSPHOLIPID SYNDROME management
AYSMPTOMATIC: observe
SYMPTOMATIC 9i.e have had a thrombotic event) = thromboprophylaxis
- WARFARIN
(if warfarin contraindicated, low dose aspiring and low molecular weight heparin)
ANTI-PHOSPHOLIPID SYNDROME features
- venous/arterial thromboses BUT causes a paradoxical rise in APTT (APTT test relies on phospholipid)
- recurrent miscarriages
- livedo reticularis
- other features: pre-eclampsia, pulmonary hypertension
CLOTS
coagulation
livedo reticularis
obstetric complications
thrombocytopenia
ANKYLOSING SPONDYLITIS definition
a type of seronegative arthritis
ANKYLOSING SPONDYLITIS most commonly affected demographic
males aged 20-30
ANKYLOSING SPONDYLITIS common features
- back pain and stiffness (sacroileitis which is buttock pain as well)
- relieved with movement
extraarticular involement (rare)
- Apical fibrosis
- Anterior uveitis
- Aortic regurgitation
- Achilles tendonitis
- AV node block
- Amyloidosis
- Anterior uveitis -( this is common, so warn patients about this)
- Inflammatory bowel disease
- Osteoporosis
- IgA nephropathy
- Systemic symptoms of weight loss and fatigue
O/E
- restricted movement in lumbar spine - "schober's test" can be used to assess
ANKYLOSING SPONDYLITIS investigations
- best diagnostic = MRI
- X ray
- bloods
- no need to do hla-b27
ANKYLOSING SPONDYLITIS features on X-ray
- Bamboo spine with a single central radiodense line related to ossification of supraspinous and interspinous ligaments (shown in picture)
- fused sacroiliac joint
- Squaring of vertebrae
- syndesmophytes (which go above and below the bone)
- shiny corner sign (triangular areas of sclerosis at the anterior vertebral endplates on X-ray.)

ANKYLOSING SPONDYLITIS management
conservative
- physiotherapy
medical
- first line: NSAIDs
- second line: biologic DMARDs e.g infliximab
(do not use methotrexate, as useless for backpain)
ANKYLOSING SPONDYLITIS examination findings
- reduced chest expansion,
- reduced lateral flexion
- reduced forward flexion (Schober's test)
BEHCET'S DISEASE features
Relapsing-remitting oral and genital ulceration
as well as
arthritis
uveitis
mainly affects people from the Middle East, the mediterranean or east asia
DISORDERS OF ELBOW - medial epicondylitis definition
- aka golfers elbow
- pain worse on wrist flexion and pronation of the forearm
remember golfing and also f and p look alike
DISORDERS OF ELBOW - lateral epicondylitis features
- aka tennis elbow
- pain worse on wrist extension and supination of the forearm
DISORDERS OF ELBOW - lateral epicondylitis management options
- advice on avoiding muscle overload
- simple analgesia
- steroid injection
- physiotherapy
FIBROMYALGIA features
- widespread pain
- unrefreshing sleep
- chronic
FIBROMYALGIA management
- CBT
- aerobic exercise - graded exercise therapy
- medication for neuropathic pain
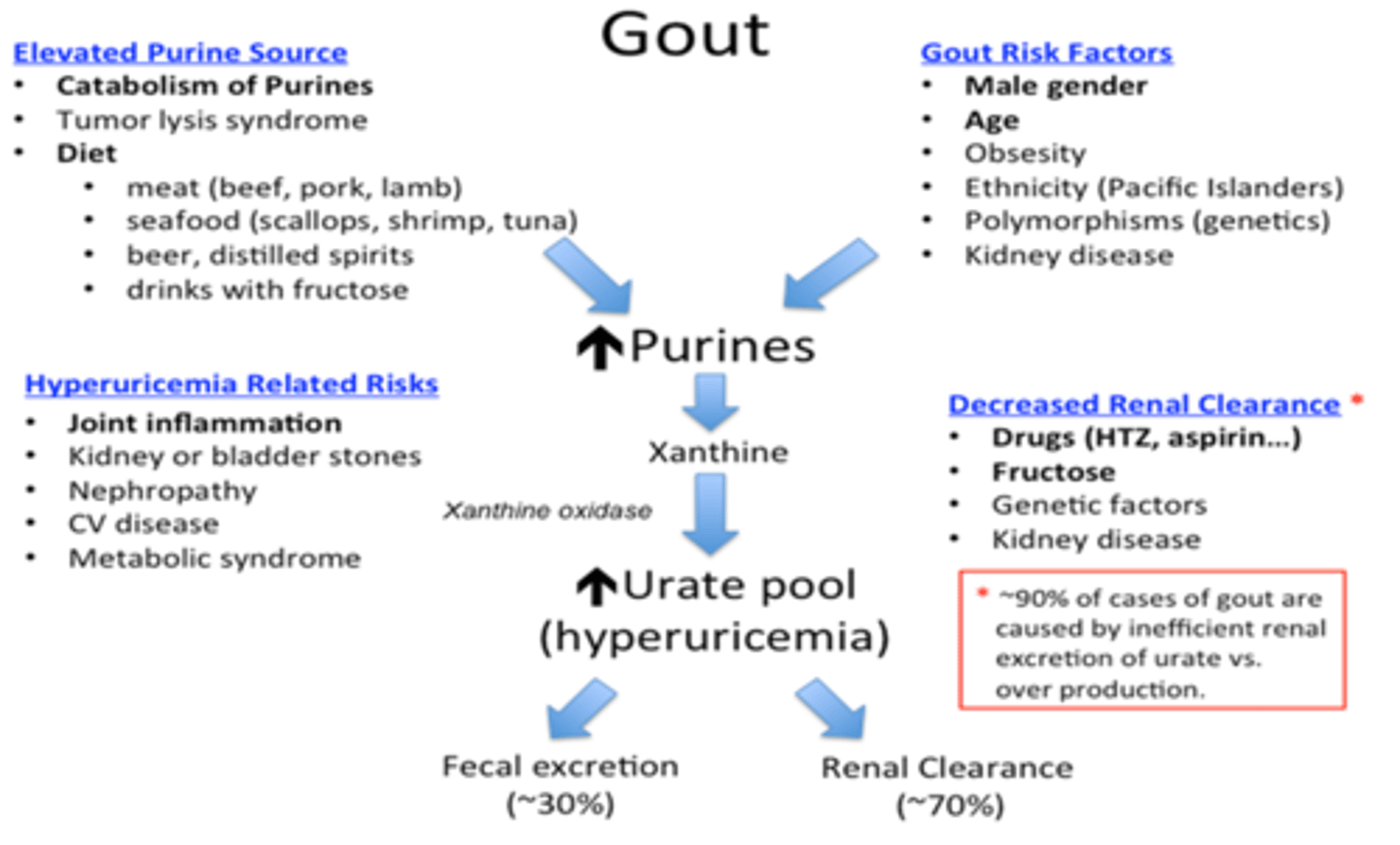
GOUT what is it
- Gout is a type of arthritis caused by the accumulation of monosodium urate crystals in and around the joints
- most commonly first presents in MTP - metatarsophalangeal joints
- chronic untreated gout can lead to the formation of tophi (hard nodules)
commonly in :
ankle, wrist, knee, 1st MTP
(gout =

GOUT risk factors
- CKD (can cause high urate)
- alcohol excess
- red meat
- fizzy drinks
- Medications such as thiazide diuretics and ciclosporin
- also tumour lysis syndrome
GOUT investigations
- mainly a clinical diagnosis
bedside:
- joint needle aspiration (synovial fluid analysis) - shows needle-shaped monosodium urate crystals with negative birefringence
- tophi can be biopsied
blood test:
- serum uric acid (if more than 360 micro mol/L, this is diagnostic)
GOUT management
ACUTE
- NSAIDs, colchicine. If both fail: short course of oral steroids.
TO REDUCE FUTURE RISK
- Urate-lowering therapy with allopurinol - first line (must wait at least 2 weeks after an attack)** or febuxostat (these are xanthine oxidase inhibitors - so reduce uric acid production
** When starting allopurinol, cover with nsaids or colchicine as allopurinol can actually cause an acute flare
** side effect of allopurinol can be a rash in which case the medication should be stopped.
HYPERMOBILITY SYNDROME
MARFAN'S SYNDROME aetiology
is a genetic disorder (autosomal dominant) caused by mutations in the FBN1 gene, which encodes fibrillin-1
MARFAN'S SYNDROME features
- usually tall and slim
- long arms and digits
- a high-arched palate
- hypermobility
- cardiovascular abnormalities
ophthalmic:
- enopthalmos
- myopia
- superior lens disclocation
OSTEOARTHRITIS definition
- most common form of arthritis
- causes degeneration of joints due to "wear and tear"
OSTEOARTHRITIS risk factors
Overuse of joints
Excessive body weight
Age
OSTEOARTHRITIS symptoms
P – Pain
C – Crepitus
T – Tenderness
R – Relieved by rest (worse with activity)
G – Grating
S – Swelling
please can the radiologist go somewhere!
Bouchard’s nodes = swelling at the PIP joints
and
Heberden’s nodes = swelling at the DIP joints
(B is proximal and H is distal)
OSTEOARTHRITIS diagnosis
- clinical diagnosis
- if uncertainty, do an X-ray, which shows:
Loss of joint space
Osteophytes
Subchondral sclerosis - white opacification
Subchondral cysts - black things within the white
can also be used to rule out other causes of symptoms
OSTEOARTHRITIS management
conservative
- lifestyle factors: diet and exercise (exercise does help!), stopping smoking
- physiotherapy, occupational therapy
medical
- first line: topical NSAIDs e.g ibuprofen gel
- work up WHO pain ladder
surgical
- arthroplasty if medical options have been exhausted and disease is severe
OSTEOARTHRITIS complications
can form a bakers cyst
OSTEOMALACIA what is it
Metabolic condition where bones become soft secondary to a calcium, vitamin D or phosphate deficiency
OSTEOMALACIA what would the lab values be
Low serum calcium, low serum phosphate, raised ALP and raised PTH
PAGET'S DISEASE OF THE BONE classical presentation
old man, bone pain, raised ALP
PAGET'S DISEASE OF THE BONE investigations
1. raised alkaline phosphatase (ALP)
2. calcium and phosphate are typically normal
3. other markers of bone turnover
4. x-rays
5. bone scintigraphy - increased uptake is seen focally at the sites of active bone lesions
PAGET'S DISEASE OF THE BONE management
bisphosphonate (either oral risedronate or IV zoledronate)
PAGET'S DISEASE OF THE BONE complications
hearing loss - due to cranial nerve entrapment
fragility fractures
heart failure - because bones need more blood?
sarcoma
POLYMYALGIA RHEUMATICA definition
stiffness and pain of the proximal large joints.
- autoimmune
- acute onset
- common in the elderly
POLYMYALGIA RHEUMATICA investigations
ESR and CRP
- no particular antibody
- creatine kinase is normal
POLYMYALGIA RHEUMATICA features
- bilateral stiffness of shoulder, neck, pelvic joints
- movement worsens pain (better with rest)
- systemic systems e.g fatigue
- O/E power is usually preserved
- should screen for GCA
POLYMYALGIA RHEUMATICA treatment
steroids
15mg oral prednisolone daily
( if not responding well to Pred, consider an alternative diagnosis)
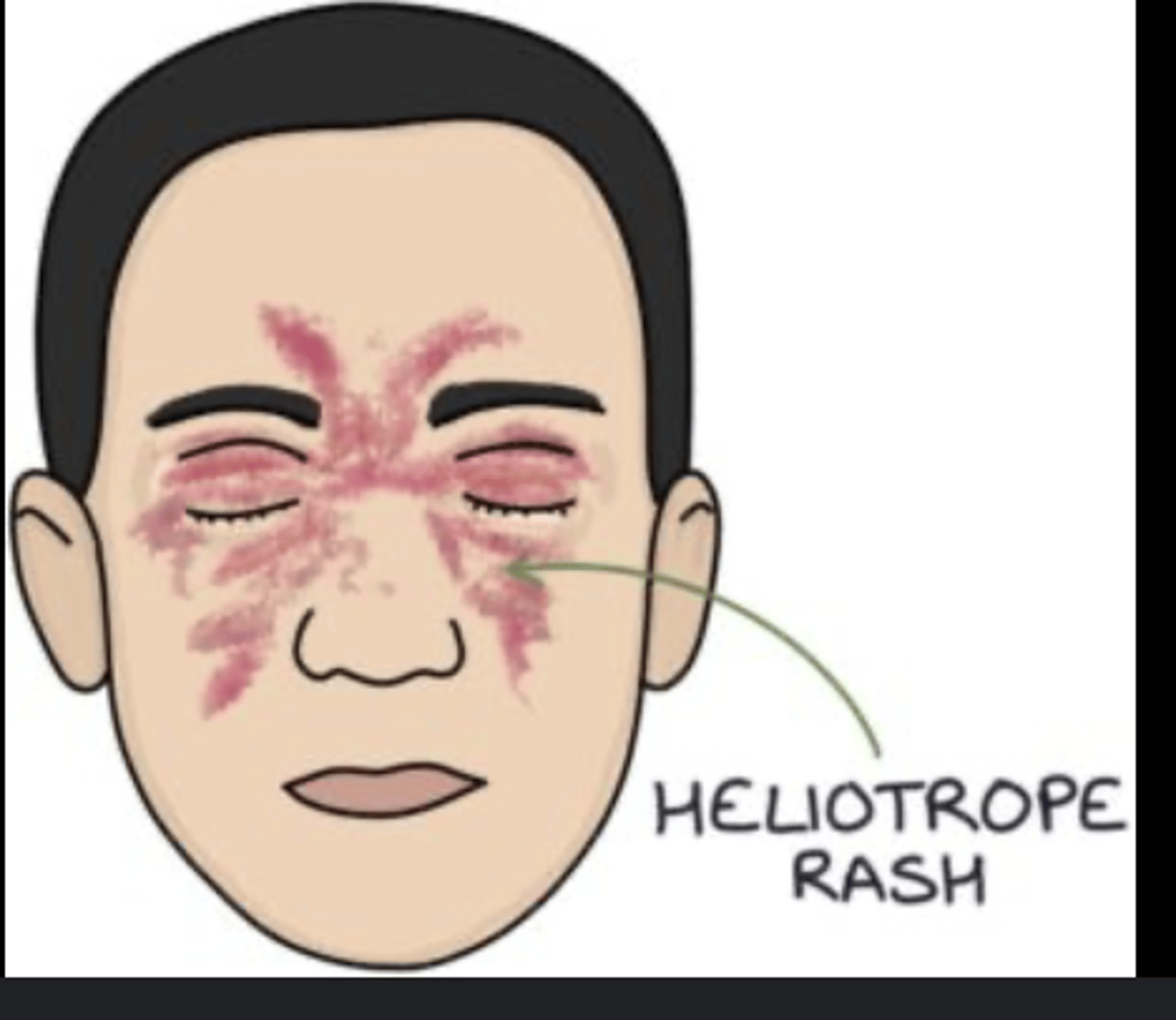
POLYMYOSITIS what is it
inflammatory disorder causing symmetrical, proximal muscle weakness
dermatomyositis is a variant of the disease where skin manifestations are prominent - eg a light purple (heliotrope) rash on the cheeks and eyelids.
Gotrans sign as well - which is rash on knuckles
- associated with malignancy, so should do a CT CAP
- can result in type 2 resp failure!
- anti -Jo antibodies
POLYMYOSITIS commonly affected demographic
typically affects middle-aged, female:male 3:1
POLYMYOSITIS classical presentation
malignancy + raised CK
"Dermatomyositis and polymyositis turn your muscles into CLAAA (clay)':
enzymes elevated are :
Creatine kinase,
Lactate dehydrogenase,
Aldolase,
ALT
AST"
PSEUDOGOUT definition
a form of microcrystal synovitis caused by the deposition of calcium pyrophosphate dihydrate crystals in the synovium
awkward news
- knee wrist shoulder
PSEUDOGOUT risk factors
haemochromatosis (iron drives pyrophosphate overproduction)
hyperparathyroidism
low magnesium, low phosphate
acromegaly,
Wilson's disease
PSEUDOGOUT investigations
1. joint aspiration: weakly-positively birefringent rhomboid-shaped crystals
2. x-ray: chondrocalcinosis* in the knee this can be seen as linear calcifications of the meniscus and articular cartilage
* this is excessive accumulation of calcium crystals in the cartilage of joint
PSEUDOGOUT management
RICE
Intraarticular steroids, NSAIDs
PSORIATIC ARTHRITIS definition
inflammatory arthritis associated with psoriasis and is classed as one of the seronegative arthritis
target is the enthuses (where ligaments and tendons attach to the bone)
PSORIATIC ARTHRITIS subtypes
1. Asymmetric oligoarticular arthritis
- 4 or fewer joints are involved;
- most common form at presentation although this may become polyarticular with time
2. Polyarticular arthritis
- is usually symmetrical and presents similarly to rheumatoid arthritis, although distal interphalangeal joints are more likely to be involved than metacarpophalangeal joints
3. Distal interphalangeal disease
- affects the distal interphalangeal joints only; nail changes are especially common
4. Arthritis mutilans
- is a severely destructive arthritis with resulting deformities including telescoping of digits
5. Spondyloarthritis involves sacroiliitis and involvement of the spine, often with concurrent peripheral joint involvement

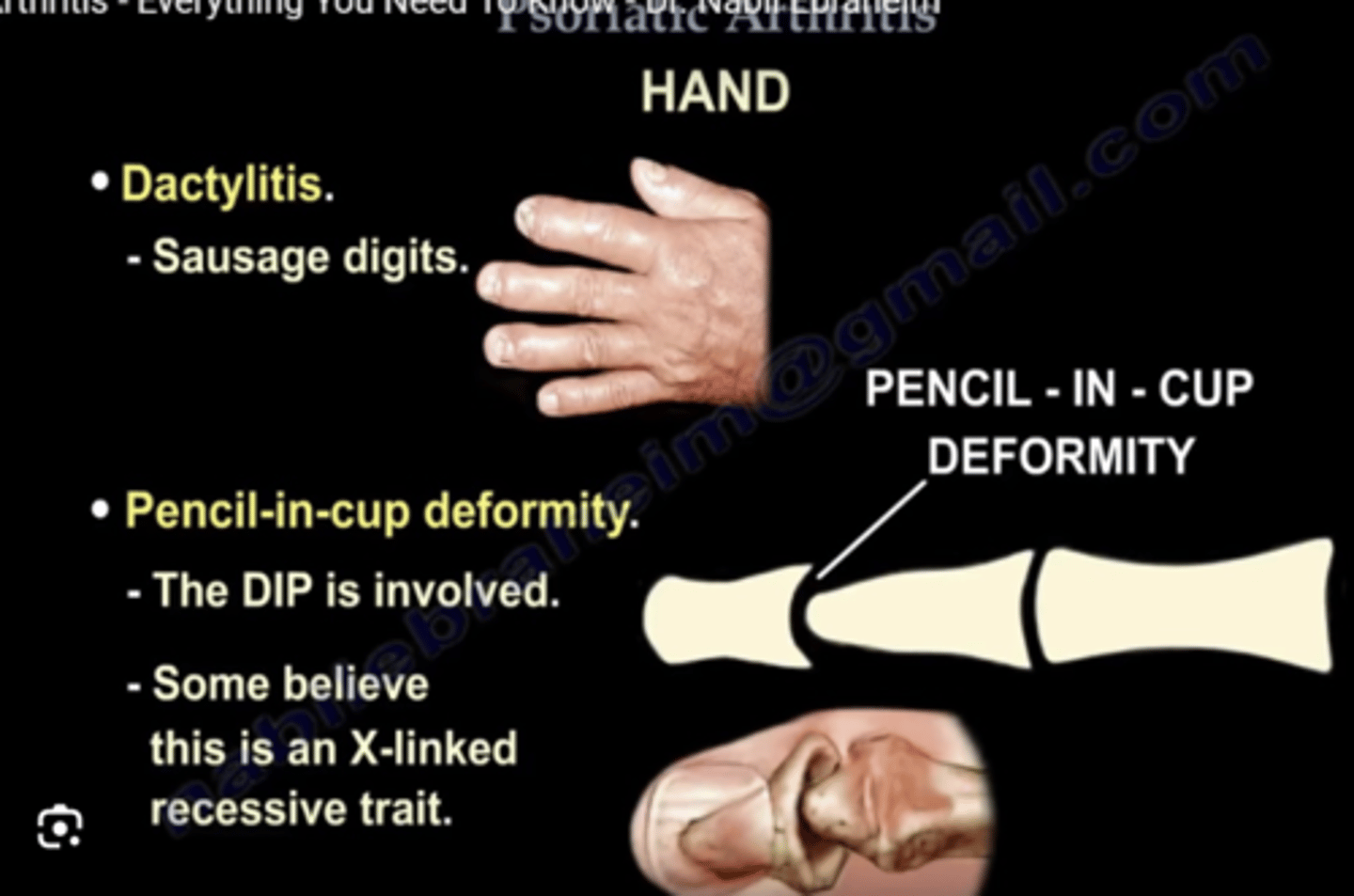
PSORIATIC ARTHRITIS features
X-ray
- unusual combination of erosive changes (resorption) and new bone formation
- "pencil in cup" deformity
- arthritis mutilans (looks really deformed)
- dactylitis = self limiting episode of a swollen digit
- rash on extensor surfaces
'Rheumatoid'-like joint problems but nail changes → ?psoriatic arthritis
PSORIATIC ARTHRITIS management
lifestyle + NSAIDs → DMARDs (MTX) → biologics
RAYNAUD'S PHENOMENON management
conservative
- wear gloves
medical
CCB e.g nifedipine
REACTIVE ARTHRITIS definition
- typically affects the lower extremity joints (most commonly the knee)
- occurs classically with conjunctivitis and urethritis following an enteric or sexually transmitted infection
- "cant see, cant pee, cant climb a tree"
(uveitis, urethritis, arthritis)
REACTIVE ARTHRITIS what organism is associated
chlamydia (so you get post STI arthritis)
RHEUMATOID ARTHRITIS features
- affects MCP and PIP joints. distal joints are spared
- affects small joints (e.g feet and hands)
- relieved with movement (you get morning stiffness- abnormal is more than 30 mins)
- sudden onset
- symmetrical
- many joints affected (polyarthritis)
- additive (more joints keep getting affected)
- constitutional: fatigue, malaise
a systemic condition
- episcleritis/scleritis
- lung: ILD (interstitial lung disease), bronchiectasis
- rheumatoid nodules
- heart: pericarditis, cardiac effusion (at an increased risk of ischaemic heart disease)
- small vessel vasculitis
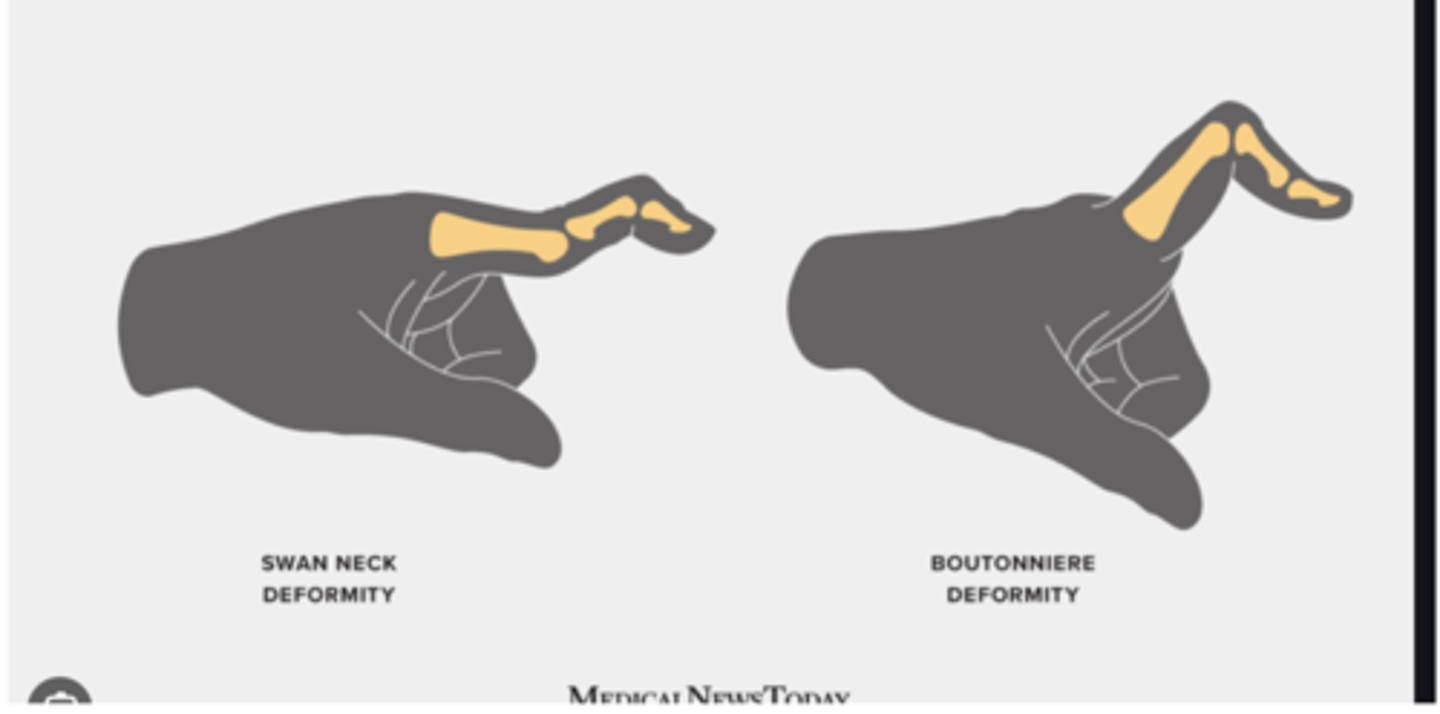
in the hand:
- ulnar deviation
- Z thumb
- swan neck deformity
- boutonniere's deformity
RHEUMATOID ARTHRITIS investigations
1. FBC, CRP, ESR, U/E, LFT, C3/C4 (to rule out differentials)
2. antibody screen:
- Rheumatoid Factor (an antibody against Fc potion of human IgG) - do this test initially. If you still suspect RA, do:
- anti-CCP (more specific)
(if both positive = seropositive - it is a sign of worse prognosis
70-80% are seropositive)
Also do:
- ANA
3. Imaging:
- X-ray of hands and feet: shows erosive changes
- US scans
- MRI
RHEUMATOID ARTHRITIS features on an x ray
LESSS:
loss of joint space,
periarticular erosions,
subluxation,
soft tissue swelling,
subarticular (periarticular) osteopenia (darkening of bones) - check pic

RHEUMATOID ARTHRITIS score to measure severity
DAS28 test
RHEUMATOID ARTHRITIS treatment
goal of treatment: reduce inflammation and pain, promote joint function, and prevent joint destruction and deformity
acute:
includes NSAIDs to reduce inflammation and pain.
If severe, corticosteroids - oral pred or IM methyl pred
-long term:
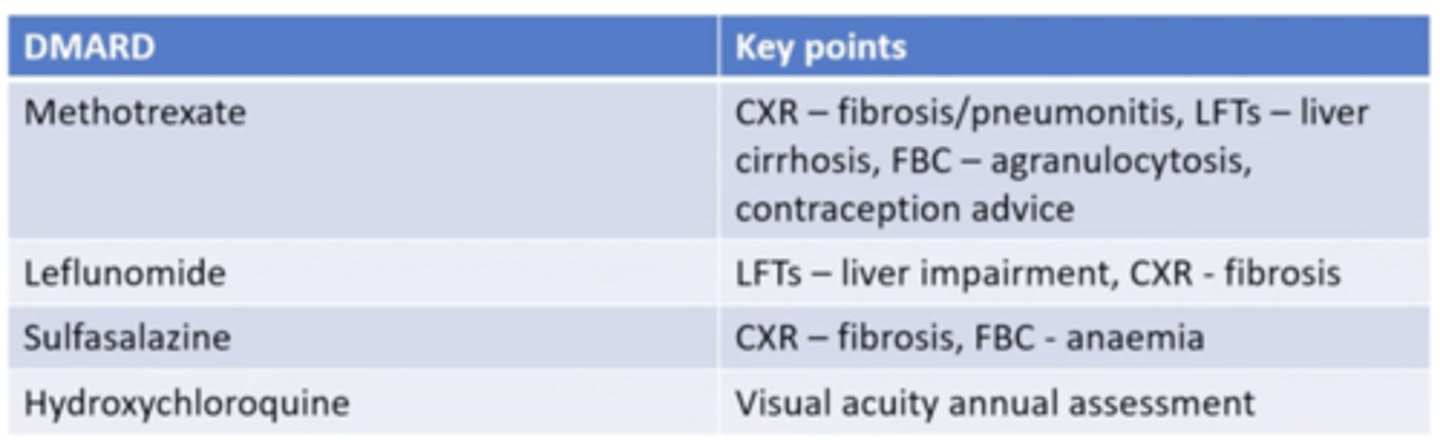
first line cDMARDS e.g methotrexate. Taken once a week. side effects: hair thinning, nausea. Can cause bone marrow suppression
Other 6 days: folic acid supplementation.
second line: increase dose
third line: add another cDMARD e.g sulfasalazine** or hydroxychloroquine, lefunomide (also teratogenic)
fourth line - need to have failed previous 2 treatments to be prescribed (because of cost)
biologics e.g
- infliximab - antiTNF-alpha
- rituximab (only if seropositive RA) = anti-cd20, stop production of B cells (therefore antibodies). Side effect = immunosuppression. 2 infusions 2 weeks apart. Can increase risk of severe covid.
- JAK inhibitor (tablet)
physiotherapy and hand therapy
sulfasalazine
- give this to women of childbearing age
- careful if also allergic to aspirin
- can cause oligospermia (resolves on stopping the drug)
- Stevens-Johnsons syndrome
- may colour tears , so you get stained contact lenses
what do you need to screen for before starting biologic therapy
biologic therapy can reactivate TB especially, anti-TNFa
RHEUMATOID ARTHRITIS complications
Osteoporosis
Rheumatoid nodules
Dry eyes and mouth
Infections
Carpel tunnel syndrome
Hardened and blocked arteries - CVD
Inflammation and scarring of the lung tissue
Non- hodgkin Lymphoma
Secondary amyloid
Felty's syndrome (triad: neutropenia, RA, splenomegaly)
methotrexate:
- advice for pregnancy
- significant side effects
- Methotrexate should be avoided during pregnancy due to the risk of teratogenicity. A washout period of 6 months is recommended preconception
- hepatotoxicity, bone marrow suppression and pneumonitis
SEPTIC ARTHRITIS definition
infection of the joint
SEPTIC ARTHRITIS aetiology
most commonly: staph aureus
young adults who are sexually active, Neisseria gonorrhoeae is the most common organism
IV drug users: pseudomonas aeruginosa
SEPTIC ARTHRITIS features
- Acute onset of tender, swollen joint
- Reduced range of joint movement
- Systemic symptoms such as fever, malaise, or chills
SEPTIC ARTHRITIS investigations
1. joint aspiration for MC&S - shows neutrophils >90% and very high WCC
2. bloods
3. blood culture
SEPTIC ARTHRITIS management
- IV antibiotics guided by local guidelines
- joint washout under general anaesthesia to remove infected material
- Physiotherapy following the resolution of acute infection to restore joint function
- sepsis 6
SEPTIC ARTHRITIS complications
1. Osteomyelitis: infection of the bone
2. Chronic arthritis: persistent joint inflammation
3. Ankylosis: joint fusion resulting in immobility
SJOGREN'S SYNDROME definition
an autoimmune condition where exocrine glands producing tears and saliva are destroyed
SJOGREN'S SYNDROME investigations
1. RF - rheumatoid factor positive in nearly 50% of patients
2. ANA positive in 70%
3. anti-Ro (SSA) antibodies in 70% of patients with PSS
4. anti-La (SSB) antibodies in 30% of patients with PSS
5. Schirmer's test: filter paper near conjunctival sac to measure tear formation
6. histology: focal lymphocytic infiltration
7. Anti-dsDNA suggests Sjogren's syndrome is secondary to SLE if strongly positive
8. Anti-CCP may suggest associated rheumatoid arthritis
SJOGREN'S SYNDROME symptoms
- dry eyes, perhaps more susceptible to eye infections
- dry mouth, - poor swallowing, poor dental health - increases risk of decay (caries)
- dry skin
- vaginal dryness
- raynauds phenomenon
- systemic symptoms - fatigue, arthralgia, arthritis
SJOGREN'S SYNDROME complications
- complication of pregnancy: risk of congenital heart block and neonatal lupus
- increased risk of B cell lymphoma, most commonly MALT lymphoma
SJOGREN'S SYNDROME treatment
conservative
- humidifying home and work environments
- reducing screen time
medical
- oral pilocarpine to treat eye and mouth dryness
- lubricating eye drops
SYSTEMIC LUPUS ERYTHEMATOSUS definition
-Autoimmune disease characterised by the proliferation of antinuclear antibodies. These form immune complexes which can deposit anywhere in the body.
- more common in young women
- relapsing remitting course
- more common in afrocaribbeans/asians
SYSTEMIC LUPUS ERYTHEMATOSUS investigations
- ANA = most sensitive
- anti dsDNA = most specific (antidsDNA is a subtype of ANA)
- anti-smith = also specific
- Us and Es (to check kidney function)
- clotting screen - (if anti-phospholipid syndrome - paradoxical increase in APTT)
- low levels of C3 and C4 (because of consumption) - this is used to monitor flares!
- CRP may be normal or raised
- ESR raised
SYSTEMIC LUPUS ERYTHEMATOSUS commonly affected demographic
- afro-caribbeans
- women
SYSTEMIC LUPUS ERYTHEMATOSUS risk factors for getting the disease
Smoking
Ultraviolet light
Silica exposure
Epstein-Barr virus
SYSTEMIC LUPUS ERYTHEMATOSUS triggers for flare ups
Oestrogen exposure (e.g. pregnancy, the combined oral contraceptive pill). (this is also why lupus decreases after menopause)
Infections
Emotional stress
Physical stress e.g. surgery, injury
Excessive ultraviolet light exposure
SYSTEMIC LUPUS ERYTHEMATOSUS what score do we use to classify it
EULAR/ACR score
*patients need to have positive ANA antibodies and a score of 10 or more on the EULAR/ACR score
SYSTEMIC LUPUS ERYTHEMATOSUS features
- Fatigue
- Weight loss
- respiratory: pleurites, pleural effusions
- Dermatological: scalyMalar rash (butterfly shaped). Spares nasolabial folds
- cardiovascular - Libman sacks endocarditis
- Musculoskeletal: Arthralgia
- Haematological: anaemia,
- Renal symptoms: lupus nephritus - needs constant monitoring. (classified into 6 stages based on histology). You get a 'Full house' immunofluorescence pattern.
- Neuro: seizures, anxiety and depression, increased risk of stroke
- Complications with pregnancy
- Gastro-intestinal: peritonitis
- Haem: cytopenias
- mouth ulcers
remember: pericarditis, peritonitis, pleuritis
SYSTEMIC LUPUS ERYTHEMATOSUS complications
the complications of long-term steroid use!
SYSTEMIC LUPUS ERYTHEMATOSIS management
conservative
- sun protection
- cap
- not using hormonal contraception
medical
- first line: hydroxychloroquine (side effect is damage to retina, so also need regular eye checks)
- if additional joint issues/constitutional sx: add on steroids, NSAIDs,
- immunosuppressants,
drug induced lupus features
- resolves on stopping the drug
antibodies
- ANA positive
- ant histone antibodies present in 90%
drug induced lupus
sulfonamide
hyddralazine
isoniazid
phenytoin
procainamide
discoid lupus what is it
- basically lupus that mainly affects the skin
SYSTEMIC SCLEROSIS definiton
a condition characterised by hardened, sclerotic skin and other connective tissues
SYSTEMIC SCLEROSIS types of patterns
1. limited (central) systemic sclerosis
- anti-centromere antibodies
- CREST syndrome: calcinosis, Raynaud's phenomenon, oesophageal dysmotility, scleroderma (thickening of skin) - causing shiny skin and telangiectasia (red patches)
2. diffuse systemic sclerosis
- associated with anti scl-70 antibodies
- more lung involvement (affects connective tissue in lung)
SYSTEMIC SCLEROSIS complications
scleroderma renal crisis
this is more common in diffuse systemic sclerosis
it causes:
-AKI
- severe hypertension
also
pulmonary hypertension
more common in limited systemic sclerosis
drug induced lupus causes
Most common causes
procainamide
hydralazine
Less common causes
isoniazid
minocycline
phenytoin
VASCULITIS types
- small vessel (granulomatosis with polyangitis - GPA, microscopic polyangitis, churg-strauss syndrome, henoch-schonlein purpura)
- medium vessel (e.g kawasaki, polyarteritis nodosa, buerger's disease)
- large vessel (e.g giant cell arteritis, takayasu arteritis)
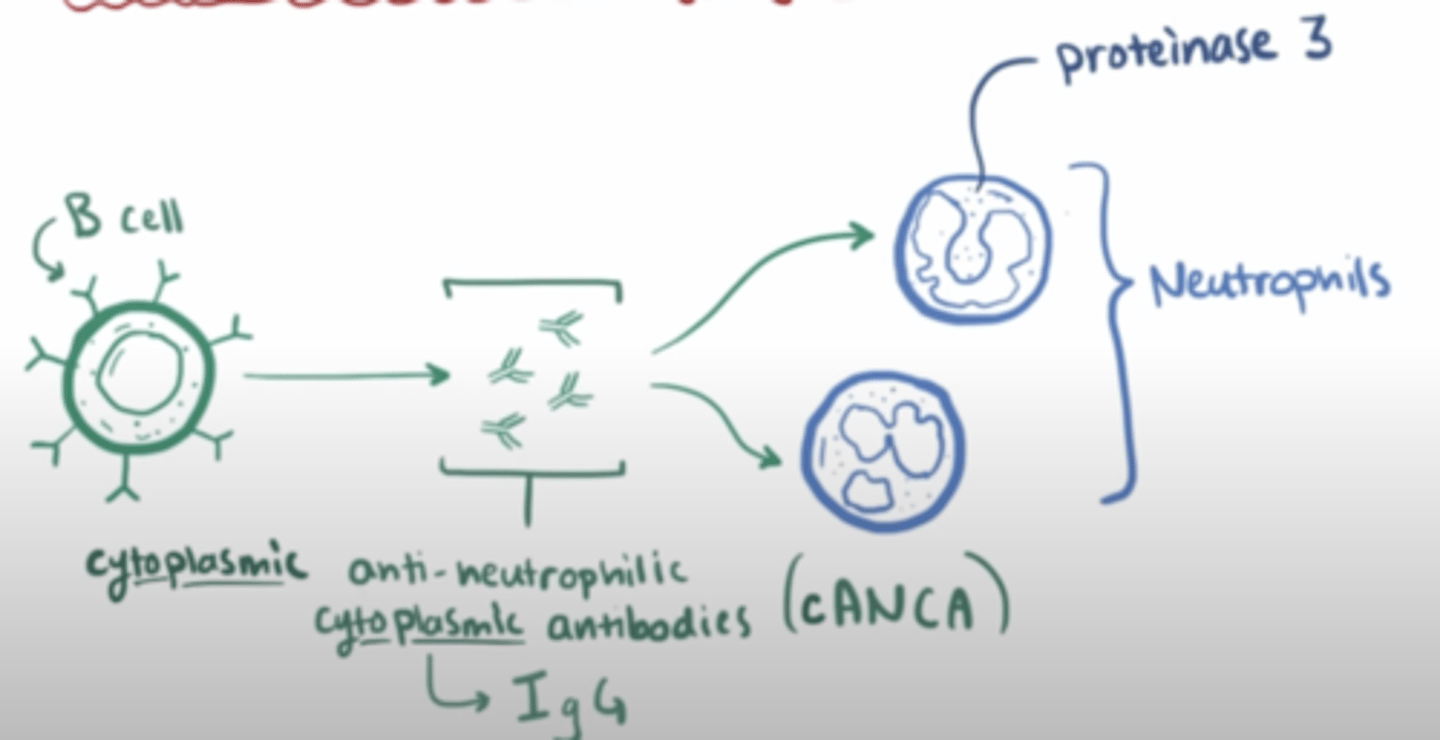
VASCULITIS - small vessel: granulomatosis with polyangitis (GPA) what is it
- a disease where a persons b cells targets granules which are released by their neutrophils (granulomatosis) with an autoantibody called c-ANCA
- this causes free radicals to be released which damages endothelial cells and affects blood flow
this then blood supply to
1. nasopharynx - can cause saddle nose deformity
2. lungs - can cause difficulty breathing, and ulcers -> causing bloody cough
3. kidneys - decreased urine output, increased blood pressure (because kidneys cant maintain function to decrease BP). Can cause rapidly progressive glomerulonephritis,
(classic triad of upper respiratory tract, lower respiratory tract and kidneys)
VASCULITIS - small vessel: granulomatosis with polyangitis (GPA) demographic
middle aged males
VASCULITIS - small vessel: granulomatosis with polyangitis (GPA) treatment
1. corticosteroids
2. cyclophosphamide
VASCULITIS - small vessel: microscopic polyangitis (MP) what is it
very similar disease to GPA except
- doesn't affect nose (only kidney and lungs)
- the antibodies are called p-ANCA not c-ANCA
VASCULITIS - small vessel: churg-strauss syndrome aka eosinophilic granulomatosis with polyangiitis or EGPA what is it
- a types of small vasculitis which
affects nose, kidney, lung + GI (stomach churns)
- antibodies are p-ANCA
- raised eosinophil count (churg Strauss is associated with asthma)
VASCULITIS - small vessel: churg-strauss syndrome aka eosinophilic granulomatosis with polyangiitis or EGPA management
High dose corticosteroids which are weaned after some years (to prevent long term damage)