FINAL EXAM
1/426
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
427 Terms
maximising
choosing alternative with highest expected value
brain wants to maximise ventral striatum and medial frontal cortex activation
VS: codes for expected value of upcoming reward, if it fires more you feel pleasure
fMRI: neurons fire in caudate, nAcc, putamen (ventral striatum) in expecting reward
expected value
reflected in ventral striatum
bulimic higher activity in VS for food
addicts higher nAcc activity for drugs
neural predictors of purchases
preference and price weighed —> price differential
preference pathway: more preferred products → more striatum activity → higher EV → more often purchased
high striatum activity predicts purchase
costs in the brain
ACC
insula: processes negative bodily feedback, creates disgust
pain of price: purchased somtihing —> lower insula activity
cost and value integration, making a choice
vmPFC integrates gains and losses
gains: striatum (nAcc)
losses: ACC, insula
choice:
mPFC activity when item is most preffered
striatum activity when most preferred
mPFC and nAcc track subjective value
brain scan predicting relapse
addict brains:
mPFC: drugs more activity than food or neutral
nAcc: drugs same as food (normal: the same)
nAcc responses to cues response relapse
most response —> soonest relapse
predicting behaviour change
self-reports not significant
mPFC activity is significant
predicts persuasiveness of advertisements
represents recipient resonation
neuroforecasting
neural effect measurements of a small group likely has similar effects on population level
individual preferences scale to the population level
mPFC activity is better than effectivity ranking
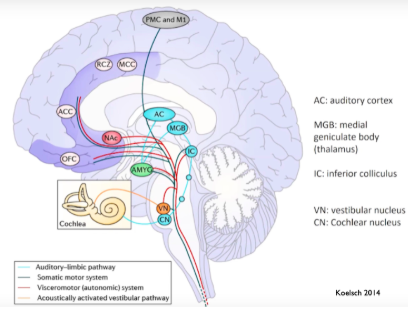
auditory analysis of sound
pattern recognition
comparison to templates: auditory cortex
entrainment (MNS)
prediction of ensuing music
prediction of reward/how nice the next music is
assessment of those predictions with reality → contribute to emotional experience (amygdla)
music and language similarities
sound patterns that unfold over time
have melody and rhythm
250-500 ms time to decide if music is familiar/emotional
decoded by brain to get meaning
music: can happen with multiple people participating at once, language only makes sense one at a time
mechanisms sound —> meaning
hardwired responses, extramusical associations, anticipation
BRECVEMA
brain stem reflex
rhythmic entrainment
evaluative conditioning
contagion (emotion)
visual imagery
episodic memory
musical expectance
aesthetic judgement
lower=more complex and individual
brain stem reflex music types
sad music → decreased heart rate and skin conductance, higher blood pressure
scary music: increased pulse, decreased pulse amplitude
happy music → decrease depth of respiration
hippocampal activity: associated w/ music-evoked emotion
auditory processing stream organisation
dorsal: spatial processing, tracks time-varying events
ventral: time-independent sound properties
melody and lyrics are processed separately
hierarchical (simple/complex
hemispheric (left:spectral, right:sequencing)
dorsal/ventral (where/what)
auditory processing streams
pitch processing
STC (superior temporal cortex), A1, A2: processes pitch, loudness, tonal relationships + templates
different aspects of a tune are processed in different streams
melodies engage neurons in anterior and posterior pathways
rhythmic entrainment
motor regions: interact to percept and product rhythm
premotor regions: track rhythms spontaneously
cortico-cerebellar circuits: subserve differential aspects of rhythmic synchronisation
cerebellar deficit → fast rhythm tracking impaired
rhythm and pitch are separate, but interact
auditory-motor co-activity when sound/movement is congruent
musical expectancy
anticipation depends on the organisation of sounds into a meaningful succession of events (predictive coding)
constant prediction means that music listening is active listening
predictions depend on
learning, familiarity with genre, short-term memory
music has many layers to predict → prediction will be right in one part (minimal prediction error)
PCM
predictive coding model: music perception is a bayesion process
goal : minimise prediction error
aspects of music experienceweighed to predict, weights are constantly updated
uncertainty and pleasure scanning (music)
predictable music: unpredictable parts are pleasurable and vice versa
amygdala, hippocampus, auditory cortex: reflects pleasure and surprise/uncertainty
nAcc: predicts the outcomes and reflects amount of uncertainty only
caudate: firing in anticipation (decides number of chills)
nAcc: firing in anticipation payoof (amount of chilsl)
social brain and music
superficial amygdala: processes stimuli with socio-affective significance (like music)
music-evoked pleasure: activity of the dopaminergic mesolimbic reward pathway
hippocampal formation : emotion related to social attachments
drug
chemical substance of known structure which produced a biological effect when administered
synthetic chemical, chemical obtained from plants, biotechnology products
toxicology
study of toxic effects of chemical substances
pharmacology
study of the effects of drugs
pharmacokinetics
what de body does to a drug
pharmacodynamics
what a drug does to the body
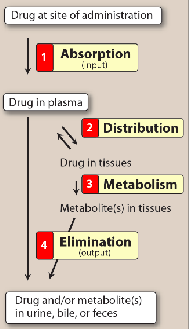
drug disposition
ADME: absorbtion, distribution, metabolism, elimination
speed of onset
intensity of effect
duration of action
pharmacokinetic parameters
aspects of the drug that help decide
route of administration
amount and frequency of dose
duration of treatment
ro
routes of administration
enteral, parenteral
enteral administration
by mouth (safest and most convenient
swallowed —> oral delivery
enteric-coated preparations: chemical envelope resisting stomach enzymes, opening in upper intestine
extended-rekease preparations: special coatings control how fast the drug is released from teh pill
sublingual: under the tongue —> direct bloodstream absorbtion
parenteral administation
any route that doesnt absorb in GI tract (IV, intramuscular, subcutaneous and transdermal routes)
most control over the dose
irreversable, pain, local tissue damage
oral and nasal inhalation —> across mucous membranes
intrathecal/ventricular —> into CSF
topical application: local effect of drug
transdermal: to skin
rectal (no liver effect to the drug)
drug absorbtion
passage of a drug from administration site into plasma
moving across cell barriers/membranes
passive diffusion, facilitated diffusion, active transport, endocytosis (into vesicles)
membrane permeation / factors affecting absorbtion
pH
drug can only pass through membranes if uncharged
acidic drugs: release proton and form charged anion (AH ←→ A- + H+)
weak bases: lose proton —> uncharged (BH+ ←-> B + H+)
distribution b/w ionised and non-ionised forms depends on pH and pK of the drug (decides absorbtion rates
bloodflow to absorbtion site
total absorbtion area
contact time at surface
expression of P-glycoprotein (transmembrane transporter
bioavailability
fraction of drug that reaches systemic circulation
need to calculate dosage
route and chemical physical properties affect this
factors affecting bioavailability
fist-pass hepatic metabolism: how much goes to the site of effect before being exposed to the liver and being metabolised
solubility of drug
chemical instability
nature of drug formulation
bioequivalence
when 2 related preparations show comparable bioavailability and similar time to peak blood concentrations
drug distribution
process where a drug reversibly leaves bloodstream and enters interstitium (extracellular fluid) and tissue
volume of distribution
how widely the drug is distributed in the body
Vd = amt of drug in body / C0 (plasma concentration at t0)
blood-brain barrier
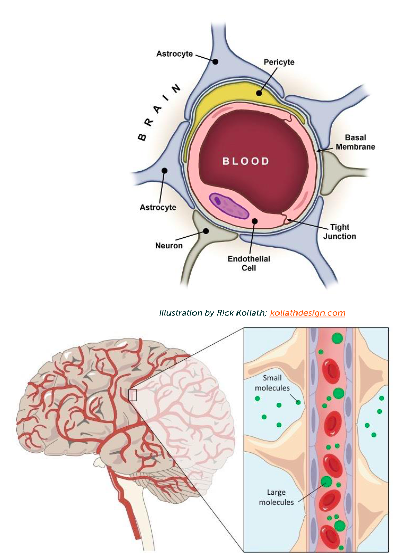
levodopa crosses BBB through aminoacid transport mechanism —> conversion to active dopamine in basal ganglia
drug half-life
time for the concentration of a drug to reduce by 50%
large Vd (volume of distribution) —> influences halflife (depende on amt of drug delivered to liver or kidneys at a time
drug elimination
hepatic metabolism
elimination in bile
elimination in urine
cause exponential decrease of plasma concentration
clearance: amount of drug cleared from body per unit of time
CL = 0.693*Vd (volume of distribution) / t1/2 (half-life)
pulmonary and hepatic clearance most important
types of drug actions on the body
receptors: agonist (stimulates receptor) / antagonist (blocks receptor)
ion channels: blockers or modulators of opening probability
enzymes: inhibitor, false substrate for breaking down, prodrug (the real drug is produced with the enzyme
transporters: inhibitor, false substrate
types of receptors
ligand-gated ion receptors (milliseconds)
G-protein coupled receptors (seconds
kinase-linked receptors (hours)
nuclear receptors (in nucleus, hours)
affinity: how mucha. drug is attracted to the receptor
signal transductionel
when a drug-receptor complex alters biochemical/molecular activity of a cell
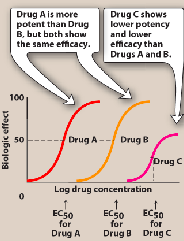
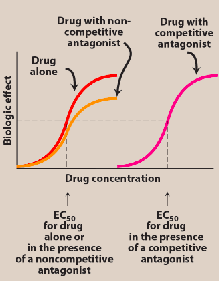
dose-response relationships (potency and efficacy)
increase in drug concentration —> its effect also increases
potency: amount of drug necessary to produce an effect of a given magnitude (potenct: EC50 == 50% of maximum
efficacy: ability of drug to elicit a response when binding to a receptor
greater efficacy > more potent
agonists
full: drug binds to receptor and produces maximal response, mimicking the normal response
partial: less than full response
inverse:binds to receptor as agonist but induces opposite response
antagonist
decrease/oppose the actions of another drug/endogenous ligand (has no effect if the agonist is not present
competitive: if antagonist and agonist bind to same site
irreversible: maximum downwards shift
therapeutic index
ratio of the dose that produces toxicity to the dose/dose that produces a desired effect
TD50: dose that produces toxic effect in half of population
ED50: dose that produces desired response in 50% of population
TI = TD50 / ED50
autonomic nervous system
sympathetic and parasympathetic divisions have antagonistic functions
sympathetic: arousal, energy
parasympathetic: oposite, calming
ACh and noradrenaline
drugs affecting autonomic nervous system
cholinergic: acts on ACh receptors
adrenergic: acts on norepinephrine/epinephrine receptors
cholinergic agonist action sites
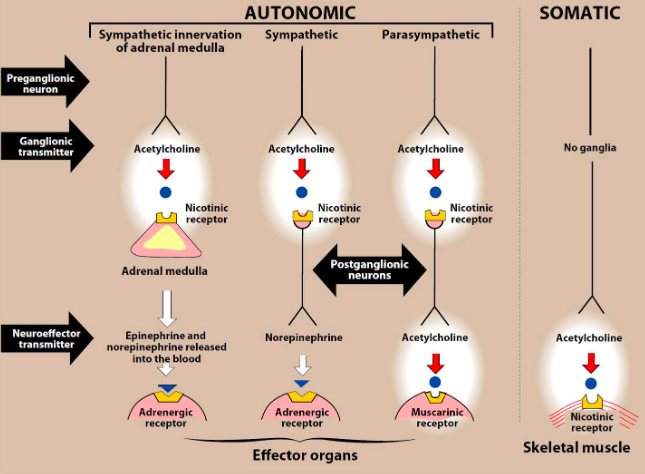
muscarinic receptors: PNS ganglia, autonomic effector organs. Ach and muscarine binding (low nicotine)
nicotinic receptors: CNS, adrenal medulla, autonomic ganglia, neuromuscular junction. ACh and nicotine (low muscarine
pilocarpine
cholinergic agonist
less potent than Ach, but penetrates CNS
glaucome use
applied to cornea
used with atropine to counteract toxicity
major catecholamines
norepinephrine, adrenaline, dopamine, isoprenaline (synthetic norepinephrine)
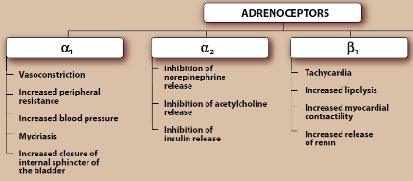
types of adrenergic receptors
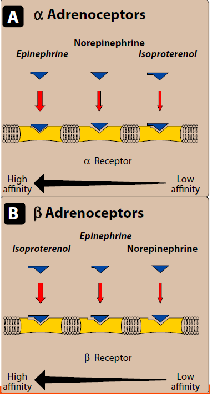
adrenergic agonists
direct-acting: direct of alpha or beta receptors —> stimulates sympathetic nerves
indirect-acting: block norepinephrine uptake
mixed-action agonist
pharmacological effect of epinephrine
cardiovascular system (contractility of myocardium, rate of contraction, renin release, dilate vessels, constricts arterioles
respiratory ystem: bronchodilation
hyperglycemia: decreased insulin, increased glucagon
lipolysis
uses: anesthetics, cardiac arrest, anaphylactic shock, bronchospasm
amphetamines
effect: locomotor stimulation, euphoria, insomnia, stamina, anorexia
side effects: anxiety, irritability, paranoia, psychosis
pharmacokintetics: absorbed from GI tract, penetrates BBB, half-life from 5 to 20/30h
parkinson’s medication
levodopa (dopamine prescursor) and carbidope (dopa decarboxylase inhibitor
DA receptors (G-protein-coupled) expressed in CNS and periphery
schizophrenia and drugs
symptoms: delusions, hallucinations
strongly genetic, probably DA pathway disturbance
reduced synaptic nerve ending density
1st gen: competitive inhibitors: bind (block) to DA neuroreceptors
2nd gen: clozazepine: less extrapyramidal symptoms (diskinesia, parkinsonism
harmful effects of drugs
paracetamol: liver cell death resultingfrom its metabolism
thalomide: teratogenesis (structural malformations in fetus)
why merge autism diagnosis? pros cons
+ easier funding, less stigma for more severe patients, more people in GWAS study, easier insurance, uniform diagnosis across countries
- studies might study different groups, high variance of symptoms makes sudying it harder, more stigma for aspergers
autism epidemic
more autism, less intellectual disability
risk factors autism
autistic family
cerebellar injury at birth
romanian orphanage
>9 weeks premature (skip out on gliogenesis)
<1 birth interval
hurrican strike zone
marent wth mental illness
father >40
mother >35
genetics autism
very polygenic
deletion and duplication de novo
network of genes related to synapse development, axon targeting, neuronal signalling
gender bias autism
females have stronger average connections with other genes from identified network
females have a protective effects needs higher genetic differences to trigger ASD phenotype

A: multiple threshold model: higher predispostion needed for females to reach threshold of symptoms
B: multifactorial liability model: female-specific factors shift female’s autism liability distribution away from the universal threshold
neuropathology ASD
amygdala: 13-16% bigger in young children, abnormal growth trajectory in puberty
disorganisation of neocortex in children
cerebellum: smaller, loss of purkinje cells, hypoplasia of vemris
eary autism diagnosis (lecture)
cognitive and adaptive rates are better when getting intensive behavioural intervention young
access more intervention, better verbal and overall cognition, more likely to attend mainstream school, required less ongoing support
basis of autism 2 hypotheses

cerebellum and autism
cerebellar damage: ASD symptoms
developmental perturbation → long lasting perseveration and deficits in social preference
acute cerebellar perturbation → increased cerebellar perturbation and decreased cognitive flexibility
ASD in mice
count behaviours in standard and enriched housing

negatives: hard to assess mood changes, tests not specific enough, medication reaction different, cannot use transgenic approach bc of polygenicity.
—> diagnosed autistic mice can then be tested in different circumstances
EEG
noninvasive
measure of electrical brain activity for scalp surface
generalised cortex activity
+ temporal precision, population-level neural activity
low spatial resolution, inaccurate for asychronous/smallscale actitivty
how does EEG work?


neurons have to be parallel and synchronous
negative voltage : excitatory synapse at dendrites
interpretation of EEG
neural oscillations: perceptual, cognitive, motor, emotional processes
no real understanding
EEG vs EMG vs fMRI
EEG+EMG better time resolution than fMRI
EEG: clinical research but EMG only research
EEG: cheap, easy to carry and use
EMG: only measure outward direction of magnetic waves
EEG signals
delta band (0.5/4 Hz)
predominant in babies
adults: sleep/hypoxia
frontal location (temporal and parietal lobe and thalamus)
theta band (4/8 Hz)
drowsy, light sleep
memory encoding/retrieval
frontal midline theta level correlates with changes in anxiety levels (associated with hippocampal theta rhythms
alpha band (8-14 Hz)
relax state, eyes closed
control inhibition
parieto-occipital brain areas
thalamus, pulvinar, lateral geniculate nucleus
beta band (14/30 Hz)
cognitive processing and motor control
frontal and central brain areas
parietal and temporal lobes
gamma band (>30 Hz)
sensory information, retrieval, episodic memory
hippocampus, sensory areas
premotor, parietal, temporal, frontal regions
ERP
event-related potential
transient-average fluctuation in the brain-s field as response to stimulus
probably reflects sum of postsynaptic potentials of synchronously active pyramidal neurons or cerebral cortex
mismatch negativity
diff b/w frequent stimulus and presentation of an oddball
100-250 ms
ERP’s: N400, P1-50, N1-100, P300
N400: semantic incongruence (negative 400)
P1-50: sensory gating (positive 1-50)
N1-100: change in auditory stimulus (can be positive or negative)
P300/P3: elicited by oddball experiment
selective attention
ERP shows that selective attention is just switching attention
SSVEP
steady state visual evoked potential
brain waves synchronise with flickering screen
can study temporal attention
personality
stable behavioural traits
phineas gage
rod through head
damaged frotnal lobas
change in personality, not intelligence
no impulse control, emotional cotnral, promiscuity
voles + vasopressin
administration
male partner preference, selective aggression, paternal care
meadow vole: asocial + promiscuous
prairie vole: social monogamous
praire vole had more oxytocin receptors and dense vasopressin strip
laws of gregor mendel
segregation: allele pairs segregate from each other during gamete formation
independent assortment: genes for different traits segregate independently
dominance: dominance decides expression of genotype
mice and burrow building
poliotonus: longer tunnels with escape routes (maniculatus)
tunnel length is hereditary, monogenically (3 loci)
escape tunnel is dominant trait (1 locus)
QTL
quantitative trait locus
dna section that correlates with phenotype variation
foxes and tameness
heridty of tameness
103 loci were associated with tameness (qtl mapping
SorCS1 gene: codes for synaptic plasticity and aids tameness
genetic archtiectures in humans

ACh system

inhibitory, fast, fast reuptake
norepinephrine system

fast acting and reuptake
dopamine system

hypothalamus and pituitary gland

serotonin system

5-HTTPLR
variant associated with neuroticism
account for 10% of phenotypic variance
mutation: more amygdala activation
functions diffuse modulatory systems
regulate
temperature (hypothalamus
uterus contraction during labor and milk secretion (oxytocin
blood pressure (vasopressin
immune system (cortisol
short-term feeding behaviour (dopamine, serotonin
attention (norepinephrine
sleep-wake cycles (serotonin
transgenerational epigenetic inheritance
new genetictheory
unconventional
there are heritable changes in gene activity without changes in DNA
persistent over gneerations
depends on environment
histone marks
can modify histones at the tails
chromatin state is dependent on the histone marks present
euchromatin (open) = transcription possibel
heterochromatin (closed) = no transcription
histone acetylation
acetylation —> dna around histone relaxes —> transcription
inhibiting de-acetylation improves LTM
histone methylation
methylation marks affect chromatin state
H3K9me3: open
H3K9me2: closed
linked to contextual feal memory formation
CpG methylation
in CpG islands (areas with a lot of C ad G’s), a repressive mark can block transcription
associated with contextual and auditory fear formation