UE Advanced DD and Interventions
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms

pt presents to PT with reports of aching pain and paresthesia along the medial aspect of the left arm extending into ring and small fingers. the PT performs the test demonsrated in image. if test is positive which is the MOST appropriate intervention?
a. strength upper trap and levator scapulae muscles
b. perform repeated cervical extension exercises
c. stretch the pectoralis minor and scalene muscles
d. perform grade III mobilizations to the first and second ribs
c. stretch the pectoralis minor and scalene muscles
Thoracic Outlet Syndrome - Definition
compression of neurovascular bundle - brachial plexus, subclavian artery and vein, phrenic nerve in the thoracic outlet at 3 sites
Neurological TOS
most common
C8-T1
paresthesia, numbness, weak grip, loss of manual dexterity
Arterial TOS
pulselessness, poor endurance, pallor, cold extremities
Venous TOS
edema, warm, cyanosis, swelling, mottled appearance
Interscalence Triangle Special Test
Adson’s Manuever
stretches scalences, decrease pulse if artery compressed
Interscalence Triangle - Intervention
stretch the scalene muscles
Costoclavicular Space - Speical Test
Military Brace Test
shoulders retracted and depressed
costoclavicular space - Intervention
mobilization of the first rib
axillary interval (pec minor space) - special test
wright test, roos test, allen test
axillary interval (pec minor space) - intervention
stretch the pectoralis minor
ULTT1 - nerve bias
median
anterior interosseous
ULTT 2 nerve bias
median
axillary
musculocutaneous
ULTT1 mnemonic
MAIN
ULTT2 mnemonic
MAM
ULTT3 nerve bias
radial
ULTT 4 nerve bias
ulnar C8 and T1 nerve roots

A patient reports tingling and numbness in the UE. the therapist decides to perform an ULTT on the patient shown in the image below found to be positive. based on the findings which nerve root is MOST likely contributing to patient’s symptoms?
a. anterior interosseous
b. ulnar nerve
c. musculocutaneous nerve
d. radial nerve
d. radial nerve
Subacromial Impingement
anterior/lateral shoulder pain
pain at night
painful arc (60-120)
subacromial impingement - special tests
Neer, Hawkins Kennedy, Yocum, Empty Can
Rotator Cuff Tear
age > 40 (overuse cases) or traumatic
anterior/posterior/superior shoulder pain with loss of strength
pain that wakes the patient during sleep, worse at night
weakness and atrophy
rotator cuff tear - special tests
ER lag sign, drop arm, hornblower’s sign, IR lag sign, lift off sign, belly press, bear hug
SLAP - labrum tear
traumatic sudden onset
deep anterior shoulder pain
clinking/clunking/joint locking - pain with throwing or biceps loading (shoulder flexion and arm supination)
SLAP labrum tear - special test
active o’brien test, bicep load, clunk test, crank test
SLAP meaning
superior labrum anterior to posterior
AC Joint Injury
trauma that displaces the shoulder girdle inferiorly or heavy weightlifting
pain at top of the shoulder
painful arc (170-180) and pain with horizontal adduction
step deformity
AC joint injury - special test
horizontal adduction, paxinos sign, AC sheer test
Bicipital Tendinitis
age 20-45
pain with overhead movements
pain with full extension to flexion. active external rotation limited when arm is at 90 abduction
bicipital tendonitis special test
speed’s, yergasons
a pt reports right shoulder pain reproduced when reaching overhead to place an item on a high shelf and when reaching across the body to fasten a seatbelt. Neer’s test and Crank test are both negative. These findings are MOST indicative of which shoulder pathology?
a. acromioclavicular joint sprain
b. subacromial impingement
c. glenoid labral tear
d. rotator cuff tear
a. acromioclavicular joint sprain
Coracoaromial Arch
a key site of pathology and an active treatment site
superior labrum anterior posterior (SLAP) lesion is superior labrum tearing/pulling away by the biceps insertion which is under subacromial arch
A patient underwent surgical repair of a SLAP lesion 2 weeks ago. Which of the following exercises is currently CONTRAINDICATED?
a. active isometric contraction of the biceps
b. passive humeral rotation with shoulder in scapular plane
c. prone scapular retraction
d. active assisted shoulder flexion to 90 in supine
a. active isometric contraction of the biceps
Repair of SLAP lesion
when bicep tendon detached - progress cautiously
limit passive or assisted elevation of UE to 60 for 2 weeks and limit to 90 at 3-4 weekks
only perform passive humeral rotation with shoulder in scapular plane for first 2 weeks
avoid tension on the biceps (elbow extension with shoulder extension) for the first 4-6 weeks
avoid active biceps contraction for 6 weeks
Rotator Cuff Rehab
initiate with isometrics
resisted exercises should not cause pain
rotator cuff strength before large primary movers
AROM for shoulder flexion and abduction must be done without shoulder hiking
no CKC 6 weeks
dynamic strengthening at 8 weeks (small tear), 12 weeks (large tear)
light functional activities 6+ weeks
a clinician is evaluating a patient with concerns of shoulder pain and concludes that this patient is potentially in the freezing stage of idiopathic frozen shoulder? which of the following is MOST accurately describes this stage?
a. pain that increases with movement and is present at night? loss of ER with intact rotator cuff strength
b. pain at rest with limited motion in all direction
c. pain only on movement. atrophy of deltoid, biceps, triceps, and rotator cuff muscles
d. minimal pain with significant capsular restriction from adhesions
b. pain at rest with limited motion in all direction
Adhesive Capsulitis - Stage 1
0-3 months
mild signs and symptoms - achy at rest, sharp at extremes ROM
capsular pattern - loss of ER and abduction present
synovitis more than contracture of capsule
Adhesive Capsulitis - Stage 2
Freezing/Painful
3-9 months with progressive loss of ROM and persistance of pain
motion loss in this stage reflects loss of capsular volume and a response to painful synovitis
loss of motion in all planes, pain in most of range
Adhesive Capsulitis - Stage 3
Frozen
9-15 months
painful stiffening of the shoulder and a significant loss of ROM
pain only with movements
atrophy of RTC, deltoid, biceps and triceps muscles
poor scapulohumeral rhythm with scapular hike
loss of axillary fold and ROM with capsular restriction
Adhesive Capsulitis - Stage 4
Thawing
15-24 months
pain lessens but stiffness persists
slow and steady recovery
Adhesive Capsulitis - Treatment
corticosteroid injection by MD
stretching determind by patient irritability
joint mobilization
joint mobilization for frozen shoulder
posterior inferior glide
a at presents with elbow pain that has gradually developed over few months. on exam tenderness over medial epicondyle and pain with resisted forearm pronation and wrist flexion. passive wrist extension with elbow extended reproduces symptoms. no sensory deficits present in UE. What is MOST likely diagnosis?
a. tennis elbow
b. pronator teres syndrome
c. golfer’s elbow
d. ulnar collateral ligement sprain
c. golfer’s elbow
Lateral Epicondylitis
lateral aspect of elbow pain
extensor carpi radialis brevis involved - activities w/ repeated wrist extension/grasping increase pain (gradual overuse)
lateral epicondylitis special test
cozen’s, mills, maudsley test
lateral epicondylitis treatment
offload to reduce pain and gradual progressive strengthening of wrist extensors
medial epicondylitis
anteromedial aspec of elbow pain
pronator teres + flexor carpi radialis involved - activties involing repeated wrist flexion increases pain (gradual overuse)
medial epicondylitis special test
medial epicondylitis test
medial epicondylitis treatment
offload to reduce pain and gradual progressive strengthening of wrist flexors
Nursemaid’s elbow
age 2-3 years
longitudinal traction on an extended elbow partial slippage of annular ligament over head of radius
position of arm - arm at side, with hand pronated (palm down), radial nerve can get injured
treatment: manipulation
DeQuervain’s Tenosynovitis
tenderness over lateral wrist and thumb
abductor pollicis longus and extensor pollicis brevis muscles are affected
severe pain with wrist ulnar deviation and thumb flexion and adduction
DeQuervain’s Tenosynovitis - Special Test
Finkelstein’s Test
DeQuervain’s Tenosynovitis Mnemonic
AbPL and EPB
apple and extra peanut butter
Carpal Tunnel Syndrome
tingling/numbness in the median nerve distribution of hand
repetitive activities and sustained positioning of wrist aggravates pain
thenar muscle atrophy seen in later stages
nigh pain
Carpal Tunnel Syndrome - special test
phalen’s test, tinel’s sign

distal radius fracture - colle’s fracture
dorsal displacement of distal fragment of radius
due to FOOSH injury
leads to dinner fork deformity

distal radius fracture - smith fracture
volar displacement of distal fragment of radius
due to fall on flexed wrist
leads to garden spade deformity
a pt who is postpartum, presents to PT with 2 month hx of pain along radial side of R wrist. pt reports pain worsens while lifting and carrying their infant and when gripping objects. on exam, tenderness over first dorsal compartment of the wrist. Phalen’s and tinels are negative. ROM of thumb limited d/t pain. Which of the following is most appropriate
a. splinting with thumb spica and activity modification
b. eccentric strengthening of AbPL and EPB
c. median nerve gliding and nighttime wrist splint
d. tendon gliding exercises with progressive thumb strengthening
a. splinting with thumb spica and activity modification
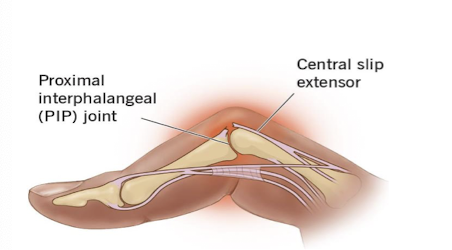
Boutonniere Deformity
extension of MCP and DIP, flexion of PIP
result of rupture of central tendinous slip of the extensor hood
most common after trauma or in RA
Swan Neck Deformity
extension of PIP, flexion of MCP and DIP
due to contracture of intrinsic muscles or tearing of volar plate
common in RA
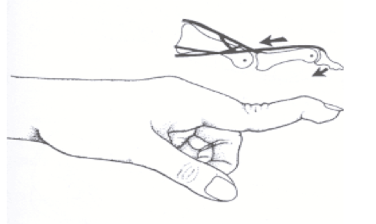
Mallet Finger
due to rupture or avulsion of the extensor tendon at distal phalanx of finger
distal phalanx at rest in flexed position
always traumatic (not RA)
Mallet Finger
splint with a finger extension splint for 6-8 weeks
Ulnar Nerve Motor Innervation - Mnemonic
MAFIA
Ulnar Nerve MAFIA meaning
medial lumbricals (on 4th and 5th digits)
adductor pollicis
FCU/FDP ulnar side
interossei
abductor digiti minimi
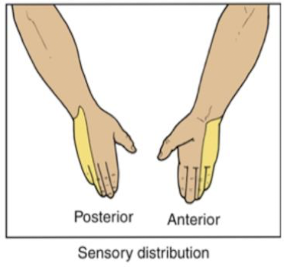
Ulnar Nerve - sensory innervation
hypothenar eminence
medial 1.5 digits dorsal and palmar aspects
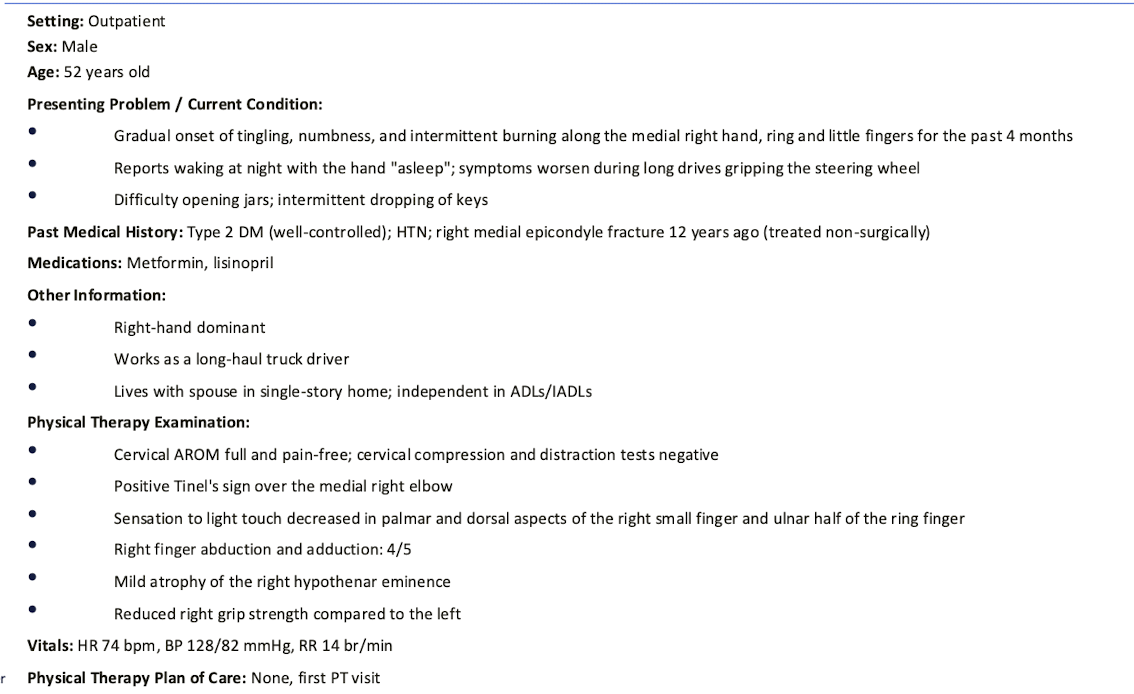
Based on the patients presentation which of the following is the MOST likely diagnosis?
a. cubital tunnel syndrome
b. carpal tunnel syndrome
c. guyon’s canal syndrome
d. cervical radiculopathy
a. cubital tunnel syndrome
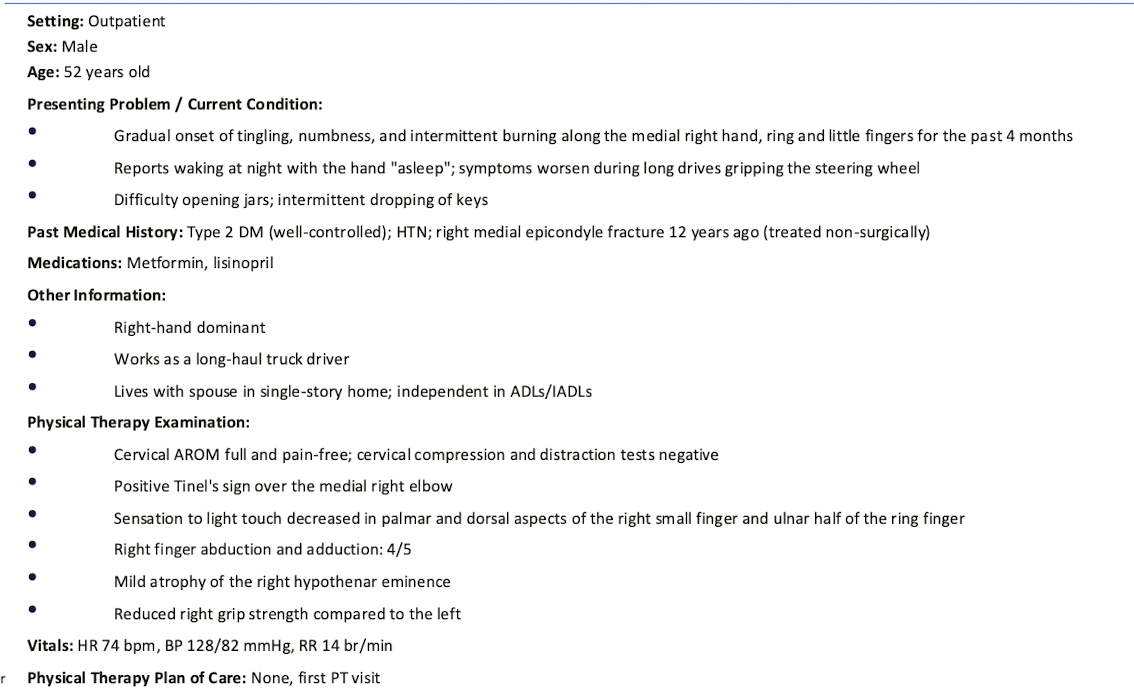
Which of the following actions is MOST likely to be different for this patient to perform?
a. opposing thumb to the tip of the small finger
b. pinching a key firmly between the thumb and side of the index finger
c. extending the wrist against gravity
d. flexing the distal interphalangeal joint of the index finger against resistance
b. pinching a key firmly between the thumb and side of the index finger
cubital tunnel syndrome
ulnar nerve entrapment between two heads of FCU
cubital tunnel syndrome - MOI
prolonged elbow flexion, fractures, spurs, arthritis
cubital tunnel syndrome - sensory or motor first
sensory
cubital tunnel syndrome - sensory symptoms
pain/sensory symptoms at 4th/5th digits (dorsal and palmar)
hypothenar (below little finger)
cubital tunnel syndrome - motor symptoms
weakness in FDP ¾
hypothenar muscles, ulnar interossei, adductor pollicis
cubital tunnel syndrome - tests
symptoms worst with elbow flexion test
positive forment’s (FPL substitutes for weak adductor pollicis)
wartenberg sign (inability to adduct the little finger)
tinels sign positive at elbow
guyon’s canal syndrome - MOI
history of heavy gripping, twisting, activities involving pressure (bicycling)
guyon’s canal syndrome - symptoms
motor - weakness in hypothenar muscles, ulnar interossei, adductor pollicis — NO FDP
sensory - pain/symptoms at 4th/5th digits (only palmar); hypothenar
guyon’s canal syndrome - test
froment’s
wartenberg sign
tinel’s sign positive at wrist
TMJ - opening of mouth (ROM)
depression of mandible
35-55 mm
opening of mouth muscle
lateral pterygoid
TMJ - closing of mouth muscles
elevation
temporalis, masseter, medial pterygoid
closing of mouth muscle mnemonic
MMT
protrusion of mandible
7 mm
medial/lateral pterygoid
retraction of mandible
3-4 mm
temporalis
lateral deviation of mandible
10-15 mm
lateral/medial pterygoid
a patient presents to PT clinic with reports of R sided jaw discomfort during chewing. on examination mouth opening measures 52 mm, and the jaw deviates to the left during the final phase of opening. there is no audible clicking and pain is minimal. which of the following is MOST likely diagnosis?
a. R TMJ hypomobility
b. R TMJ disc displacement with reduction
c. R TMJ hypermobility
d. R TMJ synovitis
c. R TMJ hypermobility
TMJ Hypomobility
decreased mouth opening and deviation to same side
TMJ Hypermobility
increased mouth opening
deviation to opposite side
TMJ disc displacement with reduction
clicking heard
no deviation
no difficulty with mouth opening
TMJ synovitis
pain and limited mouth opening
no deviation
TMJ Capsulitis
pain
limited mouth opening and deviation to same side