PSYC 322 Midterm 1 review
1/201
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
202 Terms
biopsychosocial perspective
view of development as a complex interaction of biological, psychological and social processes (not as a straightforward progression through time)
body goes through biological changes influenced by genetics + physiology
you change psychologically
happens in a social context — you change based on where you live, who you interact with, and resource availability
gerontologists use this interdisciplinary perspective
identity
how individuals view themselves in the biological psychological and social/cultural domains of life
4 principles of adult development and aging
changes are continuous over the life span
continuity principle
life span perspective
only survivors grow old
survivor principle
individuality matters
2 types of individuality differences
interindividual differences
intra-individual differences
multidirectionality
normal aging is different from disease
primary aging (Loss)
secondary or impaired aging (Loss)
tertiary aging (Loss)
optimal aging + normal aging
CSIN
Principle 1 of 4 principles of adult aging and development
changes are continuous over the life span
continuity principle: changes that people experience in later adulthood build on experiences they had in earlier years, YOU CANNOT ISOLATE THESE EXPERIENCES
applies to identity perception: you feel the same inside despite birthdays
when working with older adults: they are the people that they always were, rather than old people
eg you see an older woman walking with difficulty and don’t stop to think that she might have been a marathon runner in the past; you see someone who can no longer move their fingers as quickly and don’t stop to think that they may have been a professional musician.
Principle 2 of 4 principles of adult aging and development
Only survivors grow old
Survivor principle: people who live to old age are the ones who have managed to outlive the many threats that could have caused their earlier death
survivors have managed to avoid random causes of fatality like war, being killed in an accident, natural disaster, they are MORE LIKELY TO TAKE CARE OF THEIR HEALTH
not using drugs
not using alcohol excessively
association with biopsychosocial principle:
inherited good genes, good cognitive and emotional health, surrounded themselves with a good support system → these skills also contribute to skills desired by universities, meaning these individuals likely had good education as well
it is important to consider that older adults now were likely a special subset of their own agegroup
Principle 3 of 4 principles of adult aging and development
individuality matters
as people grow older, they become more different from each other — influences physical, psychological performance, relationships, work
Inter individual differences: differences BETWEEN people
intra individual differences: variations of performance within the same individual (individuals may gain intelligence in some spaces while losing it in others → THIS CONCEPT IS ALSO DEFINED AS MULTIDIRECTIONALITY
as people grow older, there is more divergence, and differences become magnified
people don’t start from the same point, there are already differences and these differences merely grow with time
if age is related to performance- there is a high chance that older group will differ simply due to age
2 adults of same age would differ more at older age than they would’ve when they were younger
Principle 4 of 4 principles of adult aging and development
Normal aging is different from disease → growing older =/= disease
we should not dismiss disease as “simply getting older” - do not write off health issues as simply getting older
primary aging- normal changes over time that occur due to universal, progressive alterations of body systems
secondary/impaired aging- impairment due to disease rather than normal aging
tertiary aging- rapid loss of function towards the very end of life; represents the impact of disease on already compromised areas
PRIMARY SECONDARY AND TERTIARY accumulate and in the absence of accident or injury, cause an individual’s death
optimal aging- age-related changes that can improve an individual’s functioning
interindividual differences
refers to principle of individuality- DIFFERENCES BETWEEN PEOPLE
intraindividual differences
principle of individuality- refers to variations in performance within the same individual
not all systems develop at the same rate
some decrease, others increase
MULTIDIRECTIONALITY
primary aging - principle 4 (normal aging is not diseased)
normal changes over time that occur due to universal, progressive alterations of body systems
secondary/impaired aging - principle 4 (normal aging is not diseased)
impairment due to disease rather than normal aging
tertiary aging - principle 4 (normal aging is not diseased)
rapid loss of function towards the very end of life; represents the impact of disease on already compromised areas
optimal aging - principle 4 (normal aging is not diseased)
age-related changes that can improve an individual’s functioning;
preventative or compensatory measures that adults take to counter effect of aging on their physical and psychological functioning
things that slow primary and secondary aging
issues w measuring by chronological age
measured on earth movement around the sun however physical changes in universe do not directly relate to what goes on inside the body
your body does not change significantly each time you pass a specific birthday
social meaning to age means more than the intrinsic meaning
maturity eg in apples is more easy to measure and quantify (in reference to the biopsychosocial process than people across cultures)
if we’re measuring by marriage, what if there is a lag with the economy and couples must wait to get married?
young-old subgroup
65-74
old-old
75-84
oldest-old
85+
centenarians
those who have lived 100 years+
110+ - supercentenarians
to counter chronologic age there were new concepts
functional age
biological age
psychological age
social age
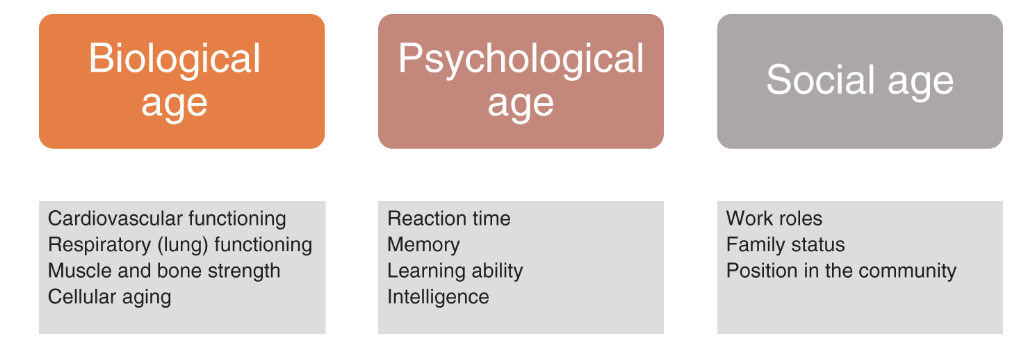
biological age
heart health
lung functioning
muscle and bone strength
celular aging
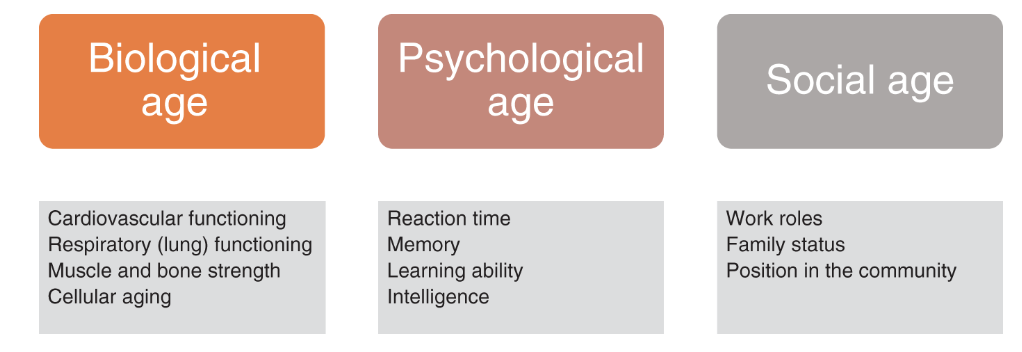
psychological age
reaction time
memory
learning ability
intelligence

social age
work roles
family status
position in community
functional age
viewing their characteristics and abilities, how they perform → has to be calculated, encapsulates biological age, psychological age, social age
biological age
age of an individual’s bodily systems → regards their ability to pump blood, get oxygen to their lungs, blood pressure
we can search for ways to manage and strengthen bone marrow, muscle strength
we can examine people through blood pressure age
psychological age
performance an individual achieves on measures of quality like reaction time, memory, learning, ability, intelligence
(all are known to change with age), compared to other adults, then scaled
social age
calculated by where individuals are compared to the typical ages expected for the positions they hold in life
ex. age getting into family roles
grandparents have older social age than parent, even though it is possible for them to be chronologically younger than the parent
parents can be in their late 20s and a grandparent
personal aging
changes in our body and body structures that reflect the passing of time
how people percieve primary, secondary and tertiary aging
social aging
the effects of a person’s exposure to a changing environment → 3 forms of social influences
normative age graded influences
normative history graded influences
non-normative influences
aging is a blend of what
social and personal aging
normative age graded influences (social aging)
age norms that traditionally dictate and direct where individuals believe they should be according to age; it is due to society’s expectations
eg. age for marriage, age for graduation/finishing school,
linked to biological aging process: when individuals are expected to fulfill specific tasks
normative history graded influences (social aging)
large scaled events that occur for everyone withina certain culture or geopolitical unit
eg. world war, economic trends, cultural changes and attitudes, ice storm
non-normative influences
random events that occur throughout life with no regular predictability → divorce, death of a relative, fire, fired from a job
key social factors in aging
sex and gender - individuals assume roles
ethnicity - ancestral origin, homeland, identity, culture
socioeconomic status - position in educational and occupational rank
religion
baby boom generation
babies born in the post WWII years 1946-1964
silent → greatest (fought in war), x, y, z
what does generation of older population statistically look like now (in terms of population)
more older people than ever, ¼ will be 65+ in around a decade, more and more centenarians
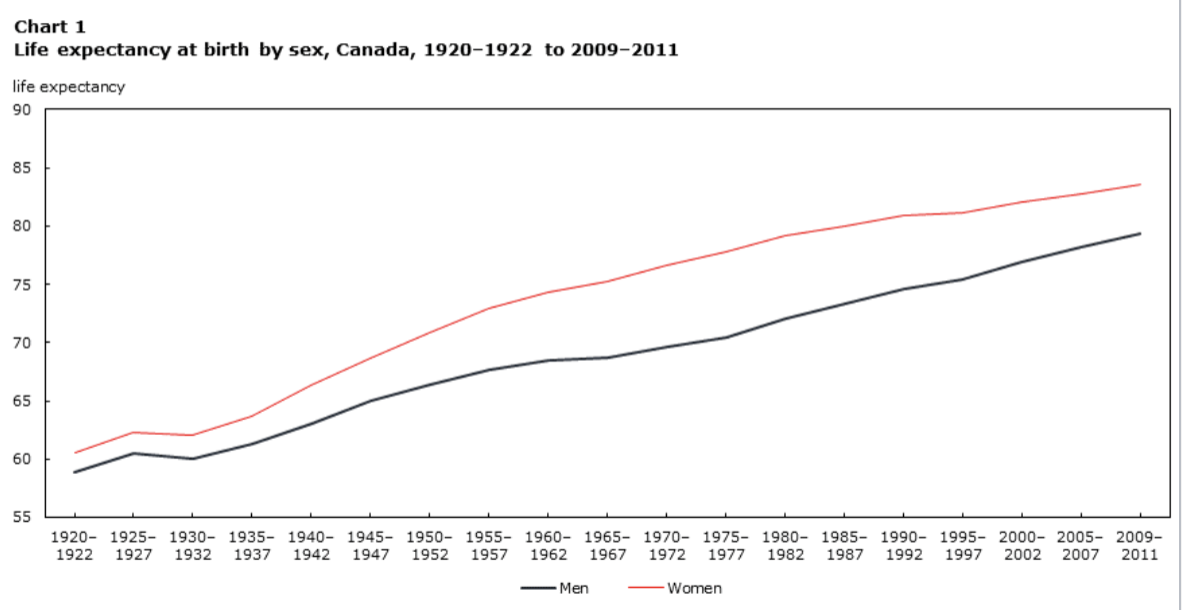
life expectancy
average number of years of life remaining for people born in a similar period of time
calculated with death rates for particular group + project to see how long it will take the entire group to die out completely
OVERALL: men are expected to live shorter than women
life span
maximum age for a given species; life span of humans has not changed but more people are living to older ages, leading to a life expectancy increase
health adjusted life expectancy
total numbers of years a person could expect to live in good health if current mortality and morbidity rates persist
compression of morbidity
an ideal situation in where the illness that burdens a society is compressed and mostly occurs closer to their time of death
sick for less time
what is happening around the world in terms of aging
there is a disproportional rate of aging from region to region; there is estimated to be 1.57 billion ppl over the age of 65 in 2050, yet right now, 55% of these individuals reside in asia, and only 7% in Africa
when we grow old, we will likely have more friends than the current population
men will live longer
what is gerontology
the scientific study of aging from maturity through old age
a newer, multidisciplinary field of study
what is the expected life expectancy difference between men and women
men tend to have a lower life expectancy than women
what is morbidity
illness and disease
mortality
death
life span perspective (continuity) - 4 principles of life
human development is divided to
early phase (childhood and adolescence)
later phase (young adulthood, middle age, old)
adulthood is influenced by early phase
consider:
multi-directionality (some things grow some things decline)
plasticity (capacity is not predetermined)
historical and cultural context
multiple causation (development is impacted)
Why are differences amplified in terms of individuality in the 4 principles of aging?
personality differences
physical function
life experiences
opportunities
pplo
what is normal aging
it is disease free development during adult aging that occurs for EVERYONE
what is secondary aging
development changes related to life style, disease, and other environmentally INDUCED changes
cancer, smoking, alzheimers
tertiary aging
rapid losses that occur shortly before death
the terminal drop/mortality aging
what is chronological age
percieved age
what is biological age
function of vital organs, frailness of body parts
what is psychological age
the functional level of psychological abilities to adapt to environmental demands
COGNITION, PERSONALITY, EMOTIONS
what is sociocultural age
related to work and family roles; IN RELATION TO SOCIETY AND OTHERS
3 theories of aging
biological theories
programmed aging theories
metabolic theories
random error theories
psychological theories
erikson’s psychosocial theory
identity process theory
selective compensation + optimization model
ageism
sociocultural theories
genes
sections of dna that contain hereditary info
chromosomes contain what
dna that carries genetic info
we have how many chromosomes
46, 23 pairs
What is a PROGRAMMED AGING THEORY - Theory of Age (biological)
aging and death are encoded in our genes
genetic timing= decline in our physiological function
evidence: species have specific life spans, cell senescence
what is cell senescence
the irreversible arrest of cell proliferation (growth or division); RESULT OF TELOMERE SHORTENING after repeated divisions over time
time and repeated cell division can lead to damage and mutation of genes
cells eventually stop dividing as much but also doesn’t die off
REDUCES RISK FOR CANCER
eg. cancer= uncontrolled growth
HAYFLICK LIMIT: fetal cells can only divide 50~ times
(programmed aging theory)
what does cell senescence lead to in the programmed aging theory
thicker artery walls
skin changes
arthritis
degeneration
changes in cardiovascular health
neurodegeneration (dementia risk + alzheimer’s risk)
telomerase
enzyme that can lengthen telomeres, slowing or stopping the cellular aging process
as you get older the telomerase doesnt work as well
metabolic theory of aging (biological)
organisms have a finite amount of energy to expend/ lifetime
an organism’s metabolism is related to its longevity
evidence: caloric restriction studies in nonhumans and humans
after 6 months on CR in non-obese adults :
lower levels of fasting insulin
lower core body temperature (metabolism)
less DNA fragmentation
ALL BIOMARKERS OF LONGEVITY
cr: decreased risks of morbidity
primates: cr= decrease in grey matter, no cognitive impact
young mice= cr = negative impact on spatial learning, negative impact on hippocampal neurogenesis
Identity Process theory (psychological theory of aging)
your identity continues to dynamically change in adulthood
some thresholds matter more than others
identity balance leads to self satisfaction
selective optimization with compensation model (psychological theory of aging)
as we age, we gain less and lose more
adults try to preserve and maximize activies of greatest importance, less maintanence of those of lesser importance
WE MAKE CONSCIOUS DECISIONS ON how to spend time and effort with declining cog and physical resources
WE OPTIMIZE WHAT WE HAVE as we grow and our functions decline to make the most of our abilities
selection → optimization (of resources) → compensation (using new processes to maintain level of functioning)
ageism - a psychological theory of aging
a set of beliefs, attitudes, and social institutions that cast way groups of people based on their chronological age
often associates old age with disease
how many generations of sociocultural theories are there
3 !
first gen (oldest)
disengagement theory
activity theory
second gen
continuity theory
life course perspective
bronfenbrenner’s ecological perspective
third gen
large focus on social structures
Disengagement theory - First Generation sociocultural theory of age
adjustment to old age is accomplished through voluntary withdrawal from social roles and activites
mutual belief that withdrawal is normal, better, universal, and inevitable
criticisms of disengagement theory - First Generation sociocultural theory of aging
engagement is not always voluntary
research was focused on individual, not society
unfalsifiable
justifies ageism
ignores thoughts and feelings of individual
“disengagement” isnt specific enough
Activity theory - First Generation sociocultural theory of aging
aging brings decreases in life satisfaction; social & psychological needs still need to be met; new roles, friends, activities lead to greater life satisfaction
social and productive activities were related to greater happiness, function, and reduced mortality
solitary activities were related only to higher levels of happiness
criticism for activity theory - First Generation sociocultural theory of aging
roles and activities mean different things for each person
assumes psychological and social needs remain constant through adulthood
presumes individuals have high degree of control over social situation
how is activity measured
continuity theory - Second Generation sociocultural theory of aging
people age and try to preserve internal and external ties as best as possible
emphasis on normal aging
keeping life a perfect mix of unpredictable and stagnant is OPTIMAL
criticism for continuity theory - Second Generation sociocultural theory of aging
normal aging ignores impact of chronic illness
theory ignores impact of social structures on aging
life course perspective - Second Generation sociocultural theory of aging
development happens on pathways of age-defined, socially marked- sequences between life events and social roles
age
historical time
social time (order you’re doing things)
life is shaped by historical + geographical placement
impact of transition depends on when it occurs
linked lives/ lives are interdependent
individuals control life course WITHIN constraints provided by history and social circumstance
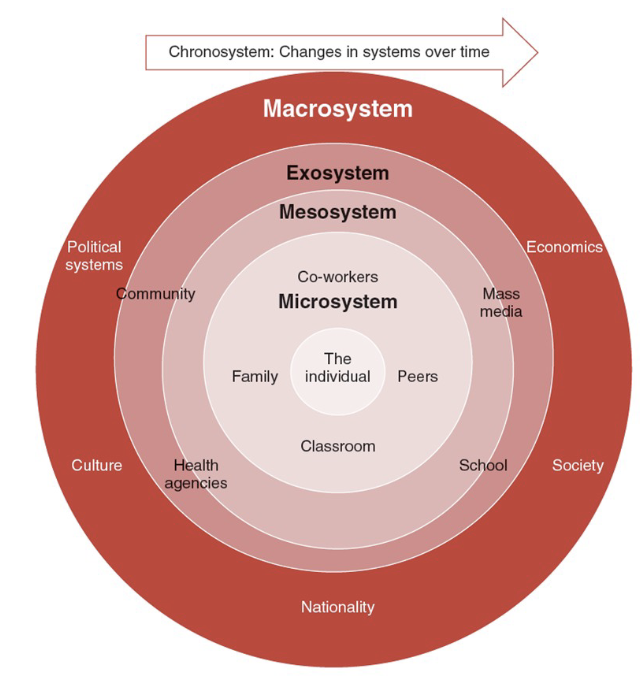
bronfenbrenner’s ecological perspective - Second Generation sociocultural theory of aging
a child's development is a product of both their biology and a series of systems that surround the child
emphasizes the importance of the space/environment that a child grows and resides in in relation to them
experimental study needs
iv (manipulation), dv, random assignment
pros + cons of experimental designs
can make a causal claim (iv caused dv)
can examine interactions with other factors like age (can be factorial)
cannot examine whether aging causes changes (this would be another kind of study) bec you cant randomly assign ages!!!!
quasi experimental designs
subjects are selected based on pre-existing values of independent variable NOT RANDOMLY SELECTED!!!
experimenter assigns values of IV to subjects
eg. pollution exposure + seniors
pros and cons of quasi experiments
allows researchers to examine effect of treatment that is likely already an occurance in one’s life hence MORE ETHICAL (eg. you cant throw people in pollution)
cons: less internal validity + no causation
correlational designs
type of non-experimental
measures association between 2 or more different variables in a sample + how strongly associations are
bivariate correlation ( r )
indexes degree and strength of relationship between 2 continuous variables
(correlation variables cannot be grouped)
pros and cons of bivariate correlation ( r )
describes relationship between two variables
CONS: DOESNT INFER CAUSATION, only useful for linear relationships, possible time of measurement, cohort effects the way descriptive research designs do
types of descriptive research designs
cross sectional
longitudinal
sequential
what can descriptive research design effects
age effects : differences caused by underlying processes that occur with things like aging
cohort effects : differences caused by experiences and circumstances unique to a generation or a person - OFTEN NORMATIVE + history graded
time of measurement effects: differences stemming from sociocultural, environmental, historical etc. at the time of data collection - often cohort effects in the making
effects are often confounded- results are not always relationship established.
cross sectional design - descriptive research design
snapshot into time
3 dif age groups and their results at the time being eg
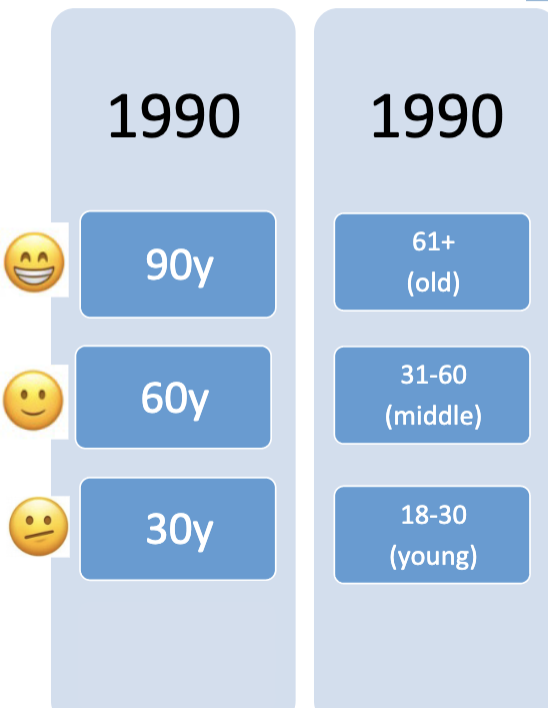
pros + cons of cross sectional design
+ age differences are examined in variable of interest, fast + cheap, addresses time of measurement effects
- might not be representative, doesn’t examine change in age, cohort effects, 3 extreme age groups can be problematic
longitudinal design - descriptive research design
follow same group of people of some period of time (like a cross sectional experiment but on multiple different occasions every few years
pros and cons of longitudinal designs
+ can assess changes as individuals age, outcomes are watched to examine any risk or possible protective factors
- age and time confounded, might not be generalizable, attrition (people can drop out), time consuming, expensive, measures may change, new studies may show up, researchers may lose interest
sequential research design
cross-sectional study conducted at 2 or more times of measurement + 2 or more longitudinal designs that represent 2 or more cohorts
cross sectional comparisons
cohort comparisons
controlling for cohort and time of measurement (same cohort in 1930 and 1960 eg)
timepoint cohorts
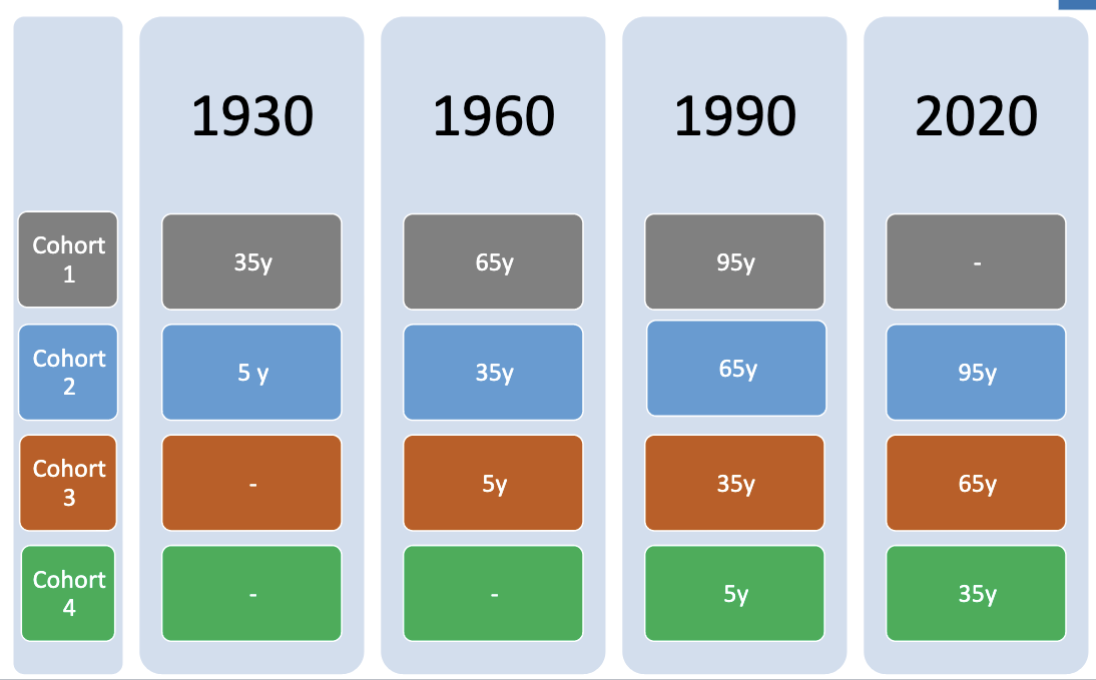
pros + cons of sequential designs
+ can examine cohort effects, different comparisons can be made, confounds can be examined
-selective attrition (some people are more likely than others to be selected), practice effects during study, measures of tech may change, researchers may change, knowledge may change, study may not get to be completed
common changes in vision - primary aging
less light passing through (more light is needed to do tasks) - iris loses strength, pupil is smaller
sensitivity to glare
light and dark adaptation is worse
loss in peripheral vision (about 1 degree a yr, 20-30 once we get old)
presbyopia -lens’ ability to adjust and focus declines (stiffening); time needed to adjust from near to far is worse
changes to vision - secondary aging
cataracts
glaucoma -loss of vision
macular degeneration - loss of central vision
cataracts disease - secondary aging
symptoms- seeing through a frosted window, difficult to see at night, read, see expressions, sensitivity, halo around light, double vision
causes- aging, injury changes tissue in eye lens, proteins and fibres break down
after treatment can be returned to normal- yes (lens is removed or artificial lens is put in)
how can one reduce risk of condition- regular eye exams, no smoking, managing health, health diet, sunglasses, less alcohol
glaucoma - secondary aging
symptoms- may vary a bit but severe headache and severe eyepain, blurred vision, redness, halos
causes- optic nerve is damaged, blind spots develop as nerve damage = increased pressure
after treatment can be returned to normal- no, but treatment and checkups can slow or prevent vision loss esp if in early stages
how can one reduce risk of condition- eye drops,know family history, eye exams, eye protection
macular degeneration - secondary aging
symptoms- visual distortions (straight becomes bent), reduced central vision, brighter light needed for work, hard to adapt to low light, blurriness of printed words, hard recognizing faces, blind spots in central vision
causes- unknown? possibly genes and environmental factors like smoking, obesity, diet
after treatment can be returned to normal- no, but if diagnosed early + vitamin supplements, eating healthy, not smoking
how can one reduce risk of condition- manage medical conditions, don’t smoke, maintain good weight and exercise, lots of fruits and veggies, eat fish and omega 3
sarcopenia is what?
process of primary aging
age related loss to muscle tissue and strength
there is a greater loss of fast twitch fibres (jump, strength)
while slow twitch (endurance) → older individuals can still run
multifactoral cause - testosterone dropes, hormonal drops (menopause)
FROM DISUSE → when you use it less, you lose it faster
chronic disease +nutritional deficiencies
how can sarcopenia be slowed
strength training and lifting weights
this decreases risk of falls and risk of physical disability
bidirectionali relationship is also established: weaker muscles <=> disability
osteoarthritis
condition in which cartilage that cushions the ends of bones in your joints gradually deteriorate
pain and swelling
occurs in foot knees hands hip and spine
can flatten, swell
NOT PRIMARY / not simply with age
risks:
age, sex, injury( in youth can lead to more consequences in the future), genetics, obesity
common symptoms of osteoarthritis
(not primary)
pain
tenderness
stiffness
swelling
loss of flexibility
grating sensations ( bones on bones)
extra bits of bones that feel like hard lumps around the site
how does osteoarthitis affect one’s life?
those with osteoarthitis are 6 times more likely to report mobility problems outside
activities of daily living are more limited to those with osteoarthitis
are there any ways to treat osteoarthitis?
no, but it is important to strengthen the muscles that support sore joints and reducing weight
taking Tylenol, ibuprofen, injections that can slightly reduce swelling
physical therapy? +occupational therapy (bench installment)
ESP HIP AND KNEES!