L2: Growth Hormone and IGFs
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Growth hormone (GH= somatotropin): features
191 amino aid somatomammotropin
secreted by somatotrophs
similar to prolactin
Somatotrophs
makes up around 40% of the anterior pituitary gland
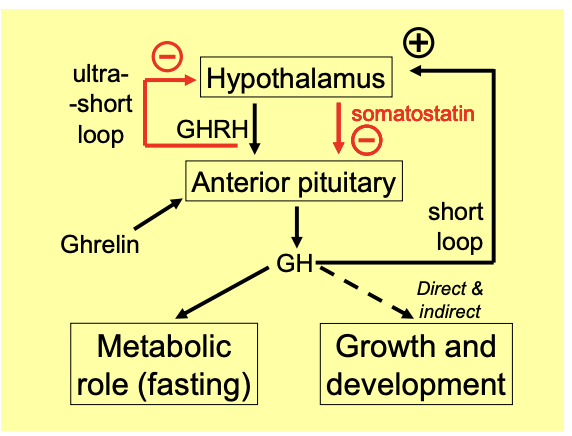
GH release is stimulated by…
Hypothalamus→ growth hormone-releasing hormone
GHRH
Stomach→ Ghrelin
What is GH released inhibited by
somatostatin
What does GH do?
promotes synthesis and release of somatostatin
→ short-loop negative feedback
GHRH inhibits its own release
→ ultra-short-loop feedback
How does GH circulate in the body
in plasma
bound to binding proteins
BUT:
half life is still just 20 mins
this is unusual for a peptide hormone
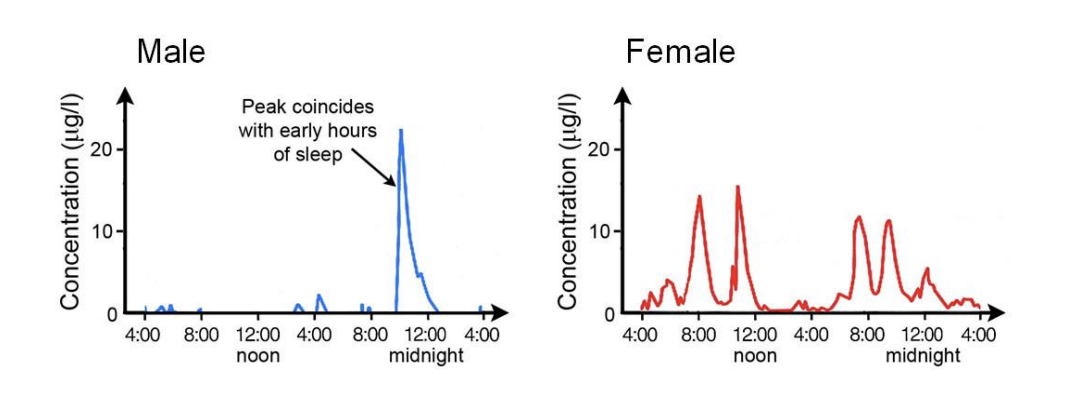
How does the release of GH occur
Erratic pulses
Men:
consistently show a large peak in early hours of sleep
driven by testosterone
Women:
mean level is higher→ suggests there is other effects other than growth
but more irregular
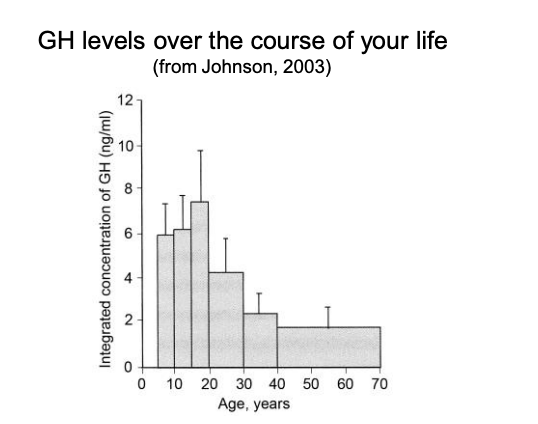
Childhood:
high
rising to a peak during puberty
declining but not zero over the preiod of adult life
exercise an other metabolic cues also promote release
GH levels in over the course of your life
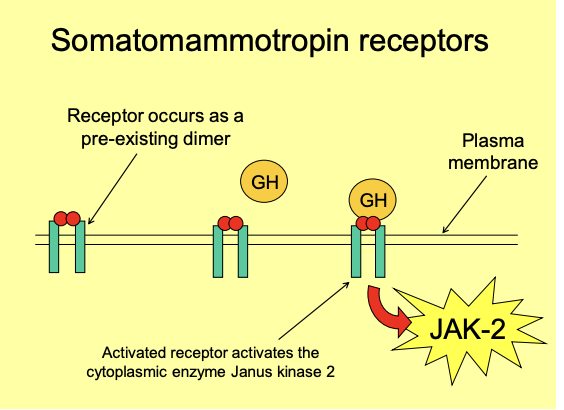
What does GH act on?
activates membrane-based receptors
which occurs as pre-existiging dimers
When activated→ receptor activates JAK-2 (Janus kinase 2)
enzyme in the cytoplasm
This phosphorylates tyrosine residues on proteins
Metabolic role of GH in fasting: when is GH release
In response to:
hypoglycaemia
low free fatty acids (FFA) levels
Metabolic role of GH in fasting: these effects may be seen during…
an overnight fast
esp after several days of starvation
Metabolic role of GH in fasting: what does GH help to do
Preserve glucose for the brain:
by switching the metabolism of peripheral tissues towards the use of FFAs
promoting gluconeogenesis
Metabolic role of GH in fasting: how are GH effects antagonistic to insulin and analogous to cortisol
GH acts on adipose tissue→ to release FFAs
GH stimulates hepatic gluconeogenesis and glucose ouput
GH acts directly on insulin-sensitive target cells
such as muscles and adipocytes
to inhibit glucose uptake
→ diabetogenic effect→ ‘mimics what happens in diabetes’ but is not a pathology!
Growth hormone and growth: GH is also released in response to
High amino acid levels:
arginine especially
Growth hormone and growth: what does GH do in this circumstanc?
promotes uptake of amino acids into
muscle cells and chondrocytes
Increases rates of protein synthesis
cellular growth and differentiation is promoted in many other tissues
Therefore, GH helps to
Break down fat→ → Increase protein
Used in dairy cows-. so promotes lactation
Used to make animals leaner and more muscle
Athletes?
if they alreayd have little fat→ will not make a differenece
Growth hormone and growth: why is control of growth complicated
affected by environmental and genetic factors
→ sex
Growth hormone and growth: other hormones and their connection with growth?
e.g insulin and thyroid hormones
→ NEEDED for growth
but
→ do not CAUSE growth
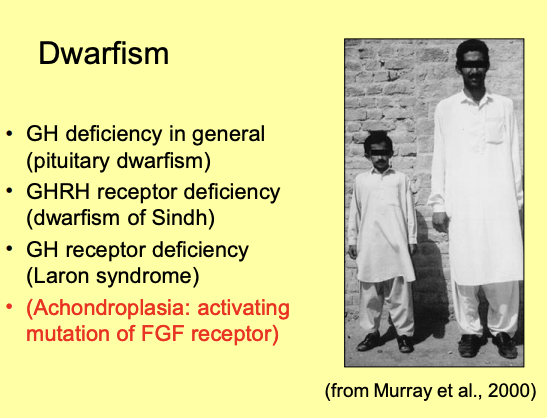
Growth hormone and growth: significant deficiencies in growth are
Dwarfism
Growth hormone and growth: possible causes of dwarfism
Pituitary dwarfism→ Failure to produce functional GH (for several reasons)
Dwarfism of Sindh→ defective GHRH receptor
Laron syndrome→ GH receptor mutations
lead to lack of IGF-1
Achondroplasia→ fibroblast growth factor receptor mutation
nothing to do with GH
most common form of dwarfism
Due to activating mutation of FGF recetpor
Note: the dwarfisms to do is GH→ rare and in proportion
Most common type of dwarfism→ limbs are smaller
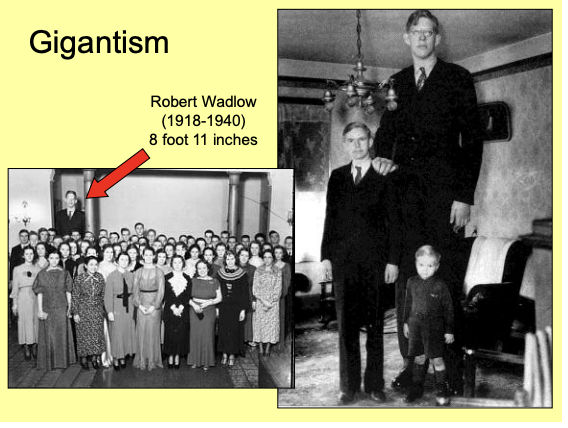
Growth hormone and growth: what happens if in excess as a child>
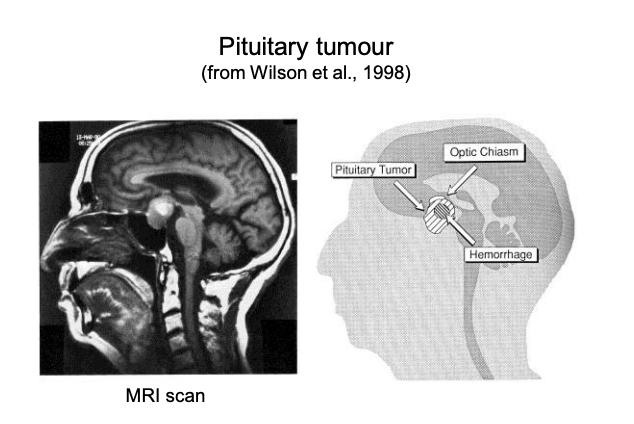
Gigantism→ over secretion from a pituitray tumour
Extreme height is due to overstimulation at the growth plates of the long bones
Growth hormone and growth: gigantism→ if growth hormone oversection occurs after the growth plates close…
height can no longer increase further
however:
periosteal (on the outside of the bone?) bone growth continues→ acromegaly
Anti-insulin effects of GH→ leads to diabetes
ALSO get poor eye sight→ due to tumour pressing on the Optic Chiasm
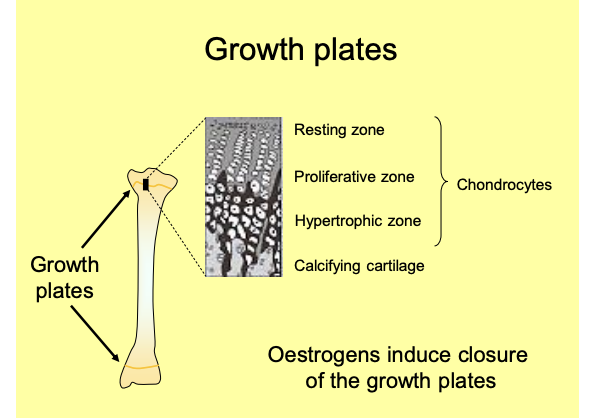
Effects of GH on growth plates: what does GH help to do
control growth at the growth plates of long bones
e.g those in the limbs
chondrocytes there lay down catilage
becomes calcified
ultimately ossified→ allows the bone to elongate at these regions
As cartilage around them calcifies→ These cells themselves proliferate, hypotrophy and then die
Growth plates ‘close’ in late teens
fuse up, such that the bones cannot elongate any further
earlier in women than men
due to oestrogen
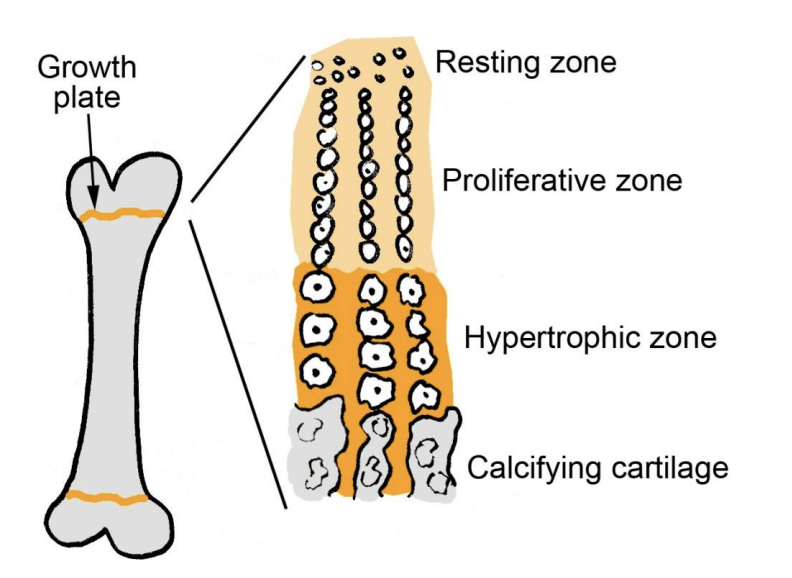
Description of growth plate strucutre/growth
Resting zone→ stem cells
Proliferate and get bigger_ .Proliferative zone→ chondrocytes
Bigger→ Hypertrophic zone→ chondrocytes
Get Calcified→ Calcifying cartilage→ bone
chonrocytes are cartilage cells
The thin layers of cartilage move away from eachother
oeastrogen induce closure of teh growth plates
Where does oestrogen come from in men?
locally converted from testosterone
Castrati→ castrated→ often taller because has more oestrogen
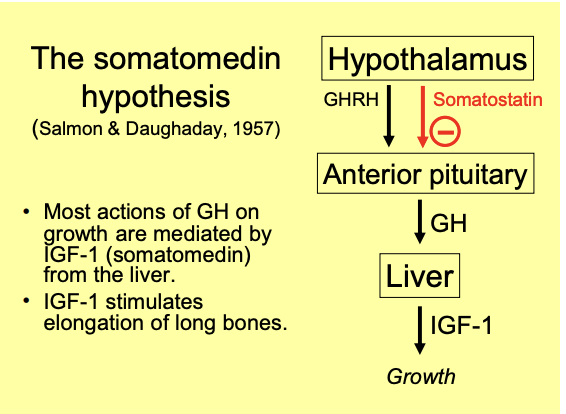
The somatomedin hypothesis: what is it
most actions of GH on growth are mediated by insulin-like growth factor1
IGF-1→ somatomedin
Released by the liver in response to GH
IGF-1 stimulates elongation of long bones
The somatomedin hypothesis: why proposed?
observation that cartilage from rates did not proliferate when incubated with GH alone
The somatomedin hypothesis: IGF features
so-called because of their structural similarity to proinsulin
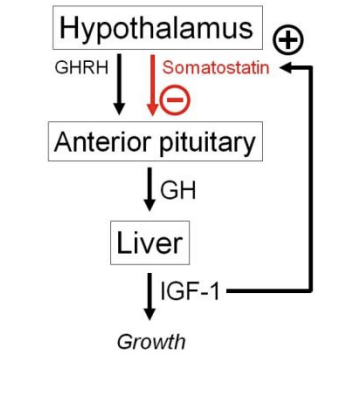
forms a negative feedback mechanism:
The somatomedin hypothesis: how does it form a negative feedback mechanism
increases somatostatin released
by hypothalamus
→ inhibits GH production by the pituitary
The somatomedin hypothesis: IGF-1 plasma levels throughout lifetime
increase with age
peaking at puberty
falling off in adulthood concomitatnt with decrased GH
The somatomedin hypothesis: how does it circulate the blood
plasma binding proteins
→ IGFBP1 to IGFBP6
half like is 20 hours
compared to under 20 mins for GH
The somatomedin hypothesis: levels of these binding proteins are controlled by
hormonal control of:
GH
Insulin
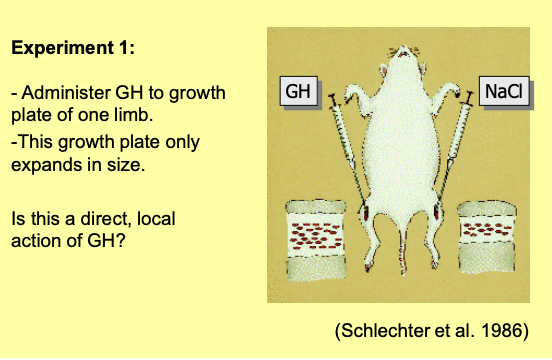
Challenging the somatomedin hypothesis 1: GH injection in growth plate
GH injection into a growth plate of a long bone in ONE LIMB
simtulates growth in the growth plate of this ONE LIMB
RESULT→ Local action of GH
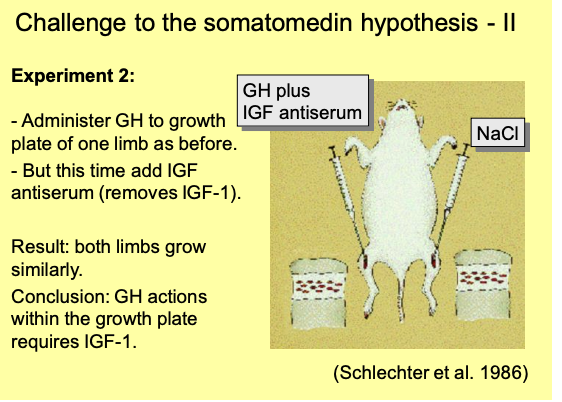
Challenging the somatomedin hypothesis 2: GH injection in growth plate with IGF-1 removed
removed by immunization with IGF-1 antiserium
GH to growth plate of ONE LIMB as before
But add IGF antiserum (removes IGF-1)
RESULT→ BOTH limbs grow similarly
Conclusion: GH actions within the growth plate requires IGF-1
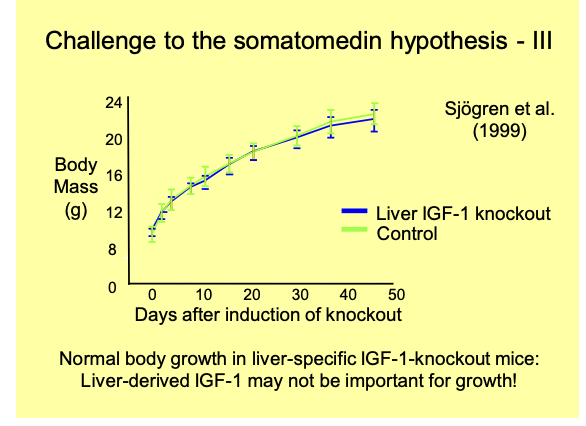
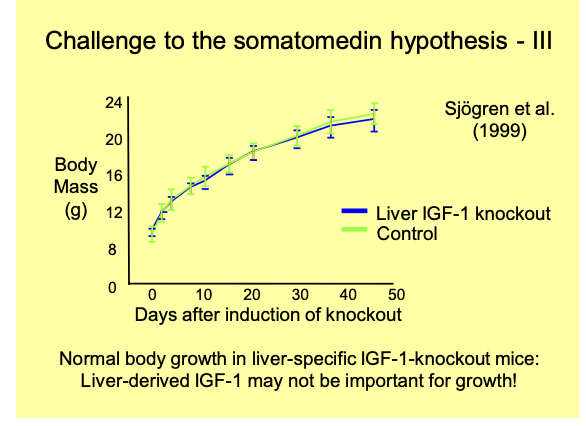
Challenging the somatomedin hypothesis 3: if liver-derived (endocrine) IGF-1 is specifically knocked out
RESULT→ body growth is normal
These experiments suggest…
IGF-1 is produced locally in target tissues
under the influence of GH
→ Liver-derived IGF-1 may not be important for growth
this developed the→ Dual effector hypothesis
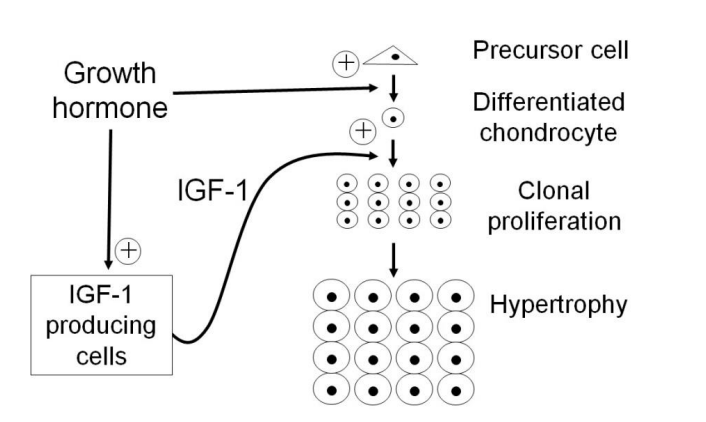
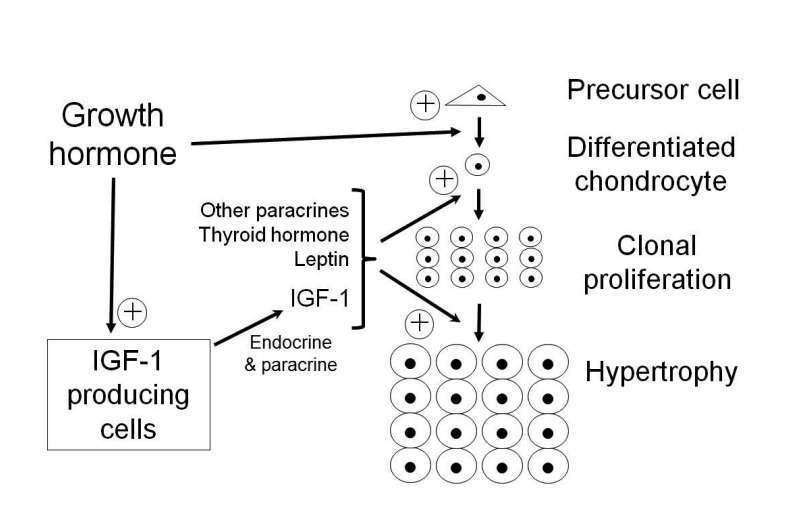
What is the dual effector hypothesis
GH stimulates the differentiation of chondrocytes in the growth plate
from precursors
and also
the local formation of IGFs
→ drives further growth
IGF-1 (endocrine and paracrine) acts as a second affector→ promoting the proliferation of chondrocytes
What did experiment 3 suggest?
that the endocrine IGF-1 is unimportant for growth
but this has been challenged!
Challenge to the results of experiment 3: is enocrine IGF-1 really unimportant?
there was still some IGF-1 circulating in the plasma
so, a reduction in IGFBPs might have resulted in higher effective IGF-1 levels than previously believed
→ later studies removing all circulating IGF-1 do show an effect on growth
In fact, IGF-1 is likely to be invovled both as…
Paracrine
and
Endocrine signal
an ever-expanding number of endocrine, paracrine and autocrine factors are being implicated as promoting intracellular growth regulatory pathways
→ very complicated!
e.g thyroid hormones, leptin (tells the body there are availbale fat stores)
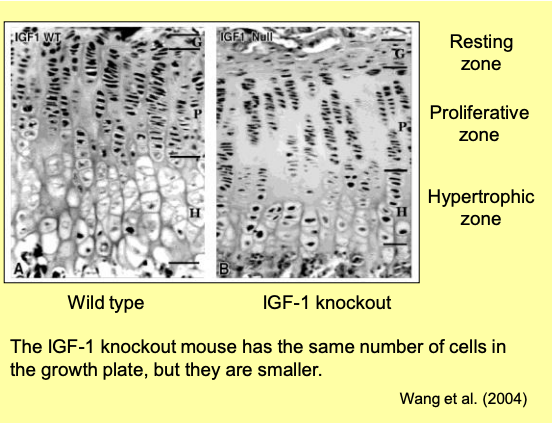
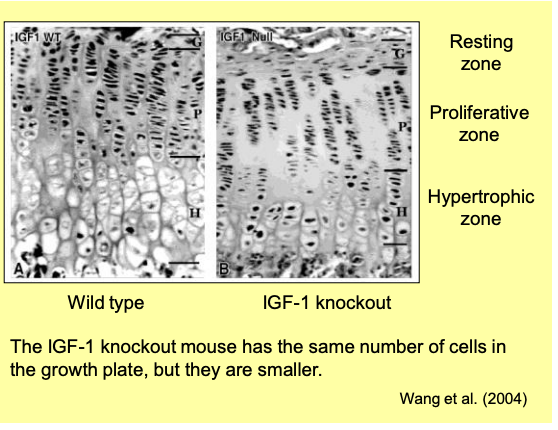
Experiment in IGF-1 knockout showed
The bone has the SAME NUMBER of cells as the wild type
→ just smaller
→ so IGF doesn’t affect the number
Overall feedback of the GH
Why does GH not promote growth during starvation?: paradox?
why would a hormones released during fasting
ALSO
promote growth?
→ how can the body dissociate the catabolic and anabolic effects of GH and ensure that growth is not promoted when resources are not availabel?
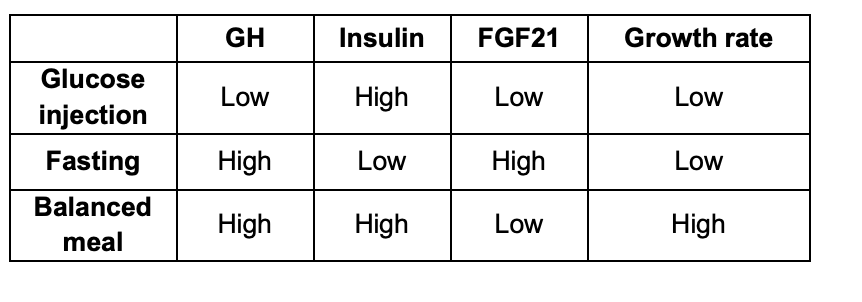
Important note: hormones have different affects depending on other hormone interactions and environmental conditions/states
When Fed→ Insulin has permissive effects on growth
When Fasting→ FGF21 promotes ‘GH resistance’
Why does GH not promote growth during starvation?: role of insulin in this question
insulin has important permissive effects on growth:
IGF-1 production by the liver
reducing leverls of some IGF binding proteins
→ increases the level of free and effective IGF-1
Why does GH not promote growth during starvation?: role of thyroid hormone in this question
also required for normal growth
Levels of thyroid hormone decline when fasting
Why does GH not promote growth during starvation?: role of Fibroblast growth factor 21 (FGF21) in this question
Released from the liver when fasting
in response to elevated free fatty acids levels
promotes ‘growth hormone resistance’
e.g by reducing the amount of IGF-1 produced in reponse to GH
Why does GH not promote growth during starvation?: Therefore, combined effect of
High GH
low FGF21
sufficient levels of insulin and thyroid hormone
→ required to promote growth
although many other factors are also involved
Interplay between GH and insulin
GH release is promoted by high amino acid levels
but
byt low glucose and FFA levels
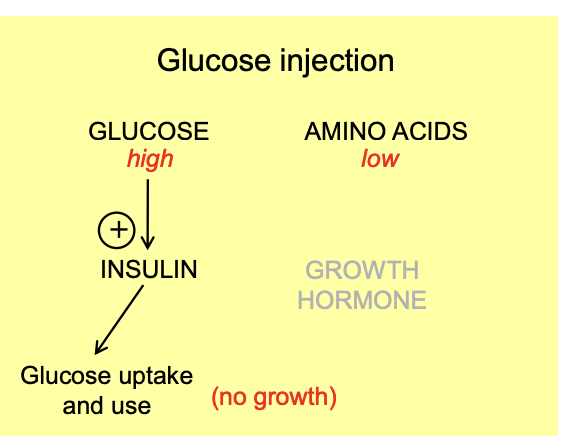
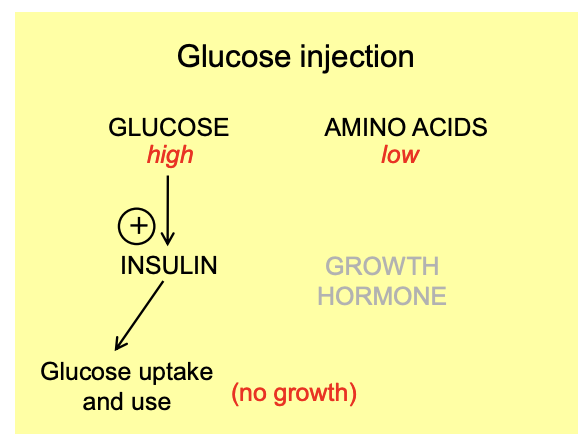
Pathway when Glucose injection
High glucose, low amino s
Promote inculin
glucose uptake and use
No growth coz growth hormone not PERMITTED by insulin co not enough aas
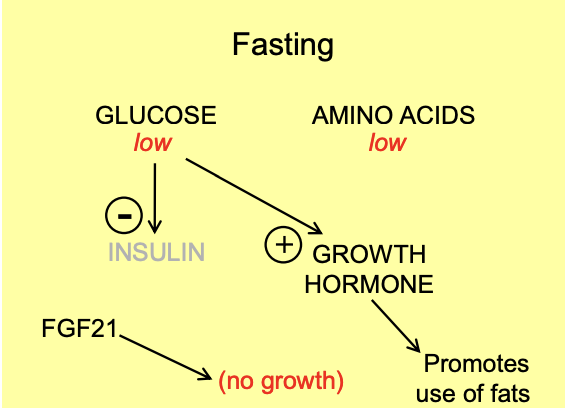
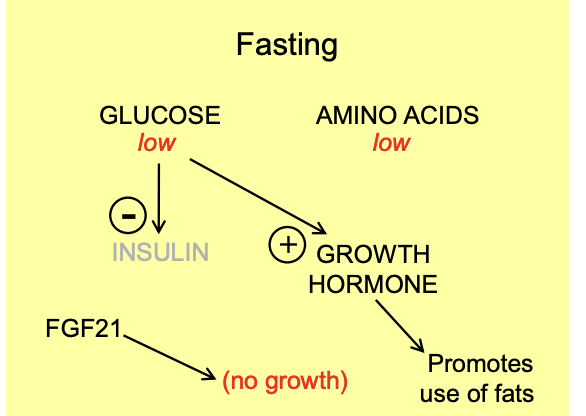
Pathway when fasting
Glucose low and aminos low
Hypoglycerimia promotes GH and is permissed by low insluin
Low gluose→ low insulin
GH promotes use of fat
FGF21 STOPS the GH growth effect
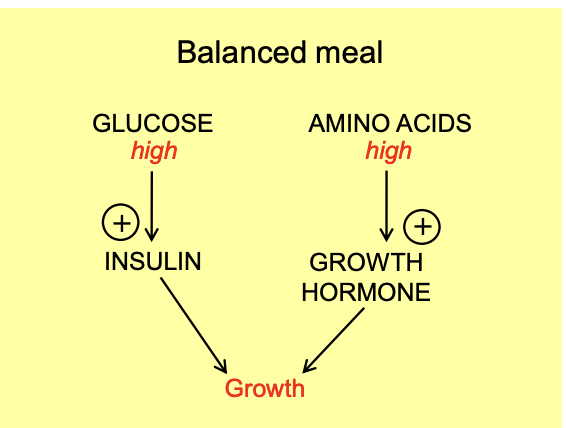
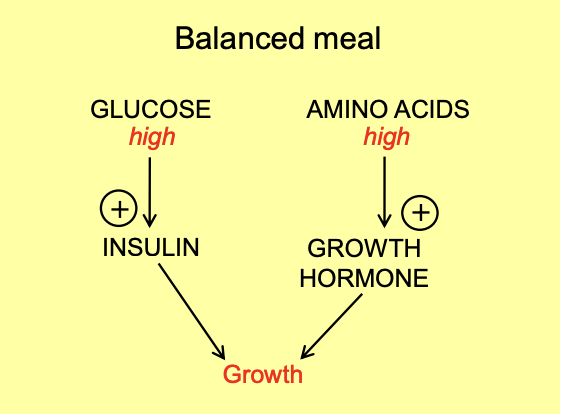
pathway when balanced meal
High glucose and aminos
Promotes insulin
AND promotes GH
FGF21 has no effect
Allows growth
Growth in utero: what is needed?
Pituitary growth hormones→ not necessary
IGF-1 and IGF-2→ important
imprinted genes
get paternal gene→ evolutionary arms race?
Growth in utero: production of IGF-1/2 are regulated before birth by…
hormones
inc: somatomammotropins and insulin
This is why:
→ pituitary growth hormone is not required
Example essay questions
Discuss the theoretical problems that you might encounter in designing and interpreting an experiment to investigate the effects of a hormone on the body.
Discuss the actions of the hormones in the growth hormone / prolactin family (NST 1B 1999: you’ll learn more about prolactin next term)
Is growth hormone inappropriately named?