Intro to Communicative Disorders: Test 4
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
Cleft lip
An opening in the upper lip
Cleft palate
An opening running through the soft palate and the bony roof of the mouth (hard palate)
What is the difference between cleft lip and cleft palate?
The location of the opening in the mouth
Cleft lip: upper lip
Cleft palate: inside mouth, through soft palate and hard palate
Can occur together or separately, both are caused by the failure of the lip and palate to form properly during pregnancy
Know the function of the velopharyngeal port and where it’s located:
Important to remember in understanding the problems associated with cleft palate; creates a tight seal between the velum and pharyngeal walls to separate the oral and nasal cavities for various purposes
Speech
Prevents food and water from entering the nasal passages
Located between the soft palate and the posterior pharyngeal wall in the back of the throat
Be able to identify the difference between an unilateral cleft, bilateral cleft, and complete cleft:
Unilateral cleft: a cleft on one side
Bilateral cleft: a cleft on two sides
Complete cleft: of the hard palate, two palatal shelves are totally separated
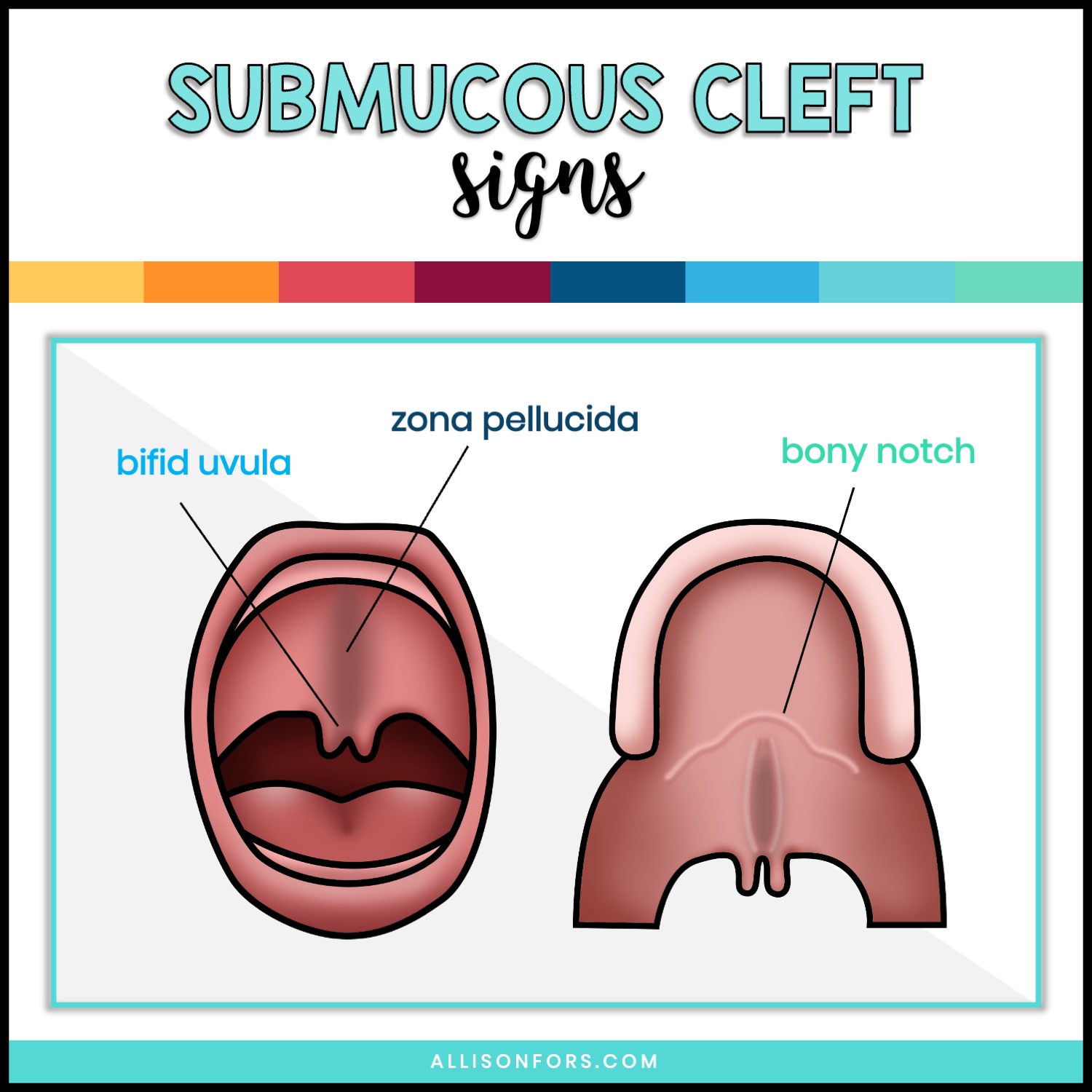
Submucous cleft
A hidden cleft of the hard palate, the soft palate, or both
Tissue covering the palate is normal, therefore the palate appears normal
Behind the normal covering, there is a cleft
Characterized by a bifid uvula
Know the definition of a conductive hearing loss and where it’s located as well as what typically causes it:
Definition: Middle ear problems resulting in hearing loss
Located: In the outer or middle ear
Causes: Otitis media (middle ear disease), earwax, fluid, foreign object, etc.
Compensatory articulation
A child’s or adult’s attempt to produce speech sounds in usual ways because of physiologic deficiencies
What is nasal emission and what are some characteristics of it?
Faulty articulation by the child with cleft palate; discharge of air through the nose during the production of non-nasal (oral) speech sounds
May be silent or audible
Audible emissions add the noise of gushing air when it escapes through the nose
Sound quality: can sound like a soft hiss or a loud snort
Mostly heard on consonants like “p, t, k”
Weak consonants, short utterance length
Aural rehabilitation
Treatment sessions to demonstrate the use of the hearing aid from the standpoint of speech
Be able to identify the difference between a genetic cause and an environmental cause of cleft lip and/or palate:
Genetic factors: Has been associated with more than 400 genetic syndromes involving abnormalities of the face, head, and neck; typically inherited, chromosomal defects
Environmental factors: Drugs, radiation during the early days or weeks of pregnancy, and infections such as mumps, flu, or other diseases have all been found to relate to clefts in babies
Why is swallowing and speech production difficult for the cleft palate child?
They cannot build up enough air pressure to adequately suck to eat and produce various speech sounds
Why are middle ear infections so common?
Because of the proximity of the ear to the palate; dental problems are also very common until repaired
Do language problems/delays occur in the cleft population?
Yes
Be able to identify the most common speech sounds that the cleft lip and/or palate population has difficult with and why:
The following common patterns of misarticulation can be commonly found in children with clefts:
/s, z, voiced and voiceless th, sh, zh, ch, j (as in job), f, v, k, g, l, and r/
Labiodentals (like /f,v/) - deformed upper teeth make it difficult for the child to produce these sounds that require precise contact between the lower lip and upper teeth
Sounds like /s, z/ - deformed alveolar ridge makes it difficult to produce these alveolar sounds as well as the interdental sounds /voiced and voiceless th/
Sounds such as these that need consistent airflow such as /s, z, f, v/ may be produced with nasals such as /m, n/ (soup may be produced noop, fan may be produced man)
Sounds like /p, b, k, g, t, d/ - clefts of the hard and/or soft palate make it hard to build up air pressure in the mouth for these sounds to be properly produced
If proper airflow cannot be built up and quickly produced, sounds produce differently
/b,p/ will become /m/ and /t,d/ will become /n/
Words like “papa” becomes “mama” and “toe” becomes “no”
Why is it so important to assess velopharyngeal function as part of the evaluation process for cleft lip and/or palate?
Because a significant number of individuals with cleft lip/palate experience velopharyngeal insufficiency (VPI) which means their soft palate can’t close fully during speech
Leads to issues like hyper-nasality and nasal air emission
Can seriously impact their communication abilities and quality of life if not properly addressed
Why are language, articulation, swallowing, and voice all typical areas targeted in therapy when treating cleft lip and/or palate populations?
Because the anatomical differences caused by the cleft lip/palate can significantly impact these aspects of communication, often leading to difficulties with producing certain sounds, managing airflow during speech, coordinating swallowing movements, and achieving proper voice quality
Therapy aims to address these challenges and produce overall communication ability
Aphasia
Language disorder due to brain damage or disease; a variety of difficulties in formulating, expressing, and understanding language
May be receptive and/or expressive in nature
Most common in stroke patients
Apraxia
Inability to perform tasks on commands
Oral structures, verbalization, and limb movement
A neuromuscular disorder of sequenced movement of body parts in the absence of muscle weakness or paralysis
Difficulty in initiating and executing the movement patterns necessary to produce speech when there is no paralysis, weakness, or discoordination of speech muscles
Can be developmental or acquired
Dementia
Degenerative brain diseases resulting in behavioral deterioration and communicative disorders; progressive intellectual and behavioral deterioration associated with diseases of the nervous system in older persons
Traumatic brain injury
Communicative and cognitive deficits caused by injury to the brain sustained by physical trauma or external force applied to the head
Dysarthria
Slurred speech
What two structures are contained in the central nervous system (CNS)?
The brain and the spinal cord
Peripheral nervous system
Contains 31 pairs of spinal nerves
Nerves are attached to the spinal cord
Several of them control breathing and speech
Broca’s aphasia
Non-fluent aphasia
Found in Broca’s area (left frontal lobe of the brain)
Primary motor cortex
Wernicke’s aphasia
Fluent aphasia
Found in the left temporal lobe of the brain
Involved in comprehension
What is the parietal lobe responsible for?
Sensory functions, sense of touch, pressure, and positions of the body
Where is the primary visual cortex located?
In the occipital lobe of the brain
What is the responsibility of the cerebellum?
Means “little brain”
Attached to the back side of the brain stem and below the cerebrum
Regulates and coordinates movement of the body, including fine and complex movements necessary to produce speech
What are the most important cranial nerves involved in speech, language, and swallowing?
CN #5: Trigeminal nerve (largest)
CN #7: Facial nerve (facial muscles)
CN #8: Vestibulocochlear nerve (hearing and balance)
CN #9: Glossopharyngeal nerve (tongue and pharynx)
CN #10: Vagus nerve (controls everything)
CN #11: Accessory nerve (shoulder and neck)
CN #12: Hypoglossal nerve (tongue movement)
What are the various types of strokes (CVAs)?
Cerebrovascular accidents (strokes)
Embolus: blood clot
Embolism: wedge-shaped obstruction of the blood flow
Thrombus: stationary blood clot
Aneurysm: sack-like bulge on the wall of a weakened artery
Hemmorage: rupture or bleed within the brain
Aphasia can consist of both _____________.
Anomia
Naming difficulties
Impaired comprehension of spoken language
Receptive difficulties
Be able to identify a treatment technique for aphasia, apraxia, dysarthria, and right hemisphere damage:
Aphasia:
Individualized treatment based on the difficulties, behavioral treatments, and counseling with the family
Apraxia
Modifying the patient’s vocal and resonance qualities, improving speech rhythm and intonation/inflection patterns, and functional word production
Dysarthria
Oral motor strengthening and control
Targeting difficulties with speech production, respiration, resonation, articulation, and prosody as well as posture, tone, and strength
Right hemisphere damage
Targets neglect to the left side of the body, disorientation, deficits with facial recognition and attention, affective deficits, reasoning and planning deficits, communicative deficits, and impaired reasoning, planning, organizing, inappropriateness, rambling, and confabulated verbal responses
What type of patients are respiratory issues typically seen in?
Patients with dysarthria
Traumatic brain injury can occur from both _________________.
penetrating and non-penetrating accidents
Be able to identify some speech pathology related effects that a TBI patient would demonstrate:
Dysarthria (slurred speech)
Confused language
Anomia (naming difficulties)
Perseverative verbal responses
Difficulty in language comprehension
Pragmatic language problems
Rambling speech
Difficulty understanding facial expressions and gestures
Reading and writing difficulties