Ventricular Rhythms (DM)
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
When do ventricular rhythms form
sinoatrial (SA) node or the AV junctional tissues fails to generate an impulse
the VENTRICLES will assume the role of pacing the heart
ventricular rhythms
Rhythms that are initiated in the area of the ventricular
What is the least efficient pacemaker of the heart
Ventricules
How are atria depolarized in ventricular
Retrograde depolarizaation
What are common charateristics of ventricular rhythms
QRS are wide (> 0.12 sec) and bizarree
P waves are absent as they get hidden or buried in QRS
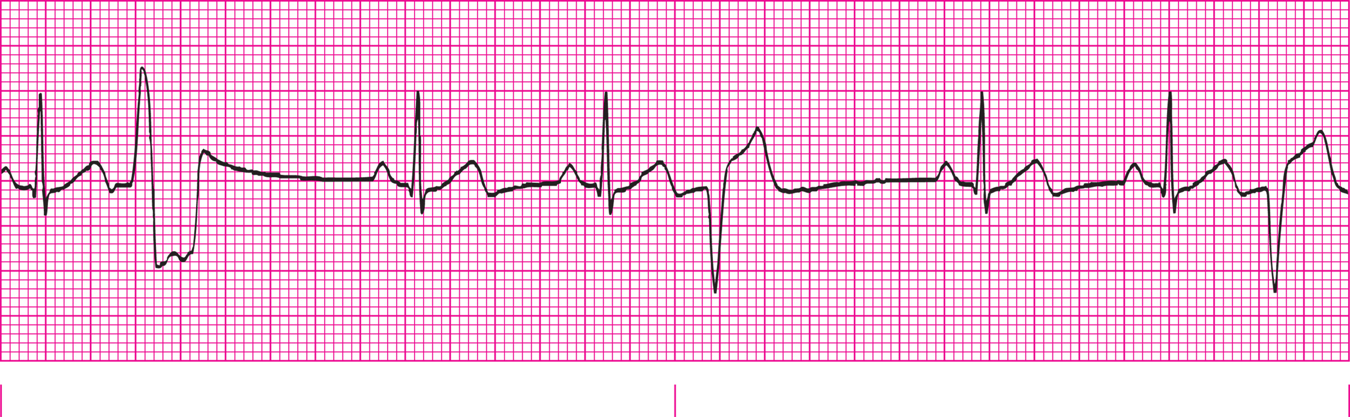
Premature Ventricular Complexes (PVC)
Single ectopic (out-of-place) complex that occurs earlier then the next expected complex
PVCs
What are the suggestive indicators of PVCs
Compensatory Pause
Wide, Bizarre, Premature QRS Complex
Where do PVCs come from
irritable site in the ventricles
PVCs are usually followed by
Compensatory Pause
Interpolated Bear
A PVC that fall between two sinus beats without interfering with the rhythm
What is the shape of the PVC base don
Site of Origin
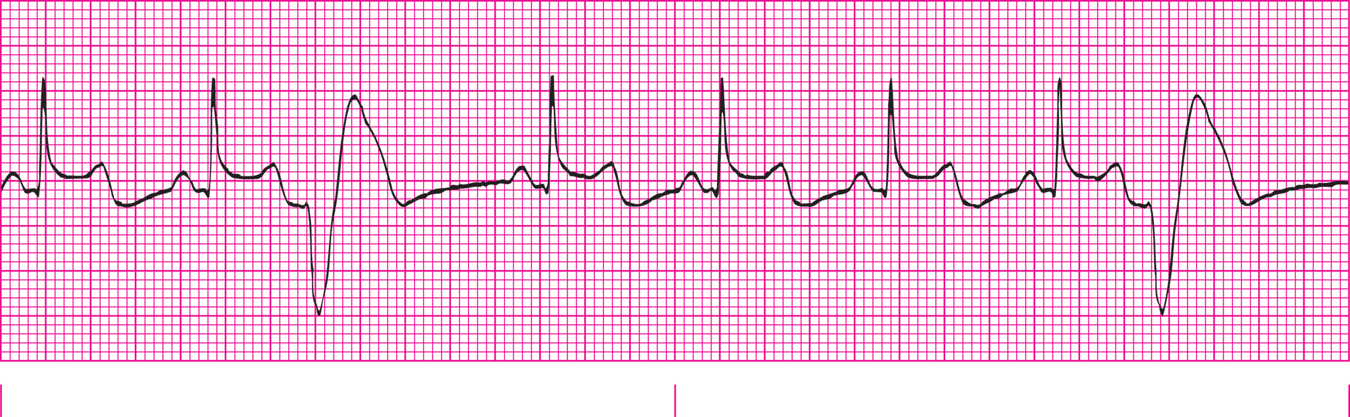
Ventricular Bigeminey
PVC every other bear
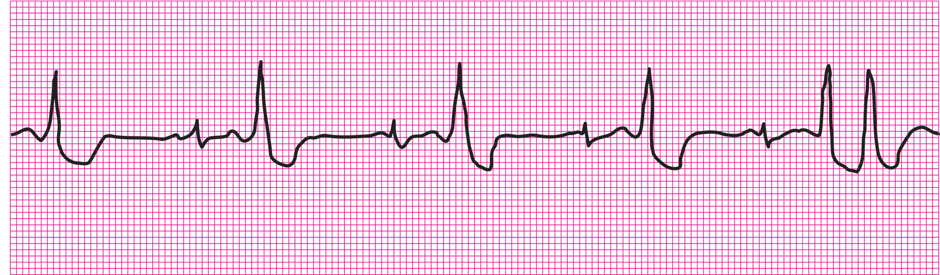
Ventricular trigeminey
PVC every 3rd beat
Ventricular quadrigemeny
PVC every 4th beat
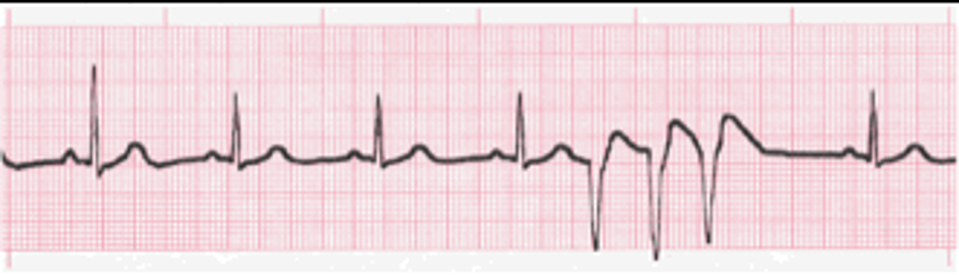
Couplet or Repetiteve PVC
Two PVC occuring together without complex in between
Runs of Ventricular Tachycardia
Three or more PVCs in a row
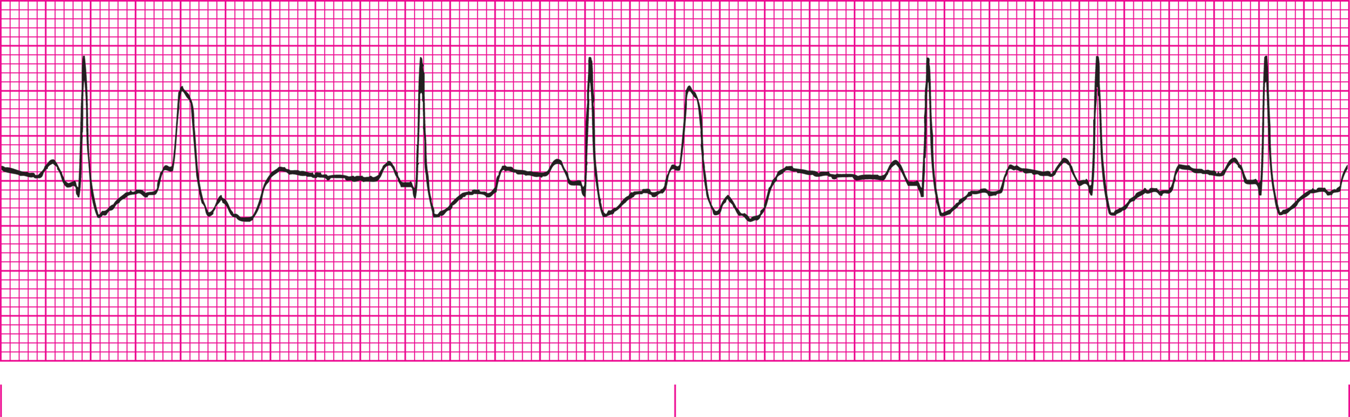
Characteristics of PVCs (5-Step)
Rate dependent on underlying rhythm and number of PVCs
Rhythm is occasionally irregular, regular if interpolated PVC
No P wave with PVC | P waves of underlying rhythms
PR interval not seen with PVC
QRS of PVC is wide and bizarre (> 0.12 sec)
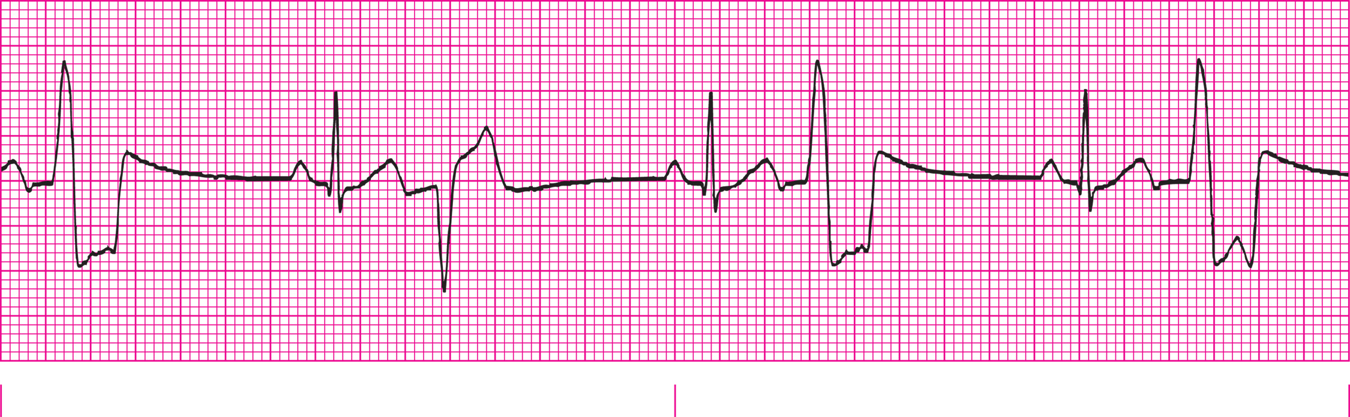
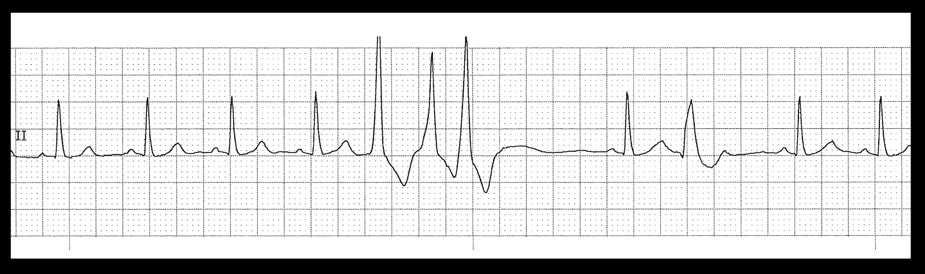
Unifocal PVCs

Multifocal PVCs
Salvos
Runs of Ventricular Tachycardia (3+ PVCs)
PVCs often indicate
Myocardial irritability
Ventricular Bigemey + Couplet PVC
Ventricular Bigemny
Ventricula Trigeminy
Salvo / Run of V-tach
Salvo / Run of VT
Salvo / Run of VT
Idioventricular Rhythms / ventricular escape rhythms
Means SA node and AV node have failed
Rate usually less than 40 BPM, and cardiac output is usually compromised
Agonal Rhythm
idioventricular rhythm falls below 20 BPM
When is agonal rhythm usually seen
either resuscitation is unsuccessful or after successful defibrillation
Causes of Idioventricular Rhythms
extensive myocardial damage
secondary to acute myocardial infarction
failure of higher pacemakers
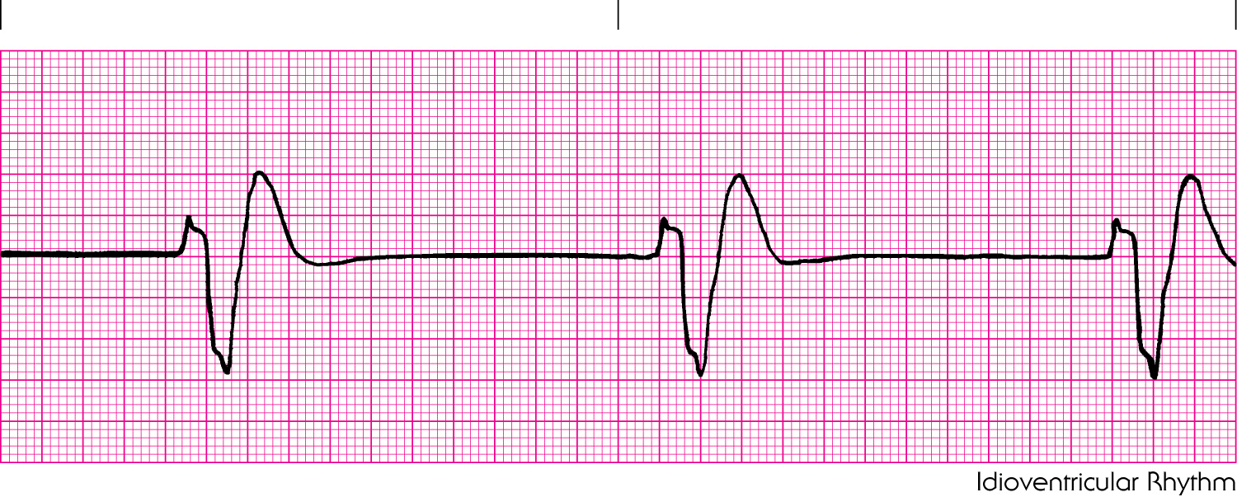
Idioventricular Rhythm
Characterisitics of Idioventricular Rhythms
Rate is 20-40 bpm
Atrial rhythm is not distinguishable | Ventricular is regular
No P waves
No PR interval
QRS are biazzare and wide ( > 0.12 sec)
Accelerated Idioventricular Rhythm
occur when the rate of the ectopic pacemaker exceeds 40 BPM
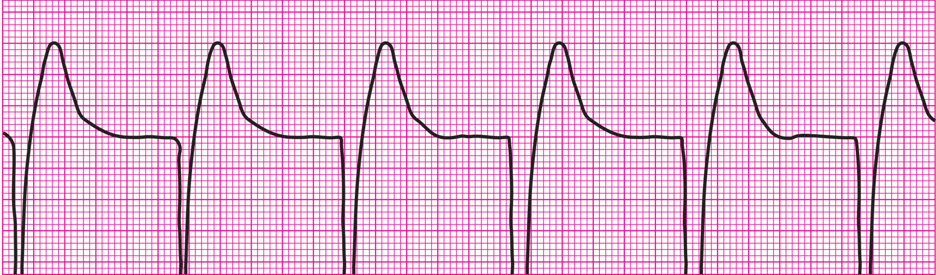
Accelarated Idioventricular Rhythm
What separates Accelarted Idioventricular from V-tach
Idio is < 100 bpm so it is not a tach
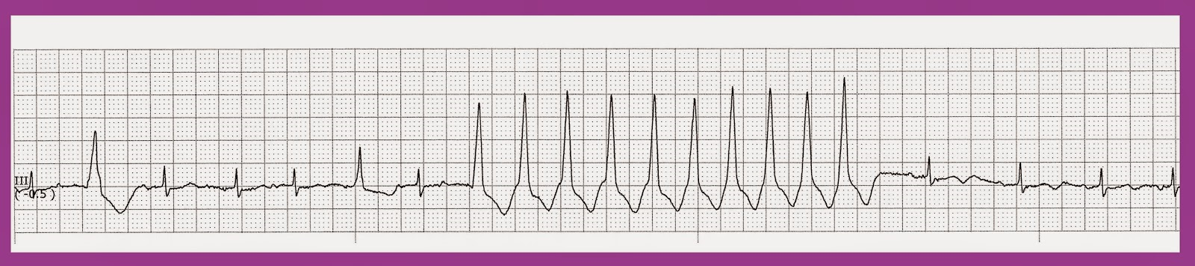
Ventricular Tachycardia Rhythms
three or more PVCs arise in sequence at a rate greater than 100 BPM
Sustained Ventricular Tachycardia
Lasts longer than 30 secs
Nonsustained Ventricular Tachycardia
Last less than 30 sec (Salvo / Run of V tach)
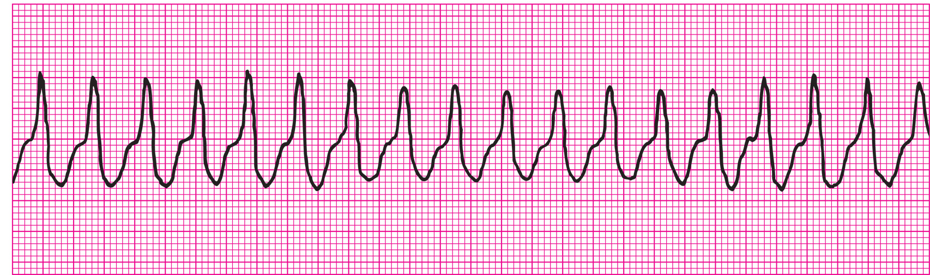
Ventricular Tachycardia
How do we subdivde V-tach
Pulseless or Pulse
Pulseless V-tach should always recieve
Immediate defib
Treatment of Unstable V-tach with Pulse
Immediate cardioversion
Treatment of Stable V-tach with Pulse
Drug intervention
Causes of V-tach
Myocardial ischemia,
hypoxia,
electrolyte imbalances
, increased anxiety or physical exertion,
underlying heart disease
Characterisitics of V-tach
Rate = 100-250 bpm
Atrial rhythm is not seen | Ventricular is regular
P wave may be seen but usually absent
No PR
QRS is uniform, bizaare, and wide
Torsades De Pointes
Morphology of QRS complexes shows variations in width and shape
Resembles a turning about or twisting motion along base line
Causes of Torsades De Pointes
Hypokalemia
Hypomagnesemia
TCA OD
Use of Antidysryhtmia
Combination
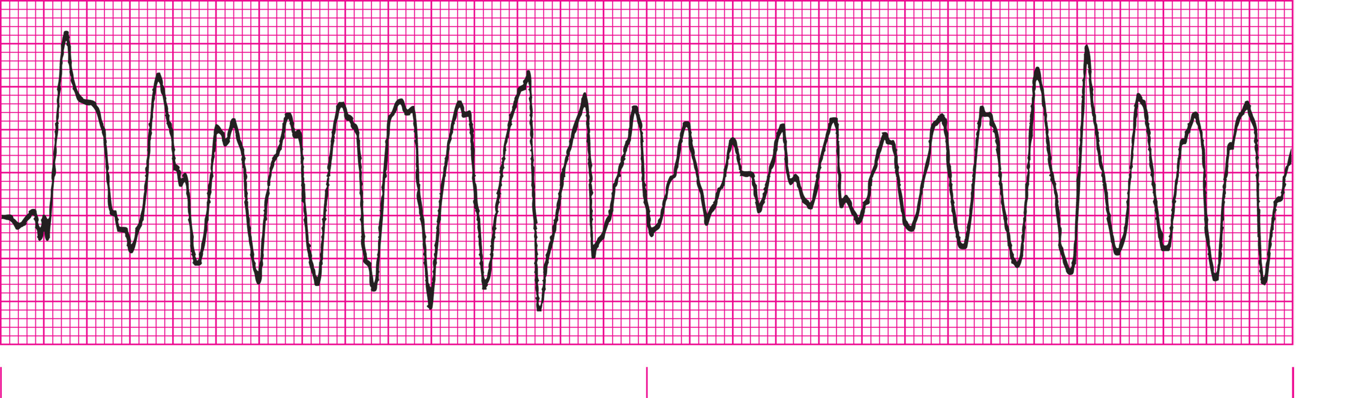
Torsades De Pointes
Treatment of Choice for Torsades De Pointes
Magnesium
most frequent initial rhythm occurrence in sudden cardiac arrest
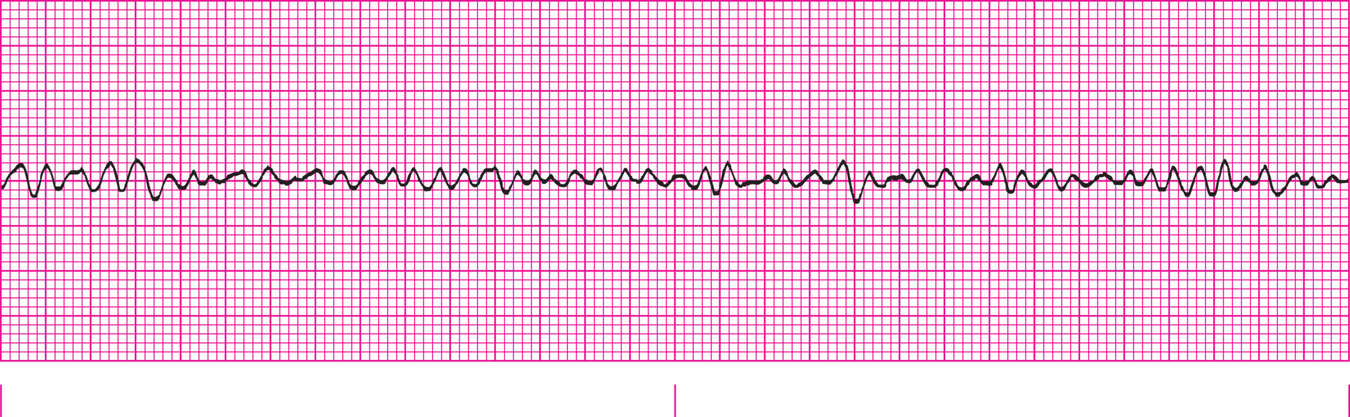
Ventricular Fibrillation
Ventricular Fibrillation
a result of multiple weak ectopic foci in the ventricles
appear to quiver rather than depolarize normally
What is not present with V-fib
Atrial contraction
Ventricular contractions
Palpable Pusle
How is waveforms for V-fib
disorganized, rapid, irregular waves whose morphology varies vastly
Fine ventricular fibrillation
Ventricular fibrillation waves less than 3 mm of amplitude
Coarse ventricular fibrillation
Ventricular fibrillation waves with amplitudes greater than 3 mm
What is critical to determine if monitor shows V-fob
artifact, or loose leads
Causes of V-fib
Acute MI
Ischemia
Drug Tox or OD
Hypoxia
Characteristics of V-fib
Rate is not discerned
Rhythm is rapid and unorganized
No P
No PR
No QRS
Fine V-fib

Coarse V-fib
Ventricular Asystole / Standstill / Asystole
The absence of all ventricular activity
How does asystole look
flat line, and is the absence of all cardiac electrical activity
How is asystole determined from fine V-fib
Check two different leads
Causes of Ventricular Asystole
Massive MI
Cardiac trauma
Ventricular Aneurysm
Complete Heart Block
Characteristics of Ventricular Asystole
No rate
No rhythm
No P
No PR
No QRS
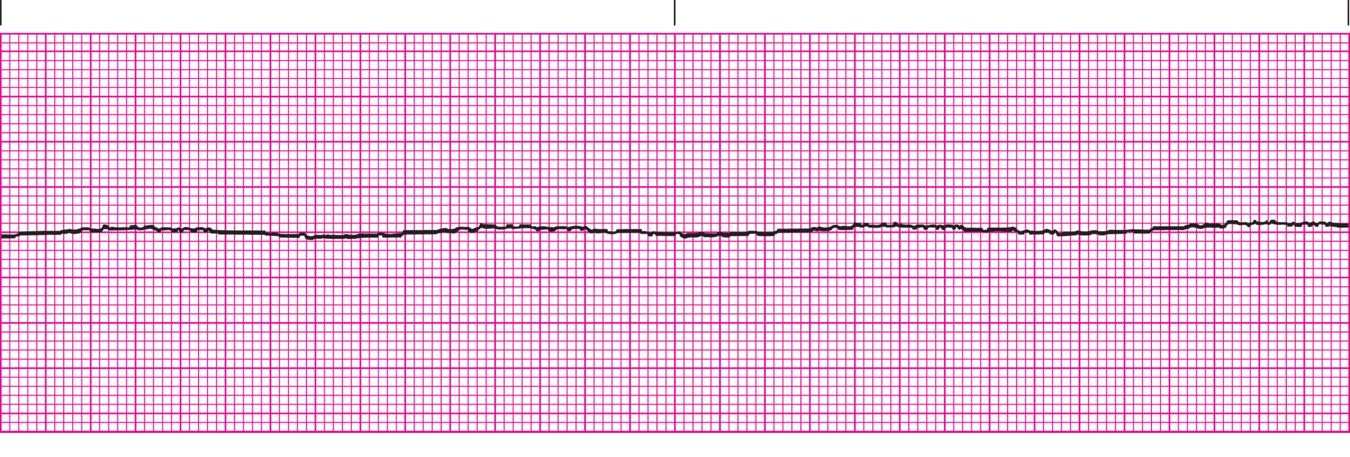
Asystole
Pulseless Electrical Activity
absence of a palpable pulse and myocardial muscle activity with presence of organized electrical activity on the cardiac monitor
What rhythm was formerly electromechanical dissociation, or EMD
Pulseless Electrical Activity
Causes PEA
Profound hypovolemia
Massive myocardial damage
Ventricular Rupture
PE
Acidosis
Cardiac Tamponade
Hypo/Hyperthermia
Drug OD
Hypo/Hyperkalemia
Tension Pneumo
What has shown assocaited to PVCs
Caffeine Intake
Stress
Giving what may cause PVCs to dissapear
O2
What is important to determine when assessing many ventricular rhythms
Perfusion status
What causes CO to compromise in V-tach
rapid heart rate, ventricles do not have time to empty and refill
The presence of fine V-fib indicates
The rhythm has been present for extended perioid