NR283- Exam 2 Review Questions with 100% correct answers -Chamberlain
1/167
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
168 Terms
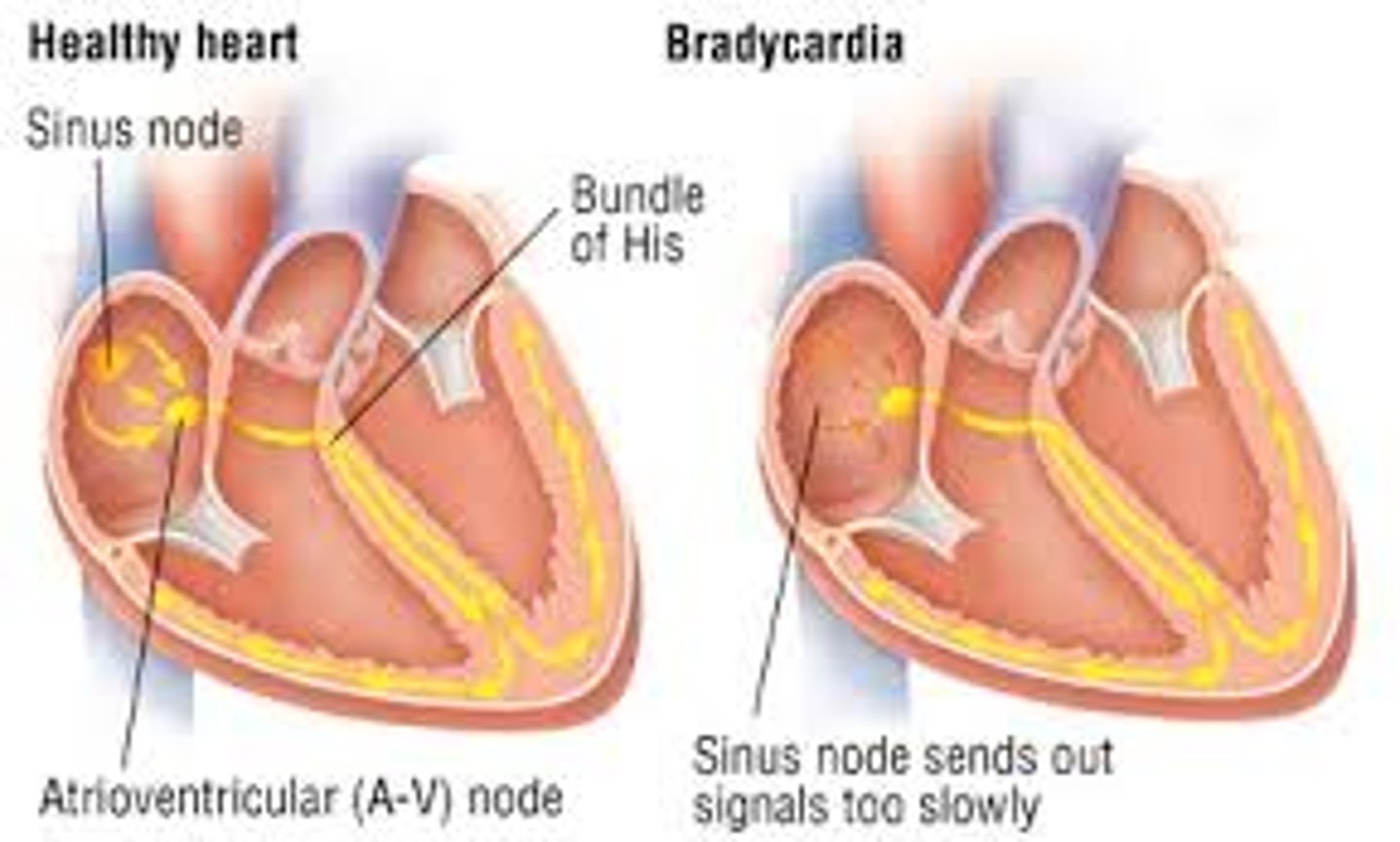
What is the primary function of the SA node in the heart?
A) To slow down the heart rate
B) To act as a gatekeeper for electrical signals
C) To initiate electrical impulses that set the rhythm and rate of the heart; "pacemaker" of the heart
D) To contract and pump blood to the ventricles
C) To initiate electrical impulses that set the rhythm and rate of the heart; "pacemaker" of the heart
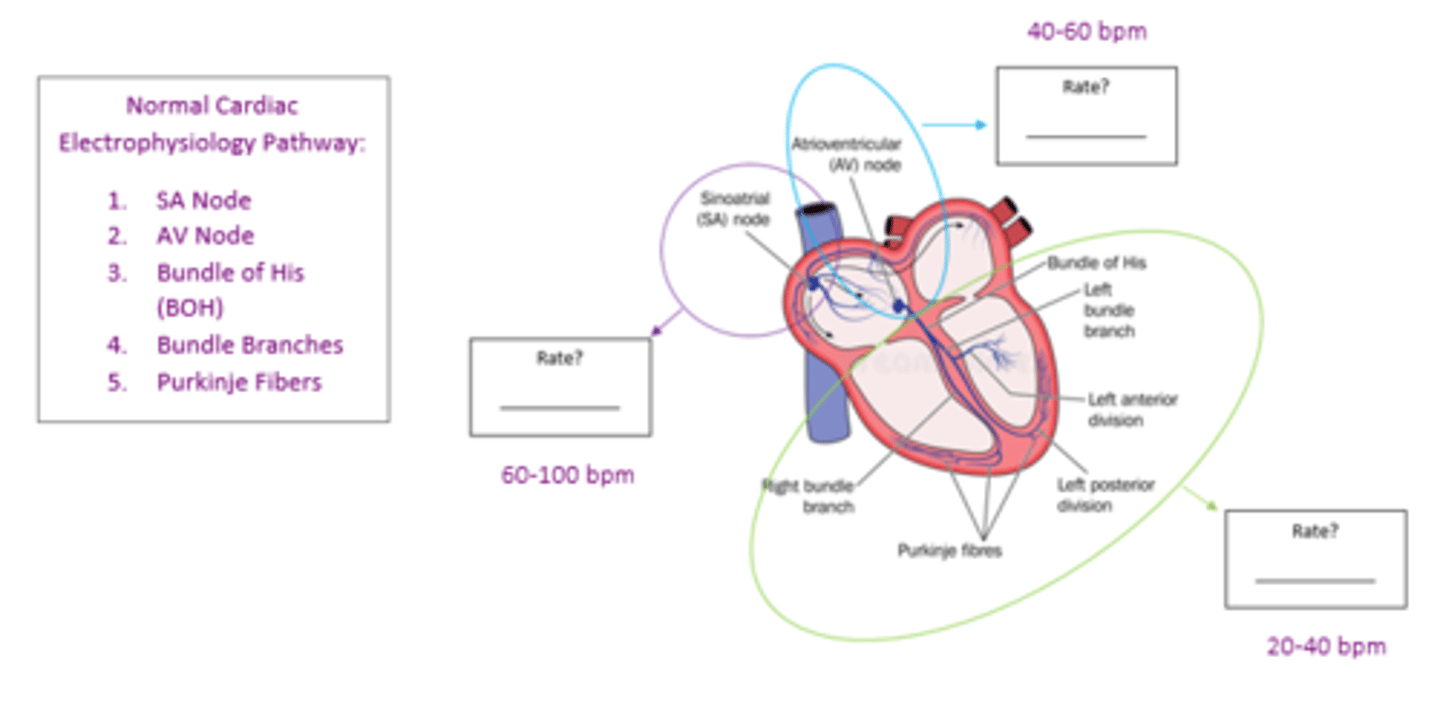
What is the role of the AV node in the cardiac conduction system?
A) To act as the primary pacemaker of the heart
B) To contract and pump blood into the ventricles
C) To slow the electrical signal before it enters the ventricles
D) To prevent the backflow of blood into the atria
C) To slow the electrical signal before it enters the ventricles

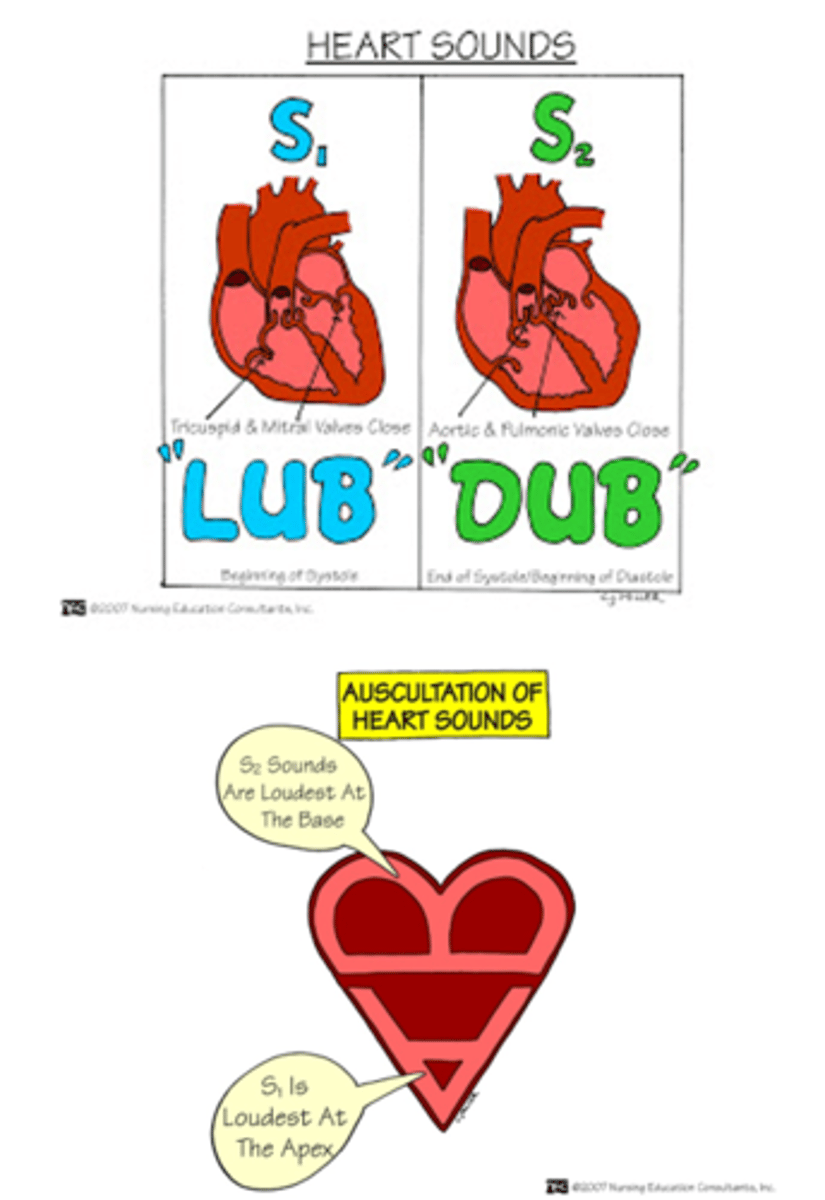
Which valves make up the S2 sound?
1. ________________________
2. ________________________
1. Aortic
2. Pulmonic
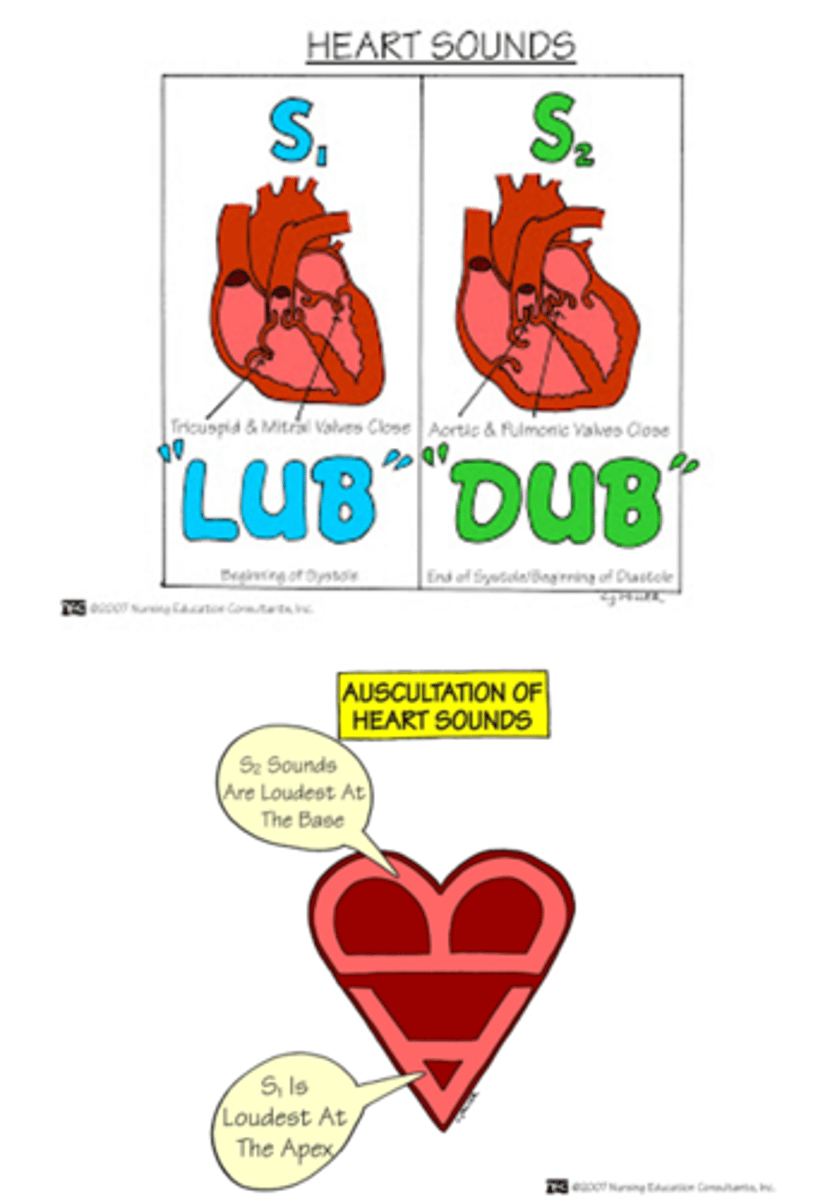
Which valves make up the S1 sound?
1. ________________________
2. ________________________
1. Bicuspid/mitral
2. Tricuspid
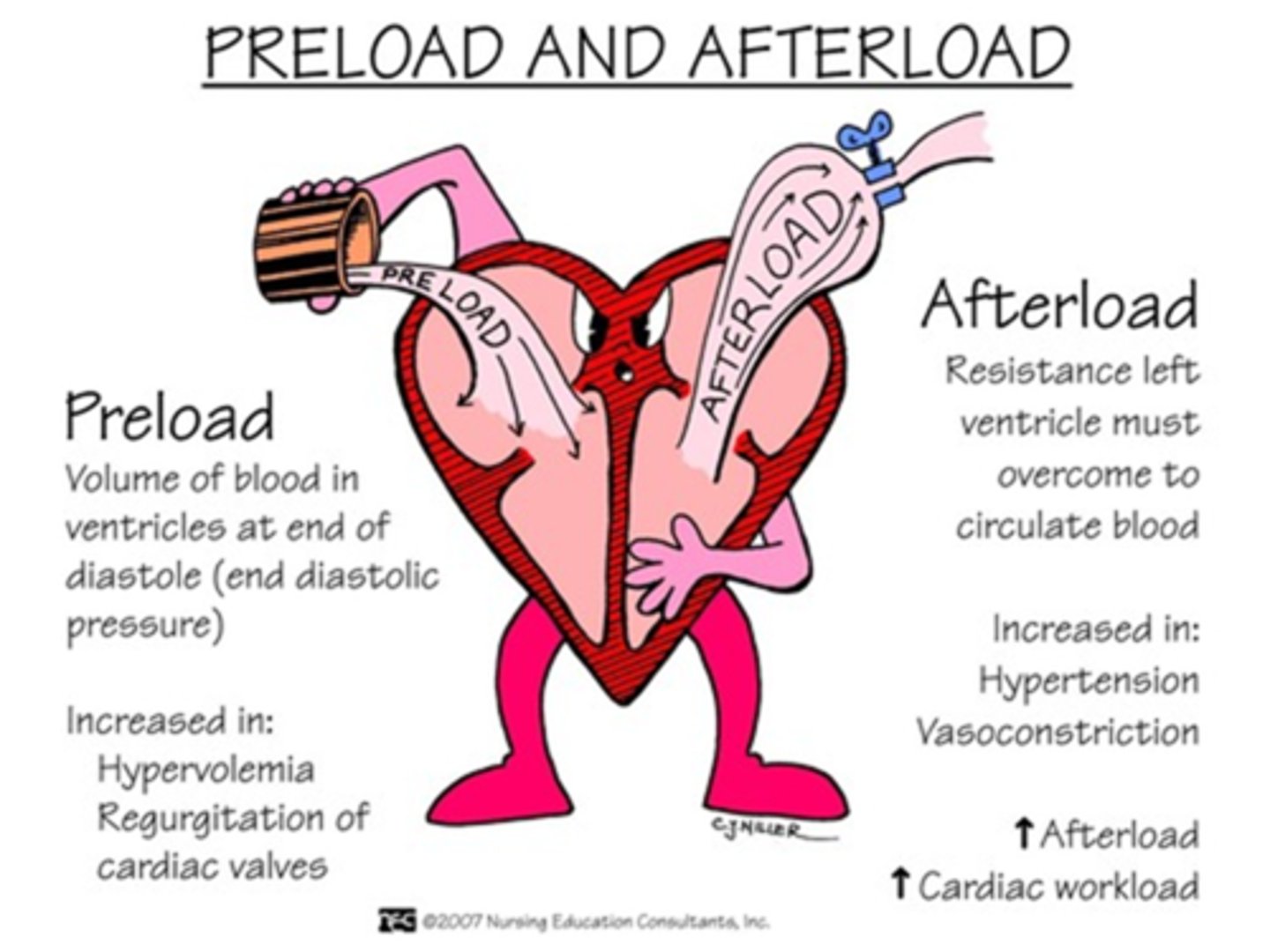
What is the term used to describe the filling of the ventricles with blood?
A) Afterload
B) Preload
C) Stroke volume
D) Cardiac output
B) Preload
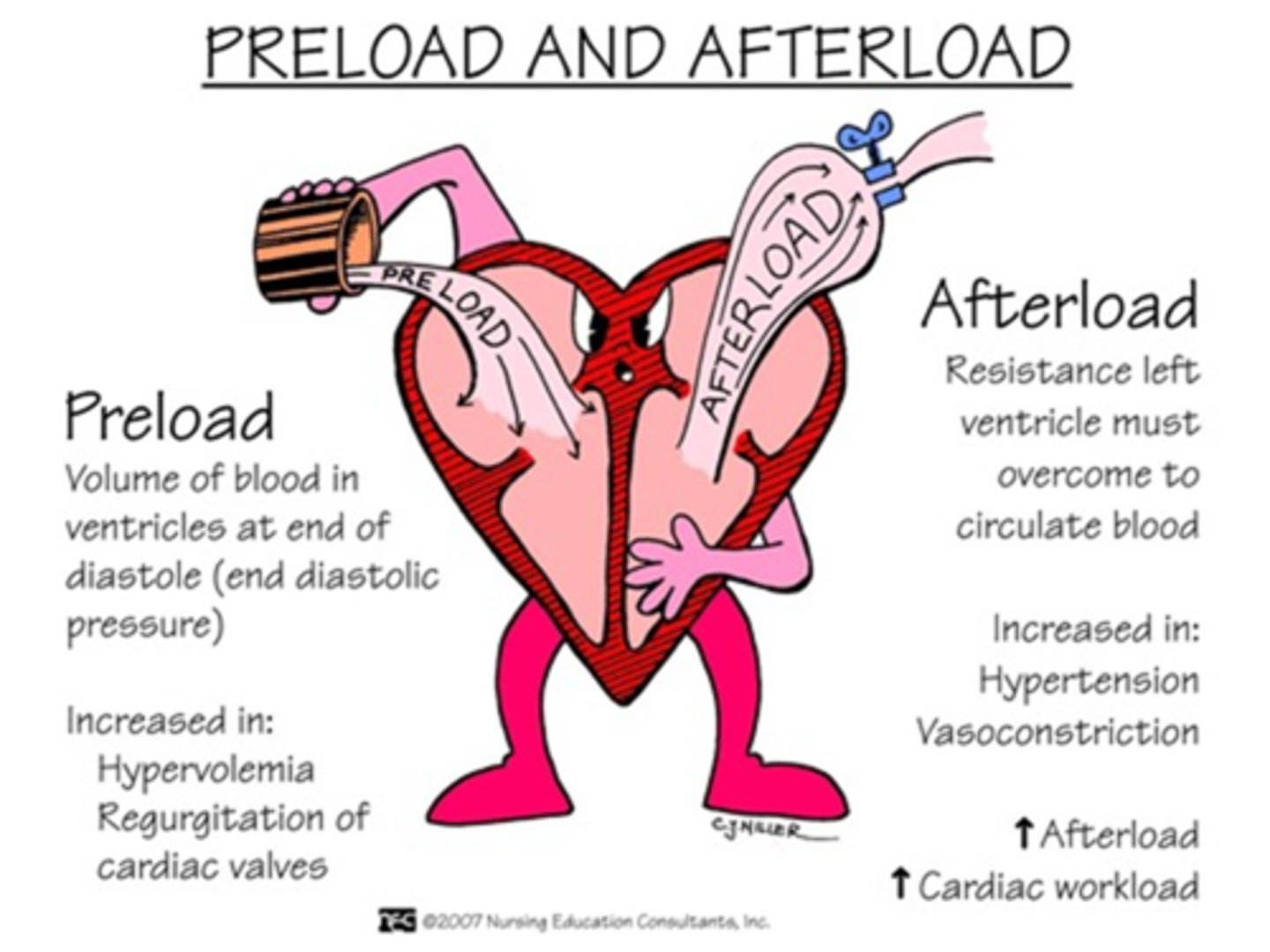
Afterload refers to:
A) The amount of pressure needed to pump blood out of the ventricles; the resistance the left ventricle must overcome to pump the blood into circulation
B) The amount of blood returning to the heart
C) The volume of blood filling the ventricles before contraction
D) The electrical impulses that set the heart rate
A) The amount of pressure needed to pump blood out of the ventricles; the resistance the left ventricle must overcome to pump the blood into circulation
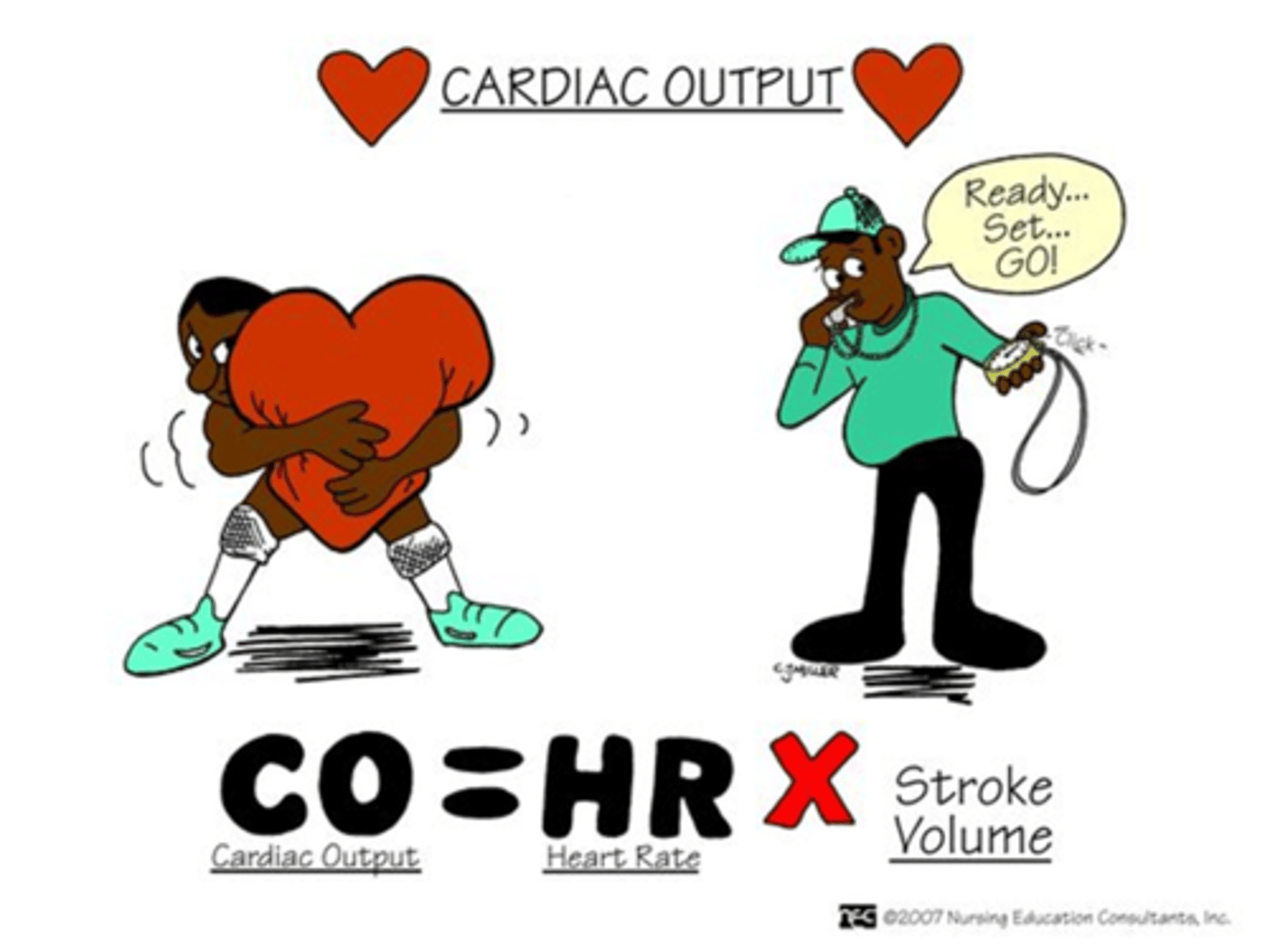
Which formula correctly represents cardiac output (CO)?
A) CO = HR + SV (Stroke Volume)
B) CO = HR - SV (Stroke Volume)
C) CO = HR x SV (Stroke Volume)
D) CO = HR / SV (Stroke Volume)
C) CO = HR x SV (Stroke Volume)
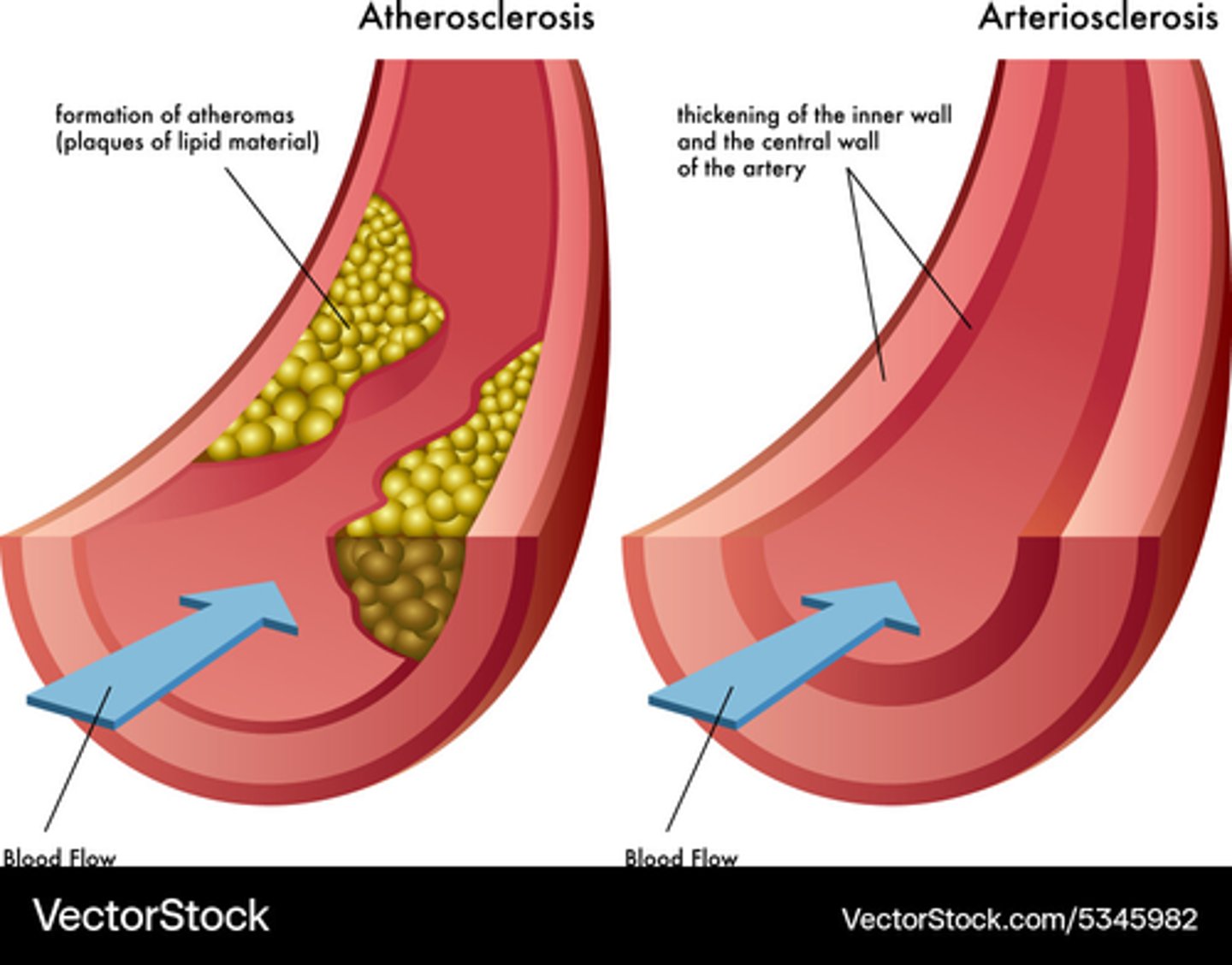
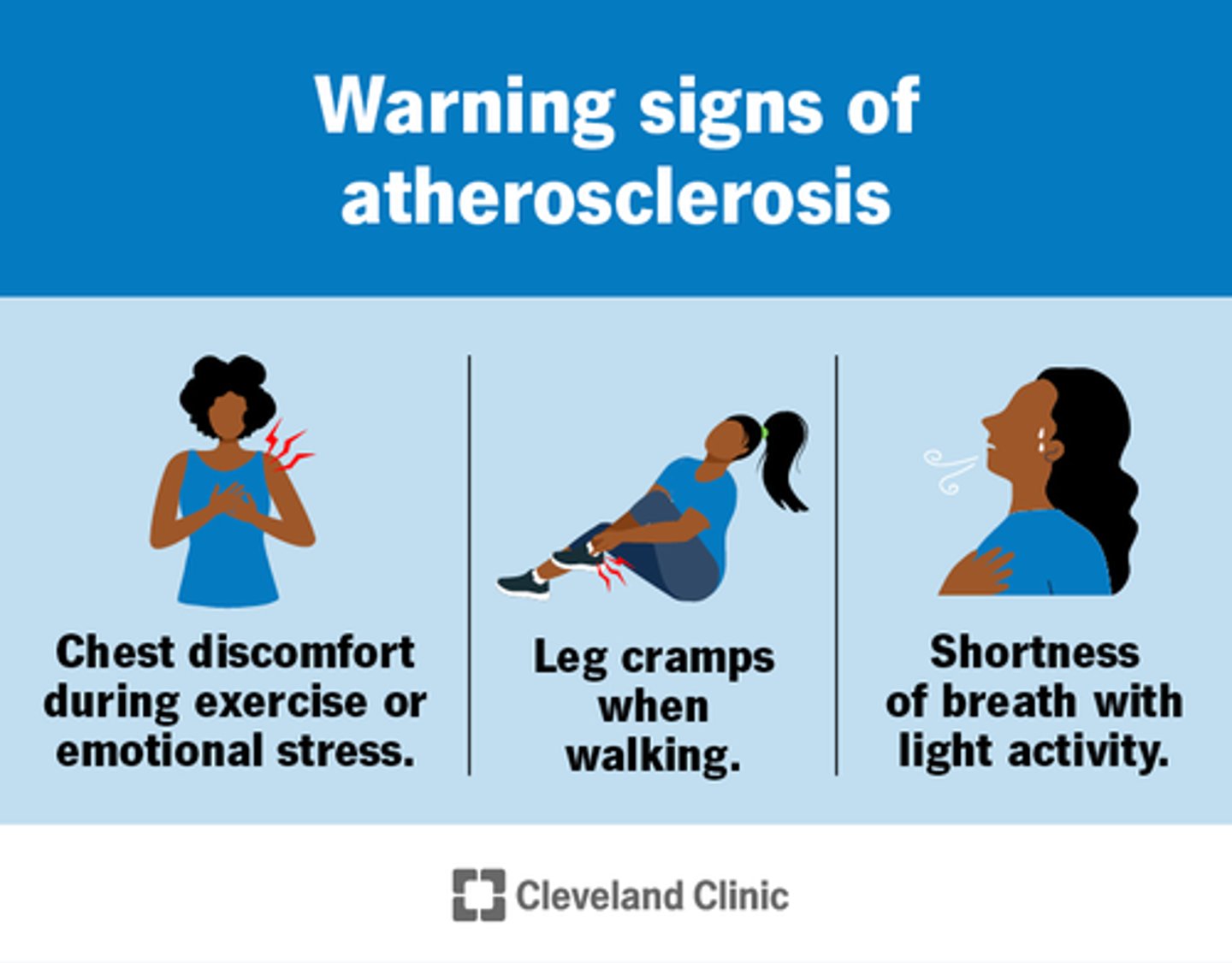
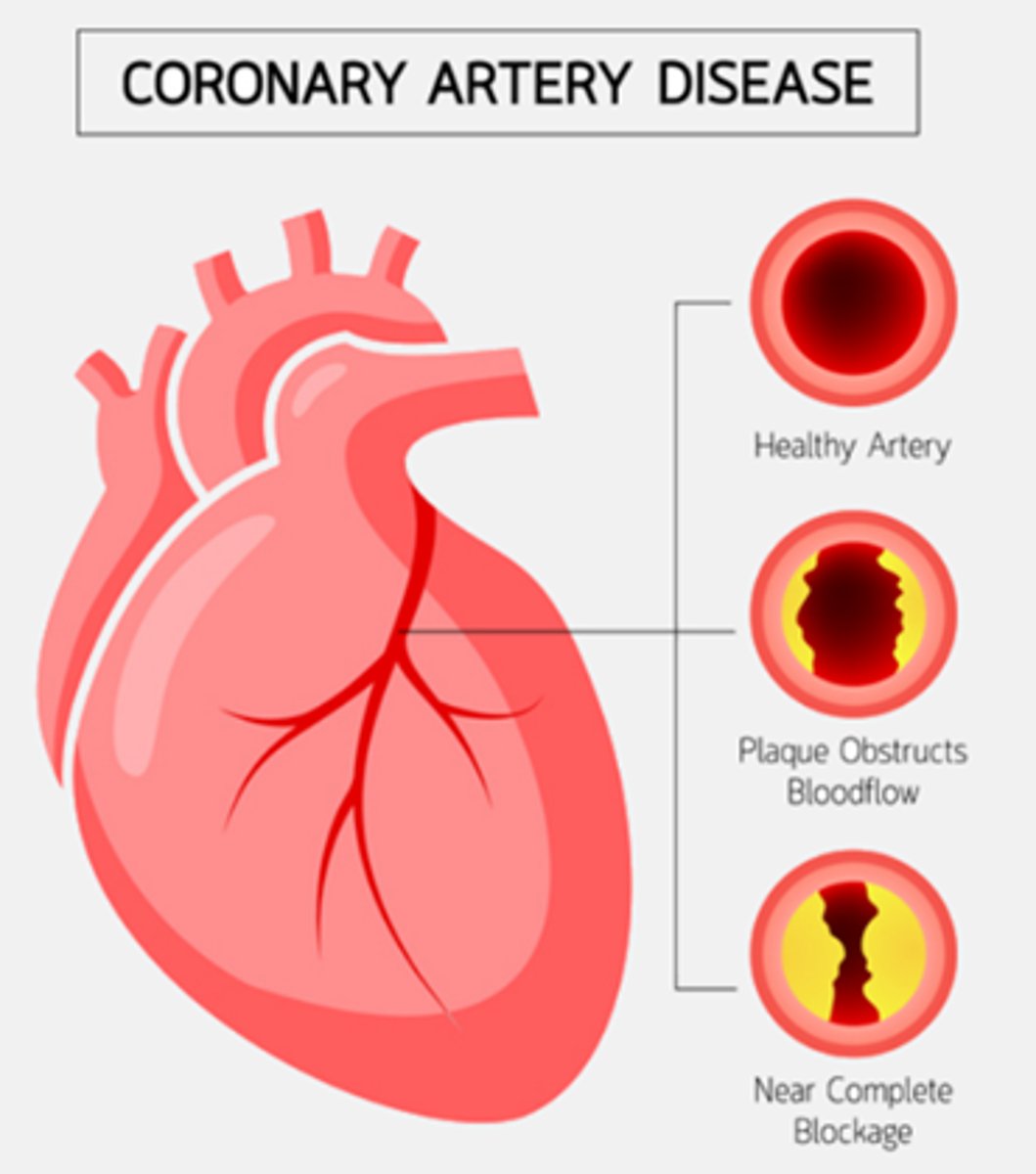
What is the primary difference between atherosclerosis and arteriosclerosis?
A) Atherosclerosis refers to the hardening of arteries, while arteriosclerosis involves plaque buildup.
B) Atherosclerosis involves plaque buildup that obstructs blood flow, while arteriosclerosis refers to the hardening of arteries.
C) Atherosclerosis is a type of arteriosclerosis that affects the veins, while arteriosclerosis affects the arteries.
D) Atherosclerosis results from high blood pressure, while arteriosclerosis results from high cholesterol levels.
B) Atherosclerosis involves plaque buildup that obstructs blood flow, while arteriosclerosis refers to the hardening of arteries.
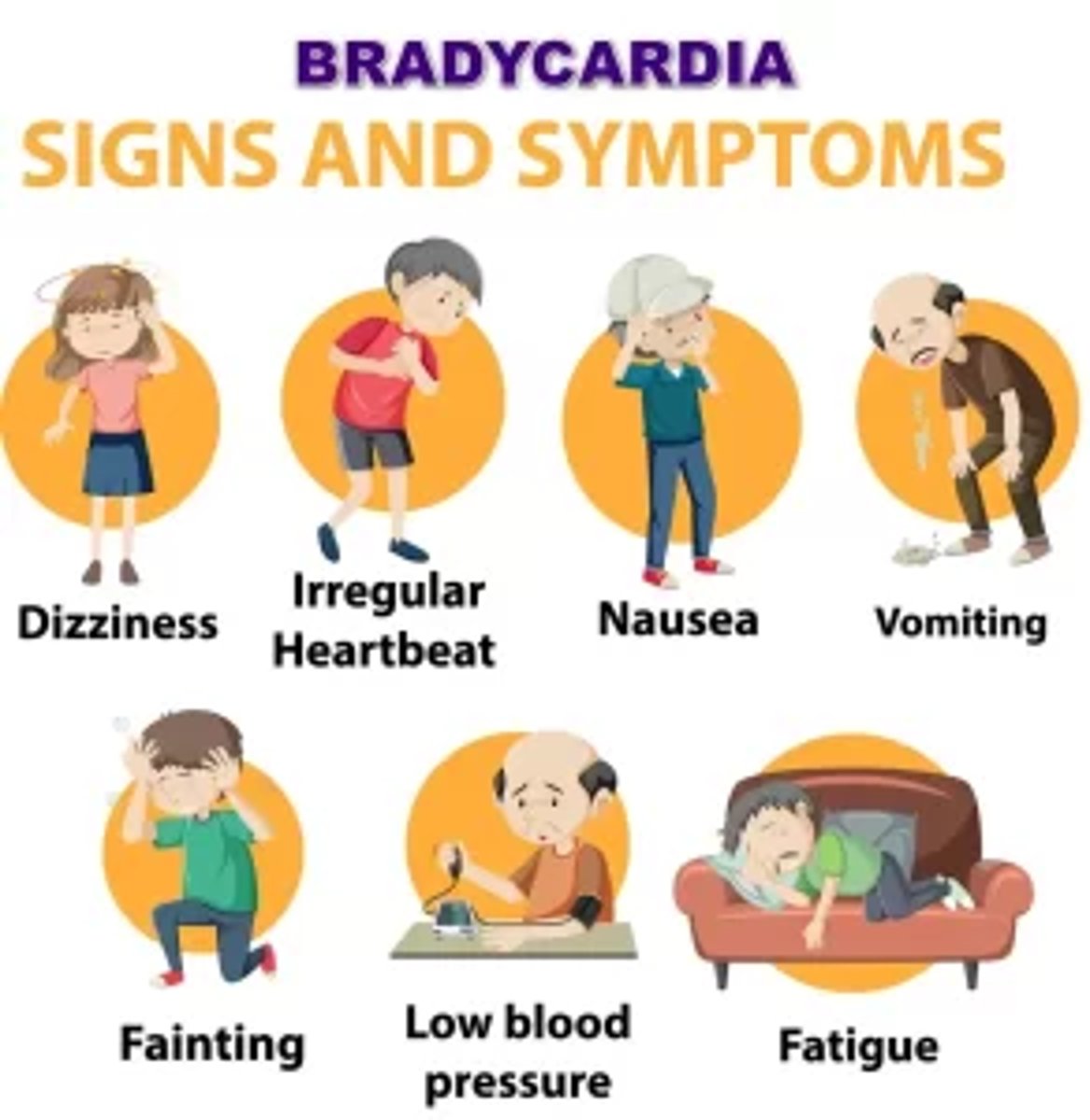
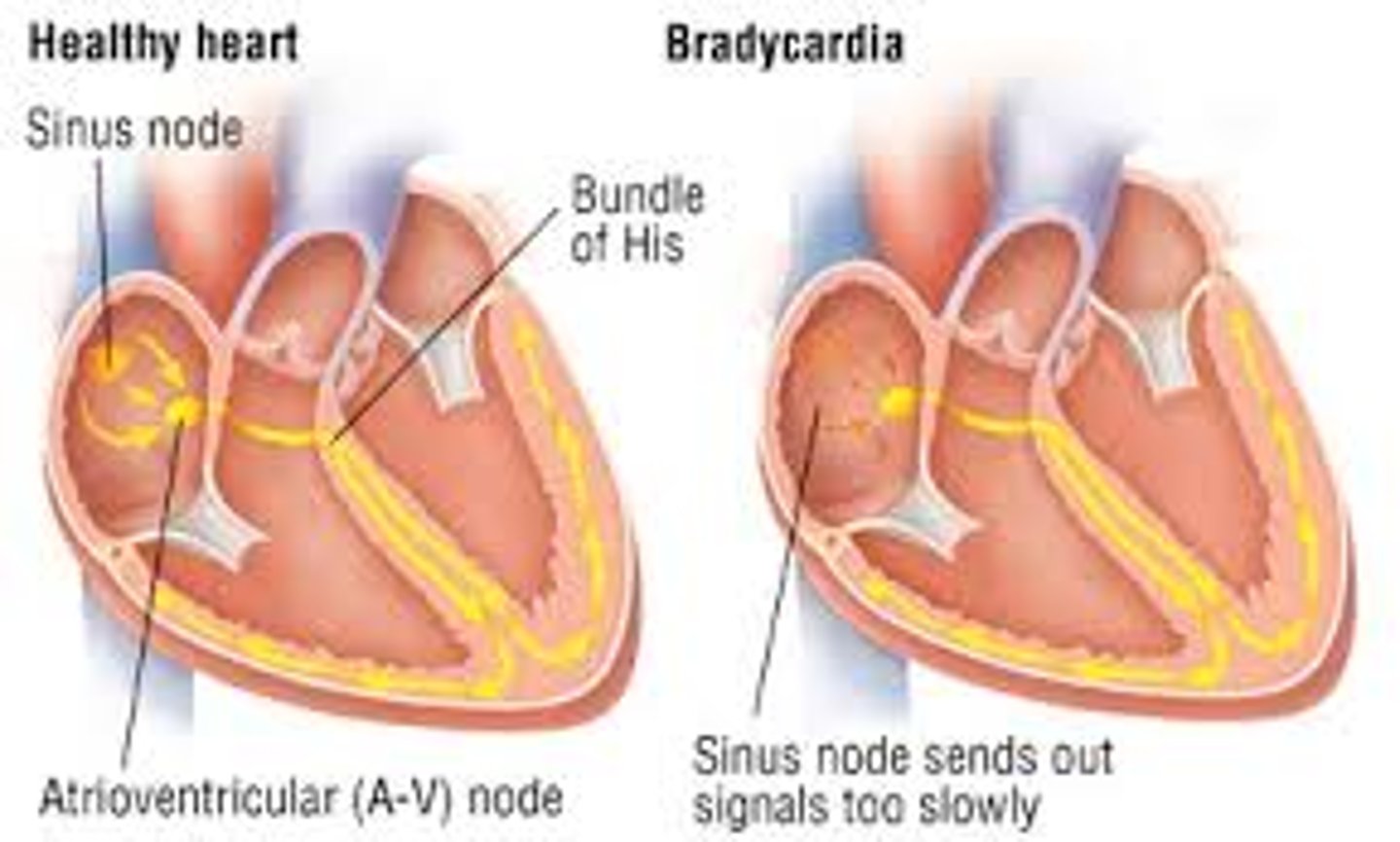
Which of the following describes bradycardia?
A) HR > 100bpm
B) HR < 60bpm
C) Irregular heart contractions
D) Normal heart rhythm
B) HR < 60bpm
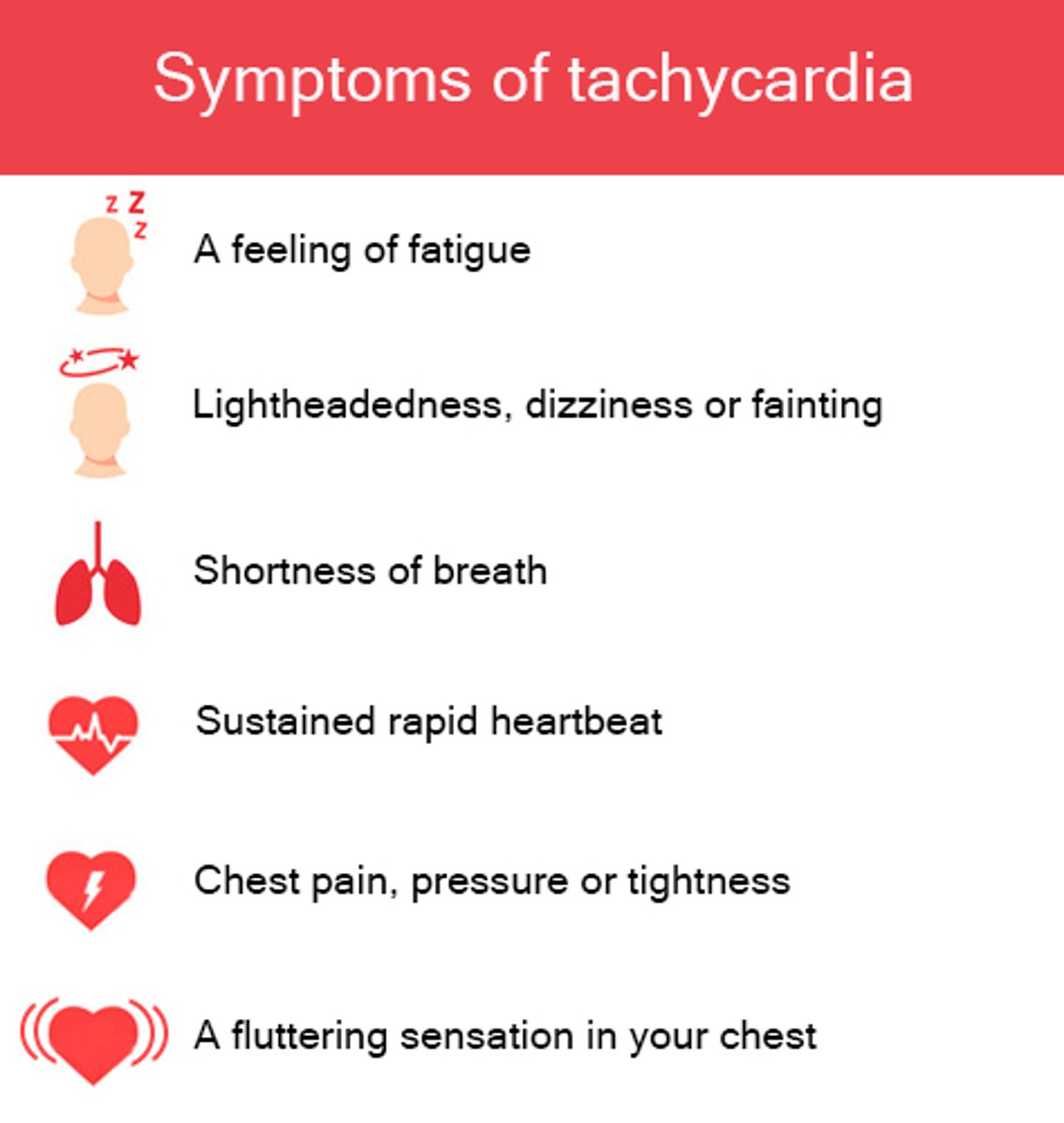
Which of the following best describes tachycardia?
A) HR > 100bpm
B) HR < 60bpm
C) Irregular heart contractions
D) Decreased cardiac output
A) HR > 100bpm
Which of the following are common signs and symptoms of bradycardia (HR < 60 bpm)?
A) Palpitations, high blood pressure, sweating
B) Weakness, fatigue, low blood pressure, change in LOC
C) Chest pain, shortness of breath, high heart rate
D) Dizziness, nausea, high blood pressure
B) Weakness, fatigue, low blood pressure, change in LOC
Which of the following are common signs and symptoms of atherosclerosis?
A) Chest pain, shortness of breath, high heart rate
B) Fatigue, weakness, pain in legs, absent/weak pulses
C) Dizziness, nausea, high blood pressure
D) Palpitations, sweating, high blood pressure
B) Fatigue, weakness, pain in legs, absent/weak pulses
What happens when the SA node fires too quickly?
A) It leads to a condition called bradycardia, where the heart beats slower than normal.
B) It results in an irregular heart rhythm known as atrial fibrillation.
C) It leads to a rapid heart rate called tachycardia, where the heart beats faster than normal.
D) It causes the heart to stop beating.
C) It leads to a rapid heart rate called tachycardia, where the heart beats faster than normal.

What happens when the SA node fires too slowly?
A) It leads to a condition called tachycardia, where the heart beats faster than normal.
B) It results in an irregular heart rhythm known as atrial fibrillation.
C) It leads to a slow heart rate called bradycardia, where the heart beats slower than normal.
D) It causes the heart to stop beating.
C) It leads to a slow heart rate called bradycardia, where the heart beats slower than normal.
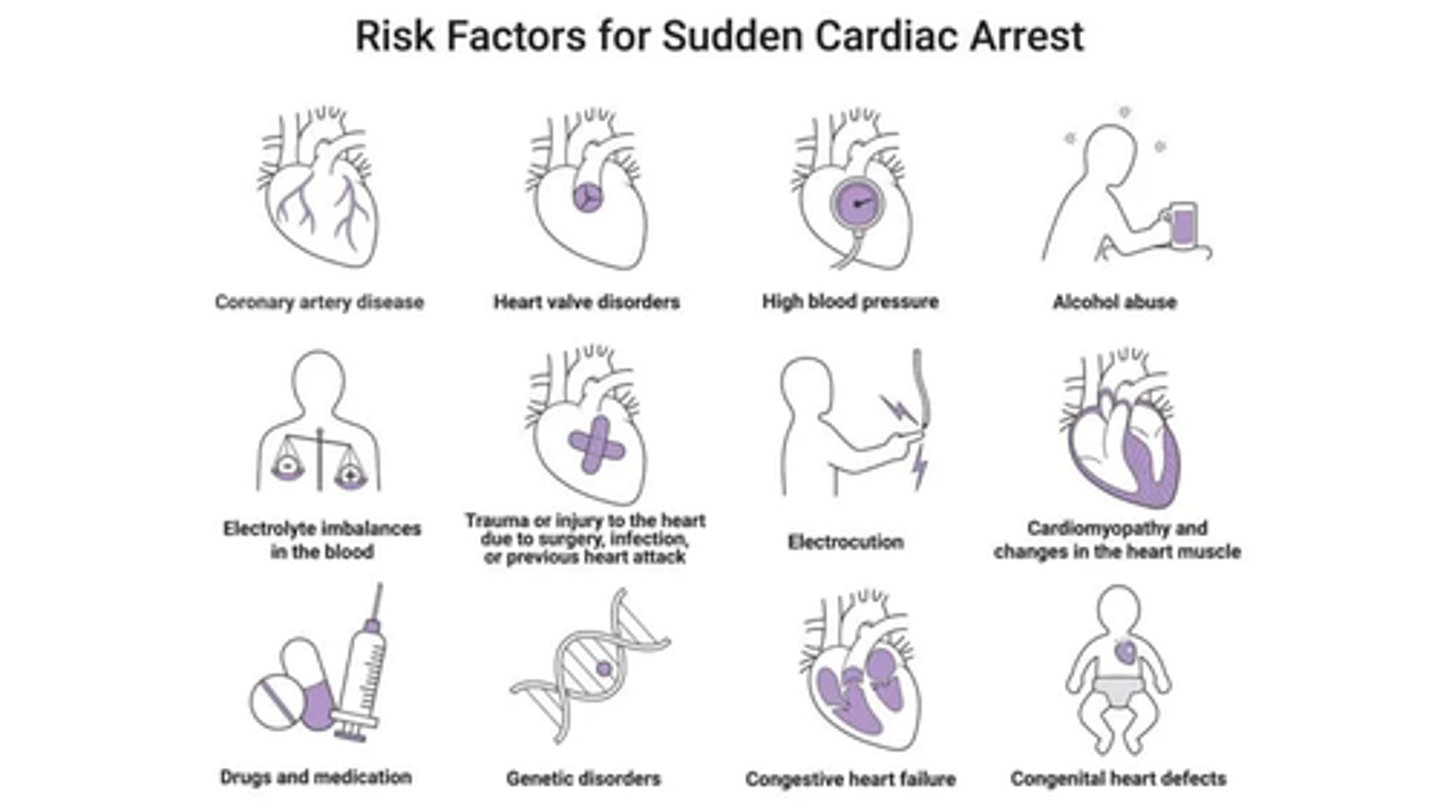
Which of the following are considered deadly cardiac dysrhythmias/arrhythmias?
A) Atrial Fibrillation, Ventricular Tachycardia, Asystole, Sinus Bradycardia
B) Asystole, Ventricular Fibrillation, Ventricular Tachycardia, Pulseless Electrical Activity (PEA)
C) Sinus Tachycardia, Atrial Flutter, Ventricular Tachycardia, Pulseless Electrical Activity (PEA)
D) Atrial Fibrillation, Pulseless Electrical Activity (PEA), Asystole, Sinus Tachycardia
B) Asystole, Ventricular Fibrillation, Ventricular Tachycardia, Pulseless Electrical Activity (PEA)
Which of the following can cause cardiac dysrhythmias/arrhythmias?
A) Caffeine, electrolyte imbalances (such as Potassium), and drugs (such as cocaine)
B) Regular exercise, Balanced diet, and Hydration
C) Proper sleep, Low sodium intake, and Regular medical check-ups
D) Stress management, Adequate vitamin intake, and Mild alcohol consumption
A) Caffeine, electrolyte imbalances (such as Potassium), and drugs (such as cocaine)
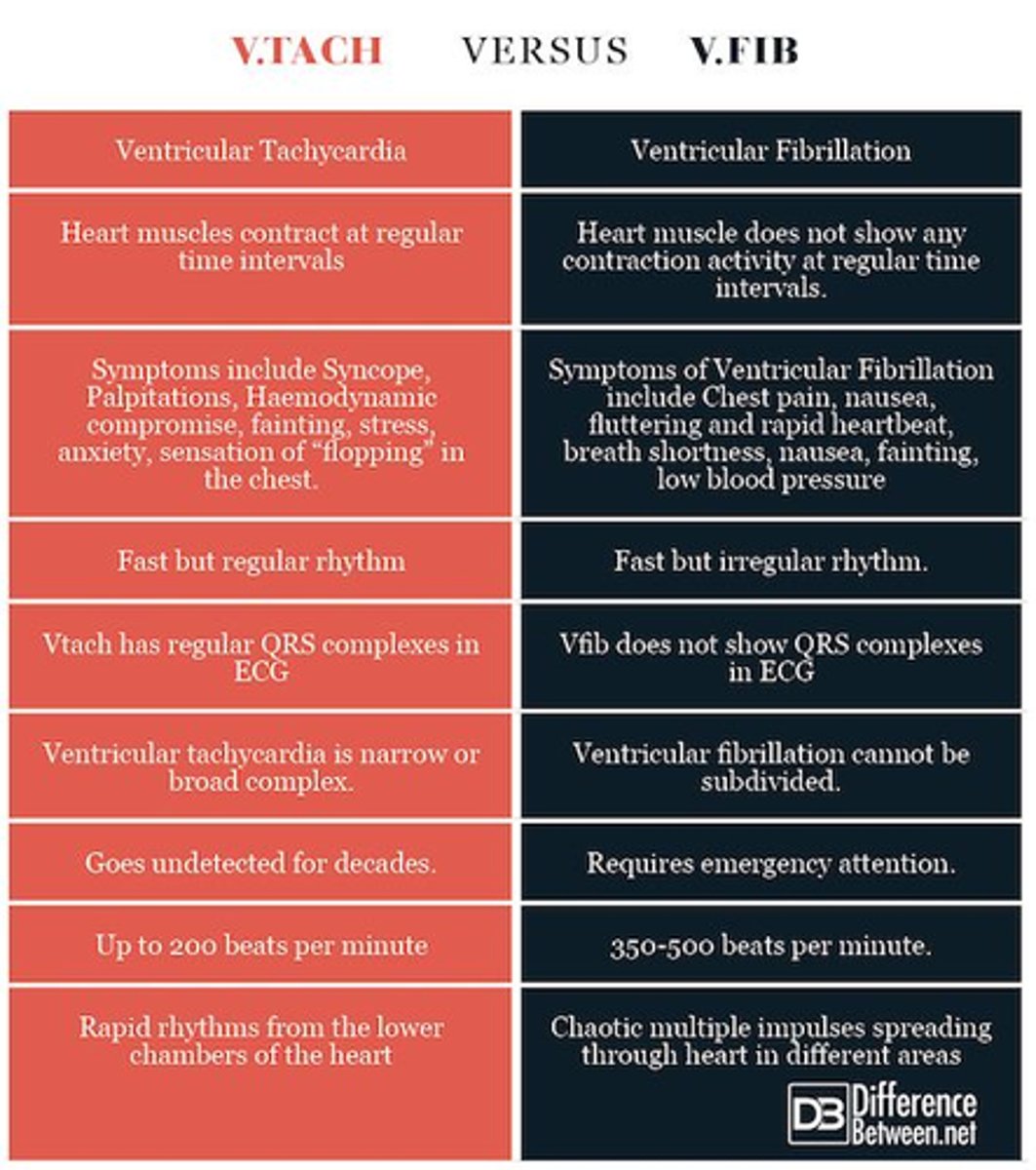
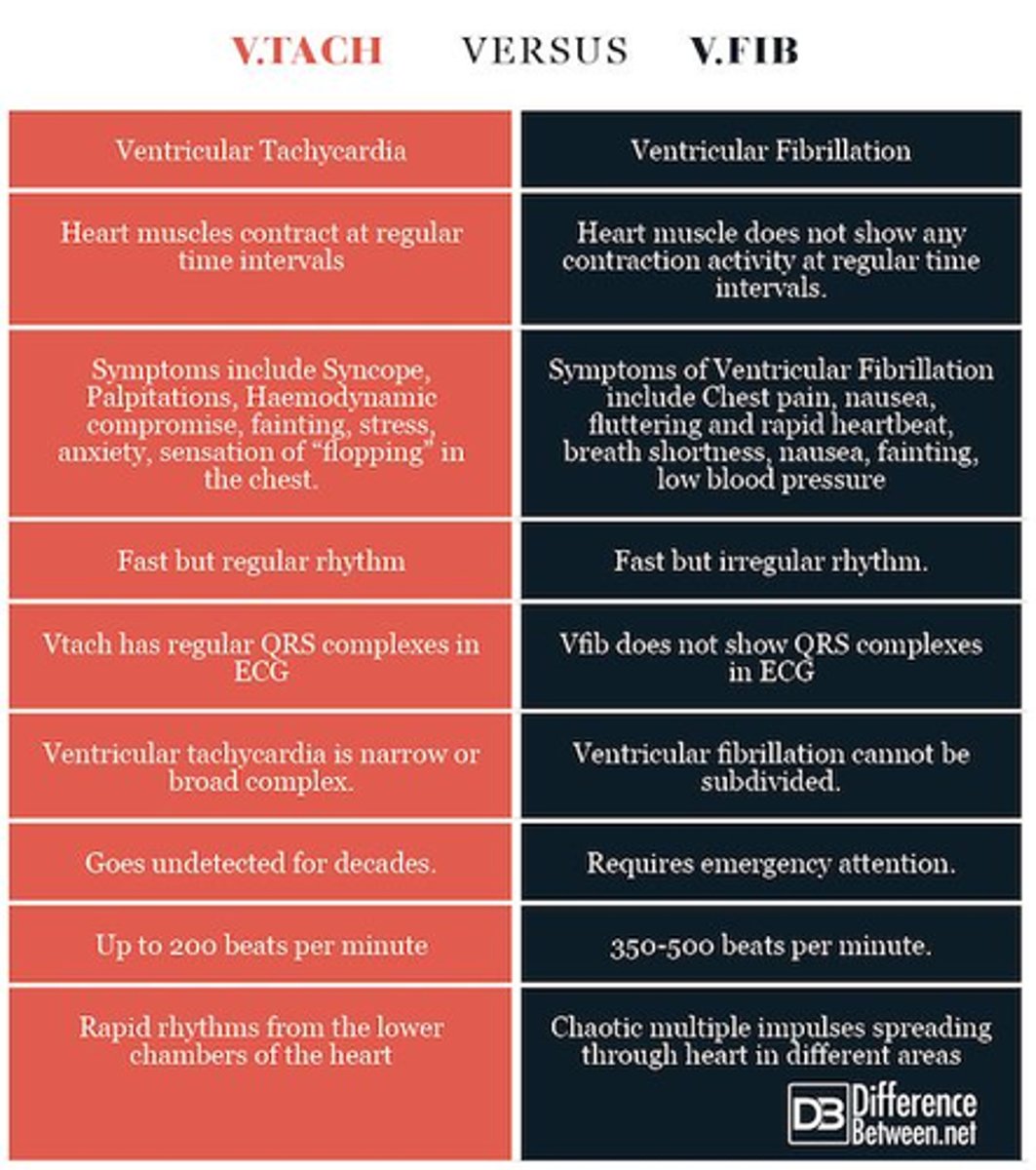
Which of the following are common signs and symptoms of ventricular tachycardia (V-tach) and ventricular fibrillation (V-fib)?
A) Slow heart rate, fatigue, and high blood pressure
B) Rapid heart rate, chest pain, dizziness/lightheadedness, and loss of consciousness (syncope)
C) Regular heart rhythm, mild chest discomfort, and shortness of breath
D) Normal heart rate, palpitations, and slight fatigue
B) Rapid heart rate, chest pain, dizziness/lightheadedness, and loss of consciousness (syncope)
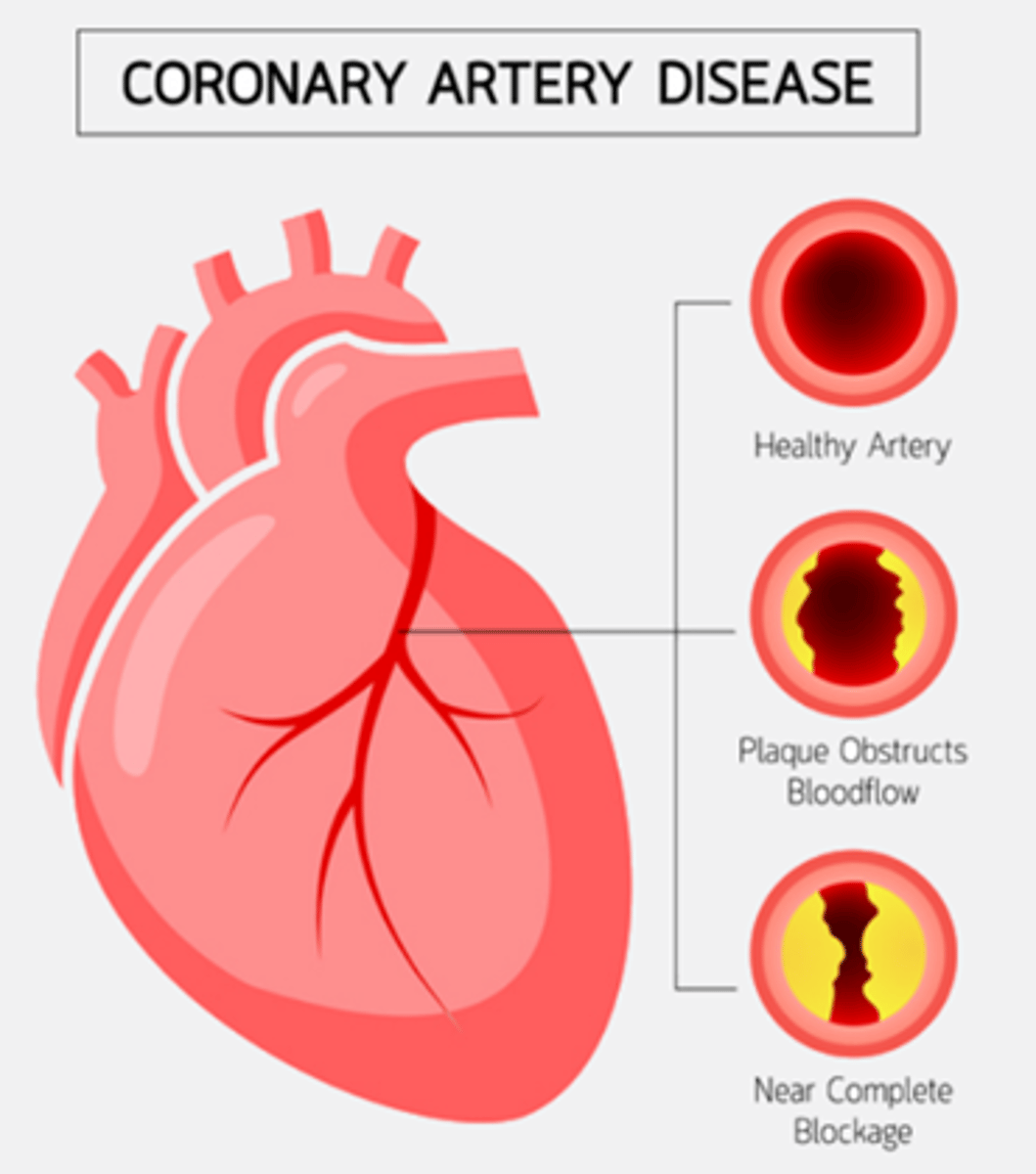
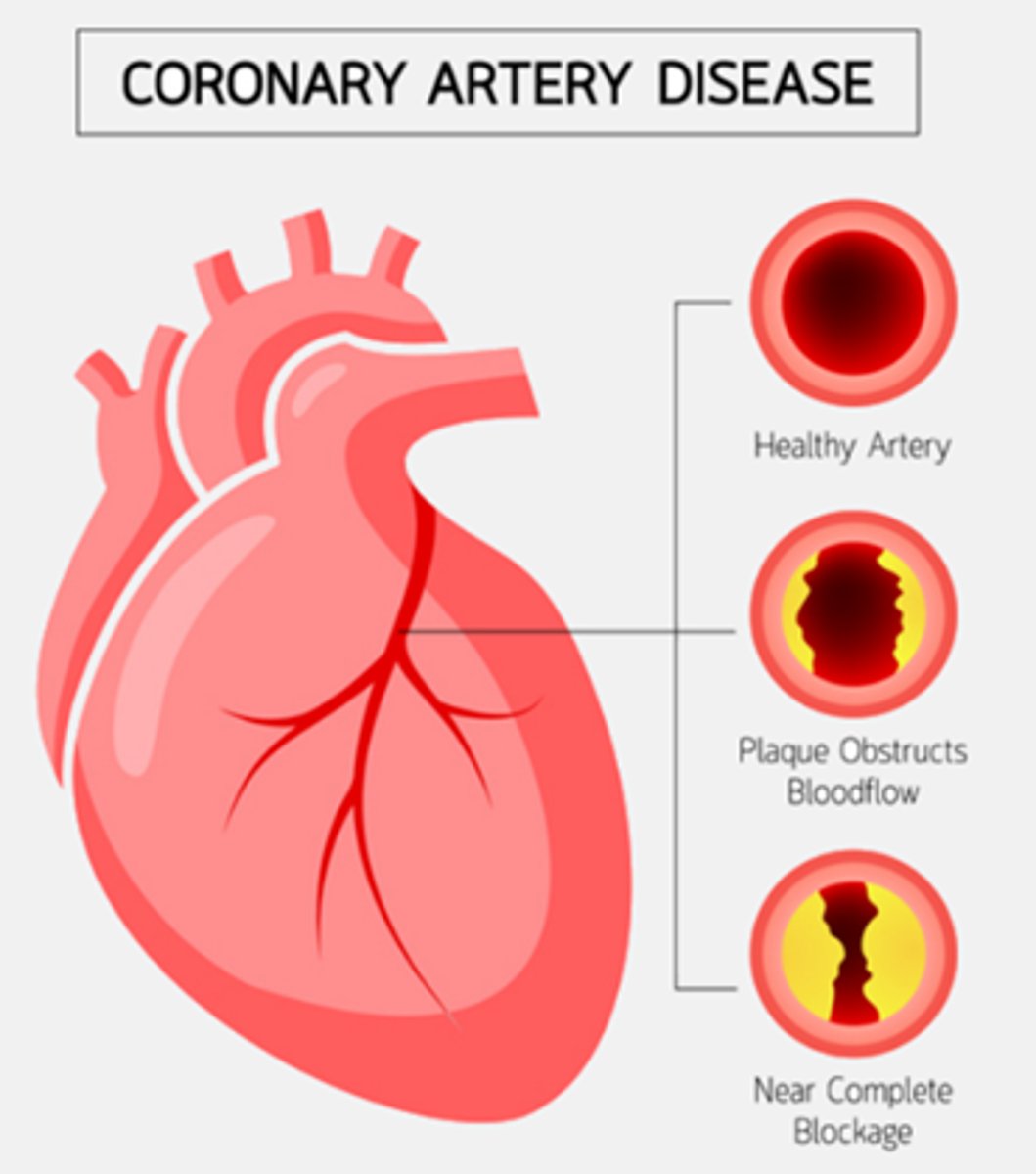
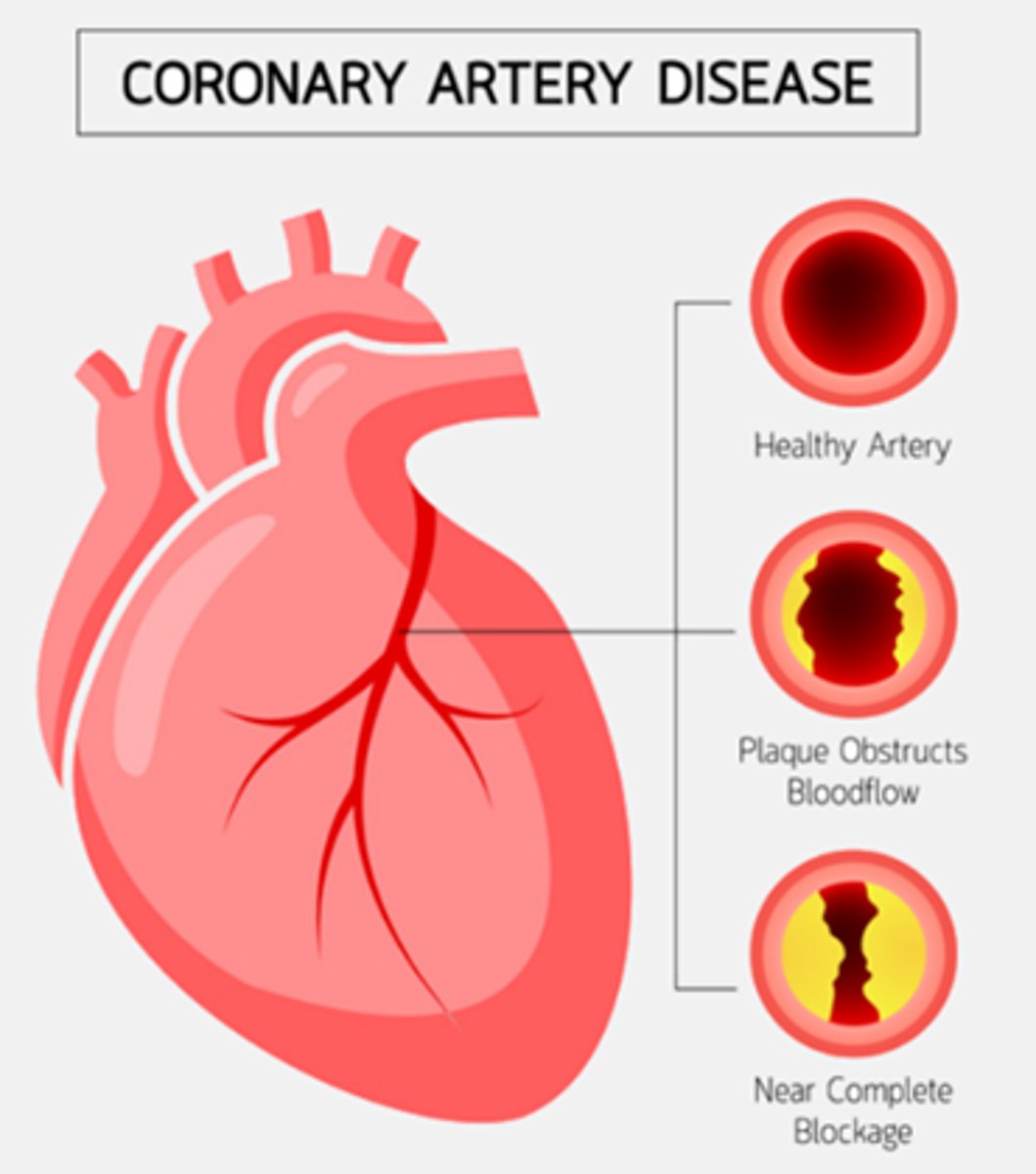
What is the pathophysiology of coronary artery disease (CAD)?
A) Increasing blood flow to the myocardial tissue due to atherosclerotic plaque deposits in the coronary artery
B) Decreasing blood flow (and oxygen as a result) to the myocardial tissue due to atherosclerotic plaque deposits in the coronary artery
C) Preventing endothelial injury in the coronary artery
D) Reducing heart rate due to atherosclerotic plaque deposits
B) Decreasing blood flow (and oxygen as a result) to the myocardial tissue due to atherosclerotic plaque deposits in the coronary artery
Which of the following diagnostics are used to evaluate coronary artery disease (CAD)?
A) Cardiac angiogram, Complete blood count (CBC), Blood glucose levels
B) Cardiac angiogram, Total cholesterol, LDL, vLDL, HDL, Triglycerides, echocardiogram (uses ultrasound waves to create picture of the heart)
C) Electrocardiogram (ECG), Blood pressure measurement, Urinalysis
D) Echocardiogram, Liver function tests, Bone density scan
B) Cardiac angiogram, Total cholesterol, LDL, vLDL, HDL, Triglycerides, echocardiogram (uses ultrasound waves to create a picture of the heart)
Which of the following are risk factors for coronary artery disease (CAD)?
A) Young age, Low blood pressure, Active lifestyle, Low triglycerides
B) Age, Hypertension (HTN), Genetics, Tobacco use, Diabetes, Obesity, Sedentary lifestyle, Hypercholesterolemia, High triglycerides, Metabolic syndrome, Stress, Illicit drug use (cocaine)
C) Proper diet, Regular exercise, Low stress, Normal cholesterol levels
D) High vitamin intake, Moderate alcohol consumption, Low sugar intake, Active lifestyleterm-45
B) Age, Hypertension (HTN), Genetics, Tobacco use, Diabetes, Obesity, Sedentary lifestyle, Hypercholesterolemia, High triglycerides, Metabolic syndrome, Stress, Illicit drug use (cocaine)
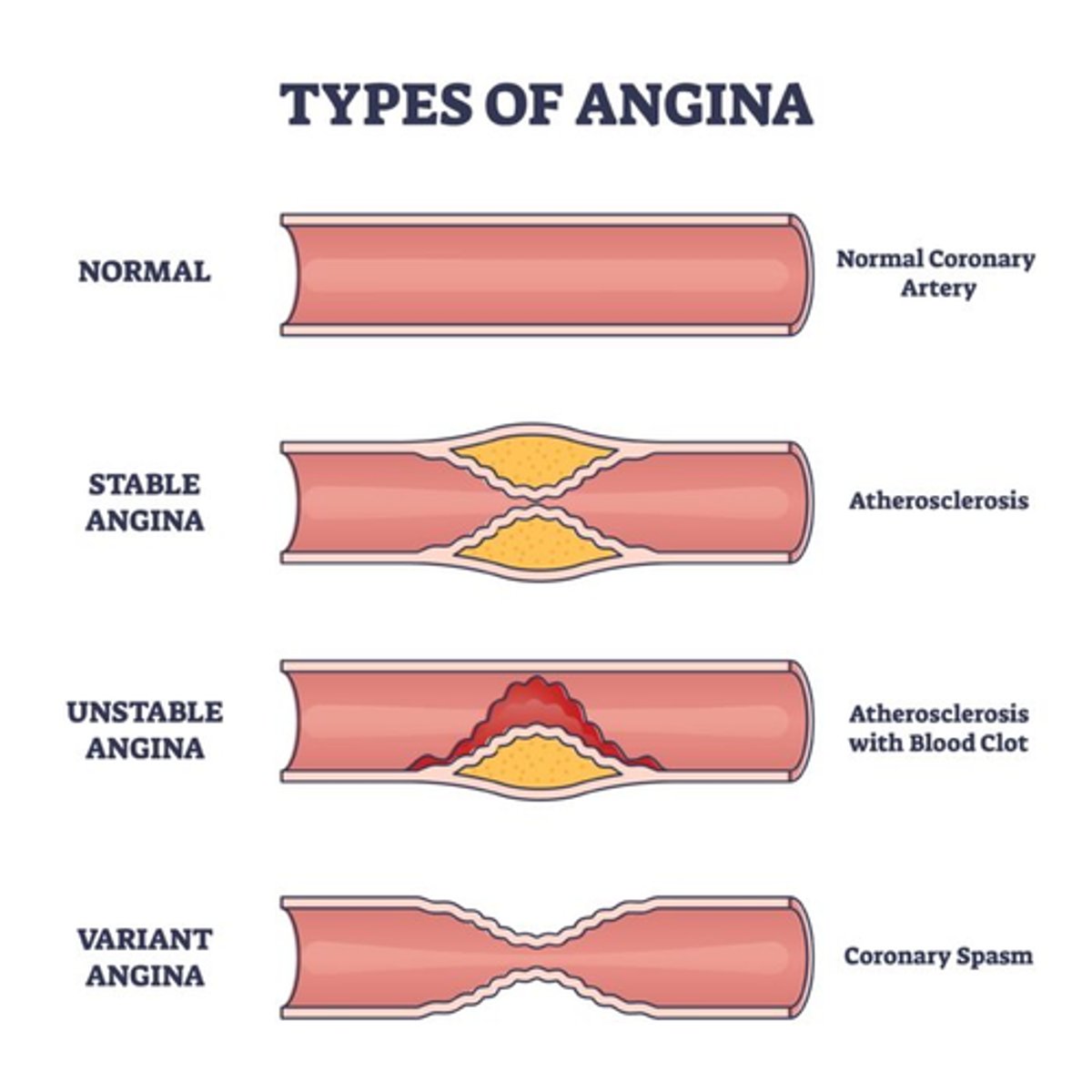
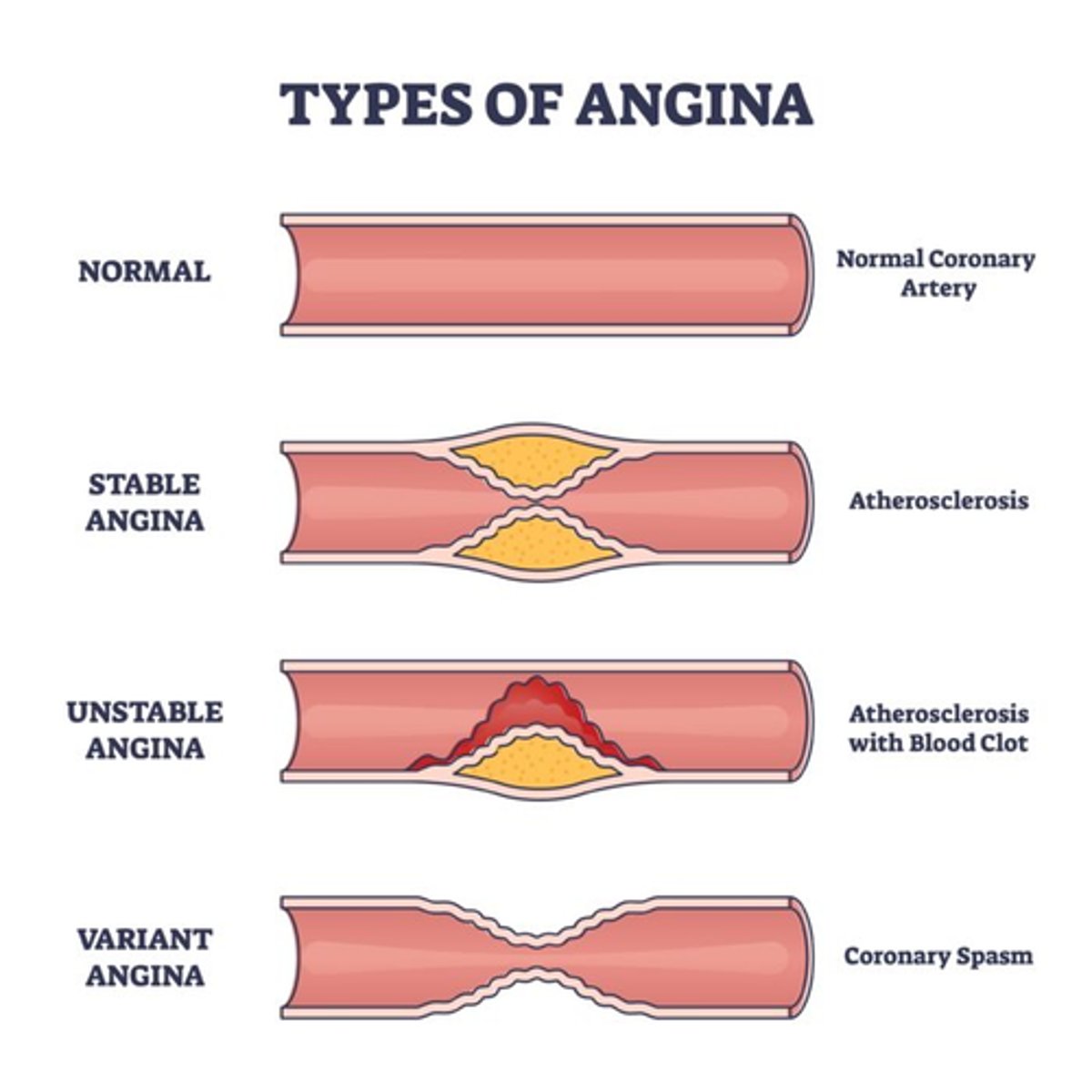
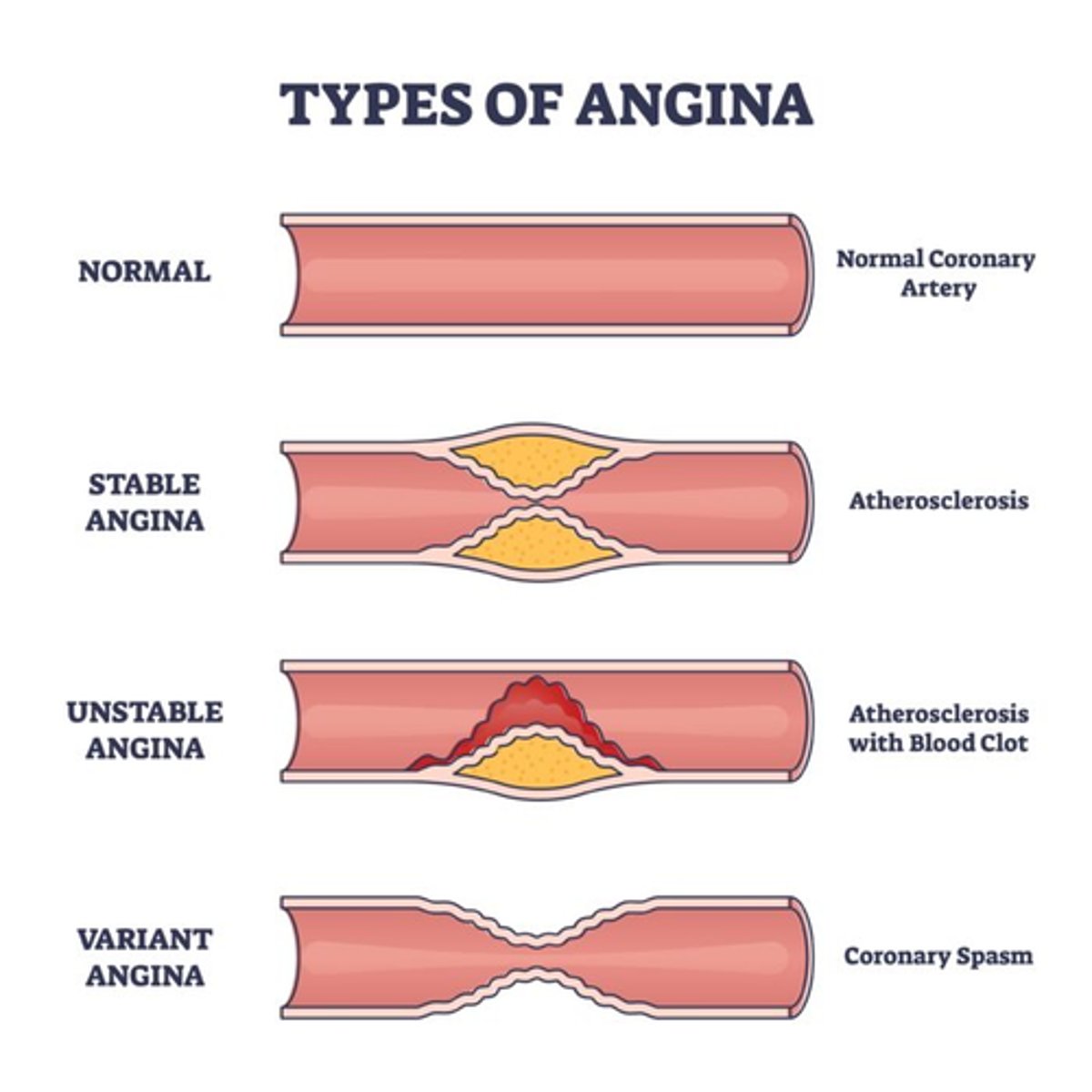
What is the definition of angina?
A) A chronic inflammatory condition affecting the joints
B) A sudden, sharp pain in the lower abdomen
C) Chest pain or discomfort due to reduced blood flow to the heart muscle
D) A severe headache accompanied by visual disturbances
C) Chest pain or discomfort due to reduced blood flow to the heart muscle

What are the characteristics of chronic stable angina?
A) Unpredictable pain that occurs at rest and is not relieved by medication
B) Episodic chest pain provoked by exertion or stress, occurring intermittently over a long period of time (predictable)
C) Continuous pain that does not change with rest or medication
D) Sudden sharp pain that occurs randomly and is relieved by physical activity
B) Episodic chest pain provoked by exertion or stress, occurring intermittently over a long period of time (predictable)
What is the underlying cause and relief mechanism for chronic stable angina?
A) Myocardial ischemia caused by O2 supply/demand mismatch, relieved by rest or nitroglycerin (NTG)
B) Myocardial infarction caused by complete blockage of blood flow, relieved by physical activity
C) Pulmonary embolism caused by a blood clot in the lung, relieved by deep breathing exercises
D) Heart failure caused by poor heart pumping, relieved by diuretics
A) Myocardial ischemia caused by O2 supply/demand mismatch, relieved by rest or nitroglycerin (NTG)
(like if you're gardening in the heat and your chest hurts, it can be relieved by taking NTG or rest)
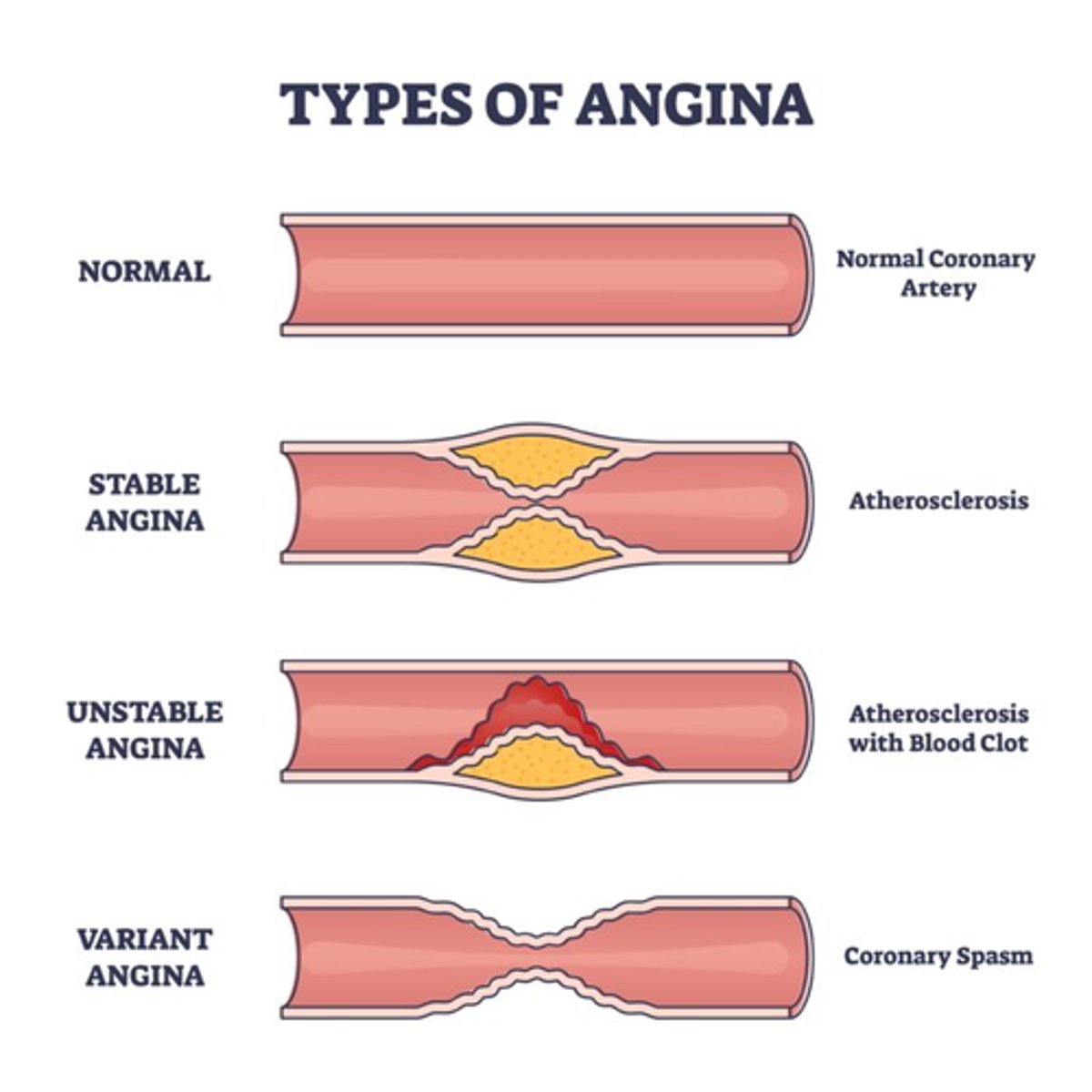
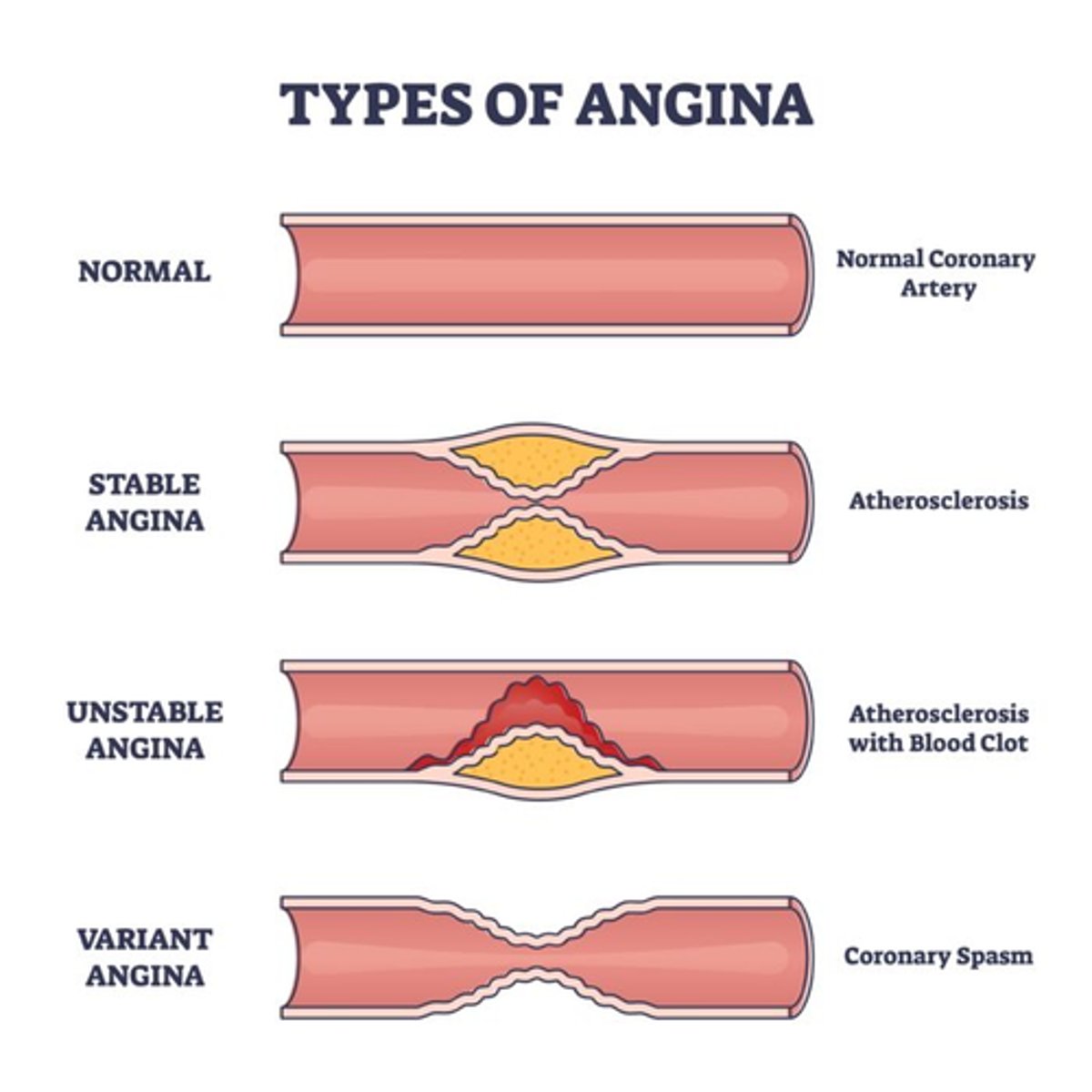
What is the underlying cause of Prinzmetal (Variant) Angina?
A) Coronary vasospasm
B) Myocardial ischemia caused by O2 supply/demand mismatch
C) Myocardial infarction caused by complete blockage of blood flow
D) Pulmonary embolism caused by a blood clot in the lung
A) Coronary vasospasm (rarely leads to heart attack)
What are the characteristics of Prinzmetal (Variant) Angina?
A) Occurs primarily during physical exertion and is relieved by rest
B) Occurs primarily at rest and is triggered by smoking and some substances
C) Unpredictable pain that occurs randomly and is relieved by physical activity
D) Continuous pain that does not change with rest or medication
B) Occurs primarily at rest and is triggered by smoking and some substances (histamines, epi, cocaine)
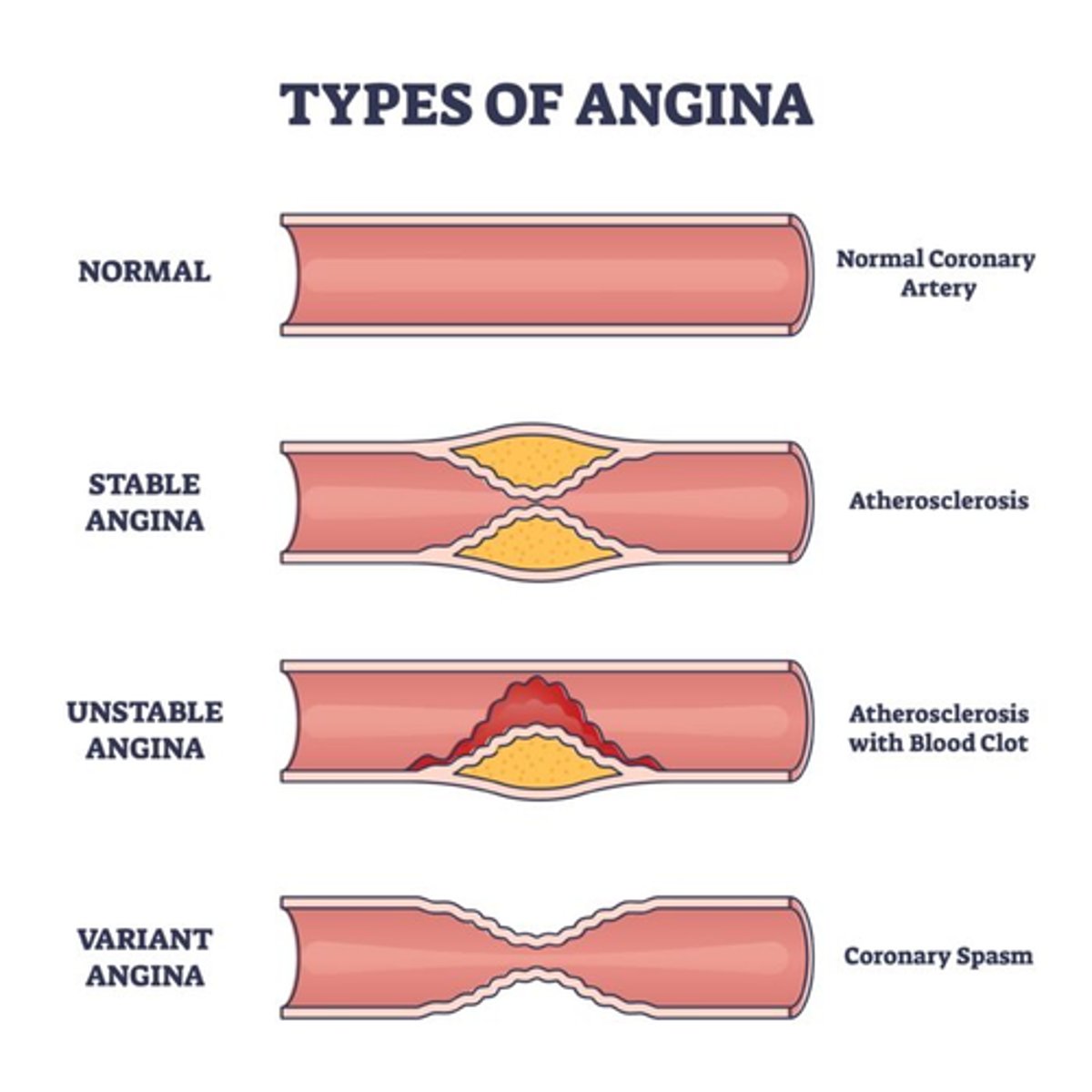
What is the primary cause of unstable angina?
A) Coronary vasospasm
B) Rupture of unstable plaque
C) Myocardial ischemia caused by O2 supply/demand mismatch
D) Complete blockage of a coronary artery
B) Rupture of unstable plaque
Which of the following are characteristics of unstable angina?
A) New onset angina, chronic stable angina that changes in characteristic, and chest pain lasting more than 10 minutes
B) Occurs primarily at rest, triggered by smoking and some substances, and relieved by rest or NTG
C) Episodic pain provoked by exertion or stress, occurring intermittently over a long period of time, and predictable
D) Continuous pain that does not change with rest or medication
A) New onset angina, chronic stable angina that changes in characteristic, and chest pain lasting more than 10 minutes (call 911! They in danger!)
Which of the following are potential complications of coronary artery disease (CAD)?
A) Sudden cardiac death, Dysrhythmias, Myocardial infarction, Heart failure
B) Stroke, Hypertension, Diabetes, Atrial fibrillation
C) Pulmonary embolism, Chronic obstructive pulmonary disease (COPD), Kidney failure, Liver cirrhosis
D) Hypotension, Anemia, Asthma, Peptic ulcer disease
A) Sudden cardiac death, Dysrhythmias, Myocardial infarction, Heart failure
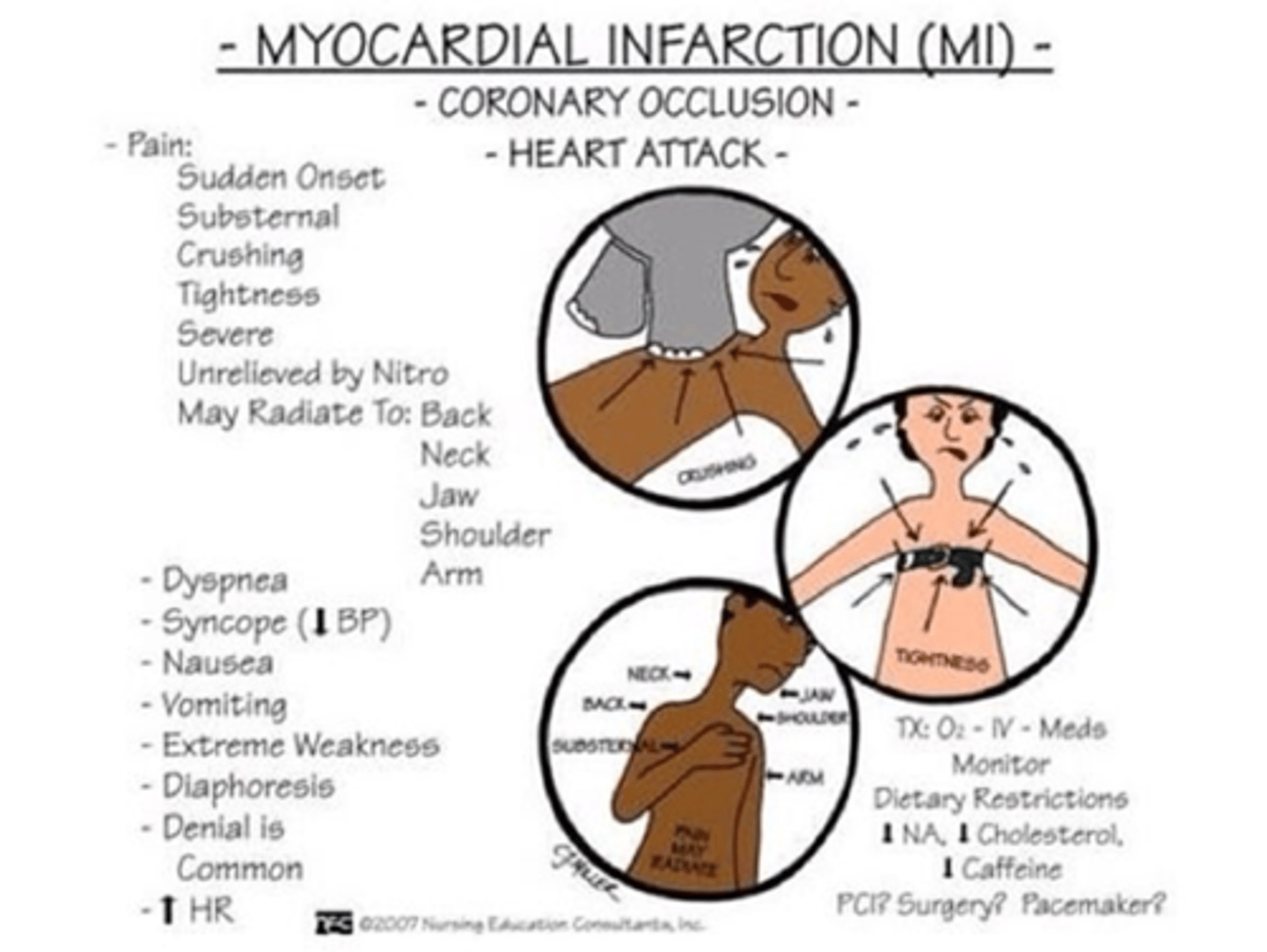
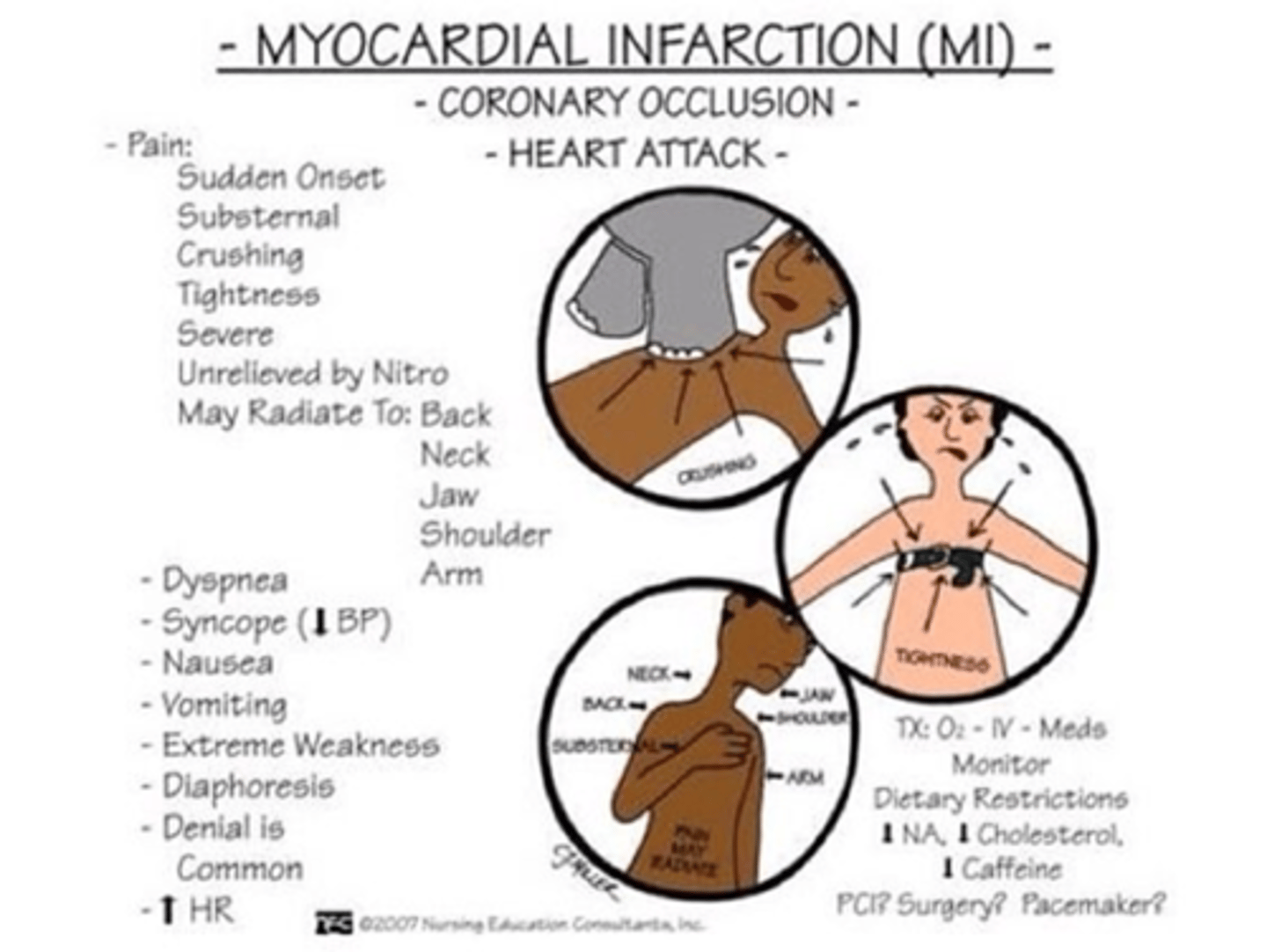
What is the pathophysiology of a myocardial infarction (MI)?
A) Reversible damage to the cardiac muscle caused by a short period of ischemia
B) Myocardial infarction is a total obstruction of the coronary artery, resulting in necrosis of the heart muscle cells caused by thrombus or vasospasm
C) Irreversible damage to the cardiac muscle caused by high blood pressure
D) Reversible damage to the cardiac muscle caused by vasospasm alone
B) Myocardial infarction is a total obstruction of the coronary artery, resulting in necrosis of the heart muscle cells caused by thrombus or vasospasm
Which of the following are risk factors for myocardial infarction (MI)?
A) Young age, Low blood pressure, Active lifestyle, Low triglycerides
B) Age, Hypertension (HTN), Genetics, Tobacco use, Diabetes, Obesity, Sedentary lifestyle, CAD, Hypercholesterolemia, High triglycerides, Metabolic syndrome, Stress, Illicit drug use, Autoimmune conditions
C) Proper diet, Regular exercise, Low stress, Normal cholesterol levels
D) High vitamin intake, Moderate alcohol consumption, Low sugar intake, Active lifestyle
B) Age, Hypertension (HTN), Genetics, Tobacco use, Diabetes, Obesity, Sedentary lifestyle, CAD, Hypercholesterolemia, High triglycerides, Metabolic syndrome, Stress, Illicit drug use (cocaine), Autoimmune conditions (risk factors the exact same as CAD with exception of autoimmune conditions being added)
Which of the following are typical symptoms of a myocardial infarction (MI)?
A) Angina, pain that spreads to neck, jaw, and/or back, shortness of breath, nausea/vomiting, diaphoresis, fatigue, light headedness/dizziness, anxiety/restlessness, low grade fever
B) Mild chest discomfort, increased appetite, low blood pressure, high energy levels, improved sleep
C) Regular heart rhythm, high blood pressure, no pain, increased physical endurance
D) Sudden weight gain, high-grade fever, headache, swollen ankles
A) Angina, pain that spreads to neck, jaw, and/or back, shortness of breath, nausea/vomiting, diaphoresis, fatigue, light headedness/dizziness, anxiety/restlessness, low grade fever
Which of the following are atypical symptoms of a myocardial infarction (MI), commonly seen in diabetic patients and women?
A) Severe chest pain, radiating to the left arm, high-grade fever, increased energy
B) Nausea, epigastric pain/heartburn, asymptomatic
C) Shortness of breath, fatigue, high blood pressure, palpitations
D) Sudden weight gain, severe headache, leg cramps, improved appetite
B) Nausea, epigastric pain/heartburn, asymptomatic
Which of the following diagnostics are used to evaluate a myocardial infarction (MI)?
A) EKG (STEMI/NSTEMI), Troponin, CK-MB, Creatinine Kinase (CK), Myoglobin
B) Chest X-ray, Blood glucose levels, Complete Blood Count (CBC), Urinalysis
C) MRI, Liver function tests, Bone density scan, Thyroid function tests
D) Ultrasound, Blood pressure measurement, Electrolyte panel, Lipid profile
A) EKG (STEMI/NSTEMI), Troponin, CK-MB, Creatinine Kinase (CK), Myoglobin
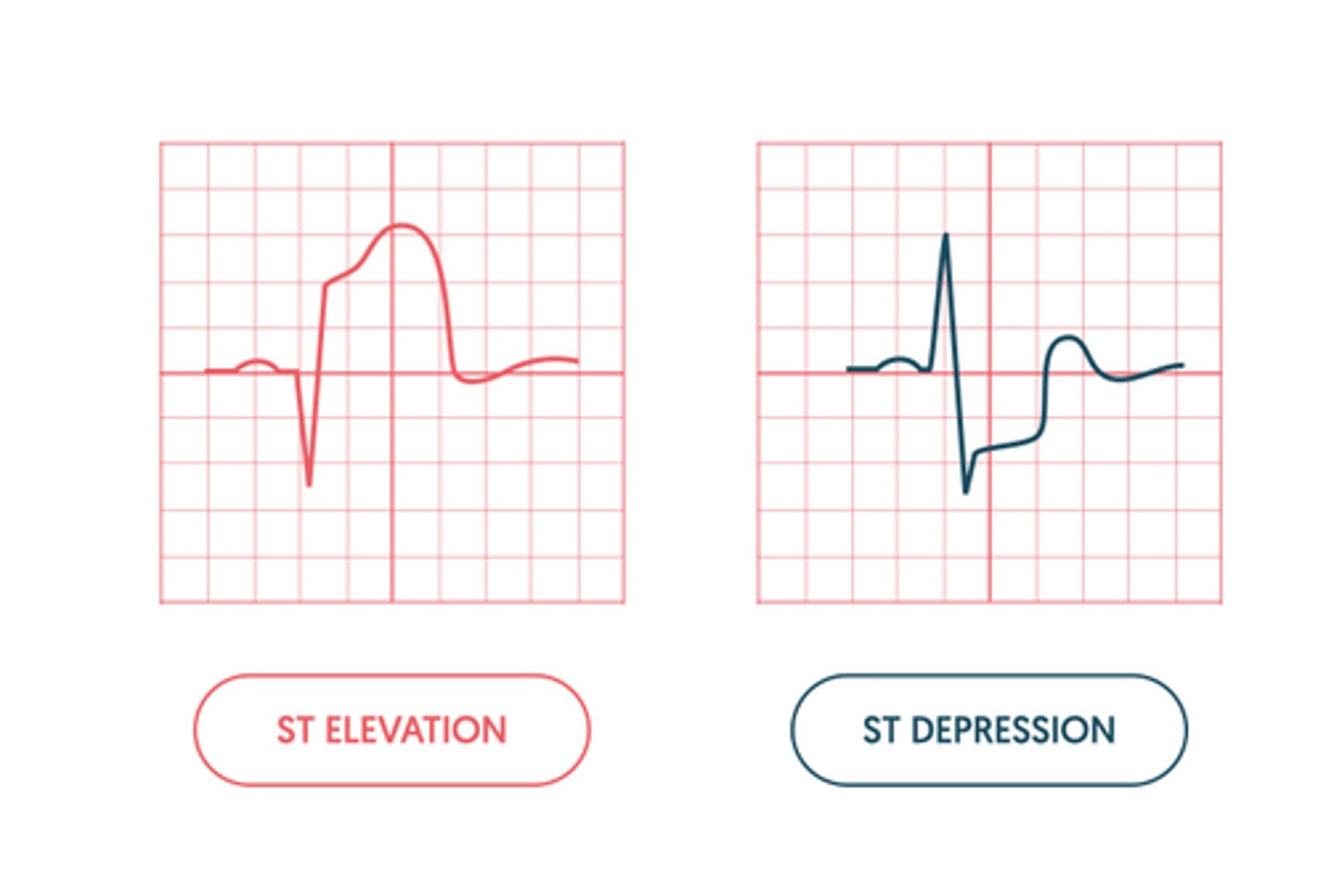
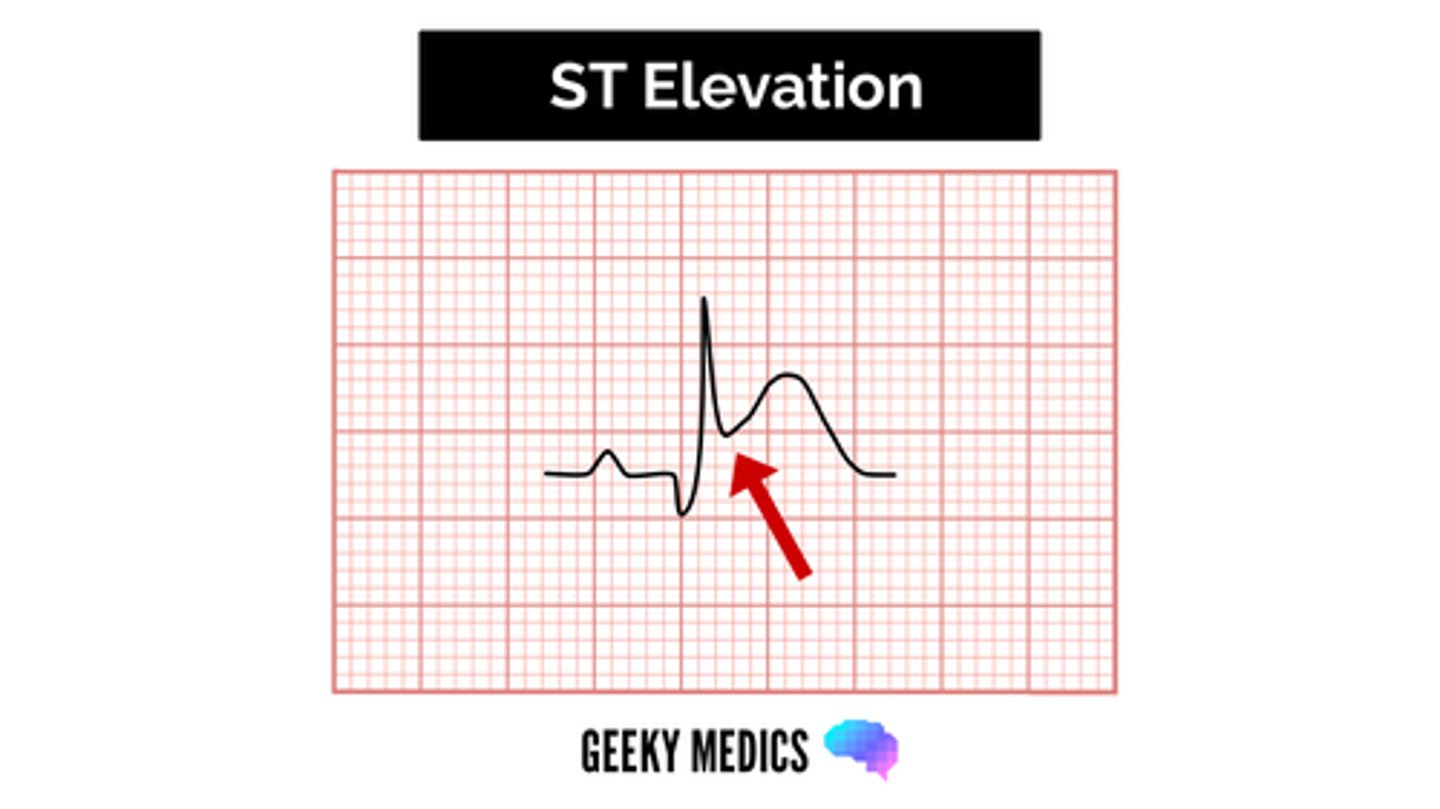
What is a key characteristic of a STEMI (ST-Elevation Myocardial Infarction)?
A) ST depression on EKG
B) No immediate need for intervention
C) Elevated ST segment on EKG and indicates an ongoing heart attack requiring immediate intervention
D) Normal EKG reading
C) Elevated ST segment on EKG and indicates an ongoing heart attack requiring immediate intervention
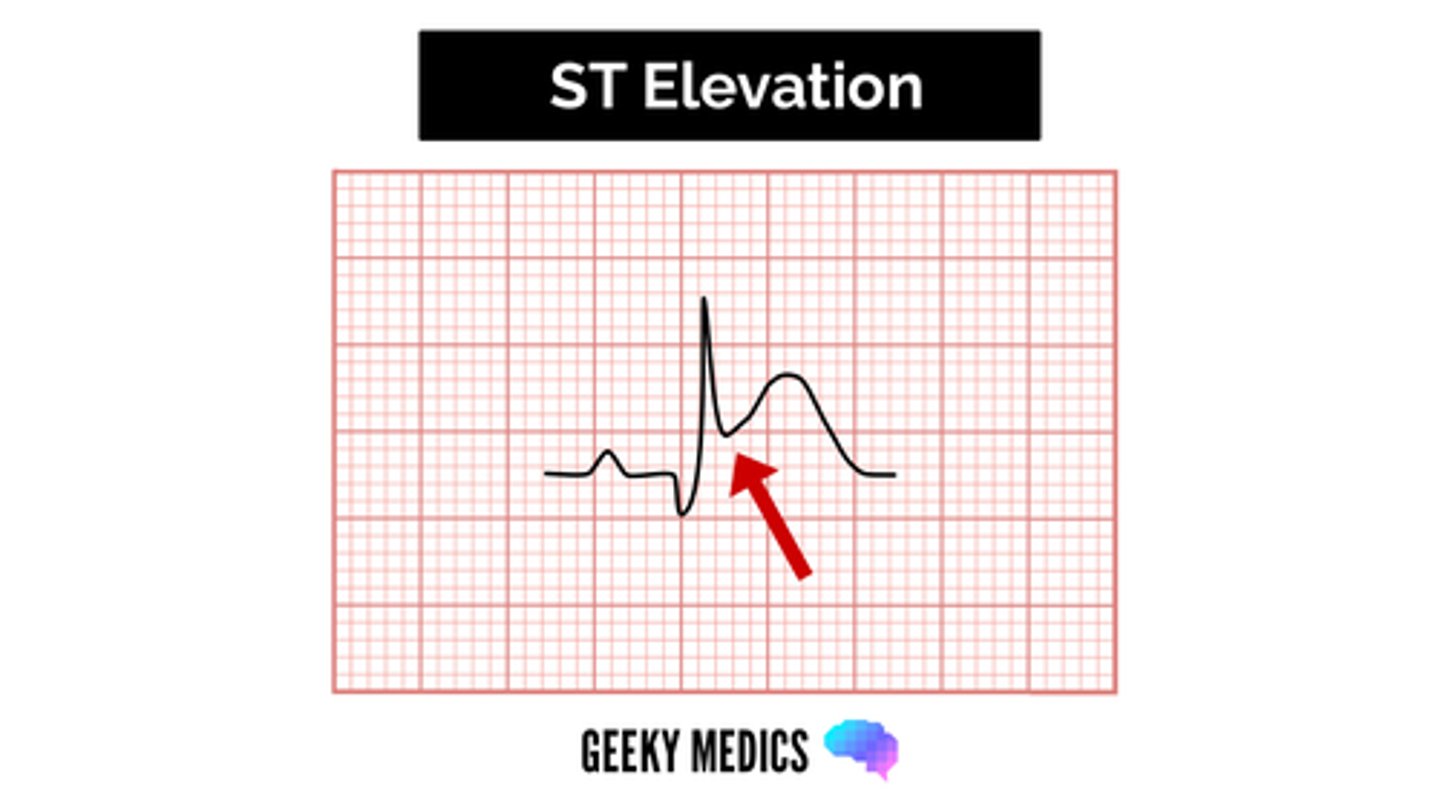
What distinguishes an NSTEMI (Non-ST-Elevation Myocardial Infarction) from a STEMI?
A) NSTEMI is associated with elevated ST segments on EKG
B) NSTEMI usually presents with ST depression on EKG and does not indicate the exact date or time of occurrence and does not require immediate intervention
C) NSTEMI is less severe and does not require medical attention
D) NSTEMI indicates a complete blockage of the coronary artery
B) NSTEMI usually presents with ST depression (typically but not all the time, NSTEMI = non-ST-elevation) on EKG and does not indicate the exact date or time of occurrence and does not require immediate intervention
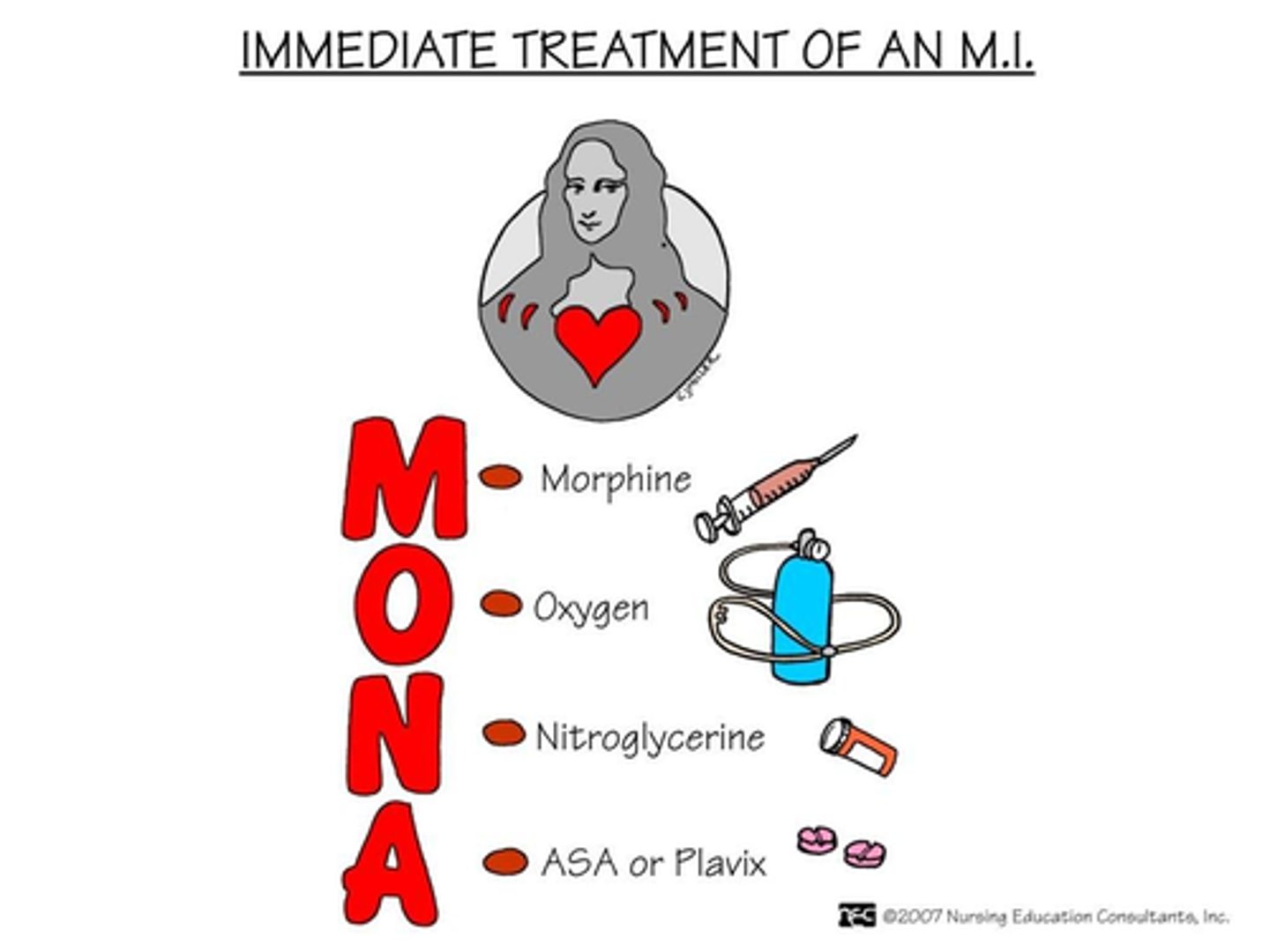
What is included in the treatment for NSTEMI using the MONAH protocol?
A) M: Morphine – vasodilates to increase blood flow & calms the patient down
B) O: Oxygen – provides O2 rich blood to the blood that may get through
C) N: Nitrates – vasodilates to increase blood flow
D) A: Aspirin – antiplatelet, prevents clot from getting bigger (patient must chew)
E) H: Heparin – prevents clot from getting bigger
F) All of the above
F) All of the above
Which of the following treatments are used for STEMI?
A) Percutaneous Coronary Intervention (PCI) involving cardiac catheterization (balloon/stent), Thrombolytic Therapy (tPA), Emergency coronary artery bypass graft (CABG)
B) Medication management only, Electrophysiological study, Thrombolytic Therapy (tPA)
C) Immediate ambulation, checking blood sugar levels, encouraging physical activity
D) Use of compression stockings, encouraging deep breathing exercises, checking for pedal pulses
A) Percutaneous Coronary Intervention (PCI) involving cardiac catheterization (balloon/stent), Thrombolytic Therapy (tPA), Emergency coronary artery bypass graft (CABG)
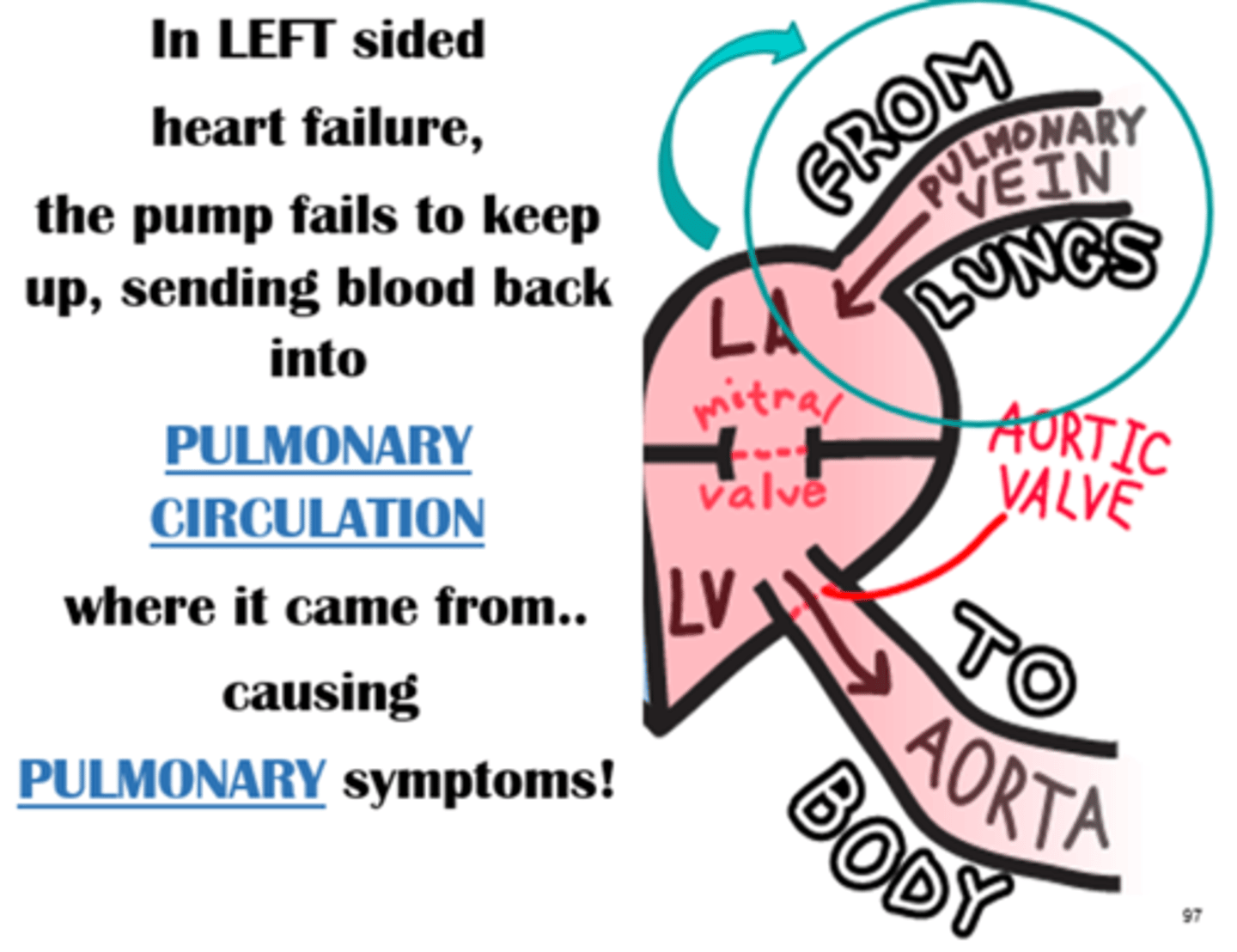
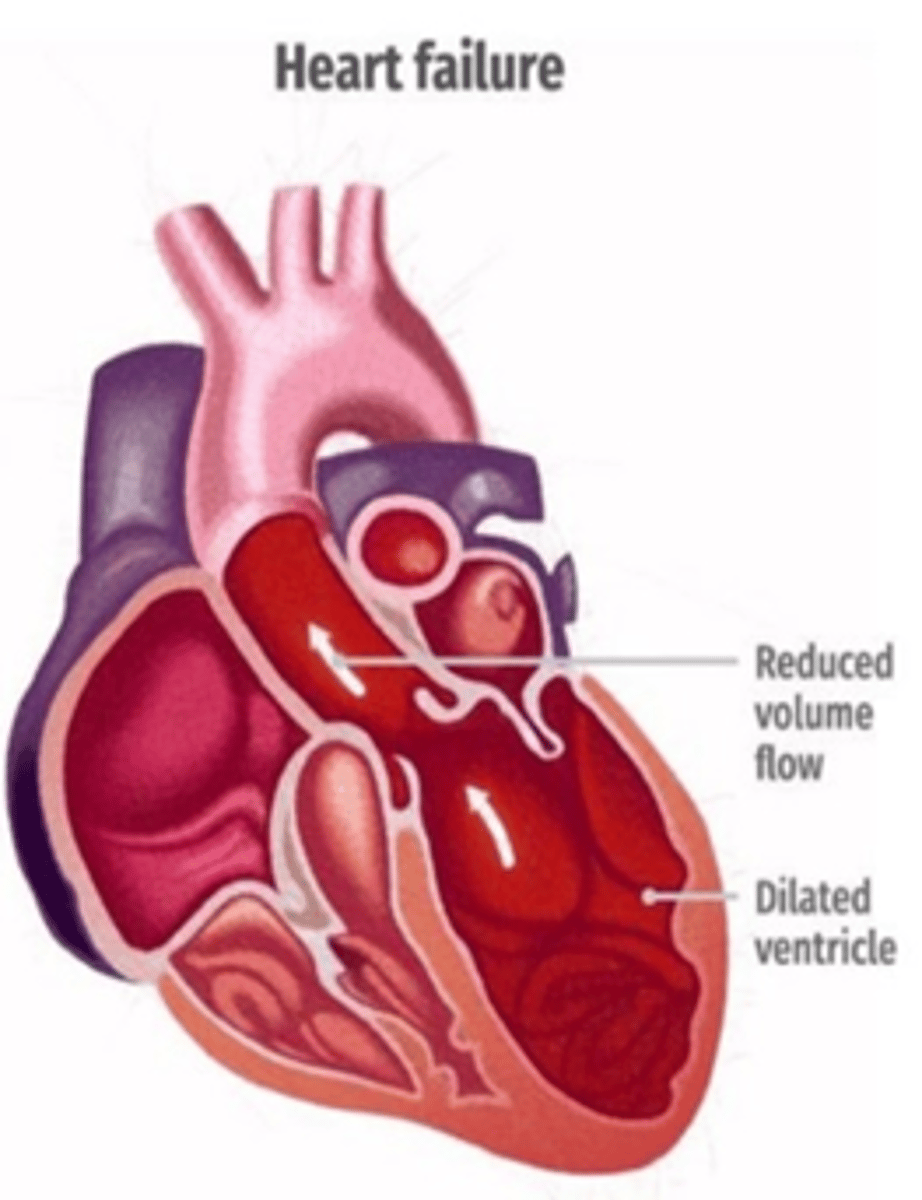
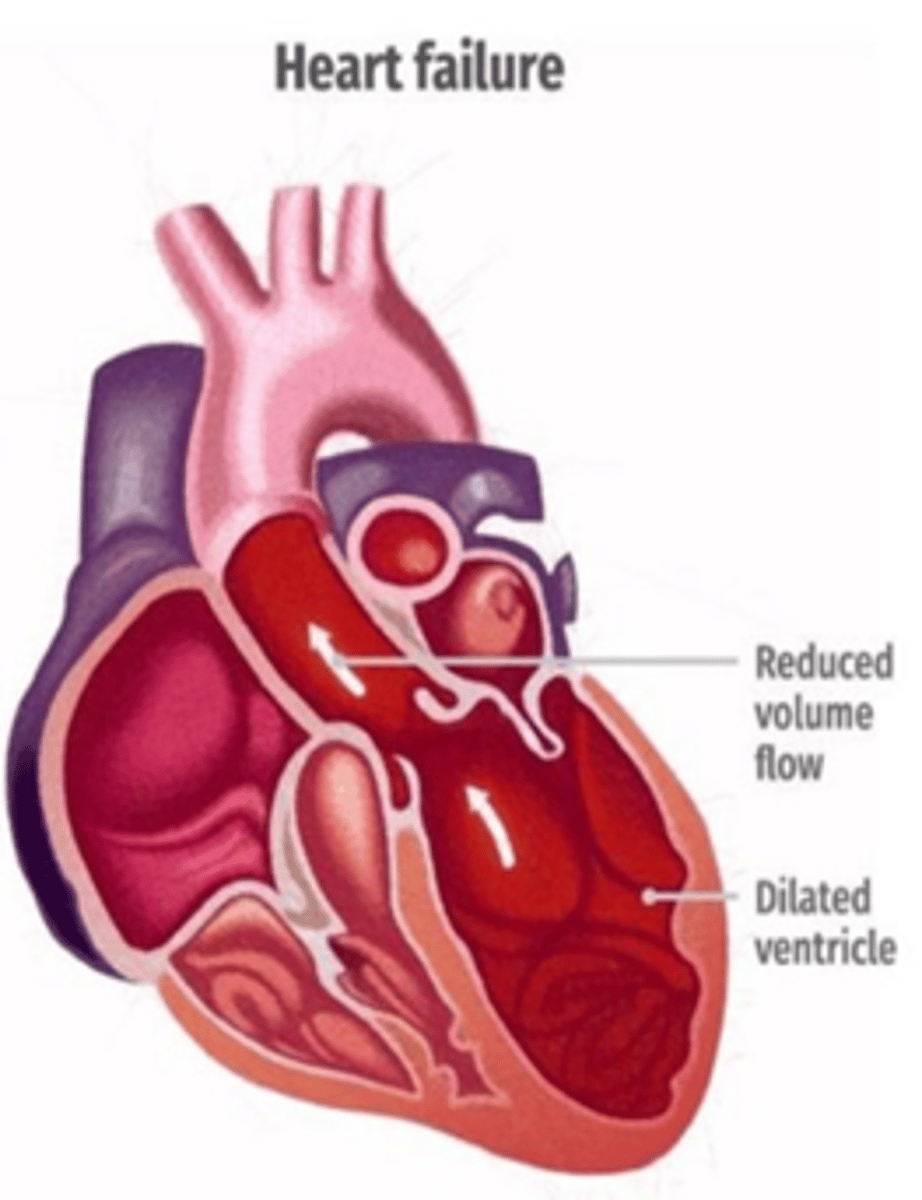
What happens in left-sided heart failure?
A) The left side of the heart fails to pump blood to the body, so it backs up and goes to the lungs
B) The left side of the heart fails to pump blood to the lungs, so it backs up and goes to the body
C) The right side of the heart fails to pump blood to the body, so it backs up and goes to the lungs
D) The right side of the heart fails to pump blood to the lungs, so it backs up and goes to the body
A) The left side of the heart fails to pump blood to the body, so it backs up and goes to the lungs
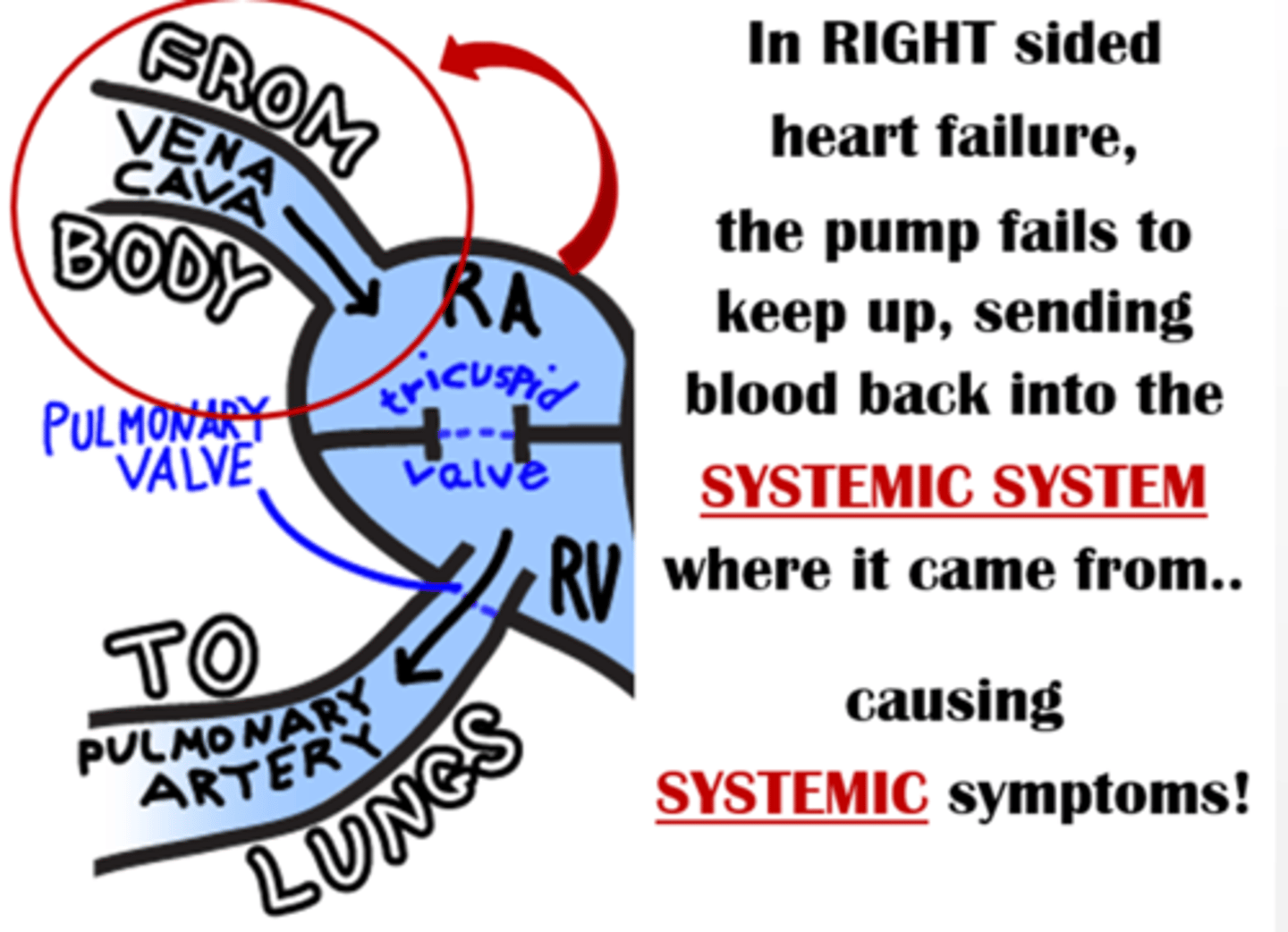
What happens in right-sided heart failure?
A) The left side of the heart fails to pump blood to the body, so it backs up and goes to the lungs
B) The left side of the heart fails to pump blood to the lungs, so it backs up and goes to the body
C) The right side of the heart fails to pump blood to the body, so it backs up and goes to the lungs
D) The right side of the heart fails to pump blood to the lungs, so it backs up and goes to the body
D) The right side of the heart fails to pump blood to the lungs, so it backs up and goes to the body
What is the leading cause of right-sided heart failure?
A) High blood pressure
B) Diabetes
C) Left-sided heart failure
D) Coronary artery disease
C) Left-sided heart failure
Which of the following diagnostics are used to evaluate heart failure?
A) B-type natriuretic peptide (BNP) level, Echocardiogram (monitor ejection fraction), EKG (monitor for dysrhythmias)
B) Blood glucose test, Chest X-ray, MRI
C) Complete blood count (CBC), Liver function test, Urinalysis
D) Spirometry, Skin test, Bone density scan
A) B-type natriuretic peptide (BNP) level, Echocardiogram (monitor ejection fraction), EKG (monitor for dysrhythmias)
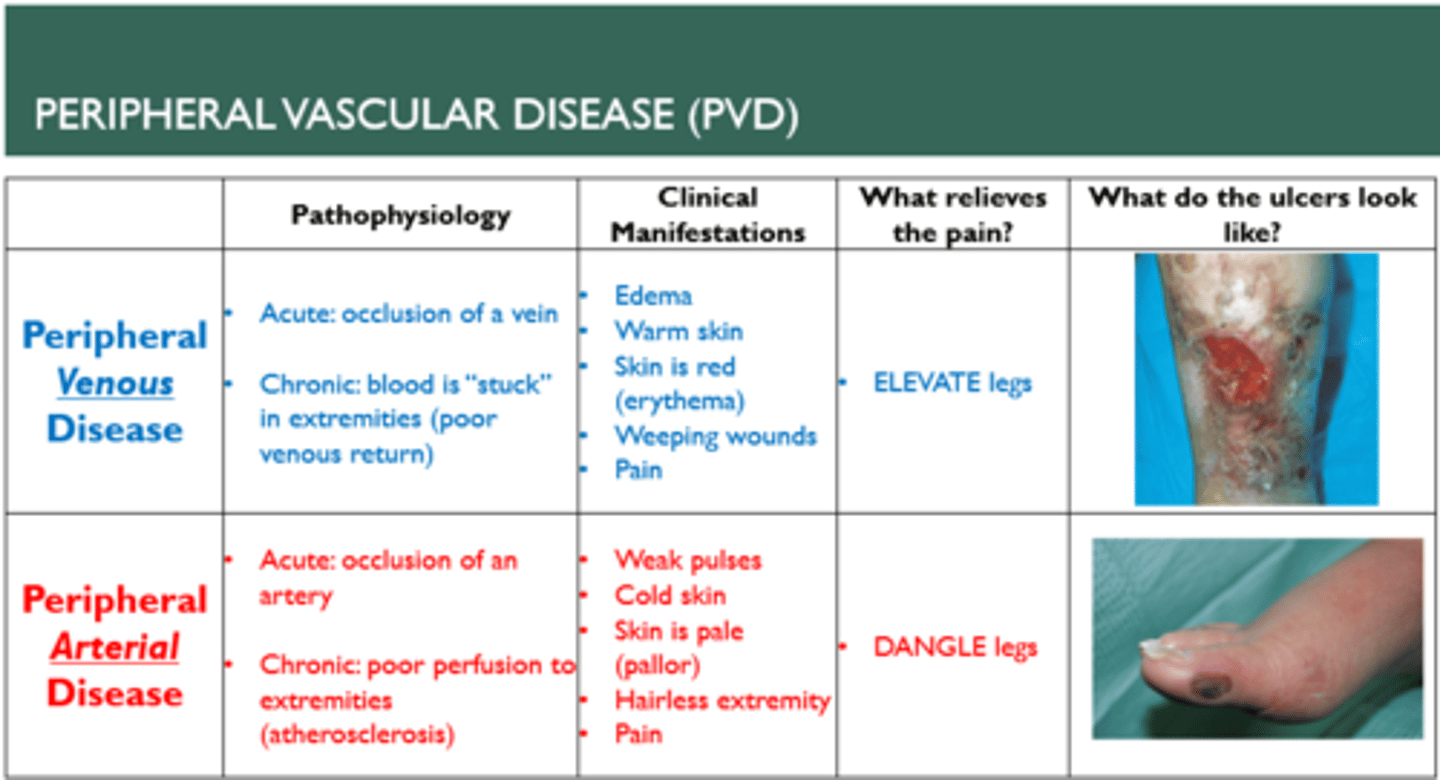
In the context of peripheral vascular disease (PVD), which statement is accurate?
A) Wet is arterial, Dry is venous
B) Wet is venous, Dry is arterial
C) Wet is localized, Dry is systemic
D) Wet is chronic, Dry is acute
B) Wet is venous, Dry is arterial
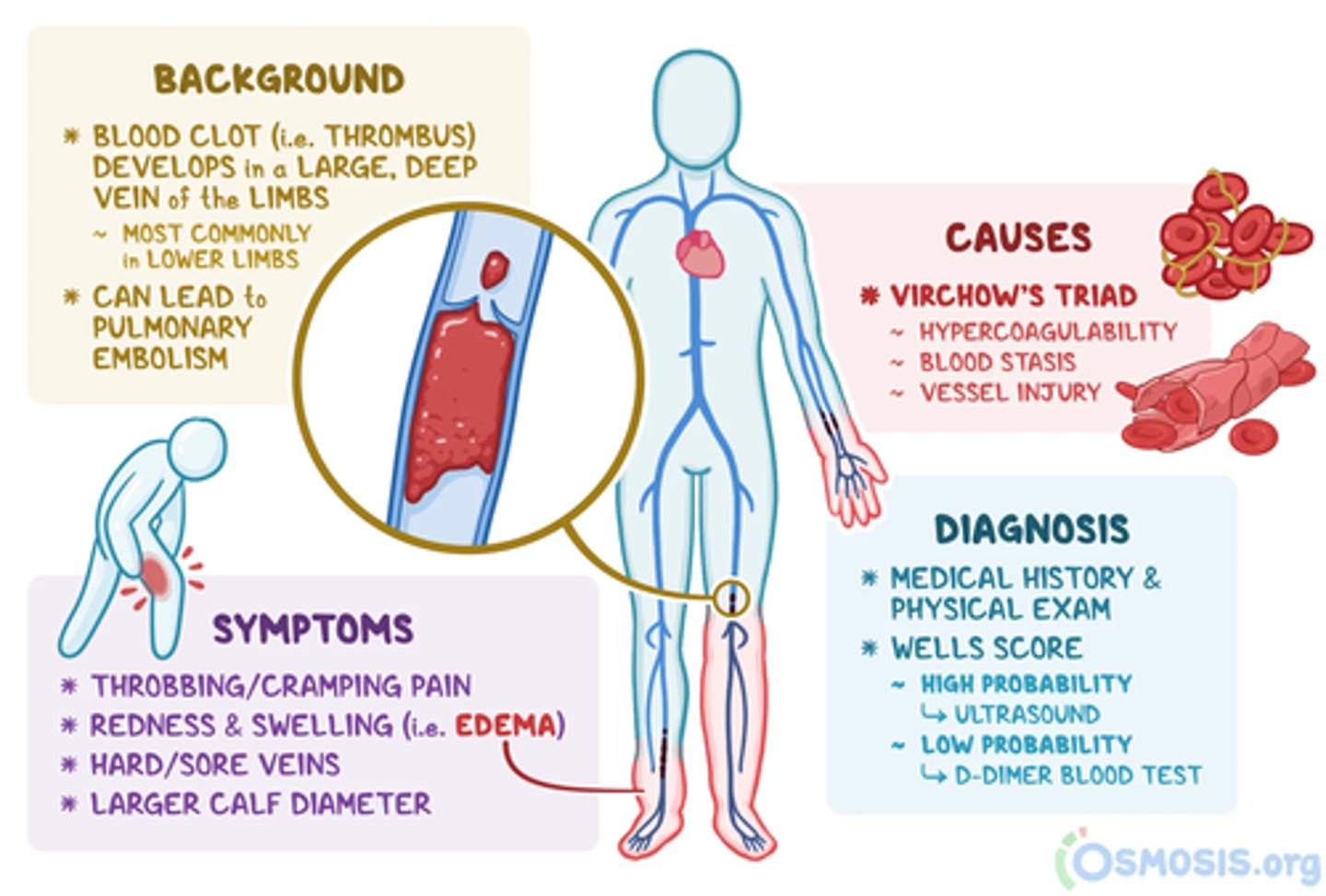
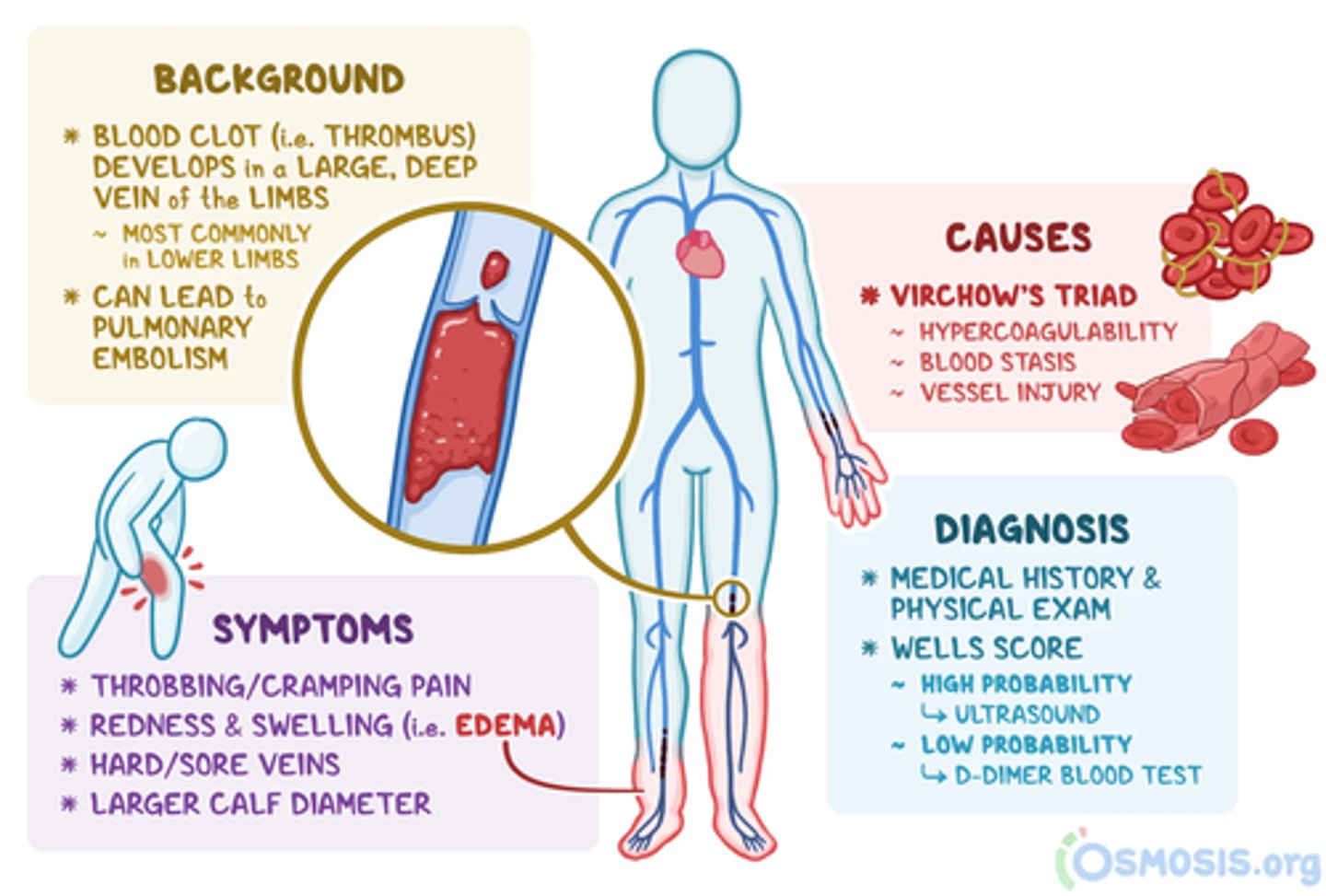
Which of the following are risk factors for deep vein thrombosis (DVT)?
A) Frequent physical activity, low blood pressure, high fiber diet
B) Sitting too long, diabetes, obesity, smoking, prolonged immobility
C) Regular exercise, balanced diet, low stress levels
D) High vitamin intake, moderate alcohol consumption, active lifestyle
B) Sitting too long, diabetes, obesity, smoking, prolonged immobility
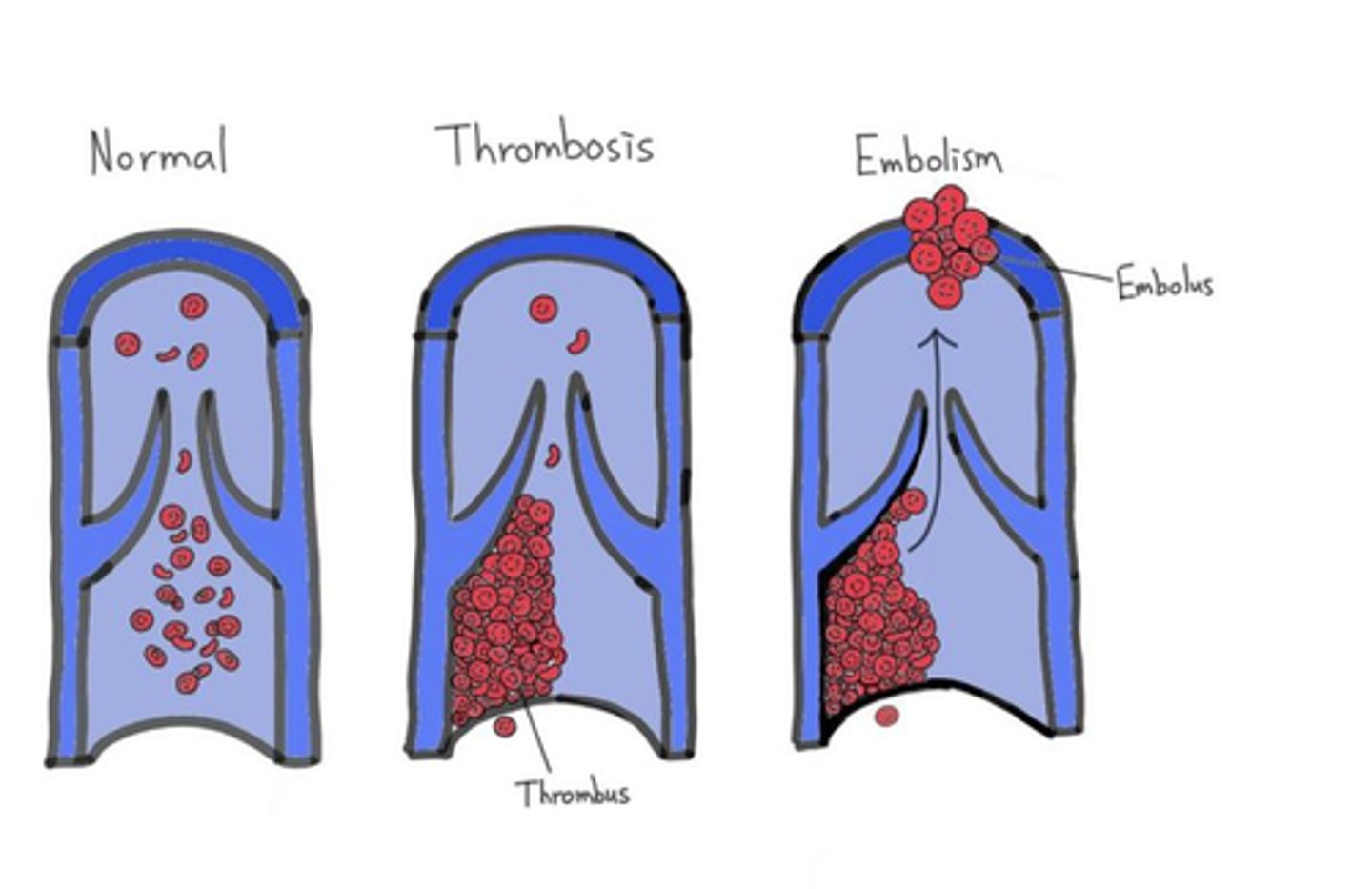
What is the primary difference between thrombi and emboli?
A) Thrombi are blood clots that form in a vein or artery and stay in place, while emboli are blood clots that travel through the bloodstream to another location.
B) Thrombi are solid masses formed from cholesterol, while emboli are solid masses formed from calcium deposits.
C) Thrombi are clots formed in the heart, while emboli are clots formed in the lungs.
D) Thrombi are related to high blood pressure, while emboli are related to low blood pressure.
A) Thrombi are blood clots that form in a vein or artery and stay in place, while emboli are blood clots that travel through the bloodstream to another location.
Which of the following are clinical manifestations of deep vein thrombosis (DVT)?
A) Cold, pale skin, slow heart rate, low blood pressure
B) Inflammatory response: redness, swelling, warmth, pain/tenderness
C) High fever, rash, dizziness, increased appetite
D) Dry skin, itching, muscle cramps, fatigue
B) Inflammatory response: redness, swelling, warmth, pain/tenderness
What is the definition of hypoxia?
A) An excess of oxygen in the tissues
B) A deficiency of carbon dioxide in the blood
C) A deficiency of oxygen in the tissues
D) An excess of carbon dioxide in the blood
C) A deficiency of oxygen in the tissues
MODIFIABLE VS. NON MODIFIABLE RISK FACTORS
Know all of them for everything :)
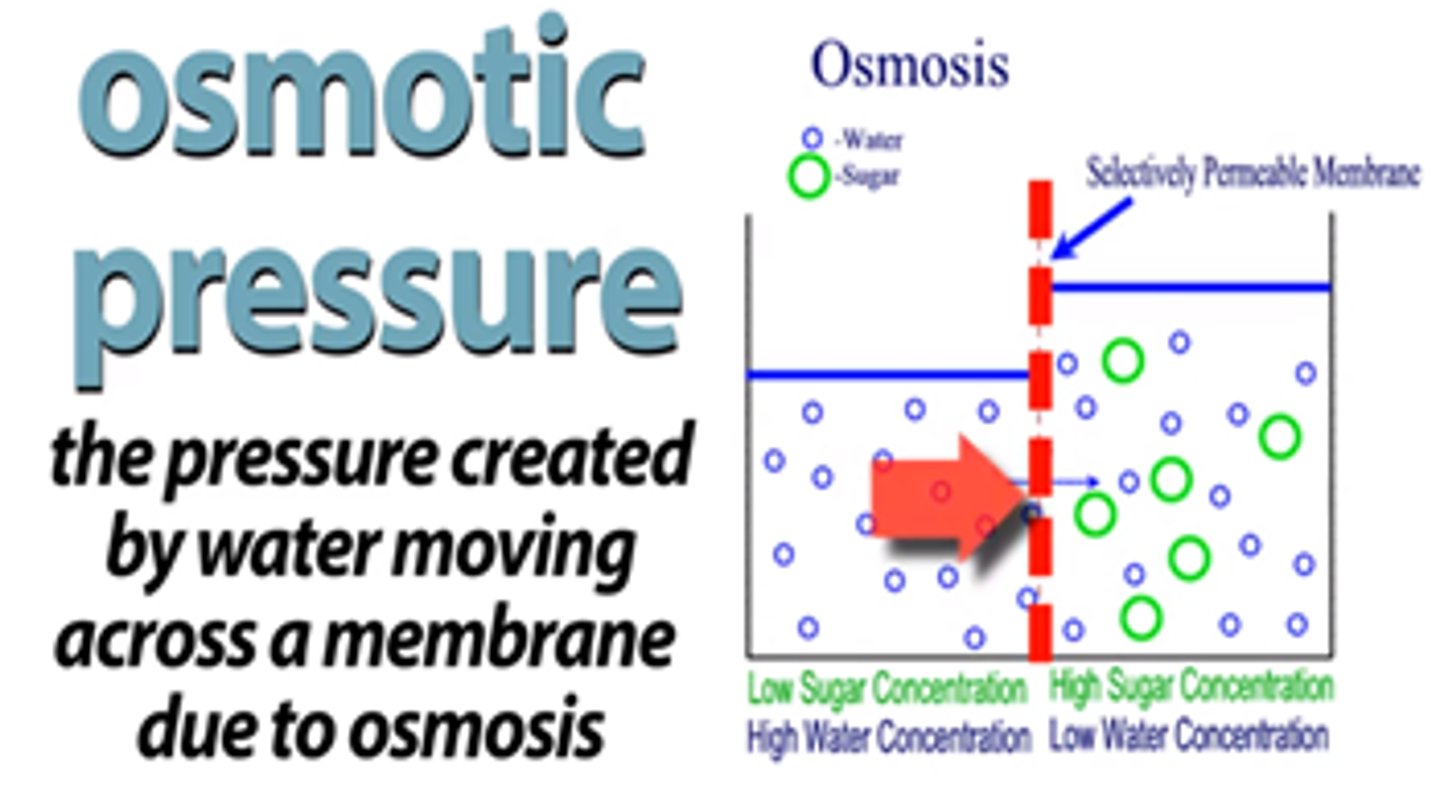
What does osmotic pressure do?
A) Draws fluid from an area of lower concentration to one of higher concentration
B) Draws fluid from an area of higher concentration to one of lower concentration
C) Prevents the movement of fluid between areas of different concentrations
D) Equally distributes fluid across areas regardless of concentration differences
B) Draws fluid from an area of higher concentration to one of lower concentration
What are the characteristics of acute and chronic renal failure?
A) Acute renal failure is characterized by a sudden loss of renal function, while chronic renal failure involves the gradual irreversible destruction of the kidneys over a long period of time.
B) Acute renal failure involves the gradual irreversible destruction of the kidneys over a long period of time, while chronic renal failure is characterized by a sudden loss of renal function.
C) Both acute and chronic renal failure involve reversible damage to the kidneys.
D) Acute renal failure and chronic renal failure are both characterized by temporary decreases in kidney function.
A) Acute renal failure is characterized by a sudden loss of renal function, while chronic renal failure involves the gradual irreversible destruction of the kidneys over a long period of time.
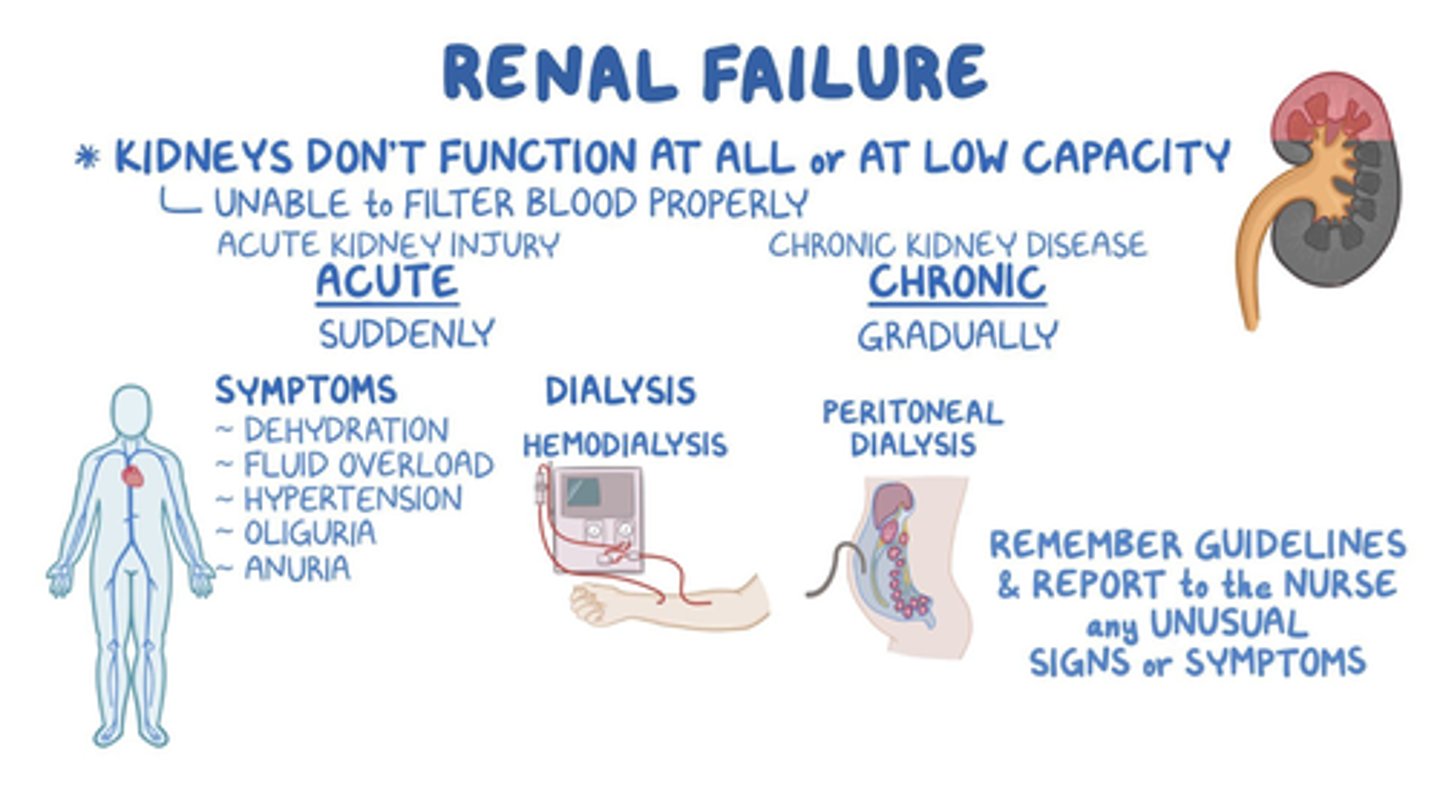
What characterizes acute renal failure, including its etiology and clinical manifestations?
A) Gradual irreversible destruction of the kidneys over a long period of time; etiology includes prolonged episodes of ARF and hypertension; clinical manifestations include a gradual decrease of GFR, increased BUN, and creatinine levels.
B) Sudden loss of renal function; etiology includes lack of blood flow; clinical manifestations include fluid retention, BP fluctuation, and electrolyte abnormalities.
C) Sudden loss of renal function; etiology includes hypertension; clinical manifestations include a gradual decrease of GFR, increased BUN, and creatinine levels.
D) Gradual irreversible destruction of the kidneys over a long period of time; etiology includes lack of blood flow; clinical manifestations include fluid retention, BP fluctuation, and electrolyte abnormalities.
B) Sudden loss of renal function; etiology includes lack of blood flow; clinical manifestations include fluid retention, BP fluctuation, and electrolyte abnormalities.
What characterizes chronic renal failure, including its etiology and clinical manifestations?
A) Sudden loss of renal function; etiology includes lack of blood flow; clinical manifestations include fluid retention, BP fluctuation, and electrolyte abnormalities.
B) Gradual irreversible destruction of the kidneys over a long period of time; etiology includes prolonged episodes of ARF and hypertension; clinical manifestations include a gradual decrease of GFR, increased BUN, and creatinine levels.
C) Gradual irreversible destruction of the kidneys over a long period of time; etiology includes lack of blood flow; clinical manifestations include fluid retention, BP fluctuation, and electrolyte abnormalities.
D) Sudden loss of renal function; etiology includes prolonged episodes of ARF and hypertension; clinical manifestations include a gradual decrease of GFR, increased BUN, and creatinine levels.
B) Gradual irreversible destruction of the kidneys over a long period of time; etiology includes prolonged episodes of ARF and hypertension; clinical manifestations include a gradual decrease of GFR, increased BUN, and creatinine levels.
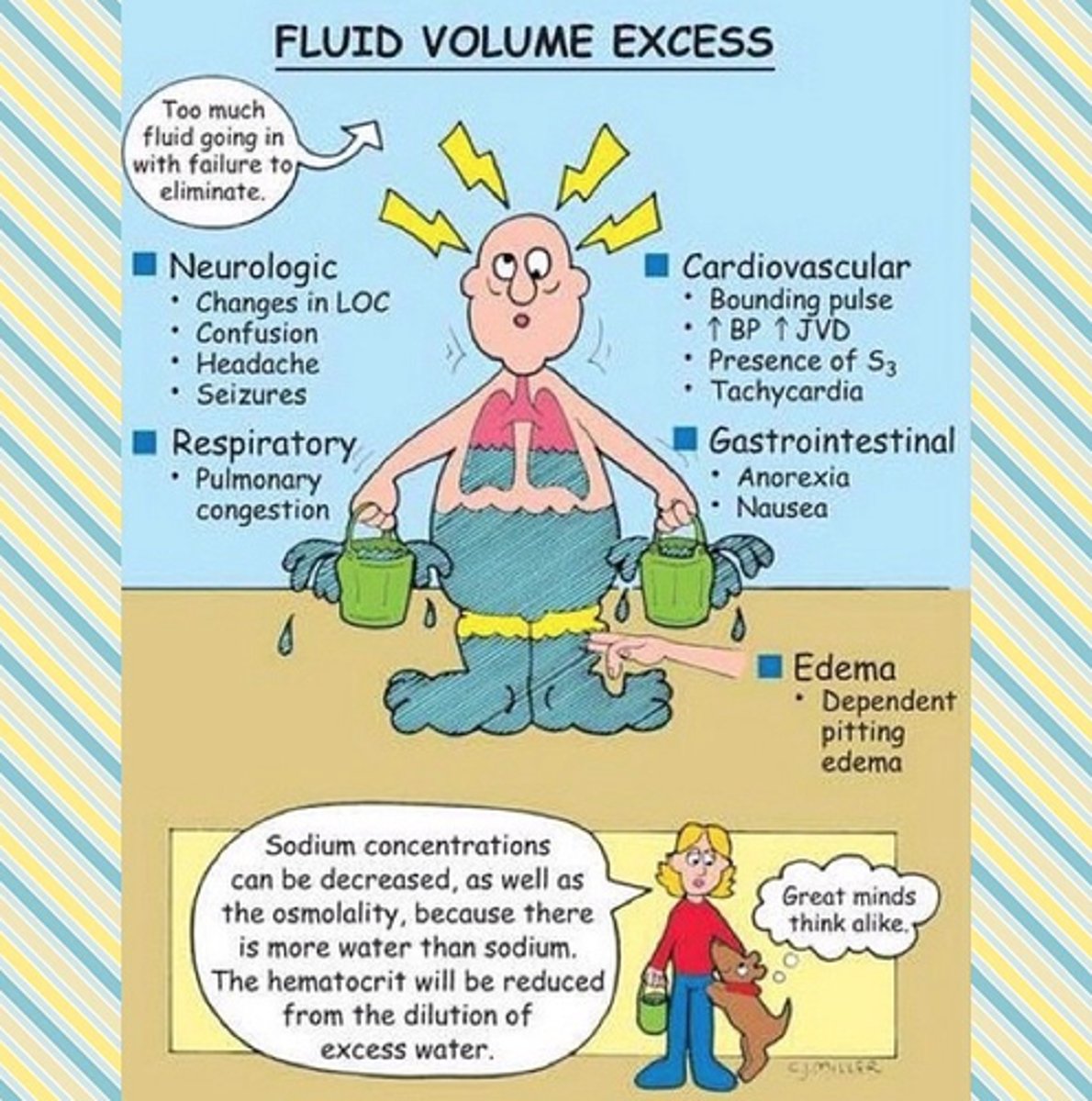
What is hypervolemia and what are some conditions associated with it?
A) A condition where too little fluid accumulates in the body; associated with dehydration and high blood pressure
B) A condition where blood becomes too thick; associated with polycythemia and clotting disorders
C) A condition where too much fluid accumulates in the body and/or organs are unable to manage or excrete it; associated with heart failure, renal failure, and cirrhosis
D) A condition where there is an electrolyte imbalance; associated with hypokalemia and hypernatremia
C) A condition where too much fluid accumulates in the body and/or organs are unable to manage or excrete it; associated with heart failure, renal failure, and cirrhosis
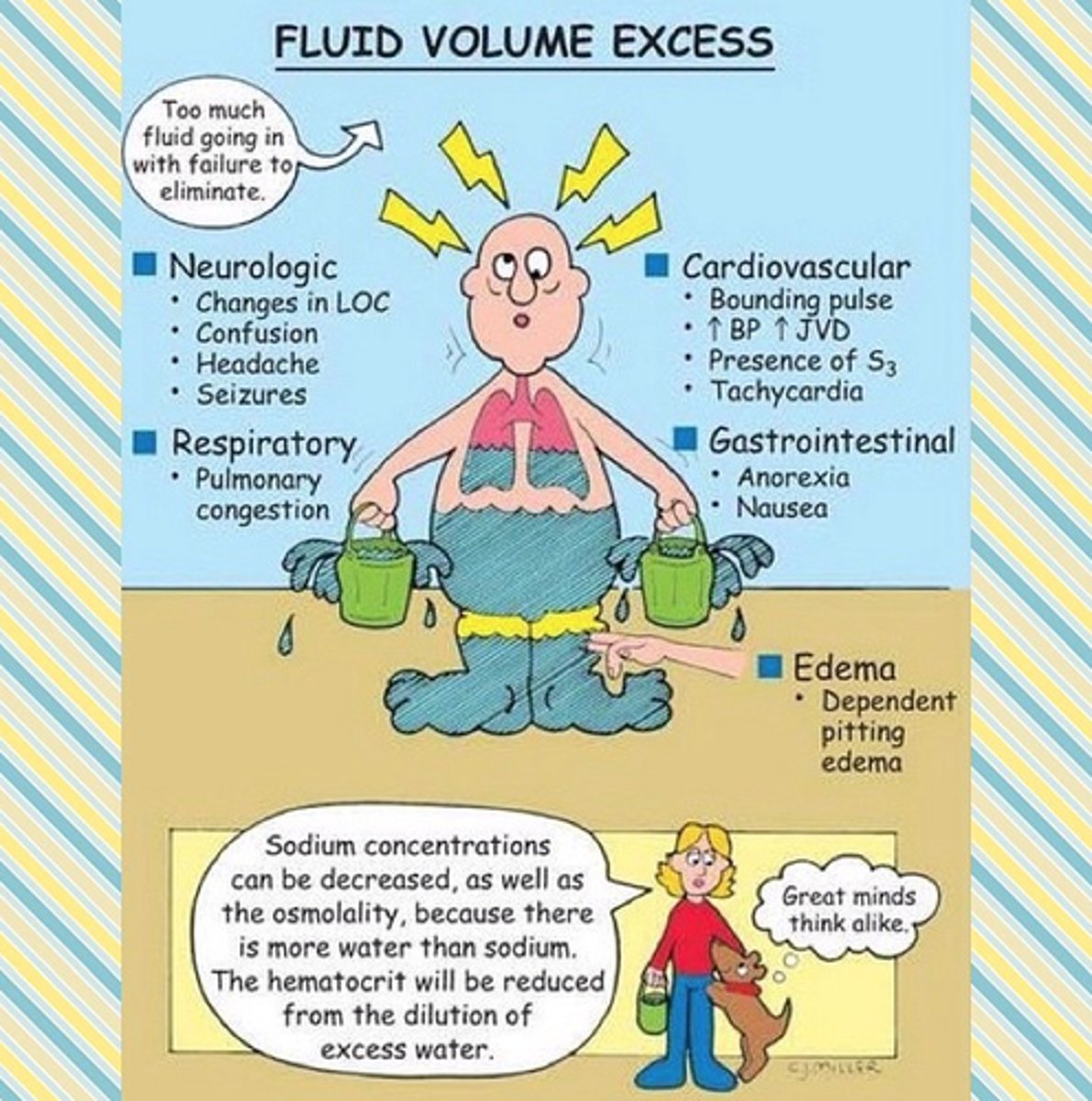
Which of the following are clinical manifestations of hypervolemia?
A) Edema, high blood pressure, shortness of breath
B) Dehydration, low blood pressure, increased heart rate
C) Muscle cramps, dry skin, weight loss
D) Fatigue, low blood sugar, decreased appetite
A) Edema, high blood pressure, shortness of breath
How does the body compensate when dehydrated?
A) By increasing insulin secretion to regulate blood sugar levels
B) By activating the Renin-Angiotensin-Aldosterone System (RAAS) to retain sodium and water
C) By decreasing heart rate to conserve energy
D) By increasing the production of red blood cells to improve oxygen transport
B) By activating the Renin-Angiotensin-Aldosterone System (RAAS) to retain sodium and water
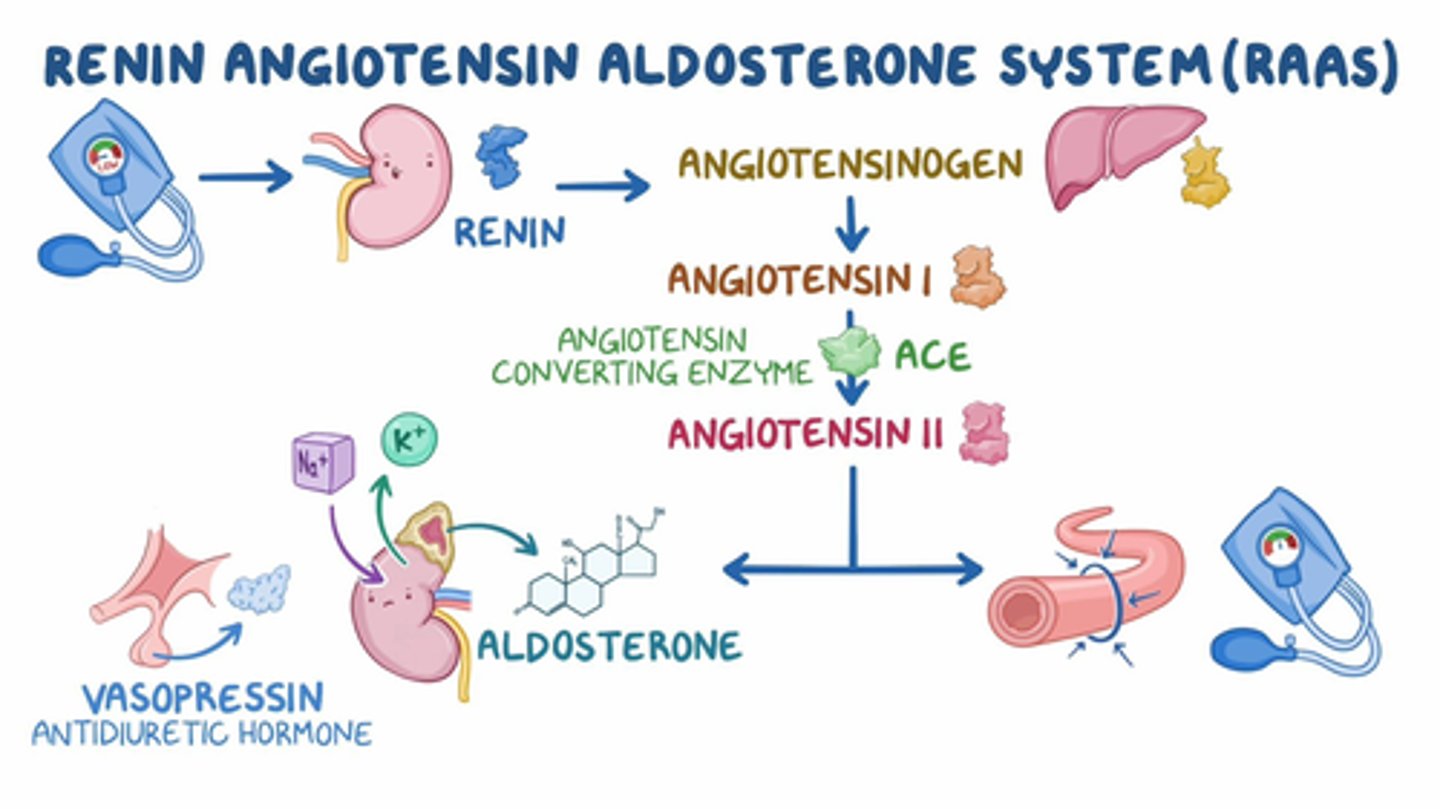
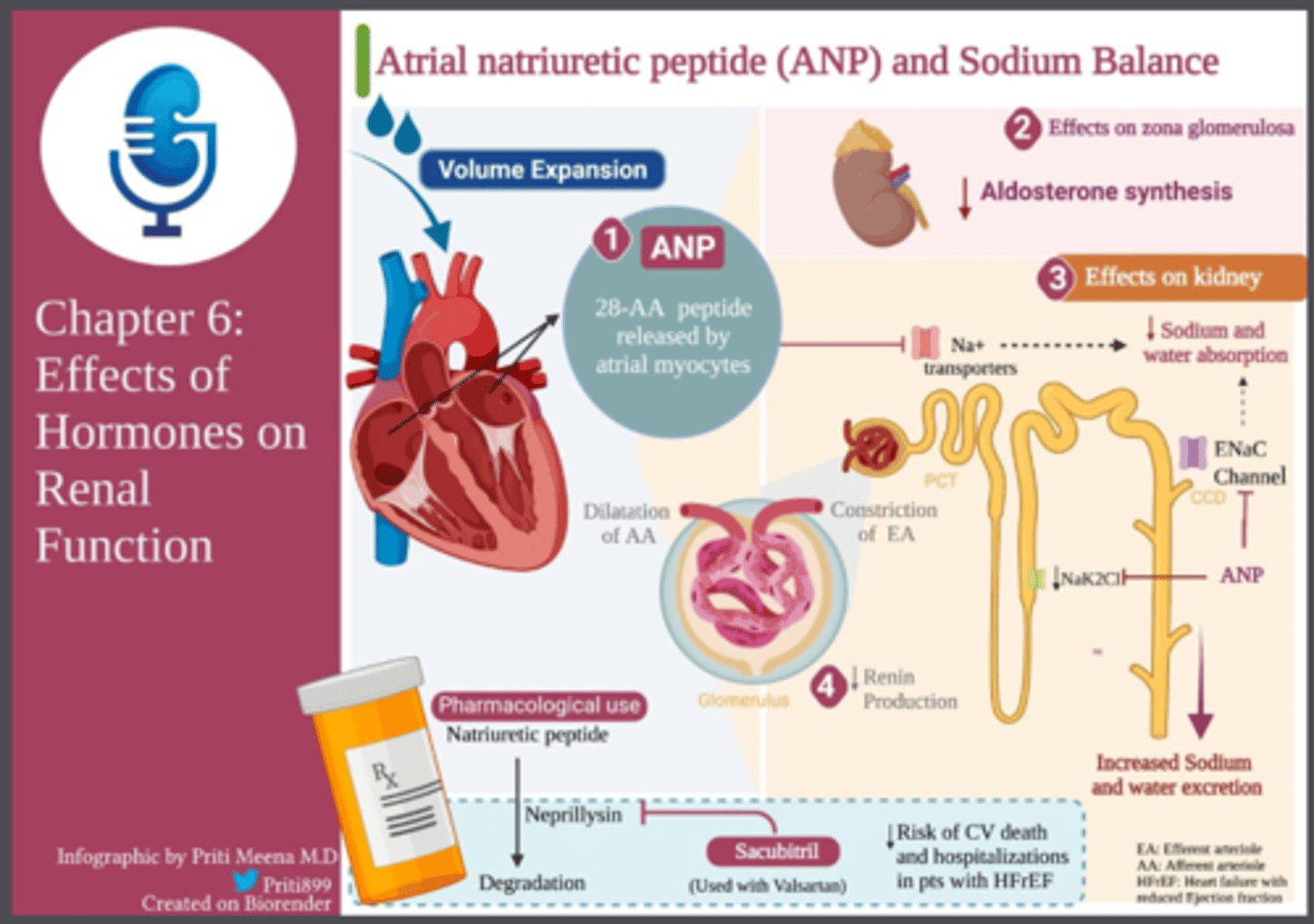
Which of the following statements accurately describe the roles of ADH, aldosterone, ANP, and BNP in fluid regulation?
A) ADH signals the kidneys to excrete water; aldosterone signals the kidneys for the reabsorption of potassium ions and water; ANP and BNP are secreted by the heart to increase fluid levels.
B) ADH signals the kidneys to promote reabsorption of water; aldosterone signals the kidneys for the reabsorption of sodium ions and water; ANP and BNP are secreted by the heart to assist with fluid level maintenance.
C) ADH signals the kidneys to excrete sodium; aldosterone signals the kidneys to decrease sodium absorption; ANP and BNP reduce fluid levels by promoting water excretion.
D) ADH signals the kidneys to excrete potassium; aldosterone signals the kidneys to increase water excretion; ANP and BNP are secreted by the liver to assist with fluid level maintenance.
B) ADH (anti-diuretic hormone) signals the kidneys to promote reabsorption of water; aldosterone signals the kidneys for the reabsorption of sodium ions and water; ANP and BNP (atrial natriuric peptide and B-type natriuric peptide) are secreted by the heart to assist with fluid level maintenance.
TRIPLE A!!
(thanks K!)
Why are elderly individuals at a higher risk of dehydration?
A) Increased physical activity and high water intake
B) Forgetting to drink water and diminished sense of taste
C) Increased renal function and improved thirst response
D) Enhanced absorption of water in the intestines
B) Forgetting to drink water and diminished sense of taste
What is the normal range for calcium (Ca²⁺) in the blood?
A) 3.5-5.0 mg/dL
B) 8.6-10 mg/dL
C) 135-145 mg/dL
D) 98-106 mg/dL
B) 8.6-10 mg/dL
Which of the following are common causes of hypercalcemia?
A) Renal failure, alkalosis (increased serum pH), malabsorption syndrome
B) Increased milk and antacid intake, excessive vitamin D
C) Hyperparathyroidism, prolonged immobility, too many calcium and vitamin D supplements, severe dehydration, lithium, cancers of the bone, breast, and lungs
D) Hypoparathyroidism, chronic kidney disease, vitamin D deficiency
C) Hyperparathyroidism, prolonged immobility, too many calcium and vitamin D supplements, severe dehydration, lithium, cancers of the bone, breast, and lungs
What are the clinical manifestations of hypercalcemia?
A) Tetany, mental confusion, tingling fingers
B) High blood pressure, rapid heart rate, excessive sweating
C) Kidney stones, muscle weakness, bone pain, increased urinary output, arrhythmias, lethargy, palpitations, osteoporosis
D) Muscle cramps, dry skin, weight loss
C) Kidney stones, muscle weakness, bone pain, increased urinary output, arrhythmias, lethargy, palpitations, osteoporosis
What is the normal range for sodium (Na⁺) in the blood?
A) 3.5-5.0 mEq/L
B) 8.5-10 mg/dL
C) 135-145 mEq/L
D) 98-106 mEq/L
C) 135-145 mEq/L
Which of the following are common causes of hyponatremia?
A) Hyperglycemia, water deprivation, renal failure
B) Diuretics, vomiting, diarrhea, sweating (diaphoresis), Addison's disease
C) Increased salt intake, dehydration, hyperventilation
D) High protein diet, chronic kidney disease, liver failure
B) Diuretics, vomiting, diarrhea, sweating (diaphoresis), Addison's disease
What are the clinical manifestations of hyponatremia?
A) Headache, loss of consciousness, seizures, coma, nausea, vomiting, confusion, muscle cramps, and death
B) Dry mucous membranes, thirst, lethargy, altered level of consciousness
C) High blood pressure, rapid heart rate, excessive sweating
D) Nausea, vomiting, muscle weakness, confusion
A) Headache, loss of consciousness, seizures, coma, nausea, vomiting, confusion, muscle cramps, and death

What is the normal range for magnesium (Mg²⁺) in the blood?
A) 1.2-2.6 mg/dL
B) 3.5-5.0 mg/dL
C) 8.5-10 mg/dL
D) 135-145 mEq/L
Answer: A) 1.2-2.6 mg/dL
A) 1.2-2.6 mg/dL
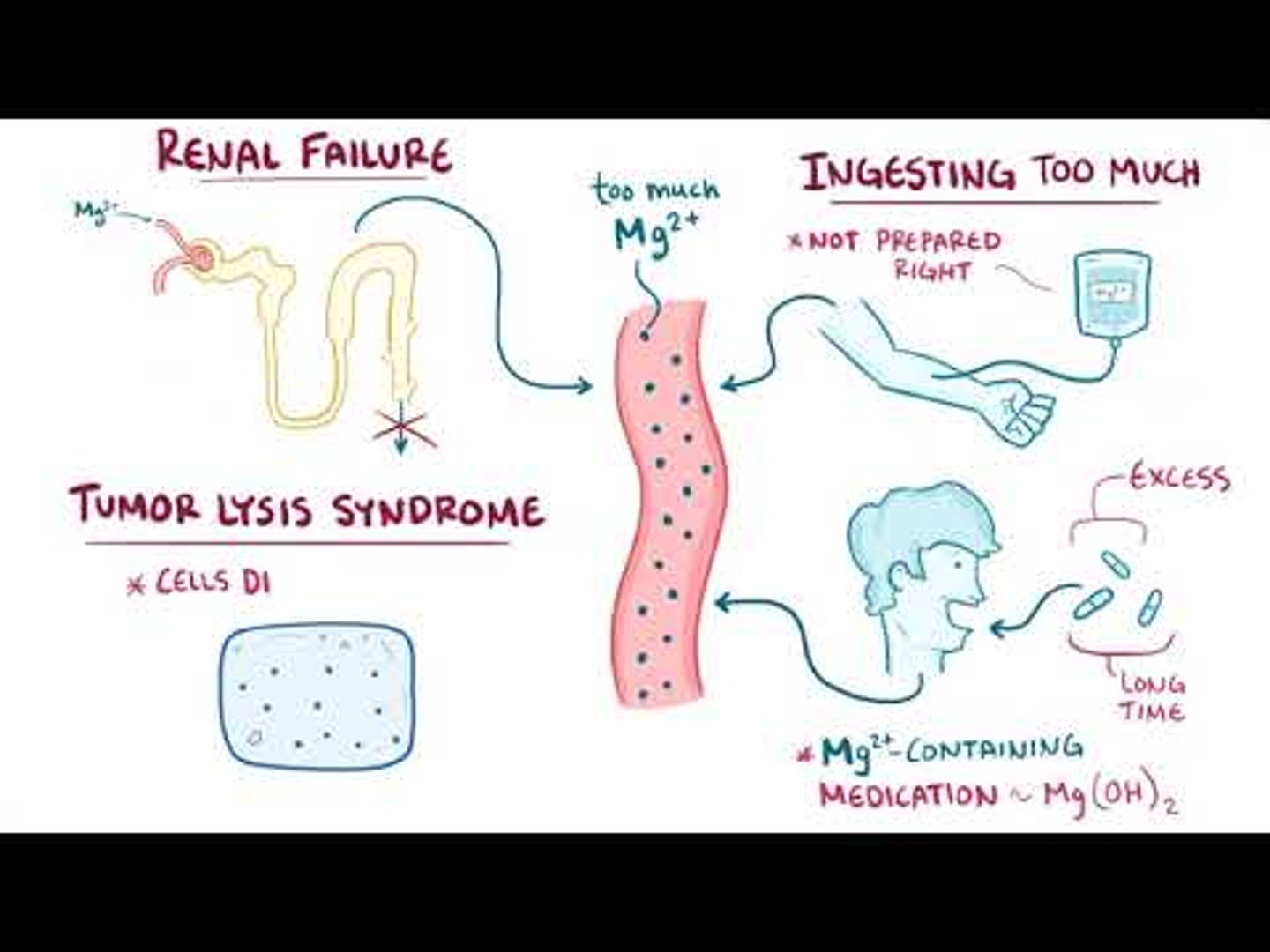
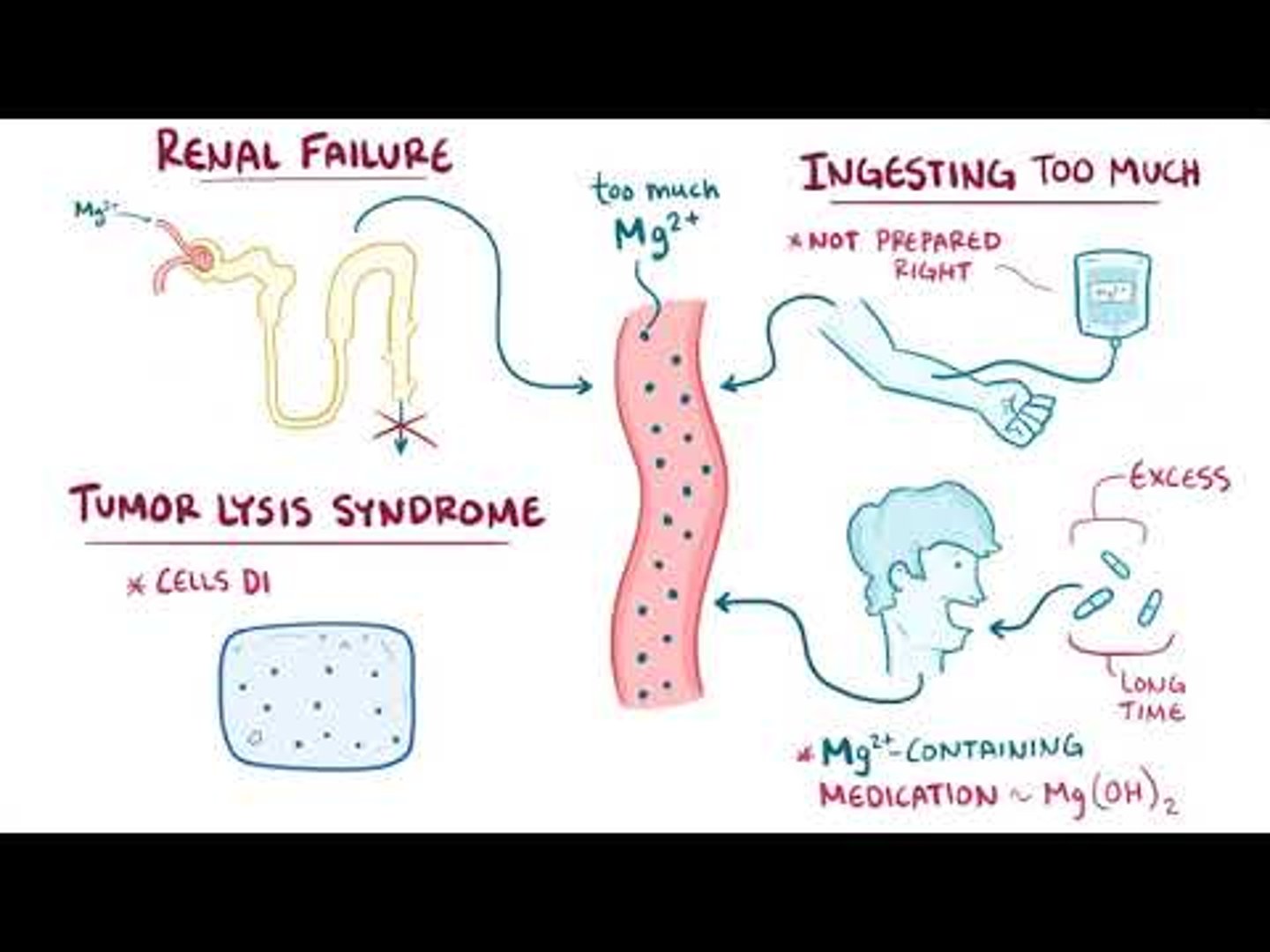
Which of the following are common causes of hypermagnesemia?
A) Poor magnesium intake, alcoholism, DKA, diuretics, hypokalemia, acidosis
B) Renal failure, laxatives, antacids, magnesium supplements, hypothyroidism
C) Low sodium intake, chronic kidney disease, liver failure
D) High calcium intake, prolonged bed rest, vitamin D deficiency
B) Renal failure, laxatives, antacids, magnesium supplements, hypothyroidism
What are the clinical manifestations of hypermagnesemia?
A) High blood pressure, rapid heart rate, excessive sweating
B) Tetany (positive Chvostek & Trousseau), hyperactive deep tendon reflexes, nausea, vomiting, lethargy, neuromuscular irritability, tremors
C) Lethargy, weakness, nausea, vomiting, decreased neuromuscular function, cardiac arrhythmias, decreased reflexes, respiratory depression
D) Muscle cramps, dry skin, weight loss
C) Lethargy, weakness, nausea, vomiting, decreased neuromuscular function, cardiac arrhythmias, decreased reflexes, respiratory depression

Which illness makes a person predisposed to hypermagnesemia?
A) Diabetes
B) Renal failure
C) Hypertension
D) Hyperthyroidism
B) Renal failure
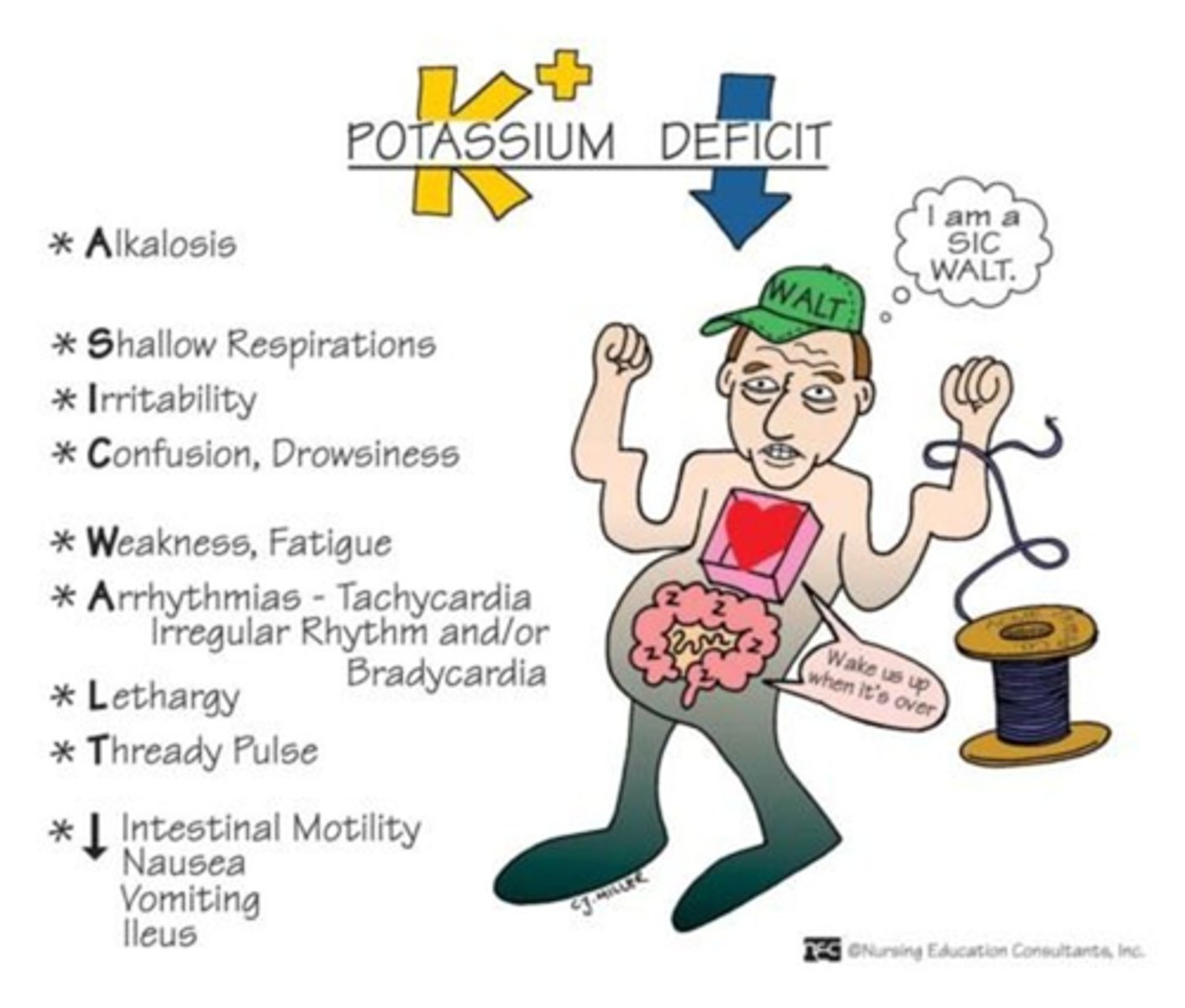
What are the clinical manifestations of hypokalemia?
A) Cardiac dysrhythmias, fatigue, heart block, anorexia, nausea, vomiting, decreased GI motility, muscle weakness, paresthesia
B) Cardiac dysrhythmias, peaked T waves, prolonged QT, muscle weakness, flaccid paralysis, increased GI motility
C) High blood pressure, rapid heart rate, excessive sweating
D) Nausea, vomiting, muscle weakness, confusion
A) Cardiac dysrhythmias, fatigue, heart block, anorexia, nausea, vomiting, decreased GI motility, muscle weakness, paresthesia
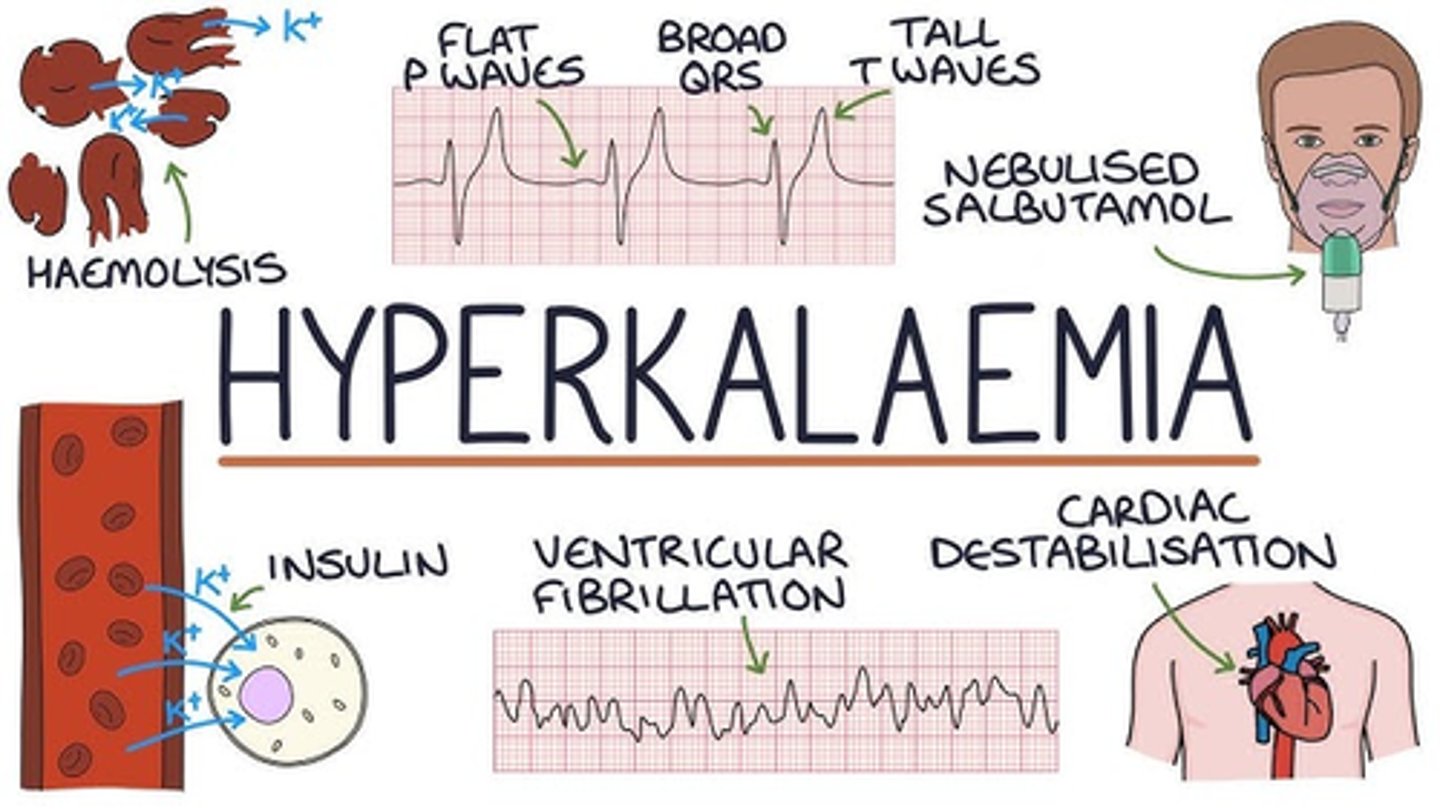
What are the clinical manifestations of hyperkalemia?
A) Cardiac dysrhythmias, fatigue, heart block, anorexia, nausea, vomiting, decreased GI motility, muscle weakness, paresthesia
B) Cardiac dysrhythmias, peaked T waves, prolonged QT, muscle weakness, flaccid paralysis, increased GI motility
C) High blood pressure, rapid heart rate, excessive sweating
D) Nausea, vomiting, muscle weakness, confusion
B) Cardiac dysrhythmias, peaked T waves, prolonged QT, muscle weakness, flaccid paralysis, increased GI motility
Which of the following are common causes of hypokalemia?
A) Renal failure, acidosis, ACE inhibitors, ARBs, beta blockers
B) Loop diuretics, vomiting, gastric suctioning, diarrhea, laxatives, corticosteroids, bulimia, hypomagnesemia, anorexia, Cushing's disease, DKA
C) Dehydration, high protein diet, hyperkalemia
D) Increased milk and antacid intake, excessive vitamin D
B) Loop diuretics, vomiting, gastric suctioning, diarrhea, laxatives, corticosteroids, bulimia, hypomagnesemia, anorexia, Cushing's disease, DKA
Which of the following are common causes of hyperkalemia?
A) Loop diuretics, vomiting, gastric suctioning, diarrhea, laxatives, corticosteroids, bulimia, hypomagnesemia, anorexia, Cushing's disease, DKA
B) Renal failure, acidosis, ACE inhibitors, ARBs, beta blockers, somatostatin, NSAIDs, heparin, lithium, oliguria, cirrhosis, adrenal insufficiency, Addison's disease, spironolactone
C) Low sodium intake, chronic kidney disease, liver failure
D) High calcium intake, prolonged bed rest, vitamin D deficiency
B) Renal failure, acidosis, ACE inhibitors, ARBs, beta blockers, somatostatin, NSAIDs, heparin, lithium, oliguria, cirrhosis, adrenal insufficiency, Addison's disease, spironolactone
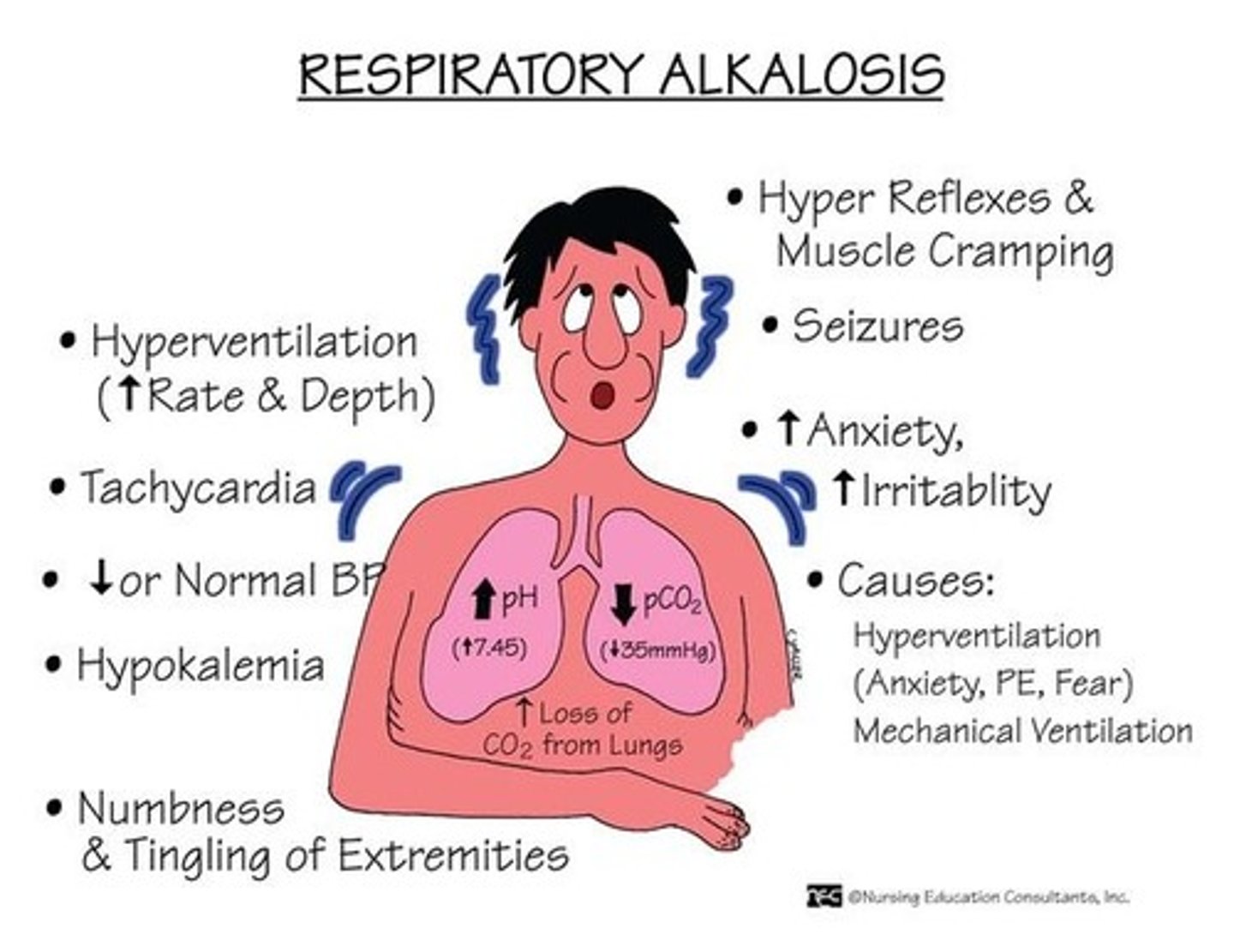
What arterial blood gas (ABG) change is commonly seen during an anxiety attack?
A) Metabolic acidosis
B) Metabolic alkalosis
C) Respiratory acidosis
D) Respiratory alkalosis
D) Respiratory alkalosis
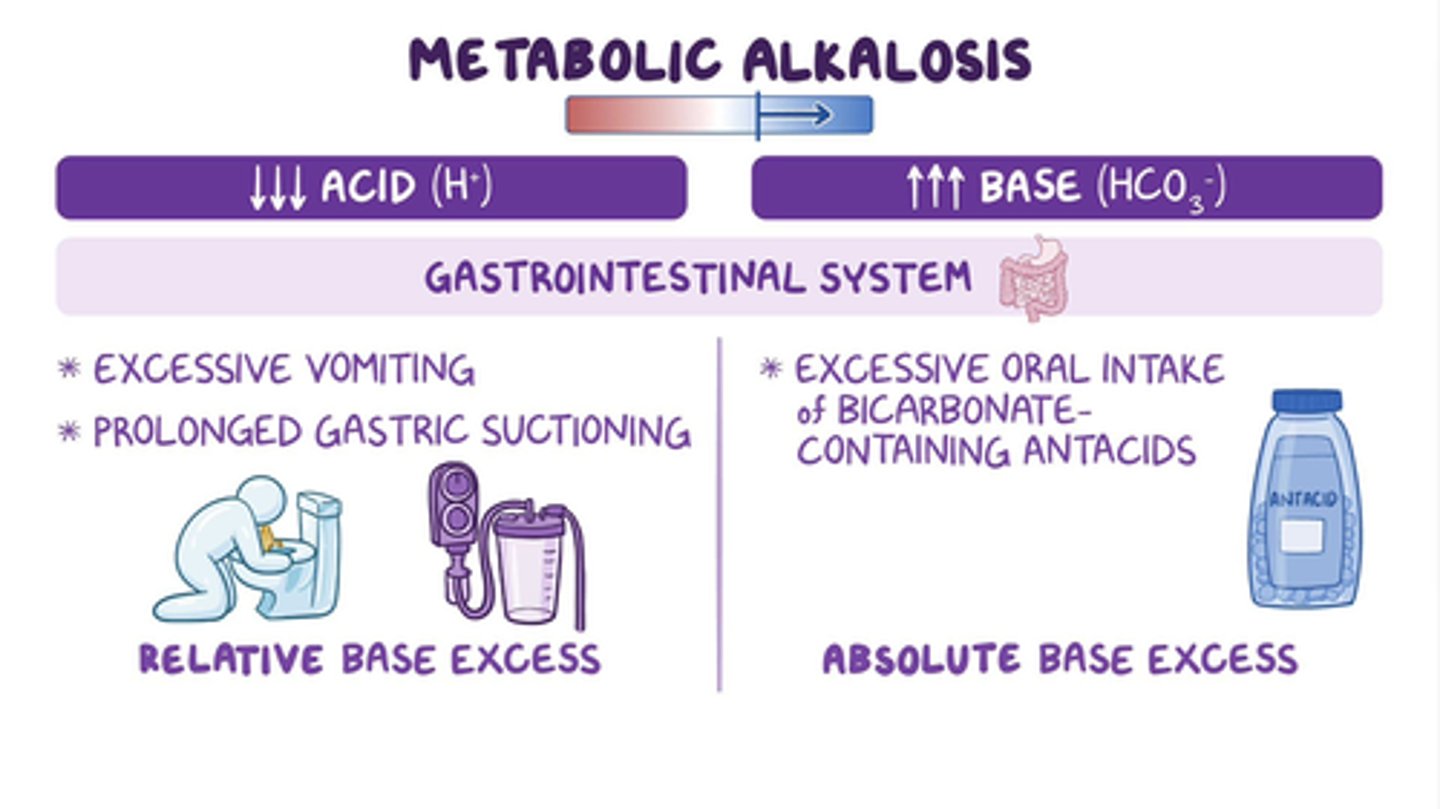
Which of the following situations may cause metabolic alkalosis?
A) Diarrhea, renal failure, diabetes ketoacidosis
B) Vomiting, nasogastric (NG) tube suctioning, excessive antacid use
C) Anxiety attack, hyperventilation, fever
D) Overhydration, SIADH, excessive water intake
B) Vomiting, nasogastric (NG) tube suctioning, excessive antacid use
What are the differences between incontinence and retention?
A) Incontinence is the inability to empty the bladder, while retention is the loss of voluntary control of the bladder.
B) Incontinence is the loss of voluntary control of the bladder, while retention is the inability to empty the bladder.
C) Incontinence is the increased frequency of urination, while retention is the decreased frequency of urination.
D) Incontinence and retention both refer to the complete inability to urinate.
B) Incontinence is the loss of voluntary control of the bladder, while retention is the inability to empty the bladder.
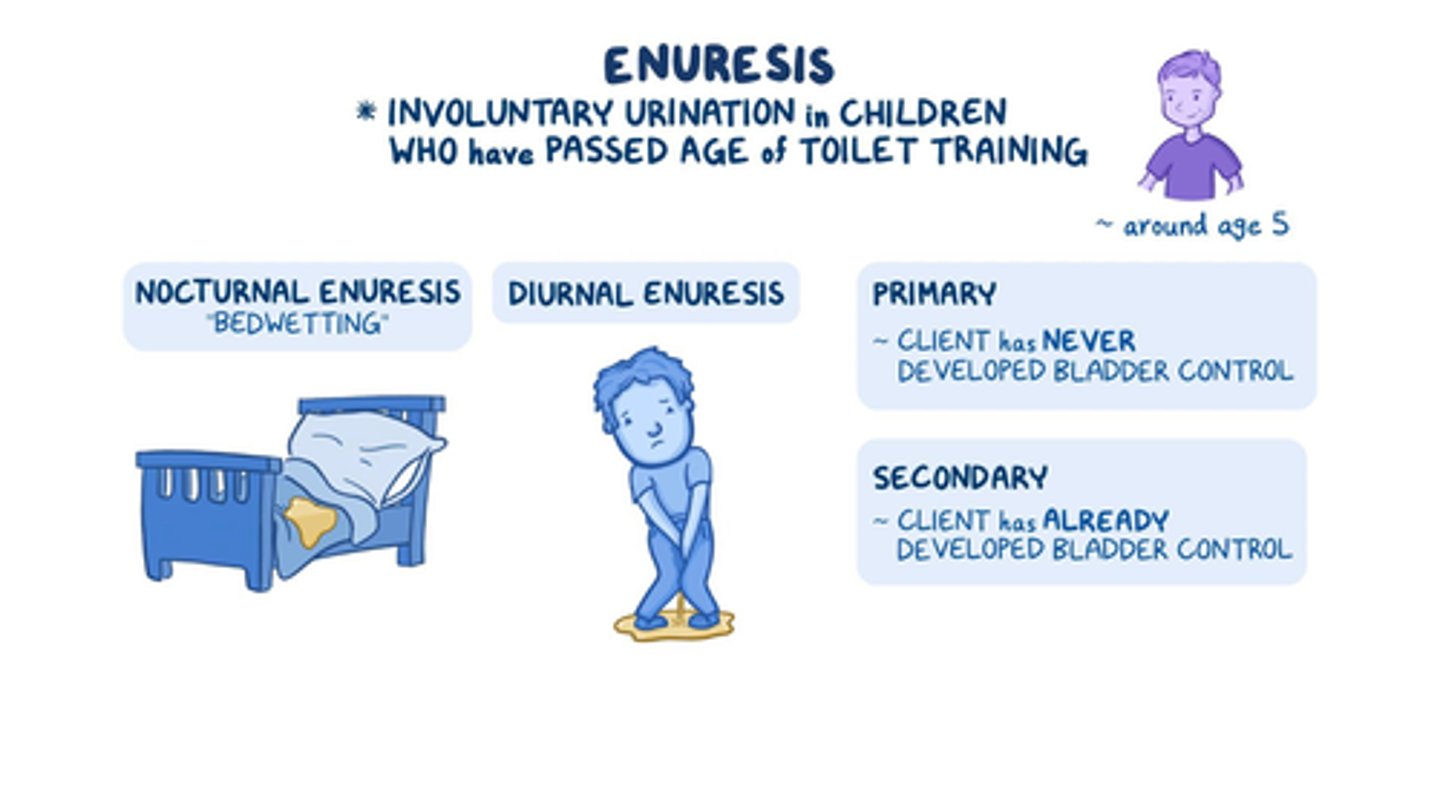
What is enuresis?
A) Involuntary urination by a child under 2 years old
B) Involuntary urination by a child over 4 years old
C) Increased intra-abdominal pressure forcing urine through the urinary sphincter
D) Incompetent bladder sphincter leading to overflow of urine
B) Involuntary urination by a child over 4 years old
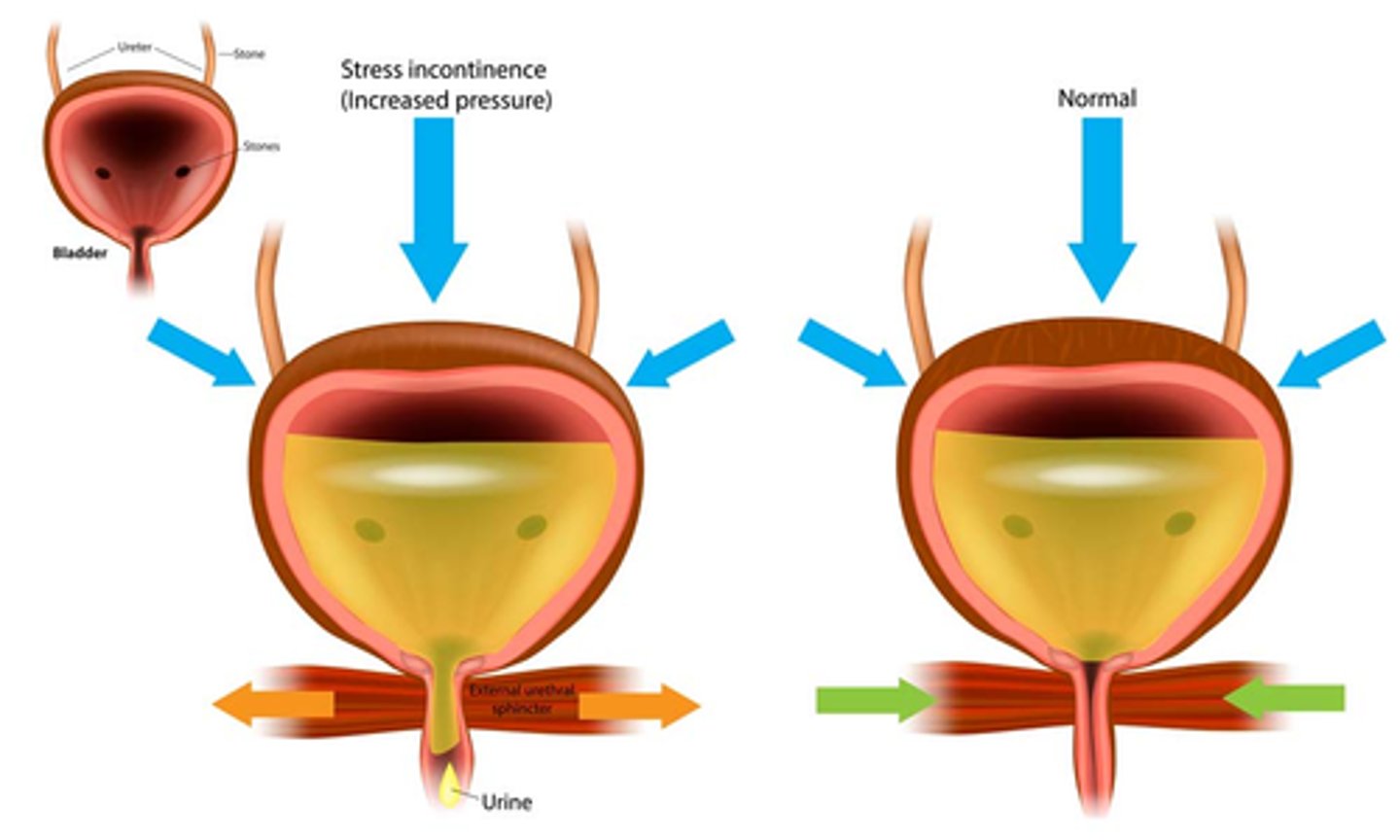
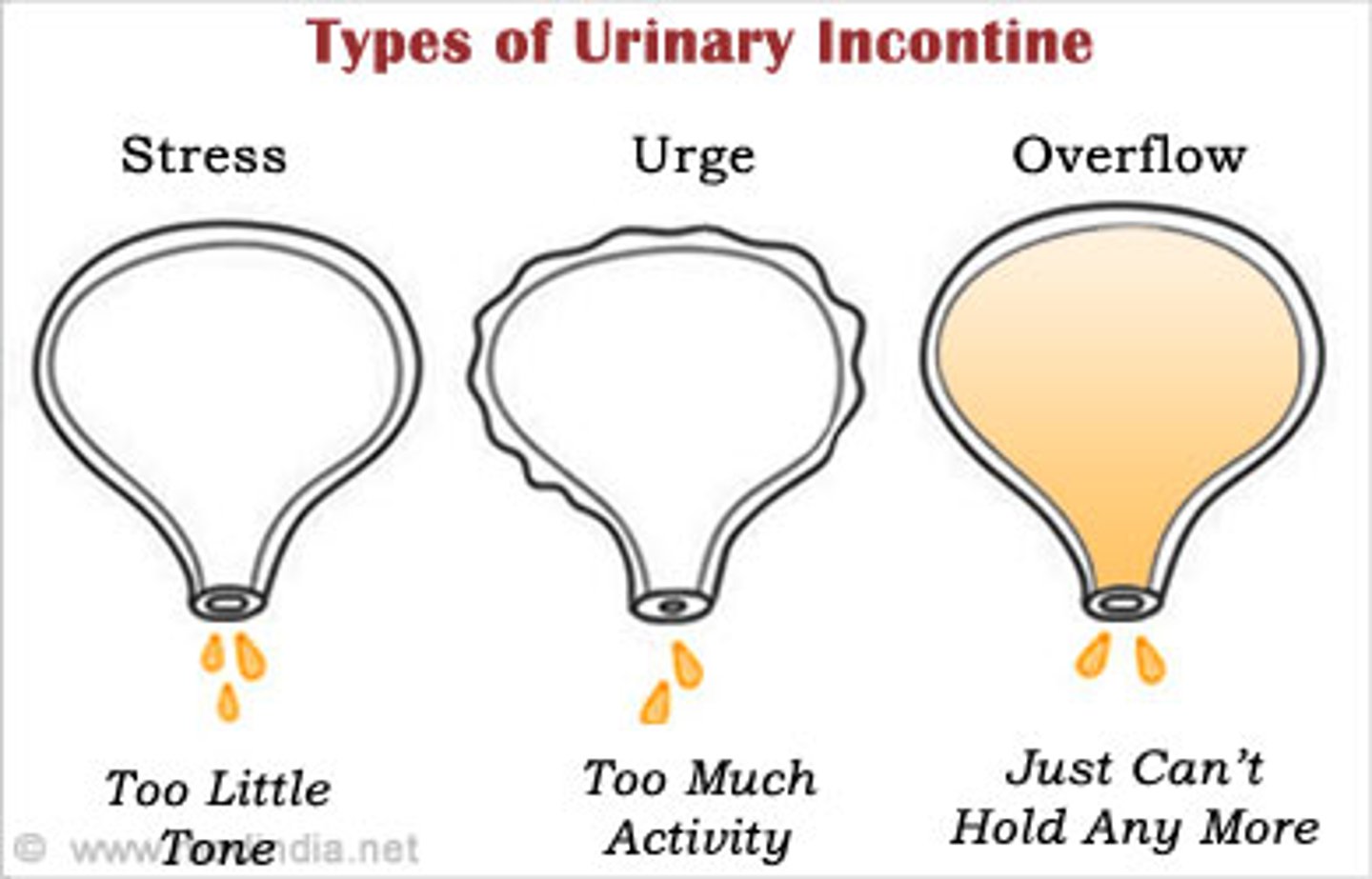
What is stress incontinence?
A) Involuntary urination due to a weak bladder muscle
B) Increased intra-abdominal pressure forcing urine through the urinary sphincter, more common in women, often triggered by activities like coughing, lifting, sneezing, laughing, and pregnancy
C) Involuntary urination by a child over 4 years old
D) Incompetent bladder sphincter leading to overflow of urine
B) Increased intra-abdominal pressure forcing urine through the urinary sphincter, more common in women, often triggered by activities like coughing, lifting, sneezing, laughing, and pregnancy
What is overflow incontinence?
A) Involuntary urination due to psychological stress
B) Involuntary urination by a child over 4 years old
C) Incompetent bladder sphincter leading to overflow of urine, often seen in older adults and those with spinal cord or brain injuries
D) Increased intra-abdominal pressure forcing urine through the urinary sphincter
C) Incompetent bladder sphincter leading to overflow of urine, often seen in older adults and those with spinal cord or brain injuries
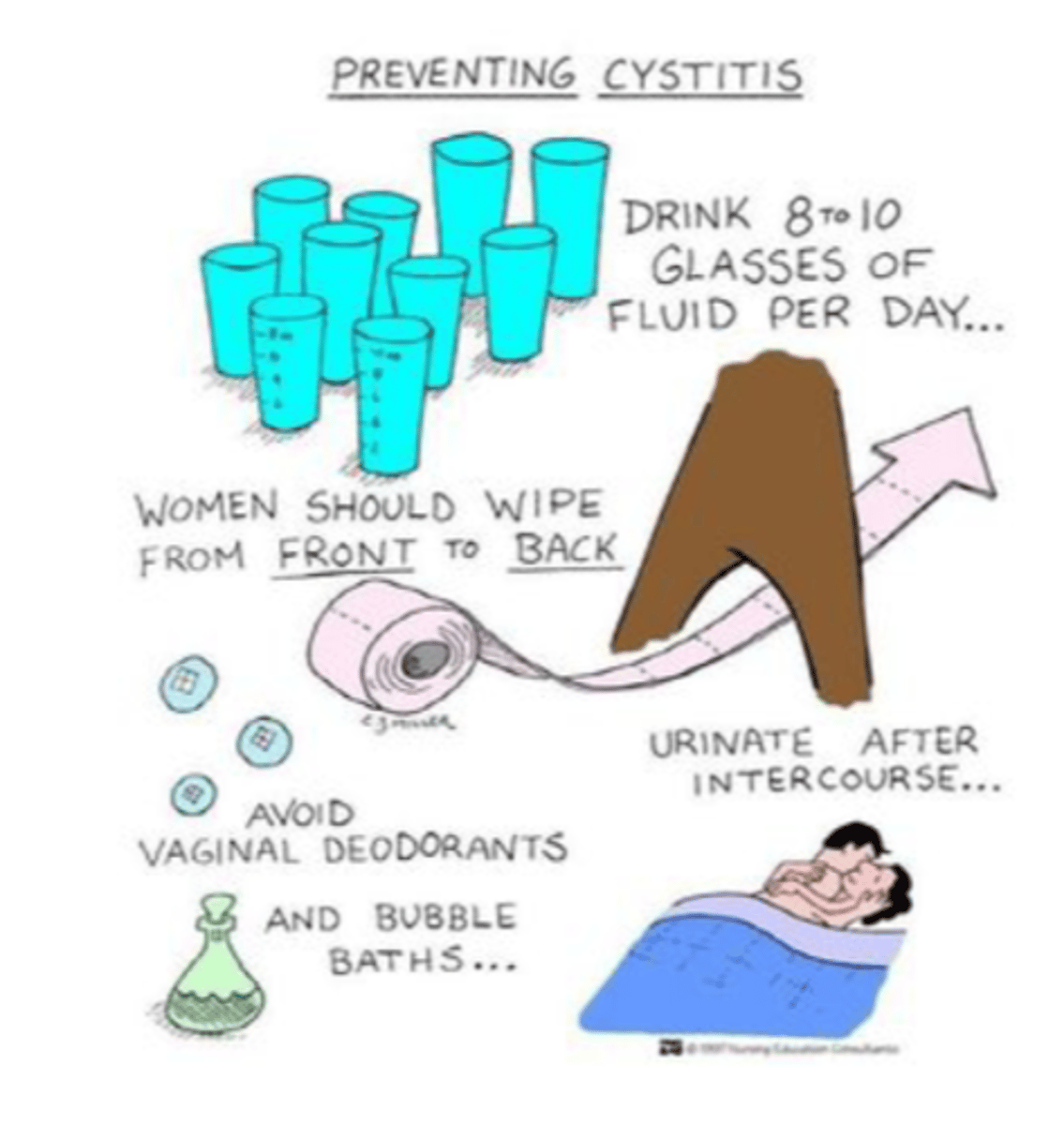
Which of the following are effective prevention methods for urinary tract infections/cystitis (UTIs)?
A) Clean front to back, urinate before and after sex, wear loose-fitting clothes, drink lots of water
B) Clean back to front, avoid urinating after sex, wear tight-fitting clothes
C) Clean front to back, urinate before and after sex, wear tight-fitting clothes
D) Clean back to front, urinate only before sex, wear loose-fitting clothes
A) Clean front to back, urinate before and after sex, wear loose-fitting clothes, drink lots of water
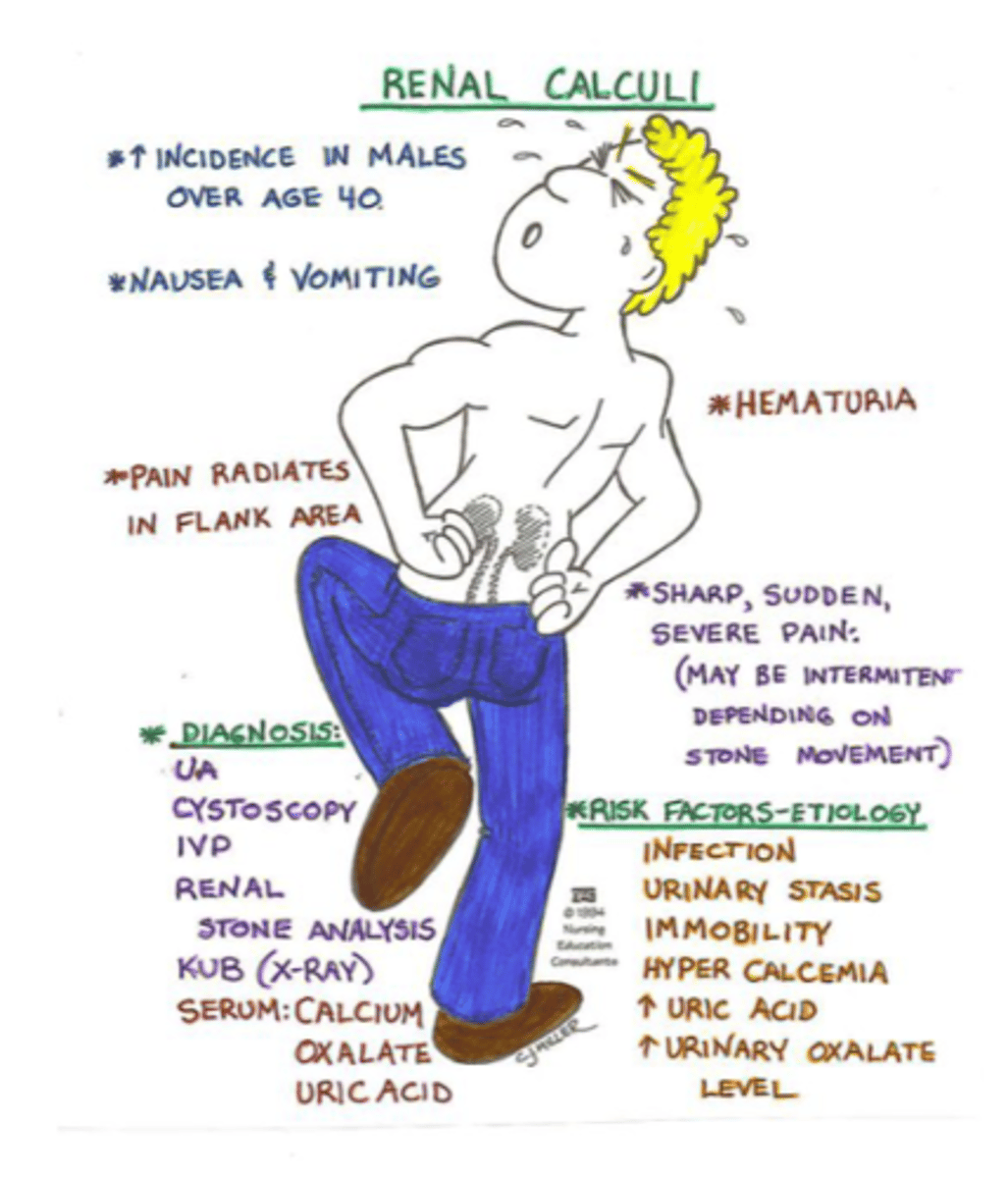
Which of the following descriptions accurately match the types and causes of kidney stones?
A) Hypercalcemia stones: caused by low urine calcium levels, form readily with acidic urine; Uric acid stones: caused by a low-purine diet, form easily with highly alkaline urine
B) Hypercalcemia stones: caused by high urine calcium levels, form readily with highly alkaline urine; Uric acid stones: caused by gout, high-purine diet (red meat, alcohol), or chemotherapy, form easily with acidic urine
C) Hypercalcemia stones: caused by low urine calcium levels, form readily with highly alkaline urine; Uric acid stones: caused by gout, low-purine diet, or chemotherapy, form easily with acidic urine
D) Hypercalcemia stones: caused by high urine calcium levels, form readily with acidic urine; Uric acid stones: caused by high-purine diet (red meat, alcohol), or chemotherapy, form easily with highly alkaline urine
B) Hypercalcemia stones: caused by high urine calcium levels, form readily with highly alkaline urine; Uric acid stones: caused by gout, high-purine diet (red meat, alcohol), or chemotherapy, form easily with acidic urine
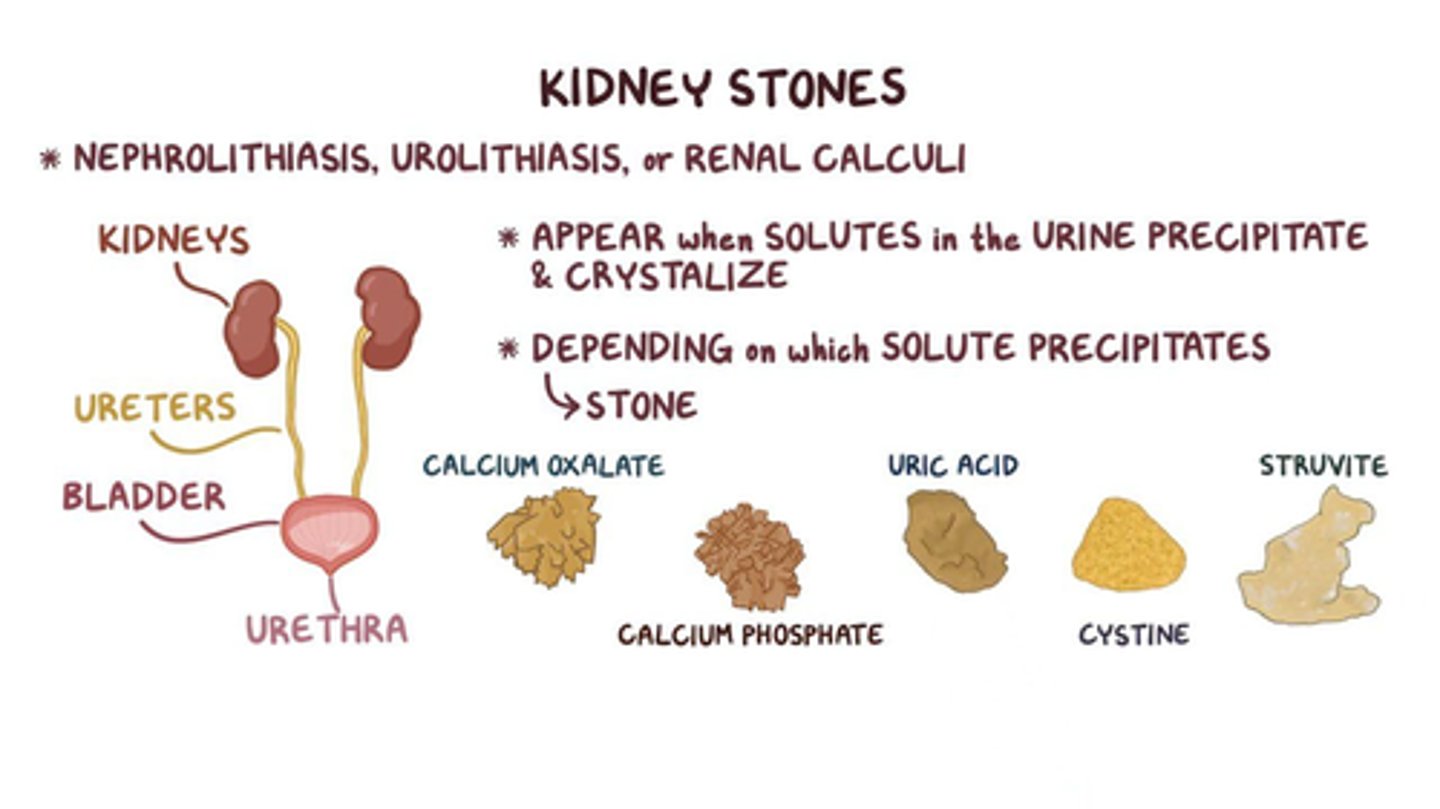
Which of the following are common causes of renal stones (calculi)?
A) Dehydration, hypercalcemia, and increased uric acid
B) Hyperglycemia, hypotension, and hypokalemia
C) Sodium and chloride deficiency
D) Iron and copper excess
A) Dehydration, hypercalcemia, and increased uric acid
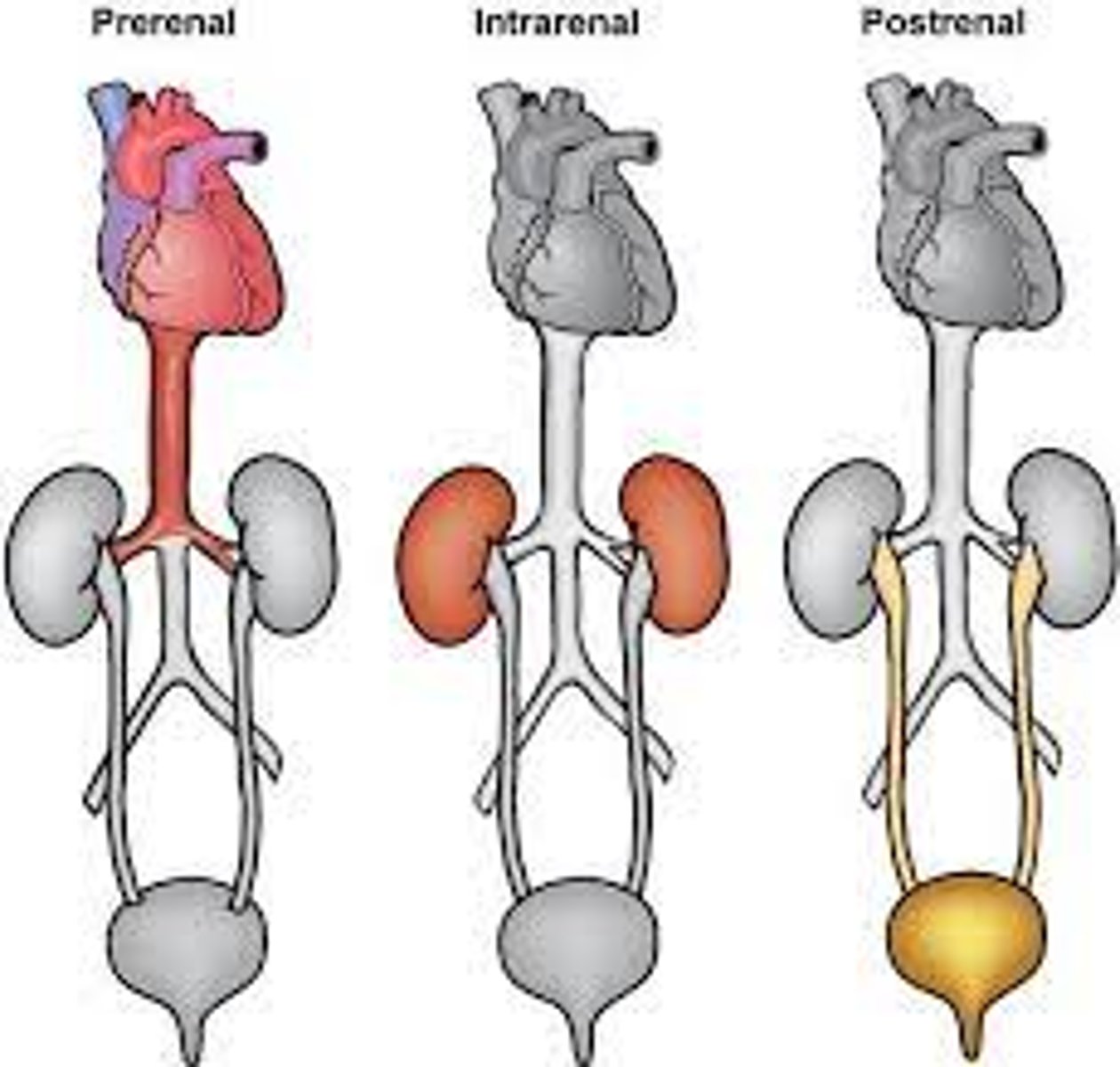
What is the primary cause of pre-renal failure?
A) Direct damage to the kidney tissues from infection or contrast dyes
B) Urine outflow obstruction like benign prostate hypertrophy or kidney stones
C) Lack of perfusion (blood flow), such as from a myocardial infarction (MI)
D) Chronic dehydration and electrolyte imbalances
C) Lack of perfusion (blood flow), such as from a myocardial infarction (MI)
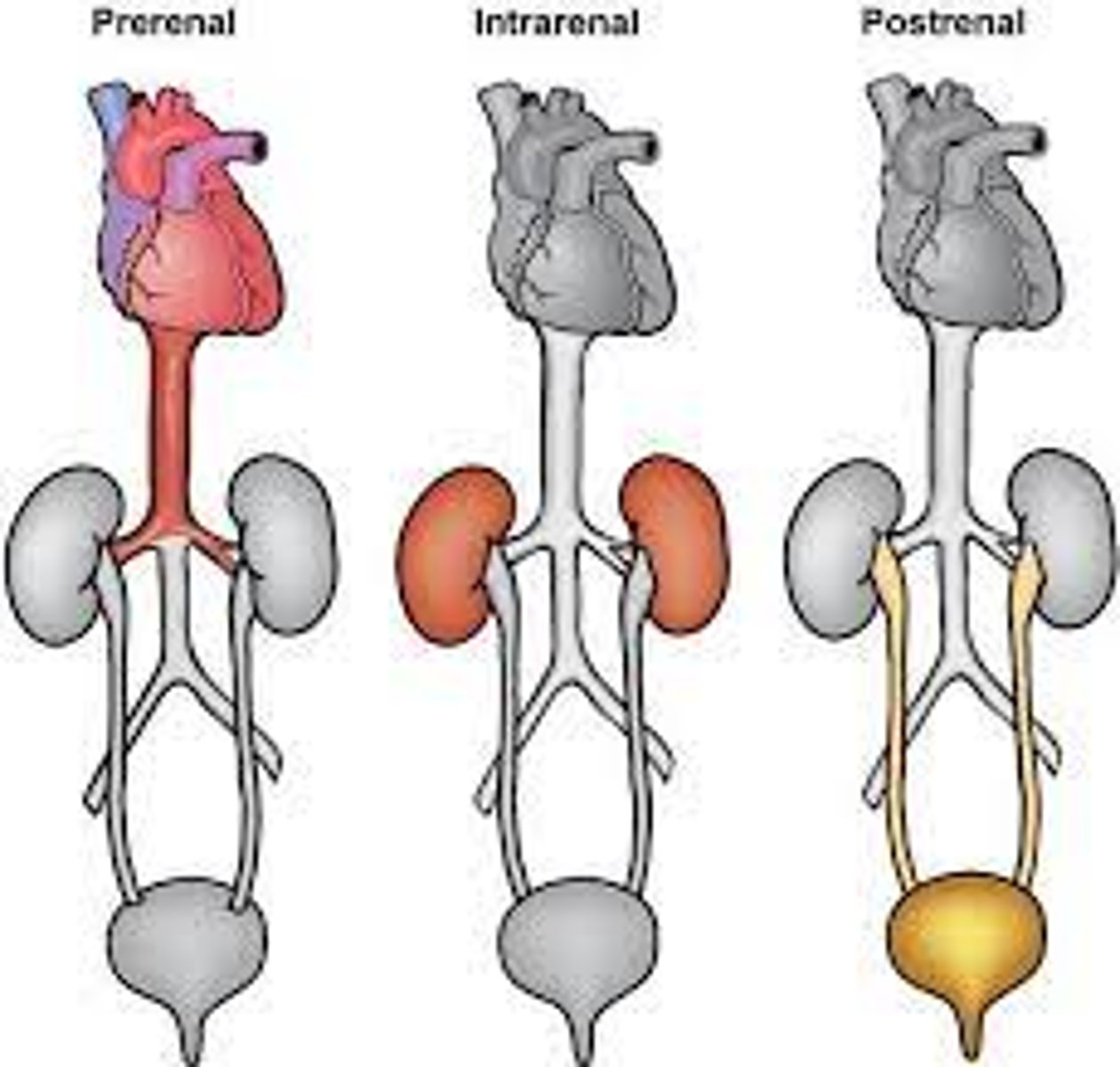
What is the primary cause of intra-renal failure?
A) Lack of perfusion (blood flow), such as from a myocardial infarction (MI)
B) Direct damage to the kidney tissues, which could be from infection, contrast dyes used in CT scans, or medication
C) Urine outflow obstruction like benign prostate hypertrophy or kidney stones
D) Chronic dehydration and electrolyte imbalances
B) Direct damage to the kidney tissues, which could be from infection, contrast dyes used in CT scans, or medication
inside the kidney
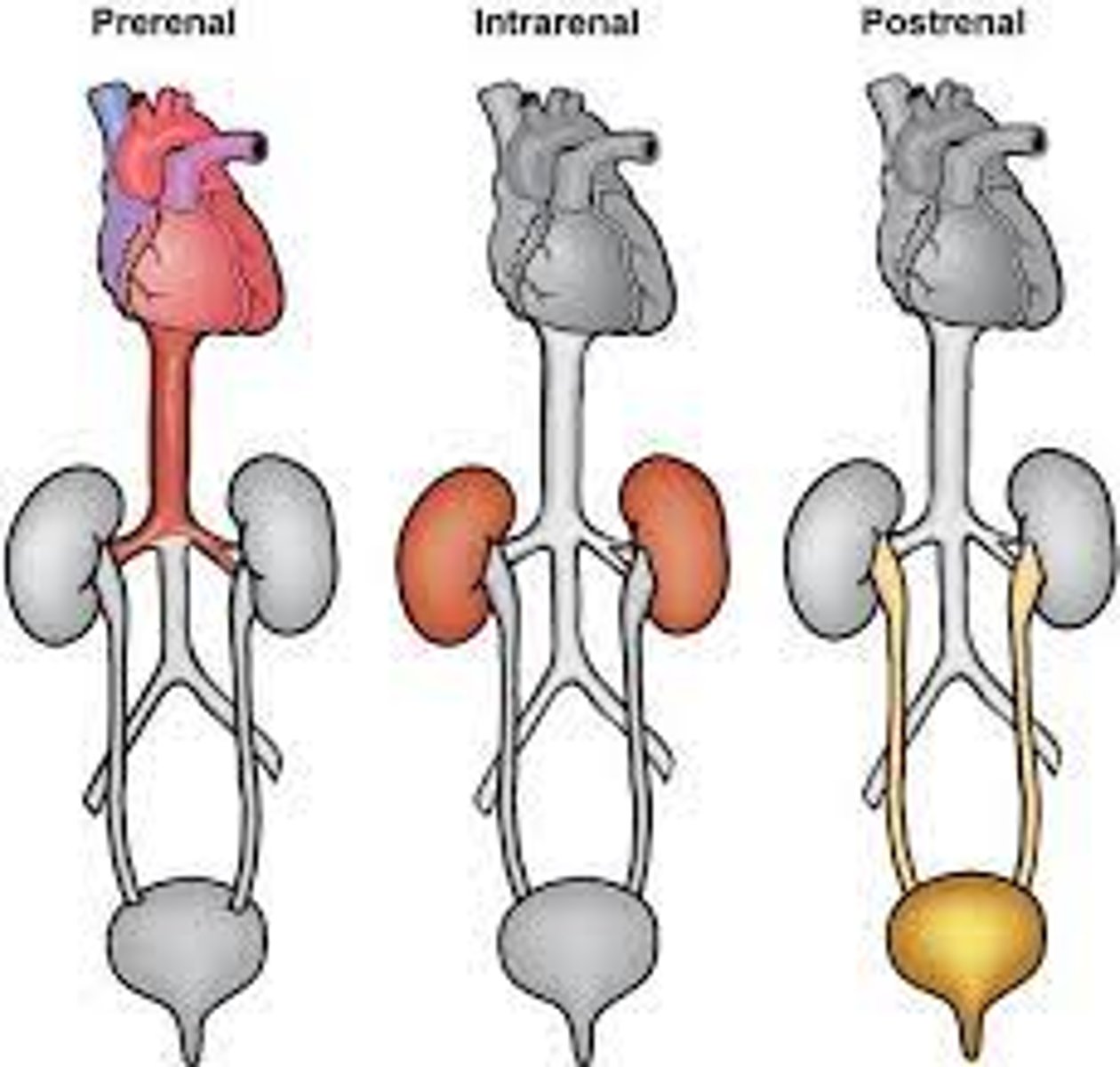
What is the primary cause of post-renal failure?
A) Direct damage to the kidney tissues from infection or contrast dyes
B) Urine outflow obstruction, such as benign prostate hypertrophy, renal calculi (kidney stones), or prostate issues (e.g., TURP)
C) Lack of perfusion (blood flow), such as from a myocardial infarction (MI)
D) Chronic dehydration and electrolyte imbalances
B) Urine outflow obstruction, such as benign prostate hypertrophy, renal calculi (kidney stones), or prostate issues (e.g., TURP)
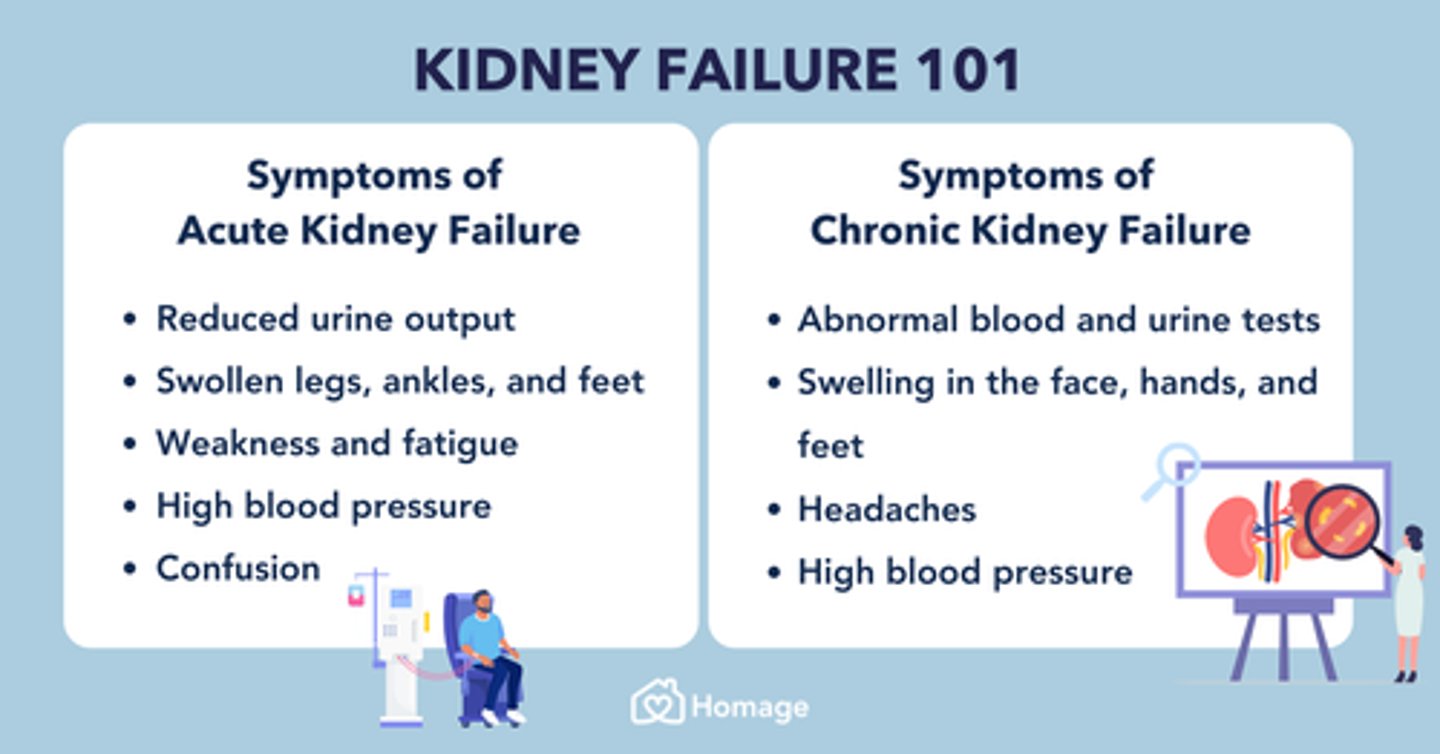
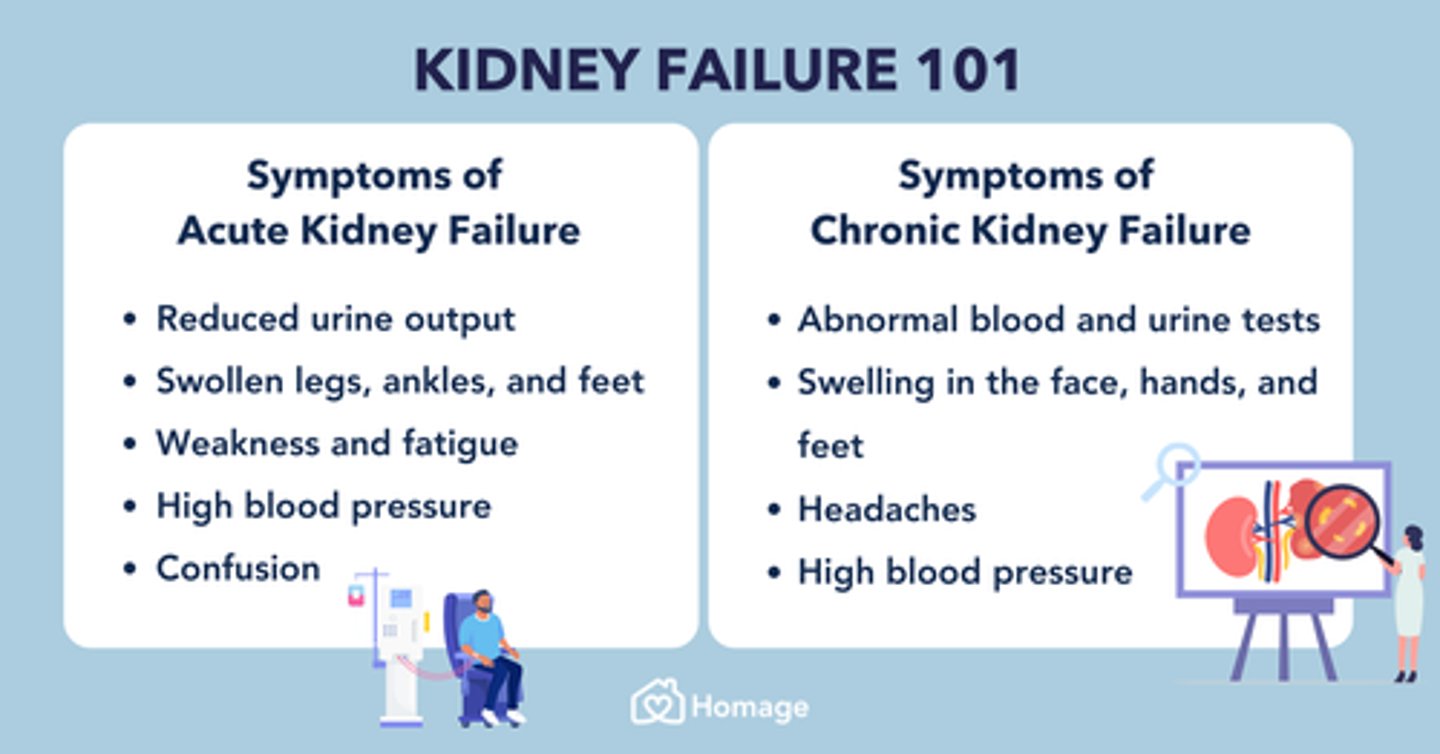
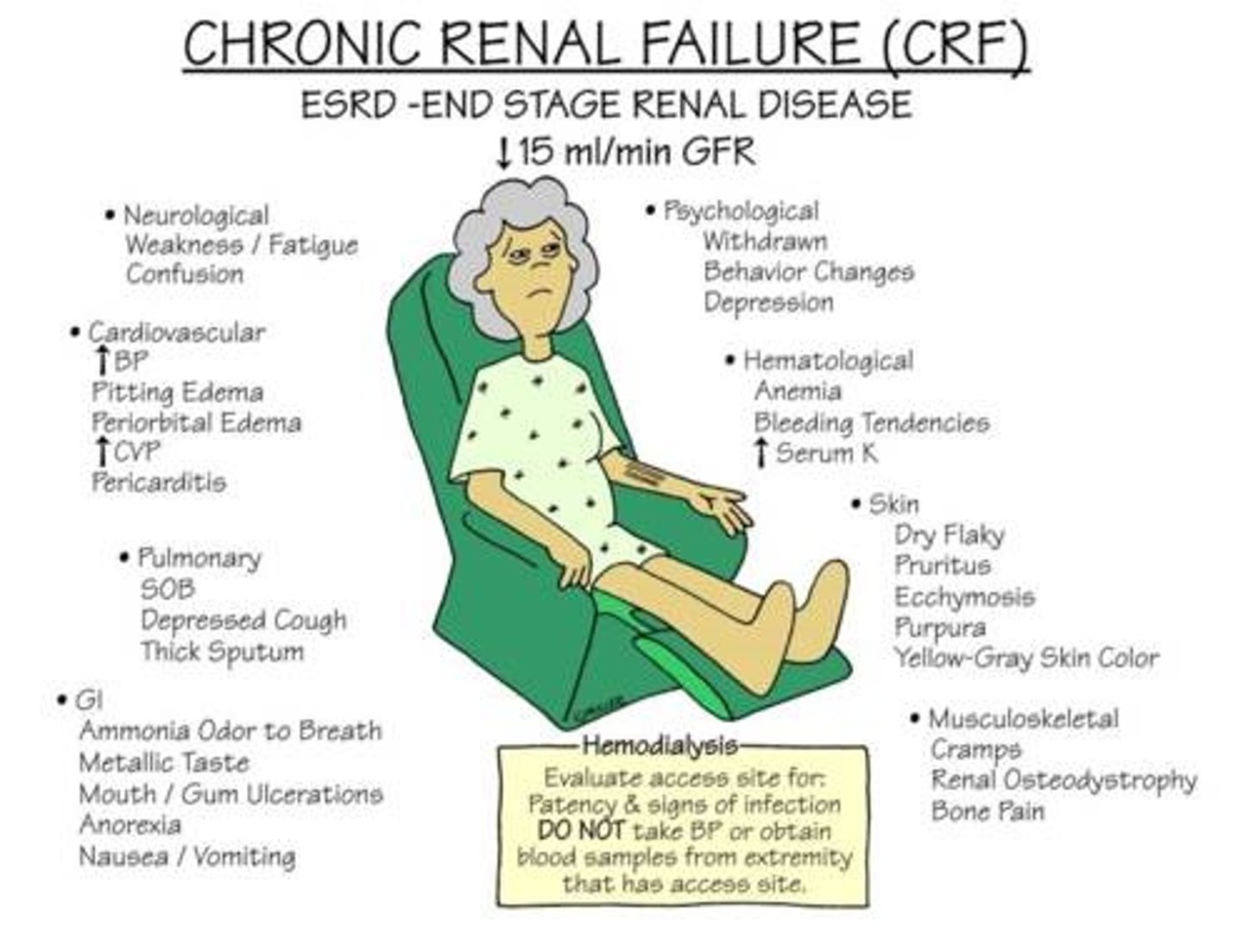
What are the early clinical manifestations of chronic renal failure?
A) Increased blood pressure and urinary output, anorexia, nausea, anemia, fatigue, unintended weight loss, exercise intolerance, bone marrow depression, and impaired cell function
B) Anuria/oliguria, dry pruritic hyperpigmented skin, peripheral neuropathy, encephalopathy
C) High blood pressure, rapid heart rate, excessive sweating
D) Nausea, vomiting, muscle weakness, confusion
A) Increased blood pressure and urinary output, anorexia, nausea, anemia, fatigue, unintended weight loss, exercise intolerance, bone marrow depression, and impaired cell function
What are the end-stage clinical manifestations of chronic renal failure?
A) Increased blood pressure and urinary output, anorexia, nausea, anemia, fatigue, unintended weight loss, exercise intolerance, bone marrow depression, and impaired cell function
B) Anuria/oliguria, dry pruritic hyperpigmented skin, peripheral neuropathy, encephalopathy, congestive heart failure, dysrhythmias, failure to activate vitamin D, systemic infections
C) High blood pressure, rapid heart rate, excessive sweating
D) Nausea, vomiting, muscle weakness, confusion
B) Anuria/oliguria, dry pruritic hyperpigmented skin, peripheral neuropathy, encephalopathy, congestive heart failure, dysrhythmias, failure to activate vitamin D, systemic infections
Which of the following are recommended treatments and nursing care practices for a patient with dysphagia?
A) If due to a food bolus, an EGD can be performed to remove it; If due to a neurological issue (e.g., stroke): chin to chest when swallowing, sit up 90 degrees when eating/drinking, no straws, thickened liquids as directed, chopped/ground food as directed, alternate bites & sips
B) Heimlich maneuver for food bolus, tilt head back when swallowing, lie down when eating, use straws, thin liquids, large solid food pieces, avoid alternating bites & sips
C) Drink water for food bolus, lean to the side when swallowing, sit up 45 degrees, no restrictions on straws, thickened liquids only when necessary, pureed food only, avoid alternating bites & sips
D) EGD for food bolus removal, tilt head back when swallowing, sit up 90 degrees, use straws, thin liquids, small solid food pieces, alternate bites & sips
A) If due to a food bolus, an EGD can be performed to remove it; If due to a neurological issue (e.g., stroke): chin to chest when swallowing, sit up 90 degrees when eating/drinking, no straws, thickened liquids as directed, chopped/ground food as directed, alternate bites & sips
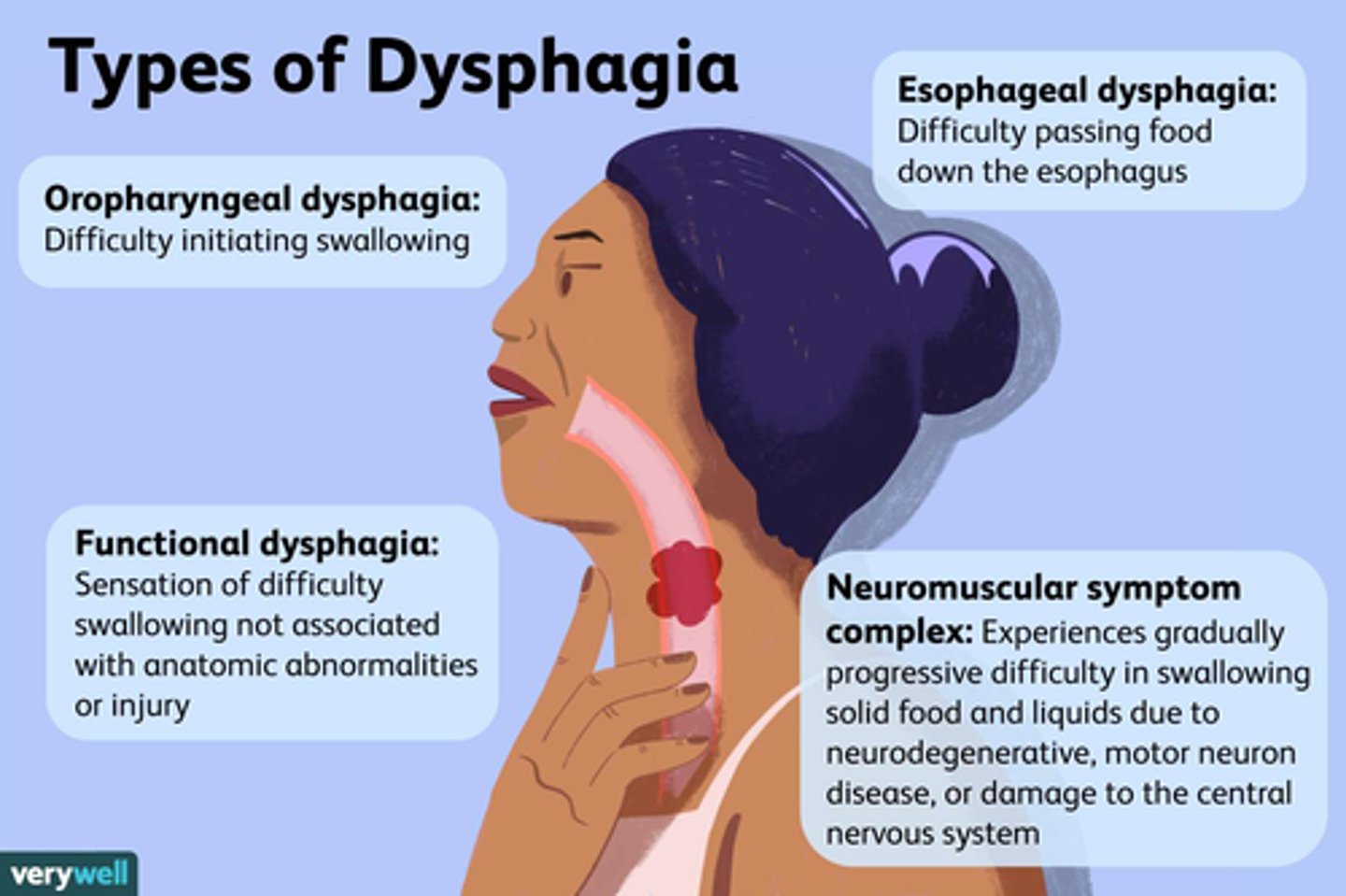
What are the potential complications of dysphagia if left untreated?
A) Aspiration, pneumonia, sepsis, death
B) Dehydration, kidney stones, liver failure, death
C) Weight gain, high blood pressure, heart attack, death
D) Muscle cramps, joint pain, arthritis, death
A) Aspiration, pneumonia, sepsis, death
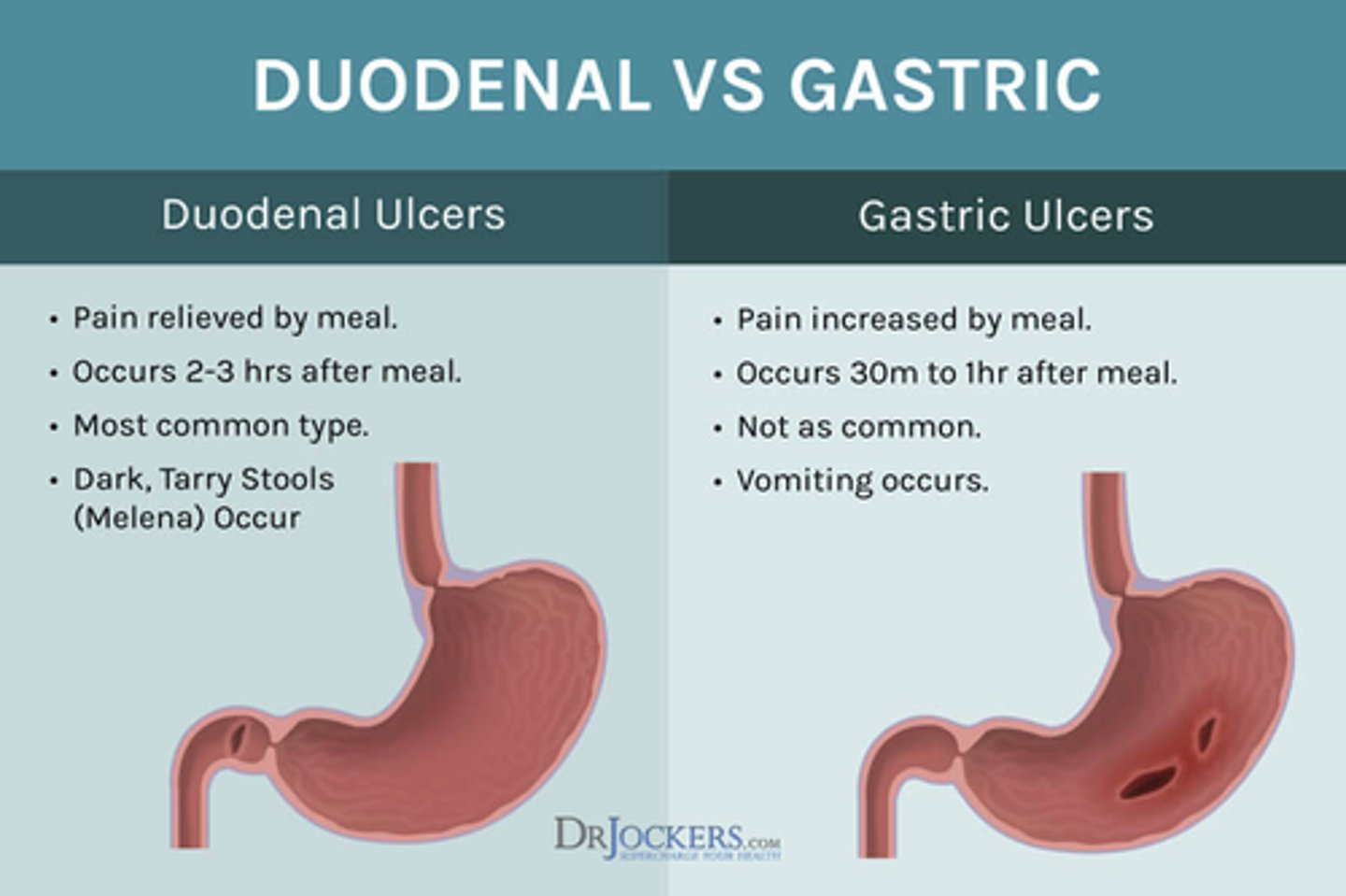
Which of the following correctly matches the timing of burning/aching pain with the type of ulcer?
A) Burning/aching pain immediately after drinking = duodenal ulcer; Burning/aching pain 2-3 hours after eating = gastric ulcer
B) Burning/aching pain immediately after drinking = gastric ulcer; Burning/aching pain 2-3 hours after eating = duodenal ulcer
C) Burning/aching pain immediately after eating = duodenal ulcer; Burning/aching pain 2-3 hours after drinking = gastric ulcer
D) Burning/aching pain immediately after eating = gastric ulcer; Burning/aching pain 2-3 hours after eating = duodenal ulcer
B) Burning/aching pain immediately after drinking = gastric ulcer; Burning/aching pain 2-3 hours after eating = duodenal ulcer
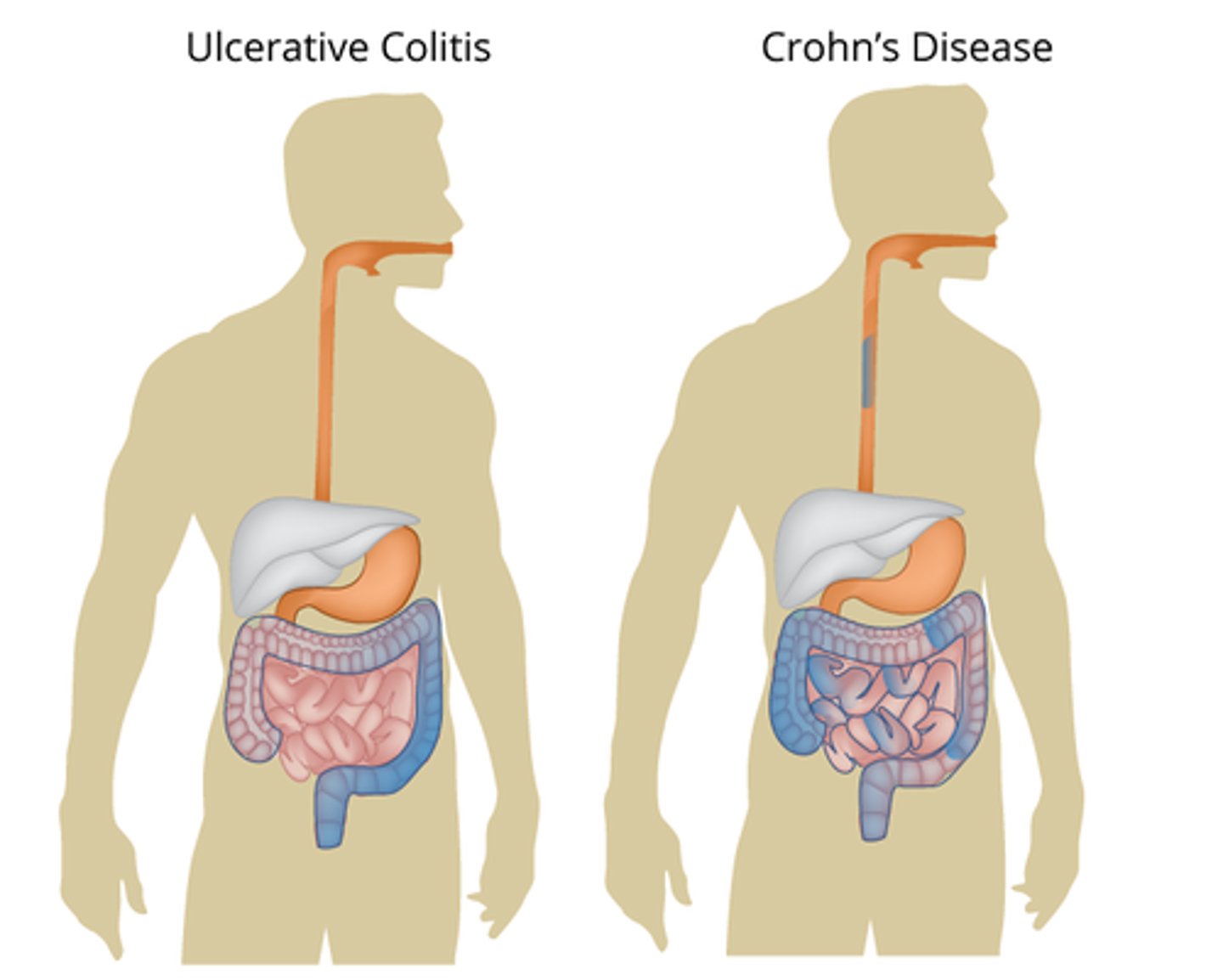
Which of the following correctly describes the characteristics of Crohn’s disease and ulcerative colitis?
A) Crohn’s disease: autoimmune disorder causing ulcerations in the rectum and large intestine; Ulcerative colitis: autoimmune disorder causing skip lesions anywhere from mouth to rectum
B) Crohn’s disease: autoimmune disorder causing skip lesions with a cobblestone appearance anywhere from mouth to rectum; Ulcerative colitis: autoimmune disorder causing ulcerations in the rectum and large intestine
C) Crohn’s disease: bacterial infection causing skip lesions anywhere from mouth to rectum; Ulcerative colitis: bacterial infection causing ulcerations in the rectum and large intestine
D) Crohn’s disease: autoimmune disorder causing continuous lesions in the small intestine; Ulcerative colitis: autoimmune disorder causing ulcerations in the stomach and small intestine
B) Crohn’s disease: autoimmune disorder causing skip lesions with a cobblestone appearance anywhere from mouth to rectum; Ulcerative colitis: autoimmune disorder causing ulcerations in the rectum and large intestine
What is a critical step in treating a patient with a perforated appendix before an appendectomy?
A) Administering pain medication
B) Providing a full dose of antibiotics
C) Performing immediate surgery without antibiotics
D) Giving fluids and monitoring vital signs
B) Providing a full dose of antibiotics
What are the potential complications of an untreated perforated appendix?
A) Dehydration, kidney failure, death
B) Infection, scarring, chronic pain
C) Perforation, peritonitis, sepsis, death
D) Perforation, sepsis, liver failure
C) Perforation, peritonitis, sepsis, death
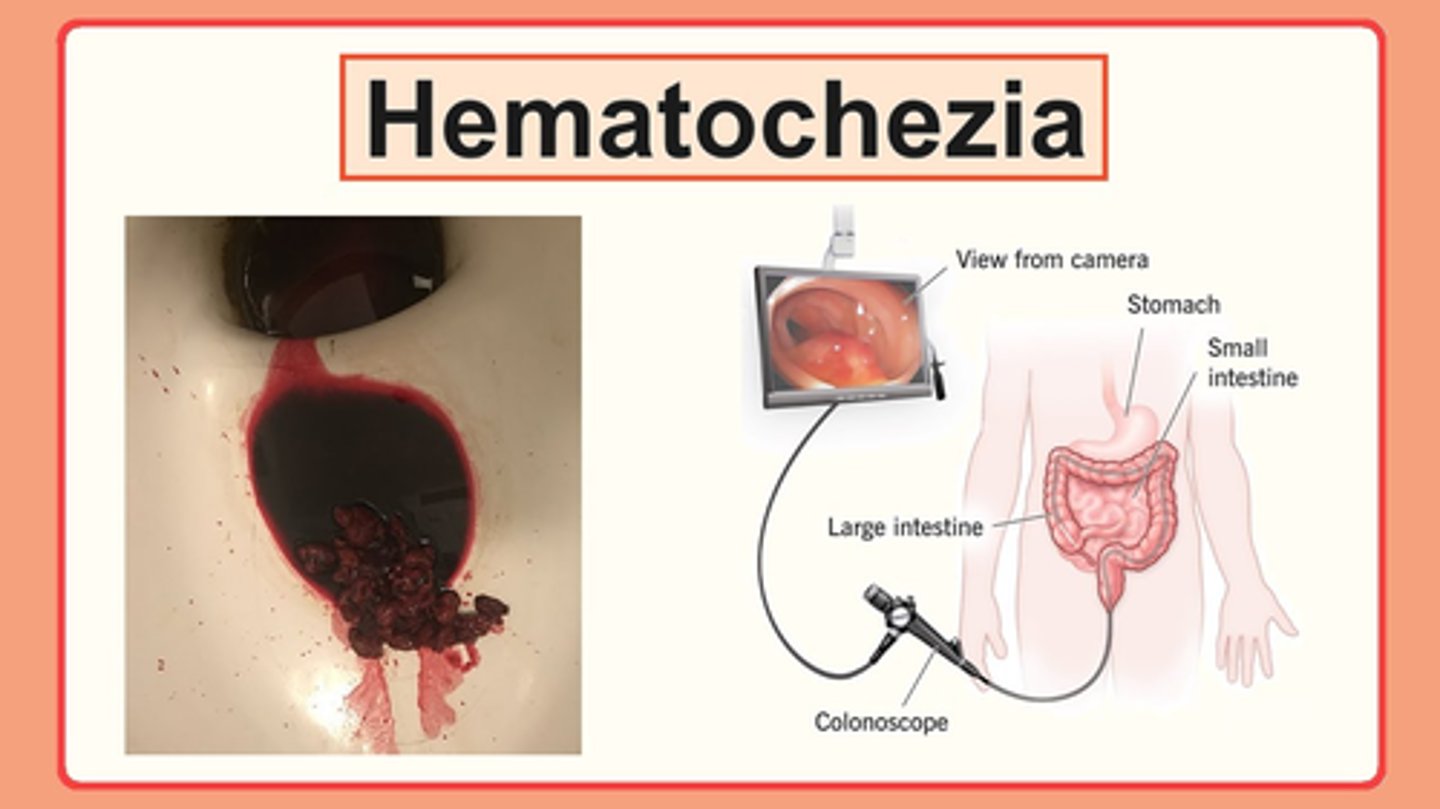
What is the definition of hematochezia?
A) Fatty stool
B) Blood in the stool
C) Black, tarry stool
D) Mucus in the stool
B) Blood in the stool
What is the definition of steatorrhea?
A) Blood in the stool
B) Black, tarry stool
C) Fatty stool
D) Mucus in the stool
C) Fatty stool
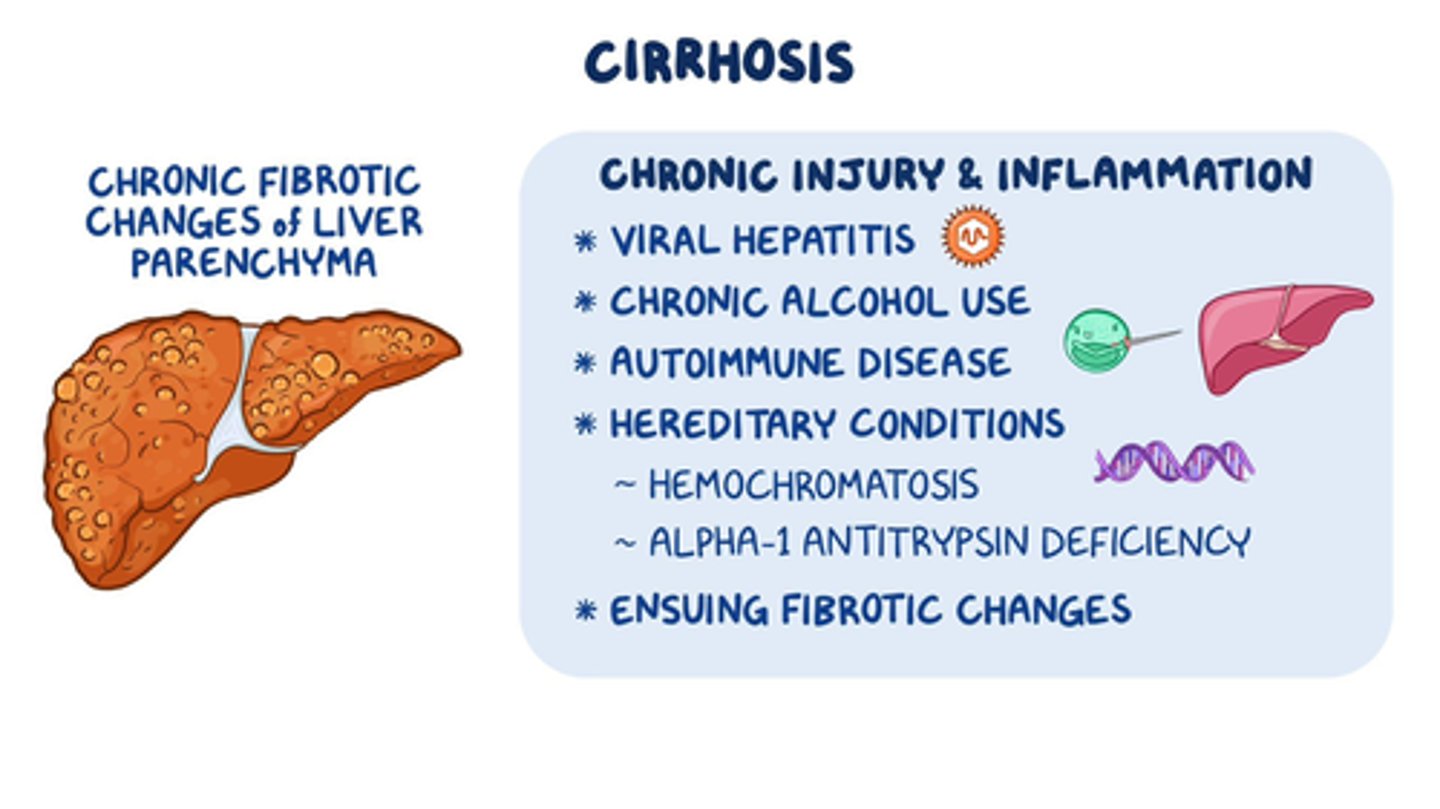
Which of the following are common causes of liver cirrhosis?
A) Hypertension, diabetes, and high cholesterol
B) Chronic alcohol abuse, viral hepatitis (B and C), and non-alcoholic fatty liver disease
C) High calcium intake, dehydration, and vitamin D deficiency
D) Chronic kidney disease, hyperkalemia, and hypothyroidism
B) Chronic alcohol abuse, viral hepatitis (B and C), and non-alcoholic fatty liver disease
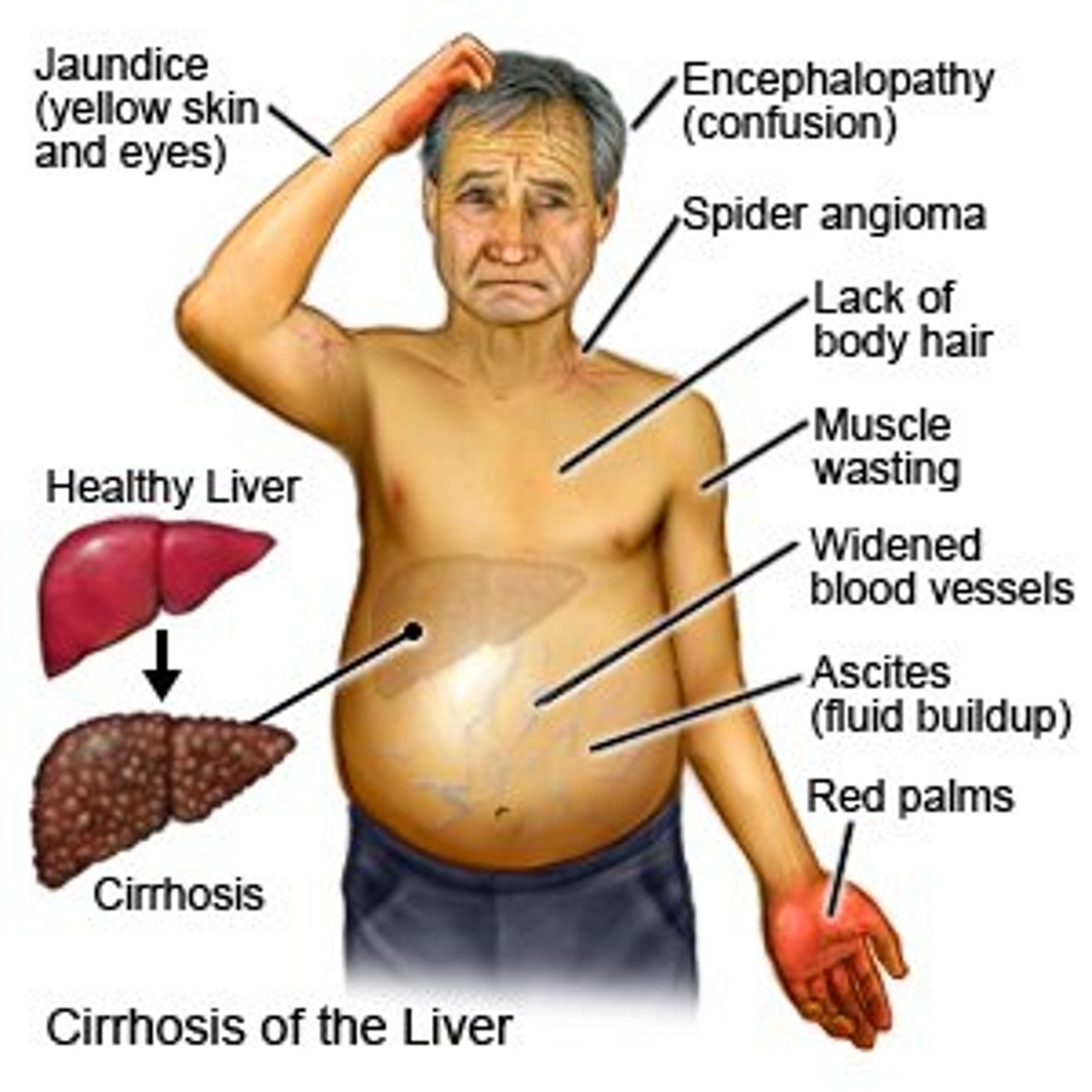
What are common clinical manifestations of liver failure?
A) Increased urine output, high blood pressure, and frequent headaches
B) Jaundice, ascites, varices, encephalopathy, and coagulopathy
C) Weight gain, muscle cramps, and increased appetite
D) Dry skin, increased energy, and normal bilirubin levels
B) Jaundice, ascites, varices, encephalopathy, and coagulopathy
What is a potential complication of advanced liver cirrhosis?
A) Improved liver function
B) Regeneration of healthy liver tissue
C) Liver failure leading to the need for a liver transplant
D) Decreased bilirubin levels and improved coagulation
C) Liver failure leading to the need for a liver transplant
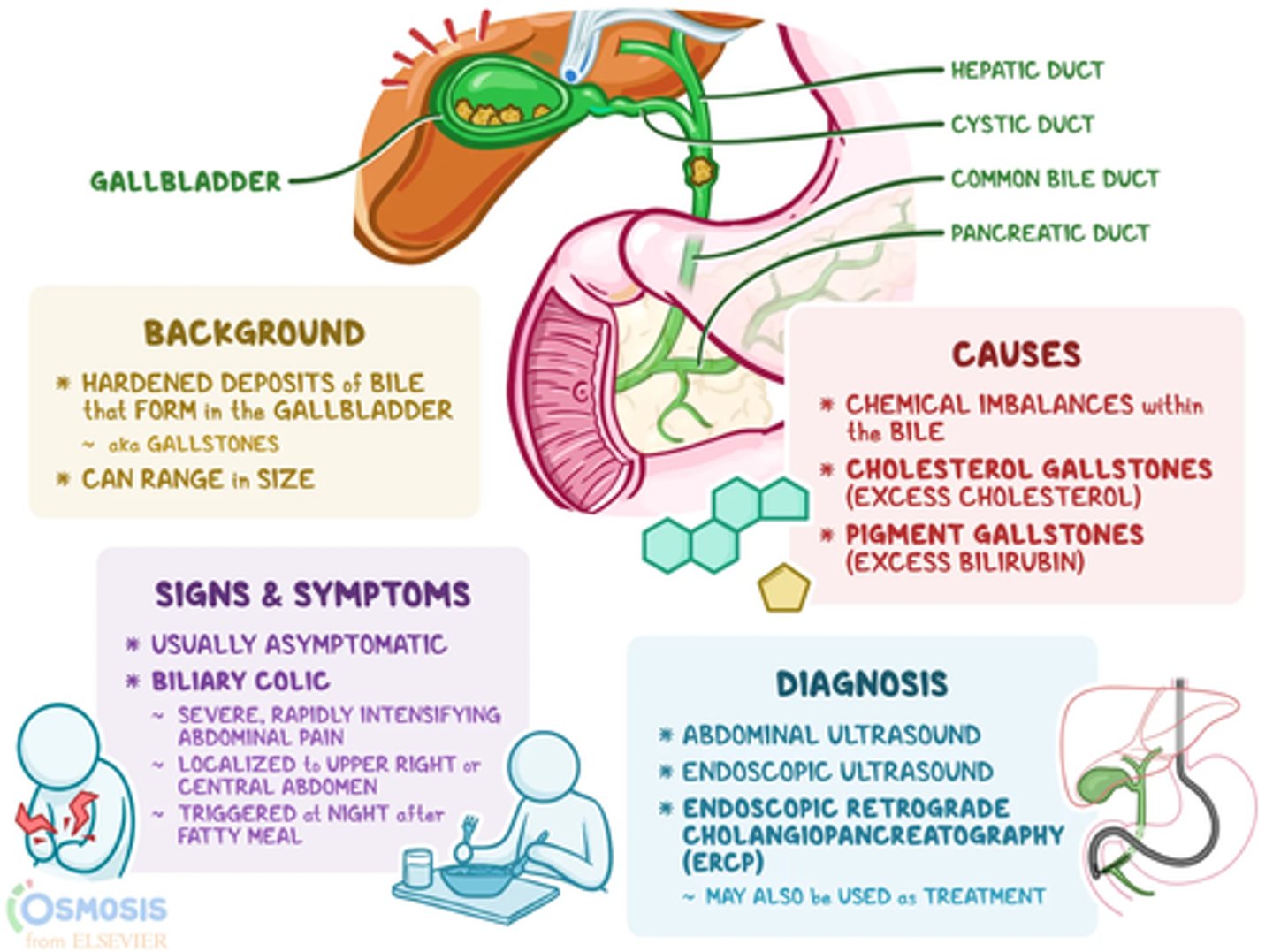
Which of the following are common clinical manifestations of cholecystitis/cholelithiasis (inflammation of gallbladder/gallstones)?
A) High fever, lower quadrant pain, black tarry stool, weight gain
B) Low grade fever, upper quadrant/RUQ pain ~30 minutes after eating a fatty meal, malaise, steatorrhea, pale stool indicating obstruction
C) Increased energy, lower quadrant pain, dark urine, frequent headaches
D) Low grade fever, upper quadrant/RUQ pain immediately after eating, jaundice, dark stool
B) Low grade fever, upper quadrant/RUQ pain ~30 minutes after eating a fatty meal, malaise, steatorrhea, pale stool indicating obstruction
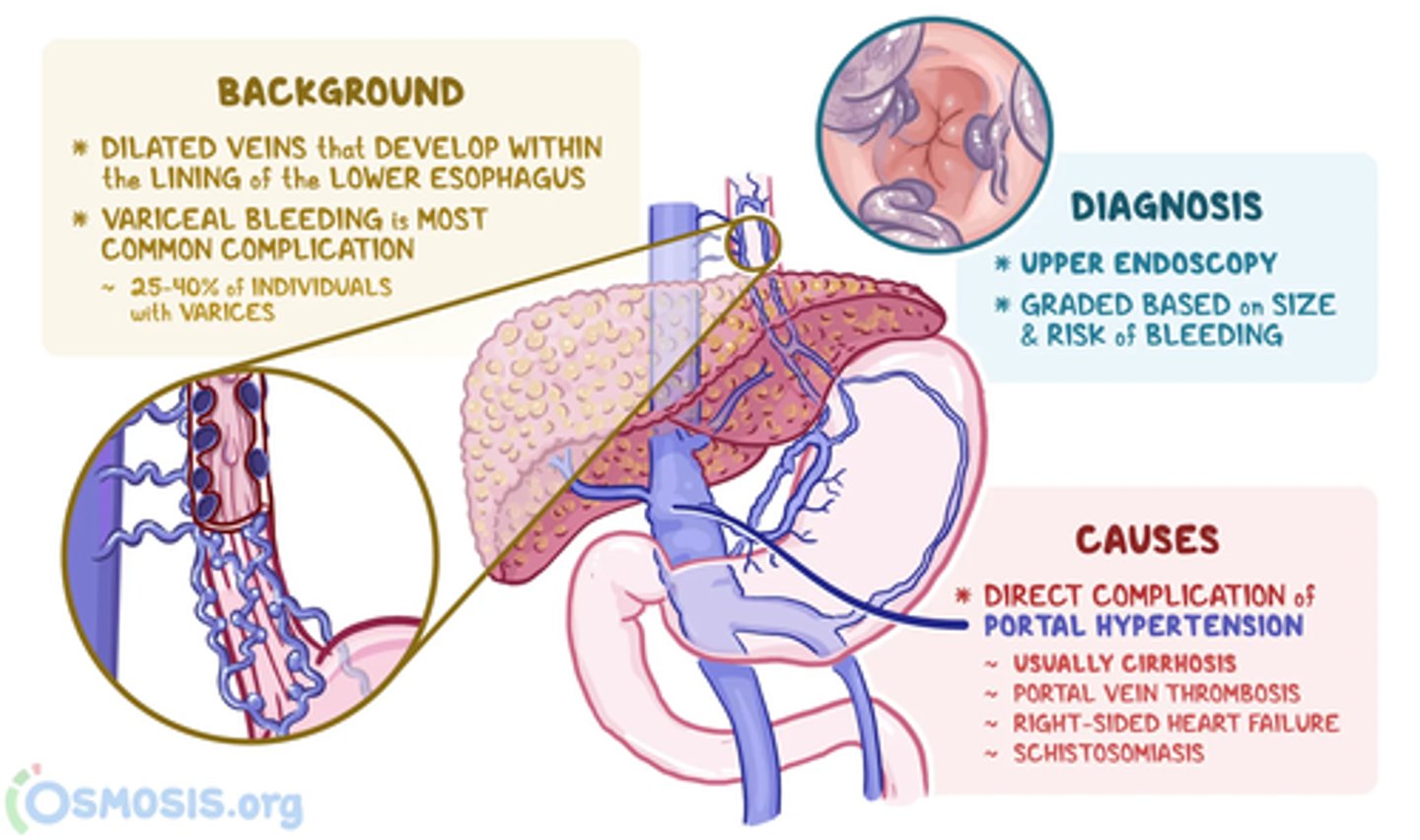
What is the primary cause of esophageal varices (enlarged veins in the esophagus due to increased pressure)?
A) Chronic gastroesophageal reflux disease (GERD)
B) Hypertension and diabetes
C) Portal hypertension, often due to liver cirrhosis
D) Chronic kidney disease and dehydration
C) Portal hypertension, often due to liver cirrhosis
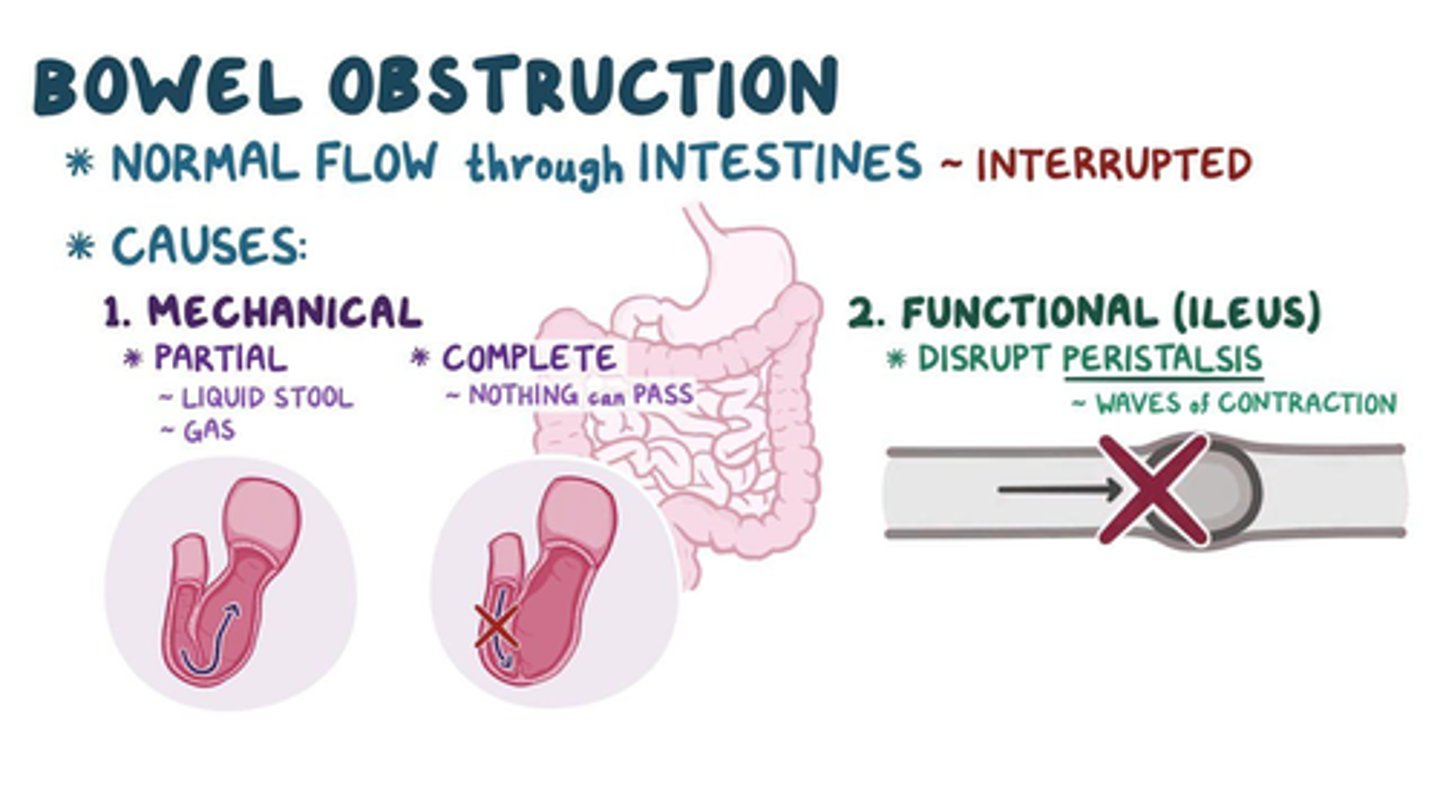
What is a mechanical bowel obstruction?
A) An obstruction caused by a functional issue in the intestines
B) An obstruction caused by a physical barrier such as adhesions, hernias, tumors, or strictures
C) An obstruction caused by a chemical reaction in the intestines
D) An obstruction caused by an infection
B) An obstruction caused by a physical barrier such as adhesions, hernias, tumors, or strictures
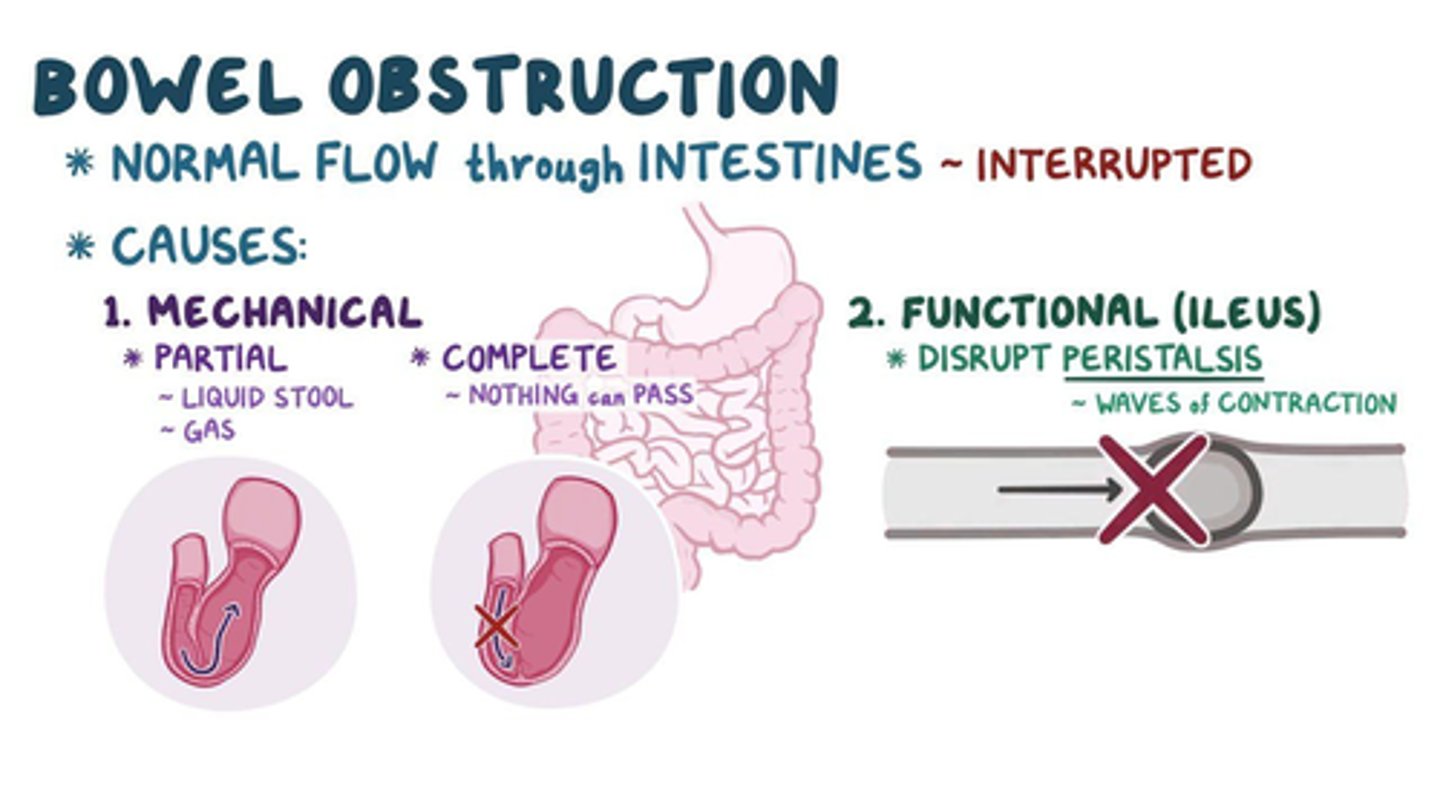
What is a non-mechanical/functional bowel obstruction?
A) An obstruction caused by a physical barrier such as adhesions, hernias, tumors, or strictures
B) An obstruction caused by a chemical reaction in the intestines
C) An obstruction caused by a lack of normal intestinal motility, often due to conditions like paralytic ileus
D) An obstruction caused by a physical injury to the intestines
C) An obstruction caused by a lack of normal intestinal motility, often due to conditions like paralytic ileus
(example- nerve function not returning after surgery)
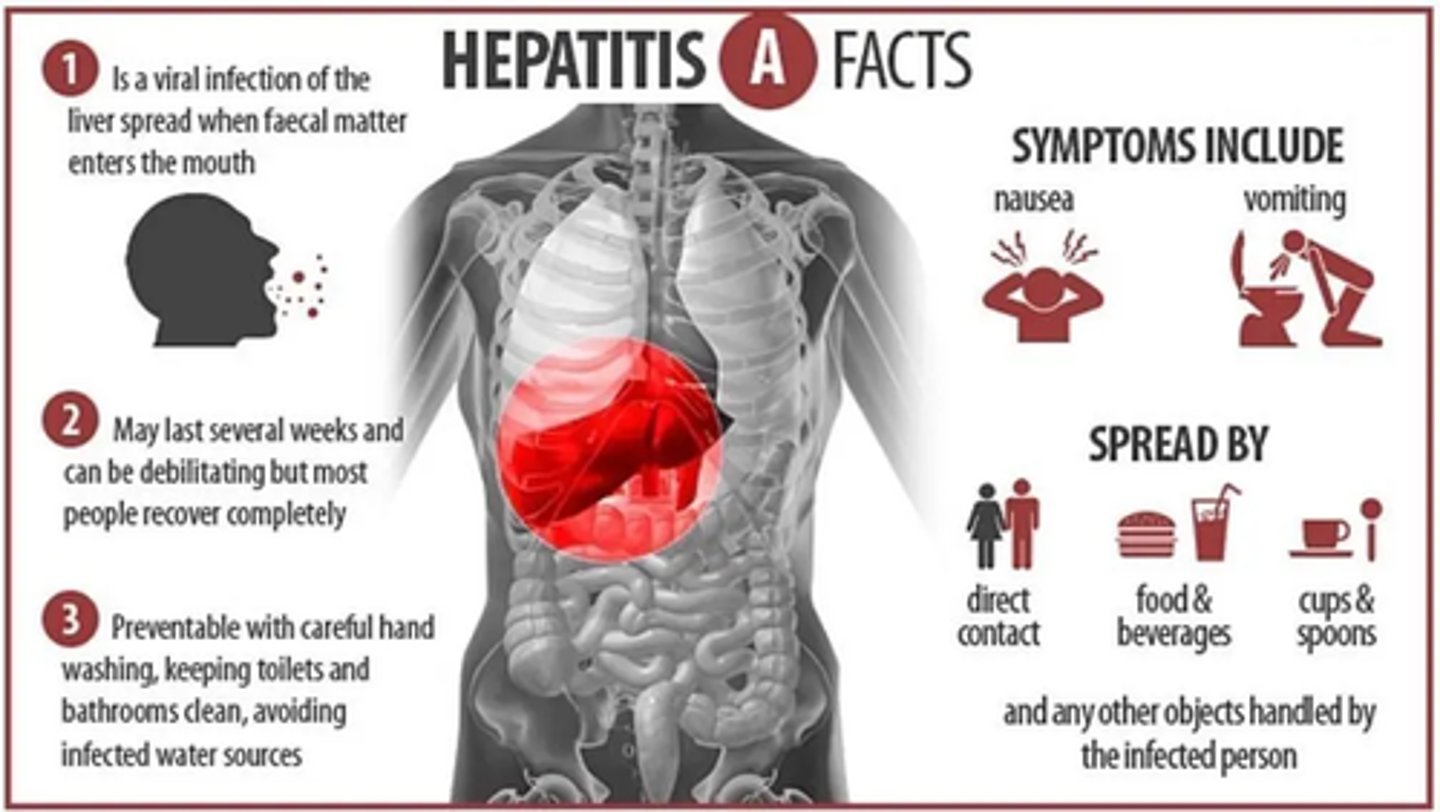
What are the common risk factors for Hepatitis A (viral infection that causes acute liver inflammation)?
A) Blood transfusions, IV drug use, sharing needles
B) Contaminated food and water, close contact with an infected person, poor sanitation
C) Unprotected sex, exposure to infected blood, mother-to-child transmission during birth
D) Chronic alcohol abuse, smoking, obesity
B) Contaminated food and water, close contact with an infected person, poor sanitation