Looks like no one added any tags here yet for you.
What is dementia?
A chronic or progressive syndrome that leads to deterioration in cognitive function, that is severe enough to have an impact on social or occupational function
What is mild cognitive impairment?
- Less severe than dementia
- Not severe enough to impact upon daily life
- Affects 5-20% of those over the age of 65 years
- At increased risk of progression to dementia
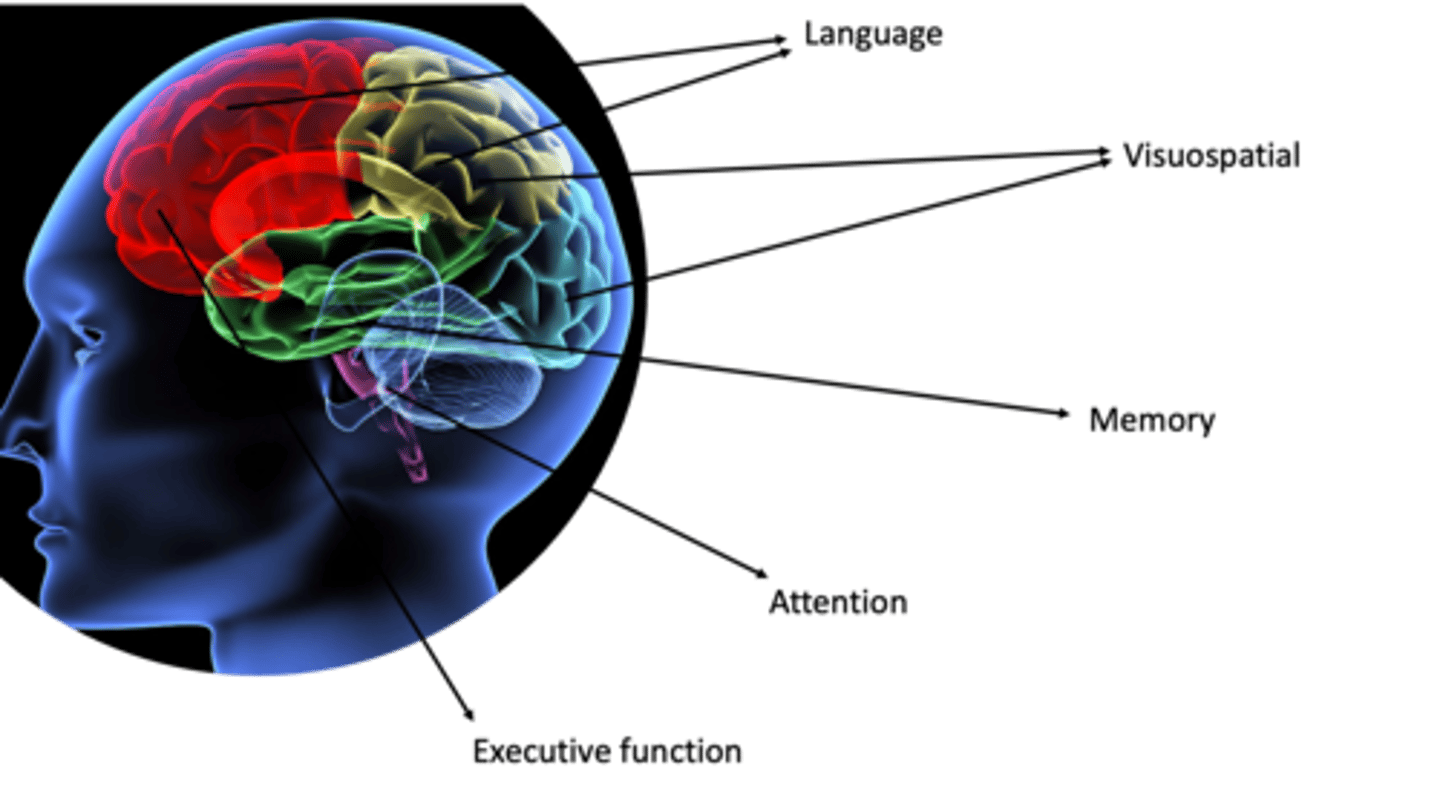
What different aspects of cognition may be affected by dementia?
Language, visuospatial, memory, attention, executive function
What is the reticular activating system?
a series of connections between the cortex, thalamus and retucular formation in the brainstem
mediates attention
What is the impact of decreased executive function?
People will struggle with things such as reduced interest in the environment, becoming fixed on one idea, difficulty switching tasks, poor empathy and impaired interpersonal relations
What are the sub-types of dementia?
- Alzheimers (50-60%)
- Vascular
- Mixed (Alzheimers/vascular)
- Dementia with Lewy bodies
- Frontotemporal dementia
- Alcohol related
- Parkinsons disease
- Creutzfeldt-Jakob disease
- Wernicke Korsakoff's syndrome
Which type of dementia accounts for 20% of dementia cases <65 yrs?
Frontotemporal
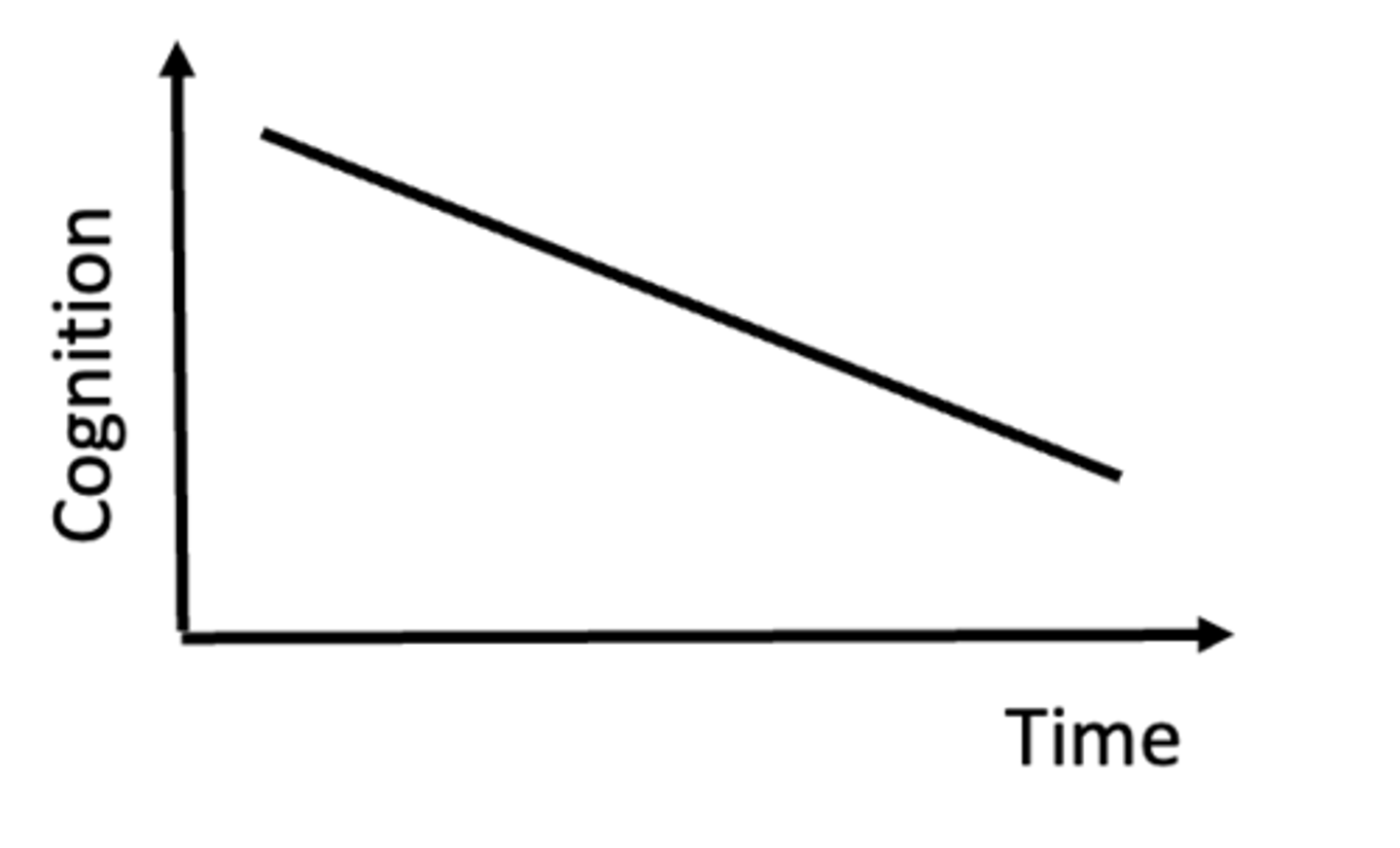
What is the pathology of Alzheimers disease?
- Accumulation of beta-amyloid plaques
- Tau protein hyperphosphorylation causing neurofibrillary tangles
- Inflammation, lipid peroxidation and excitotoxicity
- Partietal and temporal lobes most commonly affected
- Acetylcholine, norepinephrine and serotonin pathways affected
What are the signs and symptoms of Alzheimers disease?
- Early memory loss (short term memory)
- Language problems (word finding difficulties, poor verbal fluency)
- Visuospatial problems (difficulty copying objects, getting lost)
- Behavioural problems later (apathy, reduced social interaction)
- Wandering, aggression, delusions and psychosis develop late in the illness
Name some genes associated with the development of AD?
APOE4
Presenilin 1 and 2
Amyloid Precursor Protein
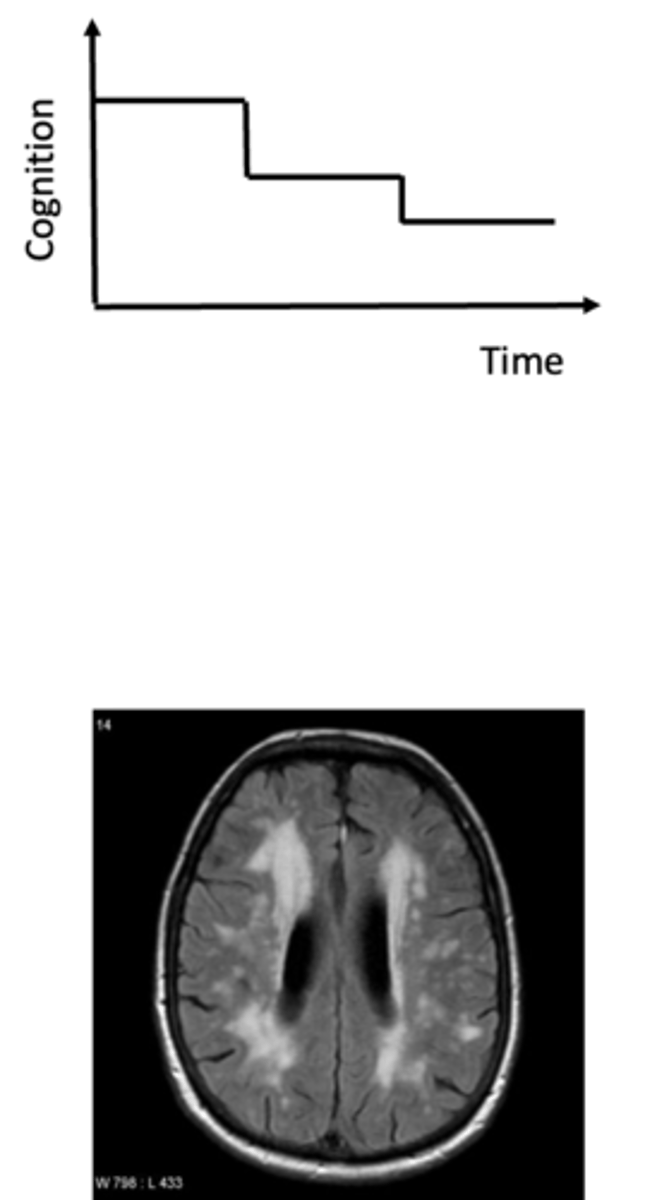
What is the pathology of Vascular dementia?
- 1-4% of dementia in those over 65yrs
- Can occur due to a single cortical stroke or a number of small subcortical events which lead to cumulative deficits
- Typically caused by small vessel disease, causing a sub-cortical pattern of dementia and affecting circuits in the basal ganglia important for information retrieval and storage
What are the typical features of vascular dementia?
- Onset is typically abrupt and deteriorates in a step-wise progression
- Typically slowness of thought, personality change, frontal-executive features
- History typically includes vascular risk factors and CT scan shows evidence of vascular lesions
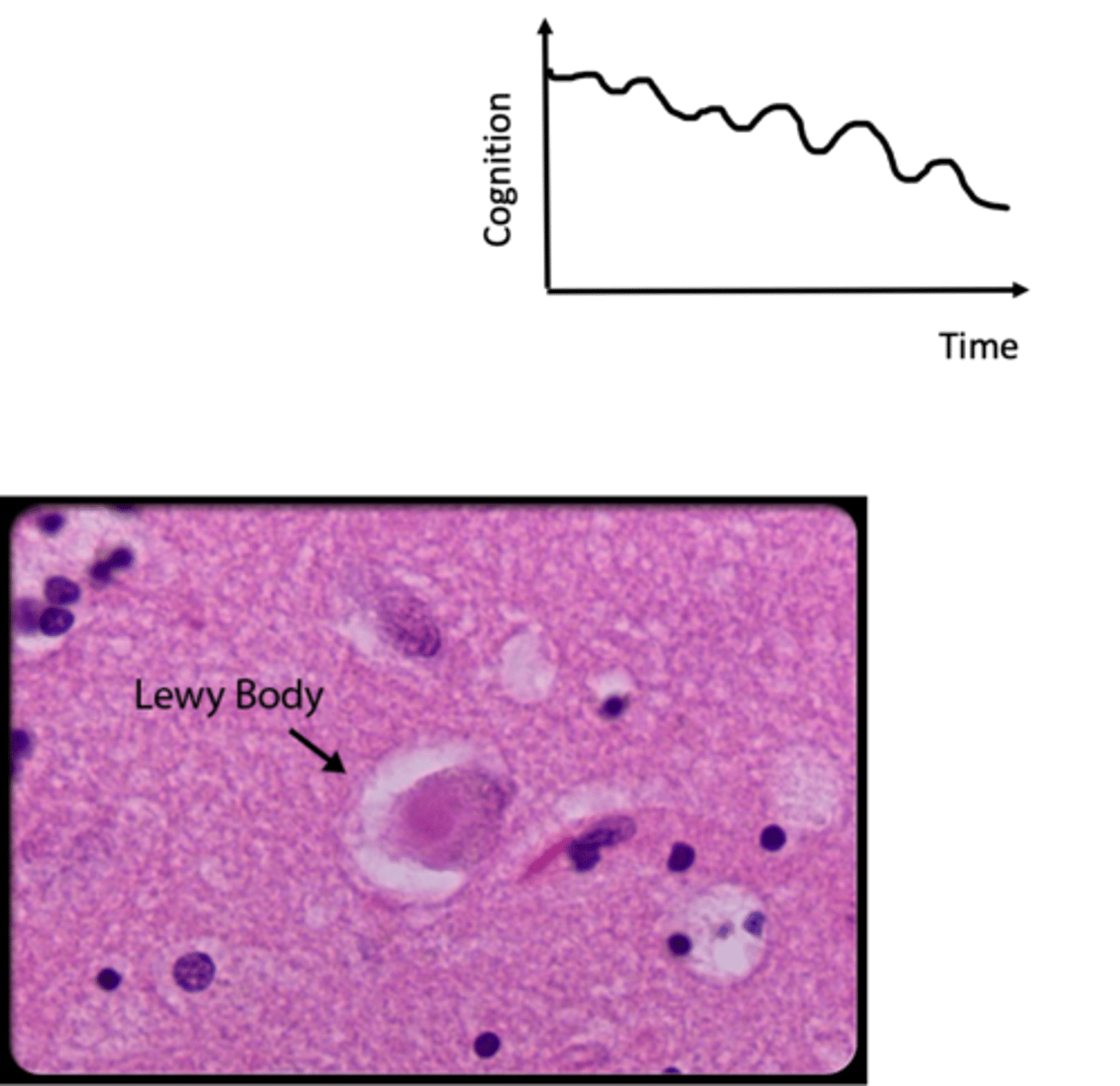
What is the pathology of dementia with Lewy bodies?
- 10-15% dementia
- Accumulation of Lewy Bodies throughout the brain (basal ganglia, limbic system and cortex)
What are the key features of dementia with Lewy bodies?
- Parkinsonism (tremor, bradykinesia, rigidity)
- Fluctuating cognitive impairment
- Visual hallucinations
- Delusions
- Falls
- Sleep disturbance
What is the pathology of frontotemporal dementia?
- 2-5% dementia
- Abnormal processing of Tau proteins (normal cellular component of microtubules)
What are the key features of frontotemporal dementia?
- More common in younger people: mean age of onset 56061 years
- Insidious and slow progression
- Typically early personality change, emotional blunting, loss of insight, interpersonal behavioural changes
- Memory and visuospatial ability are preserved early on
- 40% have an affected 1st degree relative
What are the risk factors for dementia?
- Family history (a genetic component)
- Age
- Alcohol intake
- Obesity
- Vascular risk factors
How is dementia diagnosed?
- Complex: there is no single test for dementia
- Should be diagnosed by a specialist through a memory assessment service
- Diagnosis is made based upon history and cognitive examination
- Any investigations are supportive and are done to rule out dementia mimics
How to take a history of dementia?
- Include a collateral history
- Onset of symptoms and rate of progression
- Ask about different cognitive deficits:
>Memory loss
>Attention
>Language impairment
>Calculation
>Visuospatial problems, apraxia
>Executive function
- Behavioural changes: personality change, sleep disturbance, delusions and hallucination, continence
- Ask about functional difficulties
How do you carry out an examination for dementia?
- Cognitive testing
- Many different tests available to test the different cognitive domains
> 10 point AMT (good screening test)
> MMSE (limited cognitive domains)
> MoCA
> Addenbrookes
> Clock drawing test
What investigations are used in dementia diagnosis?
Mainly used to look for reversible causes of dementia like symptoms:
- Blood tests: B12, folate, Ca, ESR, thyroid function
- Cerebral imaging: CT/MRI
What diseases/conditions may mimic dementia?
- Delirium
- Depression
- Hypothyroidism
- B12/folate deficiency
- Medications
- Normal pressure hydrocephalus
- Space occupying lesion
- Vasculitis
What are the pharmacological management options of dementia?
Cholinesterase inhibitors
- eg. rivastigmine, donepezil, galantamine
- use in mild-moderate AD
- significant side effects
- small benefit in cognition
Memantine (glutamine antagonist)
- use in moderate to severe AD
Also stop potentially harmful medications if possible (anticholinergic medications especially)
What are the non-pharmacological options for dementia management?
- Maximise function with daily routines and written down 'to do' lists
- Improve orientation with clocks and calendars
- Familiar calm environments
- Care packages to support
- Occupational therapy
- Home adaptations to improve safety
- Education, support and rest bite for caregivers
- Advance directives, power of attorney
What are the behavioural and psychological symptoms of dementia (BPSD)?
- Delusions
- Agitation
- Hallucinations
- Aggression
- Apathy
= the non-cognitive symptoms
What are the triggers of BPSD that can be prevented/managed?
-Pain
-Dehydration
-Infections
-Constipation
-Address sensory impairment
-Malnourishment
-Freedom to move
-Temperature
-Treat depression
-Stimulation and enjoyment
-Person centred care
How can BPSD be managed?
1) A period of monitoring: most will resolve in 4-6 weeks
2) Identify and treat trigger factors
3) Calming and creative therapies
4) Good sleep hygiene and regular exercise
5) Antipsychotics
How might communication with patients with dementia be different?
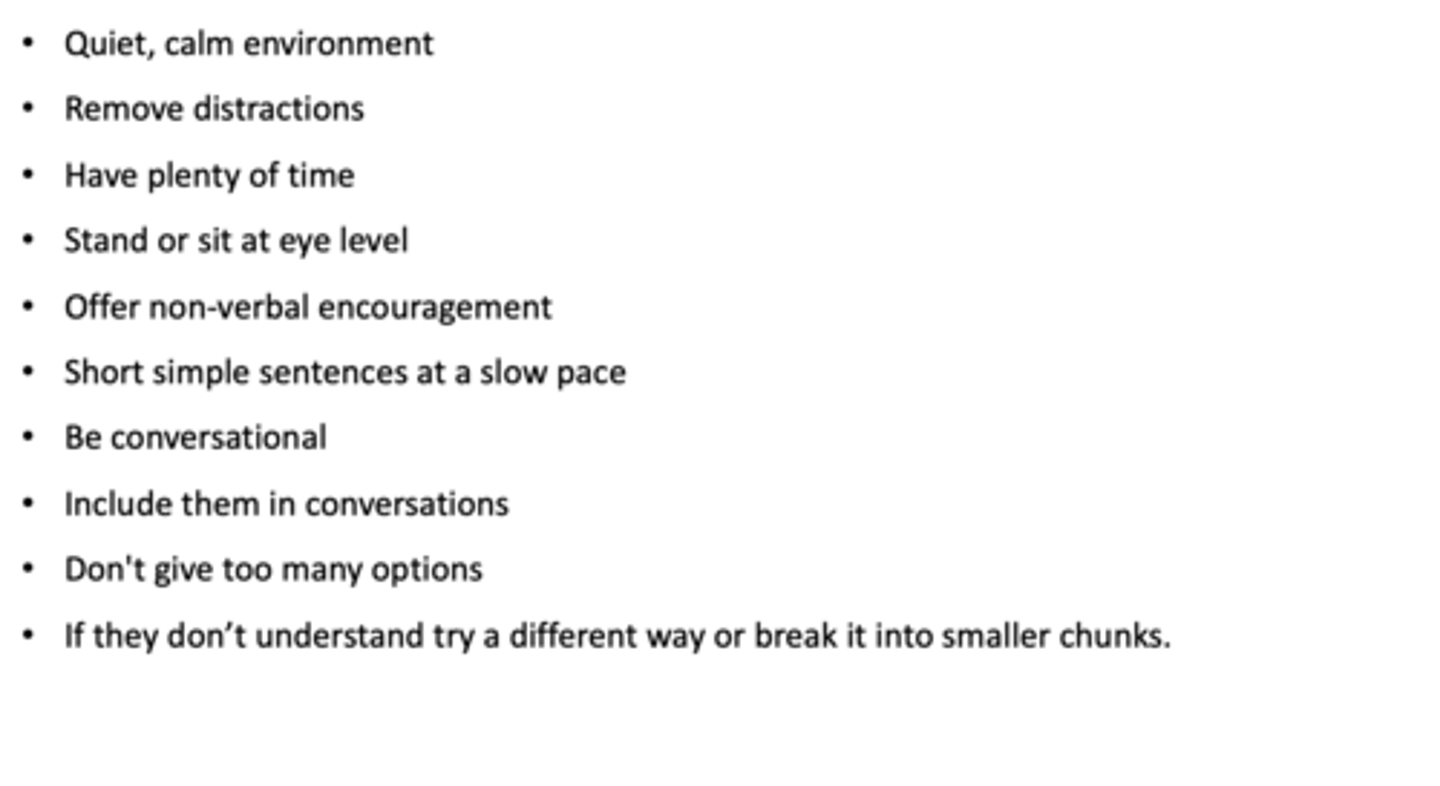
- People with dementia often find it difficult to hold a conversation -> this causes anxiety, frustration, loss of confidence and withdrawal from social situations
- Unable to find the right word: use related words or substitutes
- Repetition of words or phrases
- Struggle to understand
- Distractible: move from one topic to another
- Thoughts are slower - can't keep up
How to communicate effectively with patients with dementia?
How is pain managed in patients with dementia?
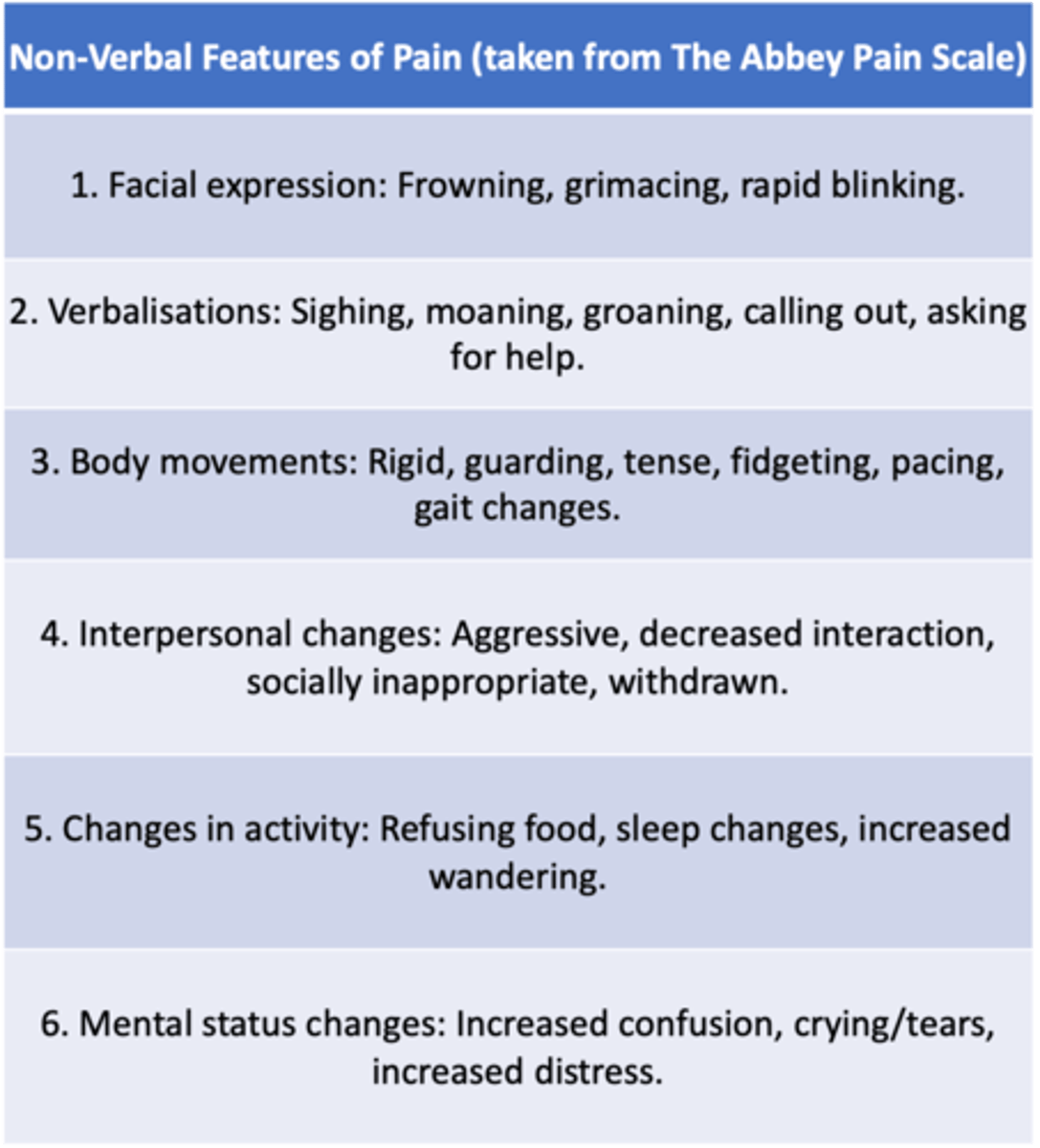
- Patients with dementia find it hard to verbalise their pain
- A non-verbal pain assessment tool can be useful eg. Abbey Pain Scale
- Family members and carers can be helpful in identifying pain
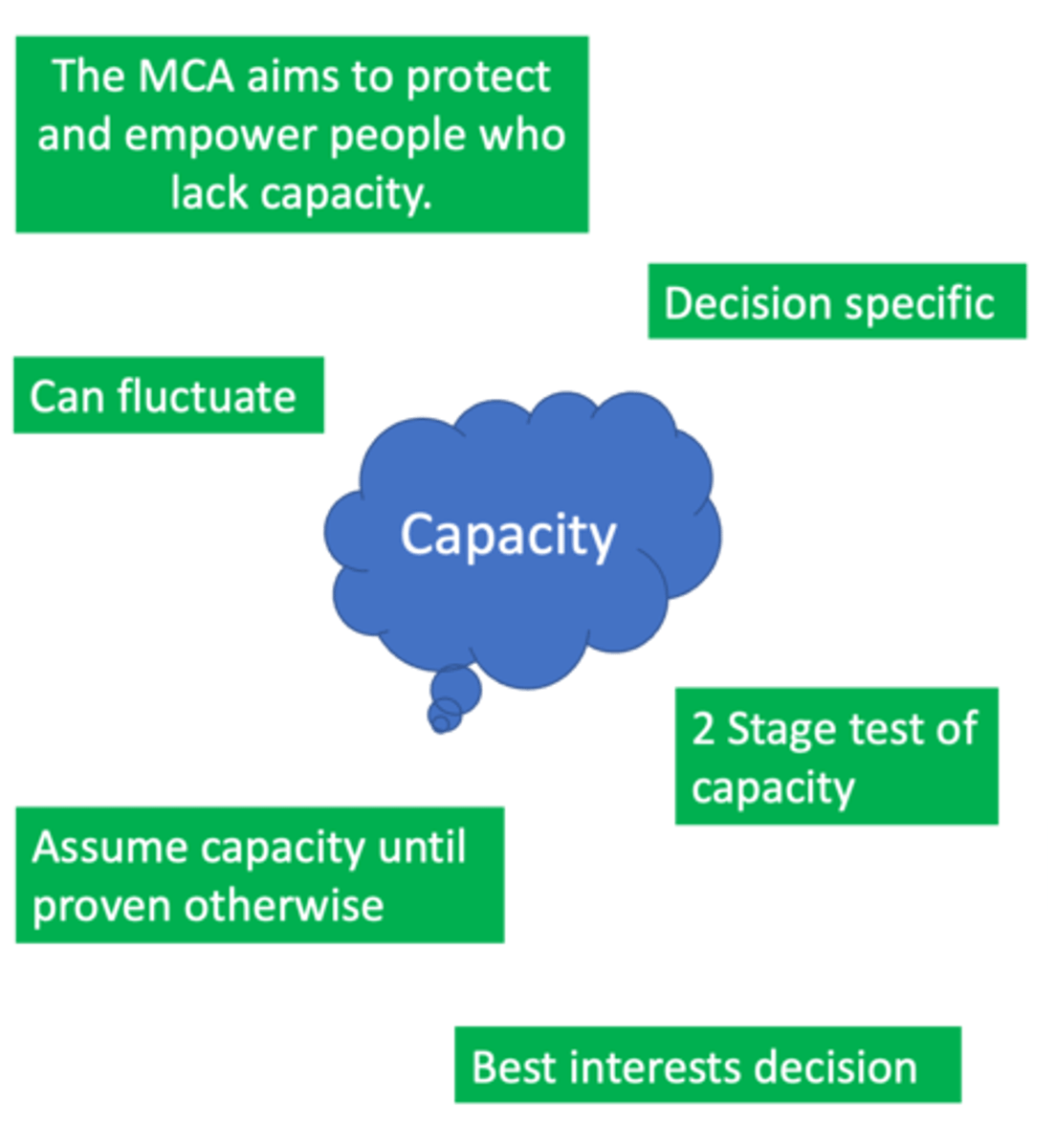
What are the components of capacity?
1. Does the person have an impairment of their mind or brain (either due to illness, or due to external factors such as alcohol or drug use?)
2. Can the person
i). Understand the information being told to them.
ii). Retain the information.
iii). Use and weigh up the information in order to make a decision
iv). Communicate their decision
What is a lasting power of attorney?
A legal document which appoints someone to make decisions on your behalf if you lack capacity.
Two types:
- LPA for health and welfare
- LPA for property and financial affairs
How does feeding change in patients with dementia?
Reduced oral intake and weight loss are signs of advanced dementia
Occurs due to:
- Loss of desire to eat
- Loss of cerebral co-ordination of the swallowing mechanism
- Depression
-> No evidence for artificial feeding in dementia
-> Does not prolong survival or improve quality of life
-> Does not prevent aspiration pneumonia
-> Offer food preferences
-> Offer small frequent meals
-> Take steps to minimise aspiration: sit upright, adjust food consistencies, supervise eating
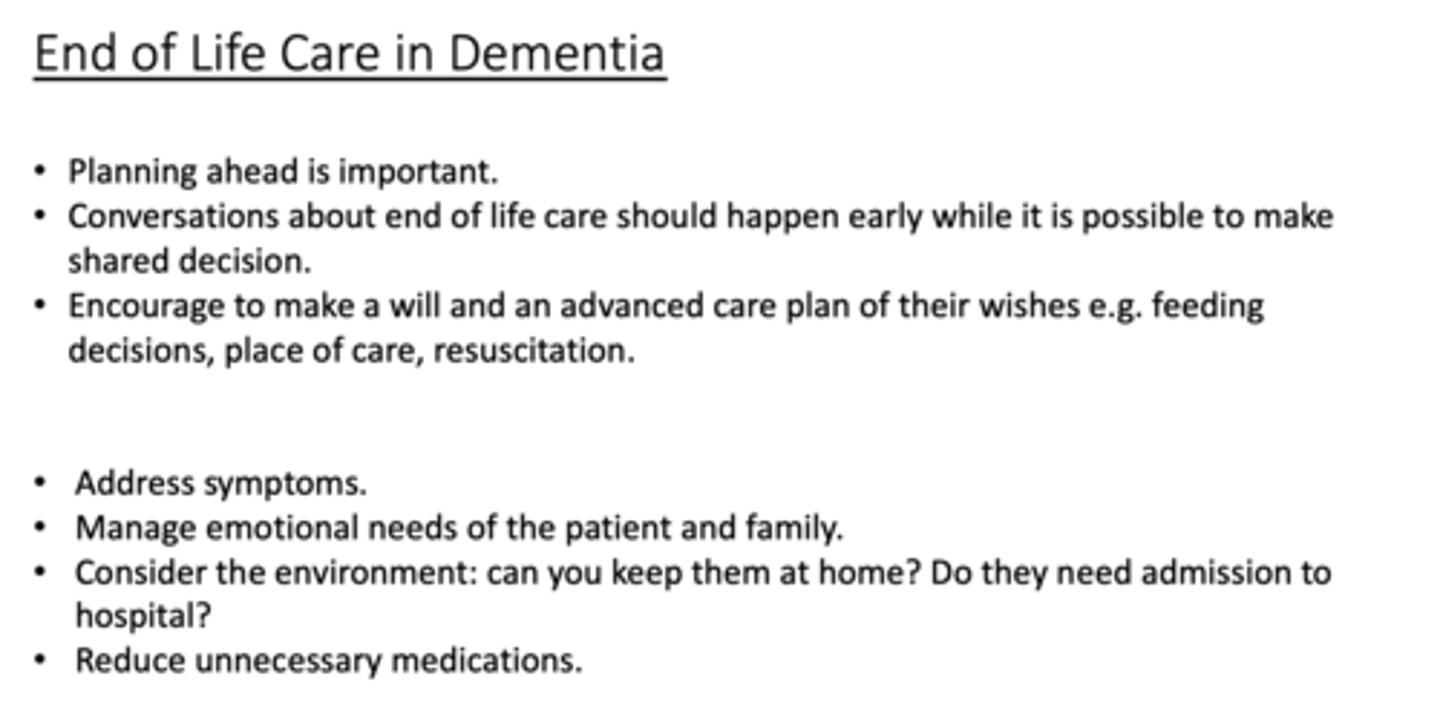
End of life care in dementia