Normal Mobility
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Mobility Defined
The ability to independently and safely move oneself from one place to another. It includes rolling, sit to stand, walk, run, etc..
Mobility according to the ICF
Activity and Participation
Body structure and function (Gait pattern)
Essential requirements of Gait
Progression: Includes ability to initiate and terminate movement
Postural control: Stability
Adaptation: Ability to maintain progression/postural control while:
Avoiding obstacles
Anticipate and react to changes
Adaptation is what qualifies mobility in the activities and participation section of the ICF
Note: These 3 requirements cause Energy Efficiency with Minimal System Stress
Normal Velocity
1.46 m/sec
Normal Candence
90 -120 steps/min
Normal Step and Stride length
Step: 28in
Stride: 56 inc
Gait changes with slow walking
Stance time increases
Swing time remains constant
Variability Increases
Increased medio-lateral COM displacement
Goals of Stance Phase
Stabilizing the limb for weight acceptance
Shock absorption
Propulsion
Goals of Swing Phase
Reposition the limb
Clearing the ground
Braking forces
Why is gait so smooth?
Excellent mechanical transfer of gravitational and kinetic forces
Brain regions that contribute to gait
▪ SMA
▪ Medial primary sensorimotor areas
▪ Striatum
▪ Cerebellum
▪ Visual cortex and visual processing centers
▪ Brain stem
▪ With gait speed increase: increased prefrontal and premotor cortex activity
What happens when a cat is spinalized?
The cat was still able to walk due to central program generators
CPGs: Dedicated networks of nerve cells that generate
movements and that contain the information that
is necessary to activate different motor neurons in
the appropriate sequence and intensity to
generate motor patterns. They are innate but can be adapted and
perfected with experiences
Role of CPG
Neural networks within the brainstem and spinal cord
Produce specific, rhythmic movements
without conscious effort
without peripheral afferent feedback
Brainstem examples: Chewing, breathing, swallowing
SC example: Locomotion
CPG 2- Level Model
Rhythm generator
Regulation of gait speed (step-cycle periods and phase durations)
Pattern formation
Level of motor neuron activity
Has its own independent mesencephalic locomotor region input
Note: Although a key element that characterizes CPG is the capacity to cause movement without sensation: CPG’s are strongly influenced by central and peripheral information. Circuits exist at birth but final organization is dependent on experiences provided to the system
Locomotion after a spinal cord injury
▪ No descending influences
▪ No contact with the cerebellum
▪ External, afferent information is needed to generate movement
▪ Gait without descending influences even with stimulation will not be smooth: caricature gait
▪ Ideas: treadmill training, electrical stimulation, robotics
2 key reflexes in gait
Stretch reflex: involved in extreme ranges of motion
Extensor thrust: Facilitates the extensor muscles of the LE during weight bearing
Role of the Mesencephalic locomotor region (Brainstem) in gait
Descending control of gait
Activates the medial reticular formation
Reticular formation activates the spinal locomotor system
Role of the cerebellum in Gait
Automatic aspects of gait control
Adjusts gait in novel contexts and when visual guidance is critical
Input: Somatosensory, visual and vestibular
Output: Reticular formation in the brainstem
Role of the basal ganglia in gait
▪ Maintains appropriate postural muscle tone
▪ Modulates rhythmic stepping movement
▪ Initiates locomotion
▪ Cognitive component
▪ Attention to task
Role of Posterior parietal cortex and posterior temporal cortex in gait
Help visual recognition of objects and events from different viewpoints and process to move efficiently in space
These and the superior colliculus are involved in orienting to novel stimuli in the visual field
Hippocampus codes topographical information, parietal cortex codes into 3-D metrics
Role of supplementary motor area in gait
Connections to the reticular formation
Believed to assist with postural control during gait
Planning and programming of locomotion with the premotor cortex
Muscle and Non-muscle contributions
Muscle contributions: use of concentric and eccentric control
Non- muscular contributions: torque - Passive extensor torques that occur during gait. Muscles are often counteracting these passive., non-muscular forces
Two critical things to consider about adaptation
1. Reactive strategies for modifying gait
2. Pro-active strategies for modifying gait
Note: Without intact sensory systems:
▪ ADAPTATION will be impacted
Loss of appropriate reactive strategies
Less efficiency with movement
Somatosensory system
▪ 1. Contributes to appropriate stepping frequency
▪ 2. Strongly influences inter-limb coordination
▪ 3. Joint receptors and muscle spindle afferents play a role in normal locomotion
▪ 4. Influence of cutaneous information assists with obstacle navigation and postural control (reactive strategies), even at the CPG level
At what level does somatosensation affects gait?
At the reflex level
Role of Visual system in gait
1. Helps us determine our speed (visual flow)
2. Gives cues to adjust body to maintain HAT upright against gravity
3. Avoid objects
4. Prediction
Piloting strategy
A mental representation of the spatial environment = topological information + metric information.
Visual system- inclines
UP:
▪ Increase in step length
▪ Increased muscle activity
▪ Reduced cadence
DOWN
▪ Decreased in step length
▪ Increased cadence
Turning Strategies
Depends on which foot is in front and which way you are turning.
▪ Step turns
▪ Spin turns
Role of vestibular system in gait
Head must be stabilized during locomotion
Head movements are independent from the movements of the trunk
Eyes will move to keep targets in the fovea as part of the VOR – allows for steady vision during gait.
Cognition ad gait
Dual-task is harder when obstacles are in the way
Dual-task will also slow down the transition from walking to running’
Posture/locomotor skill vs cognitive skills
Initiation of Gait
It is more than a controlled fall
Swing limb will push onto the stance limn (both limbs will need to bear weight)
Steady velocity is reached within 1-3 steps
What defines running?
Both feet are off the ground. A.K.A “Flight” or “Float”
Walk vs Run
Running causes
Increased velocity
Increased GRF
Stance to swing ration 40:60
Increased ROM at all joints
Increased Eccentric control
Change in initial contact of foot depending on speed (no heel strike)
No double limb stance
Decreased BOS
Decreased COG
Stair walking requirements
Progression - Muscle Forces
Stability - Control the COM with a changing BOS
Adaptation: Different heights, carpet, poor lighting etc
Stance/swing = 64%:36%
Stair walking- Ascent
Stance
Weight acceptance: Front of foot
Pull-up: 2x the force to step up
Forward continuance: Most unstable as the contralateral toe lifts off- MOST LIKELY TO FALL HERE
Swing
1. Foot clearance and appropriate placement
2. Tibialis anterior df the foot and hamstrings flex the knee
3. Rectus femoris eccentric control at midswing for
4. Hip flexion brings thigh up
5. Foot placement controlled by hip extension and ankle df
Stair walking - Descent
Stance
1. Weight acceptance
Energy absorption
GRFs are 2x body weight
Gastrocnemius activation
2. Forwards continuance
3. Controlled- lowering
Primarily quadriceps muscle and some eccentric contraction of the soleus
Swing
1. Pull through - Hip flexors
2. Preparation for foot placement
Midswing, extension dominates at all 3 joints
Contact made first with lateral border of foot with tibialis anterior and gastrocnemius activity prior to contact
Sensory cues that can “Make or break” stair walking skills
Vision can alter ability for foot clearance and placement which are critical to safe movement strategies on the stairs
Transfer tasks- What should we be aware of?
▪ 1. Essential characteristics of the task you are asking of them
▪ 2. Sensory and motor strategies that normal individuals typically use to accomplish the task
▪ 3. Adaptations required for changing environmental characteristics
▪ 4. What impairments are hindering the patient from completing the task
3 essentail task requirements for transfers
Progression
Postural control (Stability)
Adaptability
They still aply to transfers and rolling
Sit to stand order of events
Pre-Phase: scoot forward in chair
Phase 1: forward lean of the trunk (flex at hips)
Phase 2: buttocks leaves seat – critical event where the body is unstable
Phase 3: extension phase when hip and knee extend to get the body vertical
Phase 4: stabilization phase once upright
What environmental things can be altered to assist with this transition?
Order of muscle activation in sit to stand
Erector spinae
Rectus femoris
Vastus mediales
Biceps femoris
Gluteus MAc
Rectus abdominus
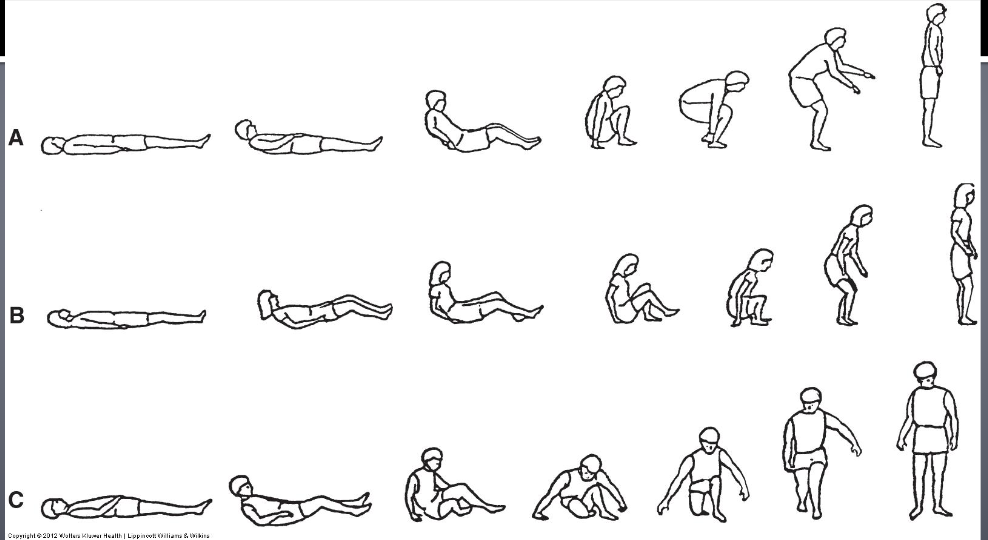
Analyzing supine to stand
Analyzed by UE, LE, axial (trunk and head)
Rising from a bed
Strategies for rising from bed are highly variable:
▪ Still requires: progression, postural control (stability), adaptation
Rolling
Variable patterns are used. Essential features of the most common patterns:
▪ the head must come off the surface