The spinal cord & spinal nerves
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
71 Terms
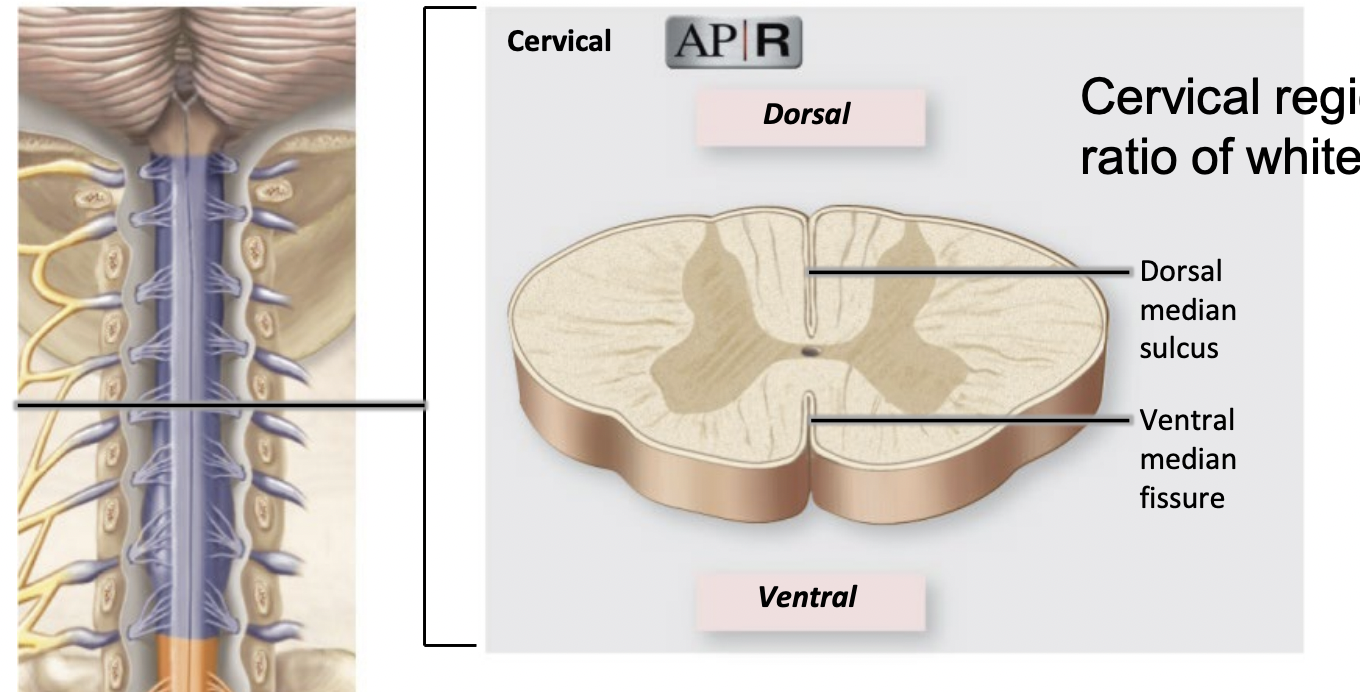
Cervical region
largest ratio of white to gray matter
Cervical conveys tract from sacral, lumbar, thoracic & cervical regions of the spinal cord, consisting of the first eight vertebrae. It controls the neck, arms, and hands and is crucial for many nerve signals to the upper body.
Thoracic region
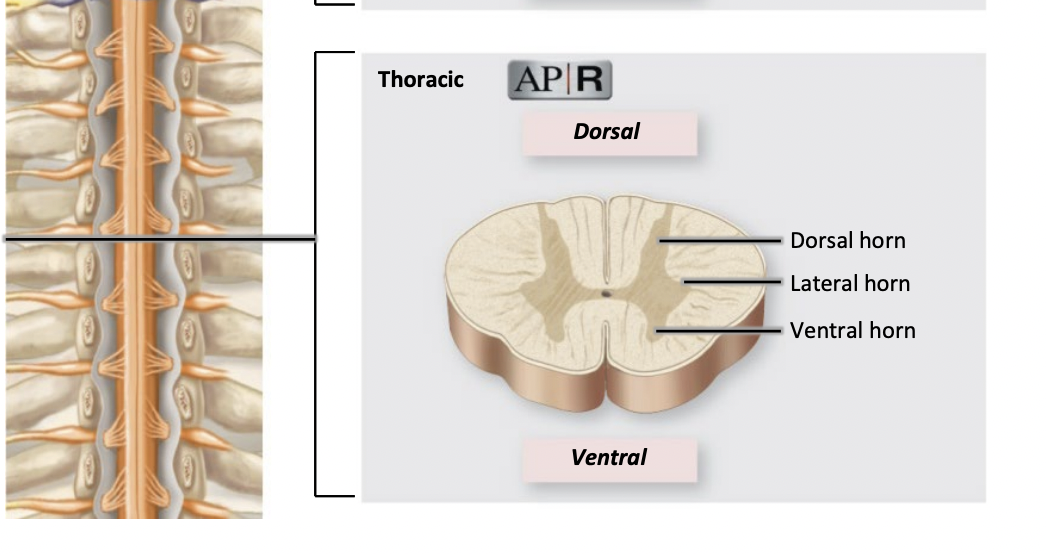
located between cervical and lumbar regions, consisting of twelve vertebrae. It controls the chest and abdominal muscles, as well as sensations from these areas.
still more white matter than gray matter
Lumbar region
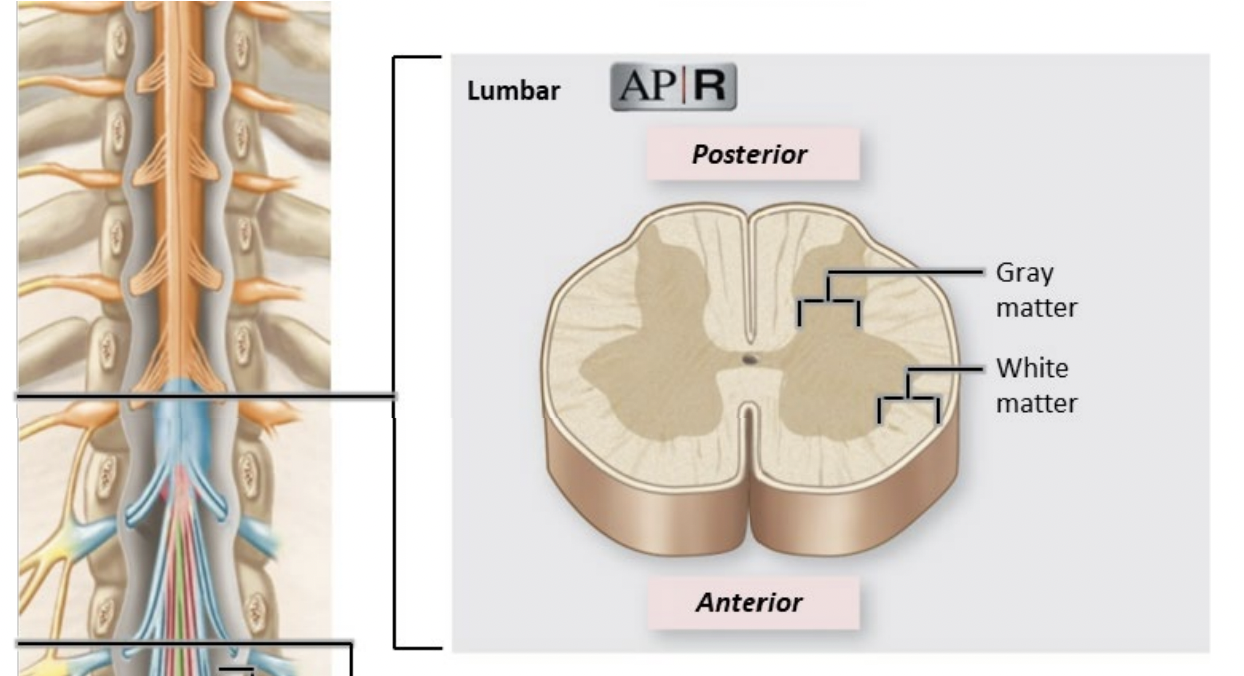
More Gray matter than white matter
It’s located below the Thoracic region
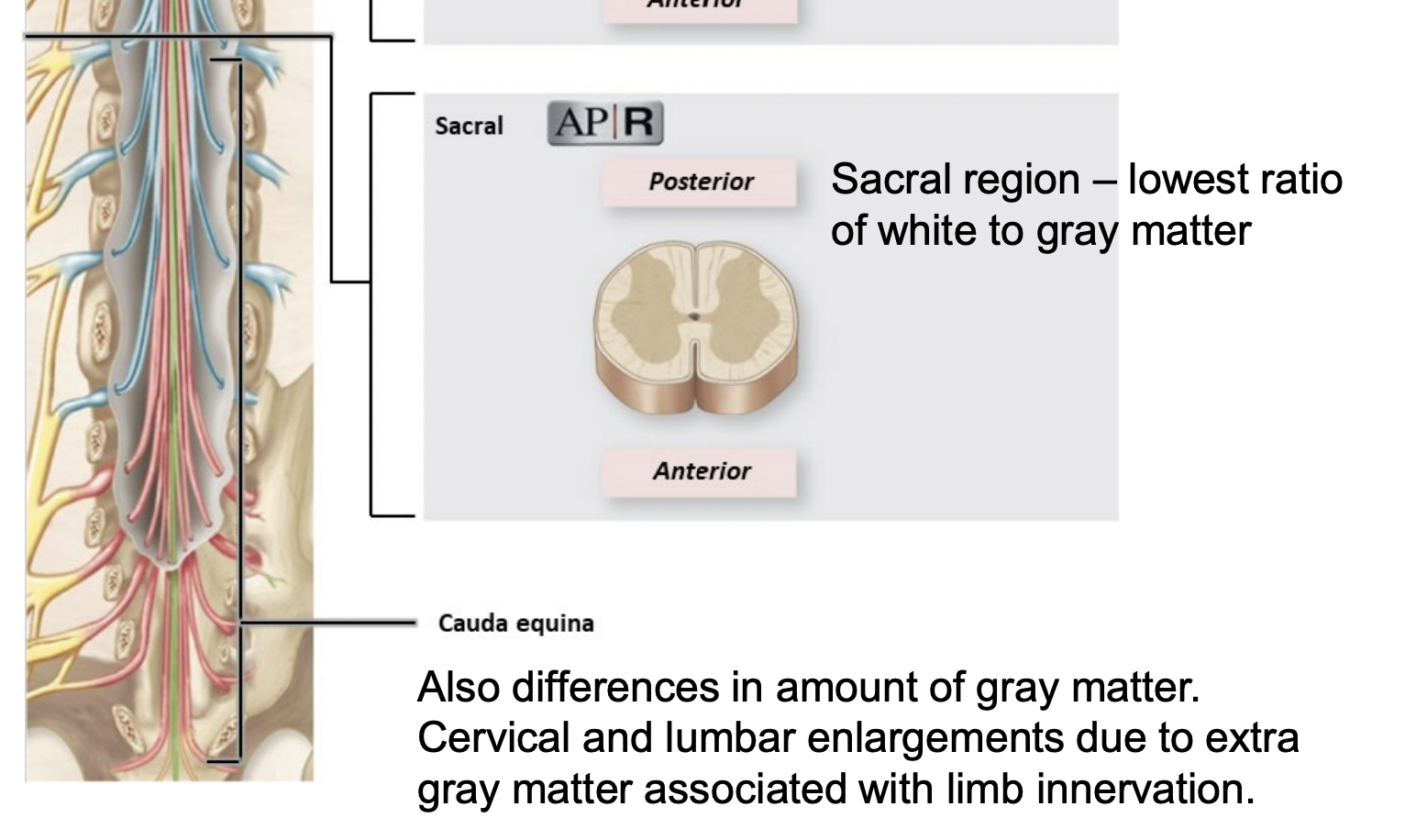
Sacral region
lowest ratio of white to gray matter
Differences in amount of gray matter
Cervical and lumbar enlargements due to extra gray matter associated with limb innervation
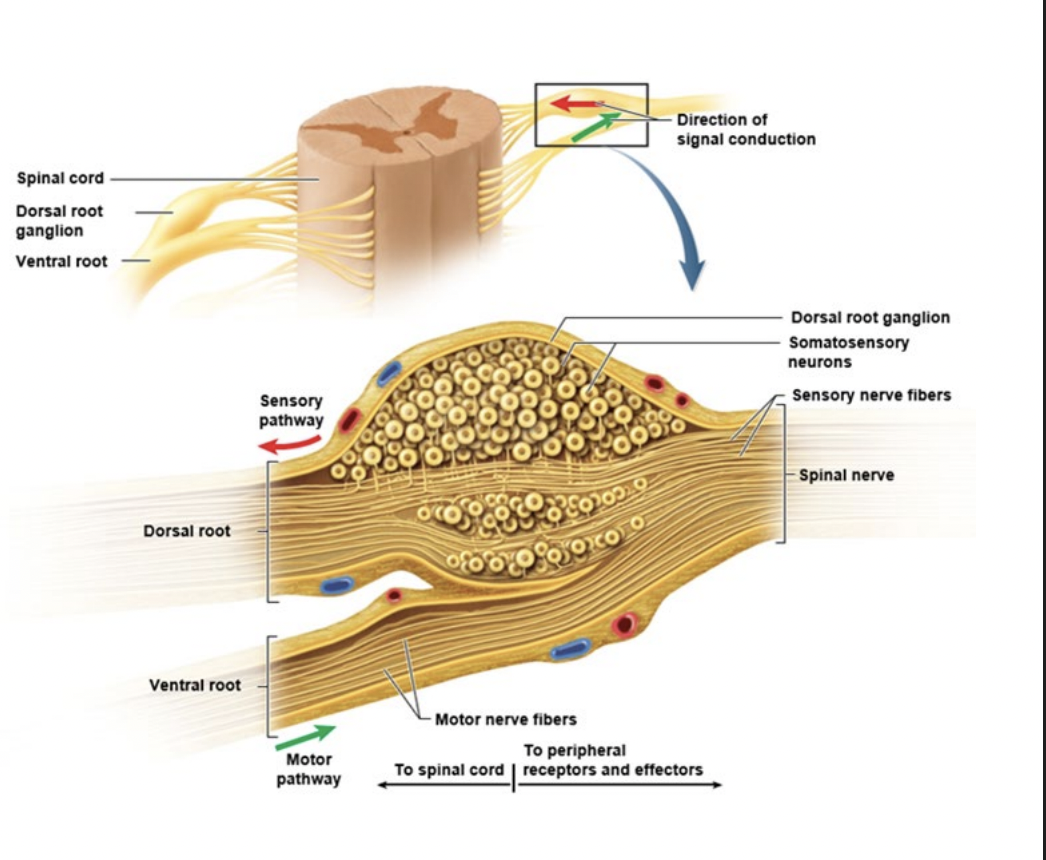
Rootlets
rootlets combine to form roots
Dorsal sensory & ventral sensory roots
these combine to form spinal nerves (mixed)
Branching of spinal nerve
they branch soon after the spinal nerve exits the intervertebral foramen
Main branches
Dorsal primary ramus
Ventral primary ramus
Dorsal primary ramus
innervates (supply) deep back muscles + associated dermis
Ventral primary ramus
Innervates (supply) everything else
Dermatomes
an area of the skin that is connected to a specific nerve root on your spine
All spinal nerves except C1 receive sensory input from a specific band/ region of skin
Concept of dermatomes and area it covers
map cutaneous (skin) regions innervated by each spine nerve
overlap at the edges up to 50%
Benefits of knowking dermatomes
assess the level of spinal injury
Diagnose shingles - distribution of lesions follow dermatomes
Chicken pox virus remains in the dorsal root ganglia for life
Reflexes
quick, involuntary, stereotyped reaction to stimuli - impact muscles & glands
Protective for body
Features of reflexes
Require stimulation, ie - input
Quick - very few neurons involved (minimal or no interneurons = minimal synaptic delay)
Involuntary - automatic - does not need stimulus to register at the brain - awareness comes later
Stereotyped - response is same everytime
Somatic Reflex Arc
Somatic receptors (skin, muscles, tendons, joints)
Afferent nerve fibres (sensory)
Integrating centre = point of synaptic contact
Efferent nerve fibres (motor)
Effector (muscles)
Somatic receptors
skin, muscles, tendons, joints
Afferent nerve fibres
sensory nerve fibers that carry signals to the central nervous system from sensory receptors.
Integrating centre
point of synaptic contact
Efferent nerve fibres
motor nerve fibers that carry signals away from the central nervous system to effectors such as muscles and glands.
Effector
Muscles
and glands that respond to signals from efferent nerve fibers.
Proprioception
sense of body position and movements
sensory nerve endings in muscle, tendons and joints
EPSP
Excitatory postsynaptic potential
IPSP
Inhibitory postsynaptic potential
Process of reflexes
Stimulus —> Receptor —> Afferent —> Integration —> Efferent —> Reciprocal Inhibition
Patellar tendon stretch reflex
is a protective reflex that causes an individual to withdraw a limb away from a painful stimulus.
Withdrawal reflex
lift injured food by flexing the knee (= ipsilateral reflex response - sensory input & motor output are on the same side of the body
Crossed extension reflex
stabilise opposite limb so you don’t lose balance
Contralateral reflex arc
stabilise opposite limb so you don’t lose balance
Contralateral reflex arc
sensory input & motor output are on opposite sides of the body
White matter tracts
exhibits 3 anatomically distinct regions
Funiculus in white matter
funis = cord
funiculus = little cord
dorsal (posterior), lateral, ventral (anterior)
Funiculi can be organised into small structural
Fasiculus
Fascis = bundle
Fasiculus = little bundle
Nerve Fibre (axons)
named tract have a similar origin, destination and function
Sensory & motor tracts
These tracts travel up and down the spinal cord
Ascending tracts
carry sensory information from the body to the brain
Descending tract
Carry motor information from the brain to the body
Spinocerebellar
starts in the spine, ends in the cerebellum - direction = ascending = sensory
Corticospinal
starts in the cerebral cortex, ends in the spine - direction = descending = motor
Sensory pathways to the cerebrum:
carry sensory information from the body to the brain for processing.
primary (1st order neuron)
Secondary (2nd order neuron)
Tertiary (3rd order neuron)
Primary neuron
cell body located in posterior root ganglion
Secondary neuron
Cell located in posterior horn or a brainstem nucleus
Tertiary neuron
cell body located in thalamus
Motor pathways
uses 2 motor neurons
one upper motor neuron and one lower motor neuron
Upper motor neuron
cell body located in cerebral cortex or a brainstem nucleus
Lower motor neuron
Cell body located in anterior horn or a brainstem nucleus
Tracts exhibit decussation
fibres cross to the opposite side of the body (contralateral origin & destination)
Do not decussate
fibres stay on same side of body (ipsilateral origin & destination)
Somatic sensory pathways
carry signals up the spinal cord (eg proprioception, fine two-point discrimination, pressure, light touch, pain, temperature, itch & tickle)
Neurons involved in sensory pathway
First order neuron
Second order neuron
Third order neuron
First order neuron
detects stimuli (unipolar afferent neuron)
Second order neuron
synapses at the thalamus
Third order neuron
carries signal to brain (e.g postcentral gyrus)
Fine two point discrimination
ability to identify two points applied to the skin as two not one
Why can we identify two points on the body?
due to sensory neurons detect stimuli within an area called a receptive field
for each receptive field, the same neuron is stimulated
Primary somatosensory cortex
Postcentral gyrus
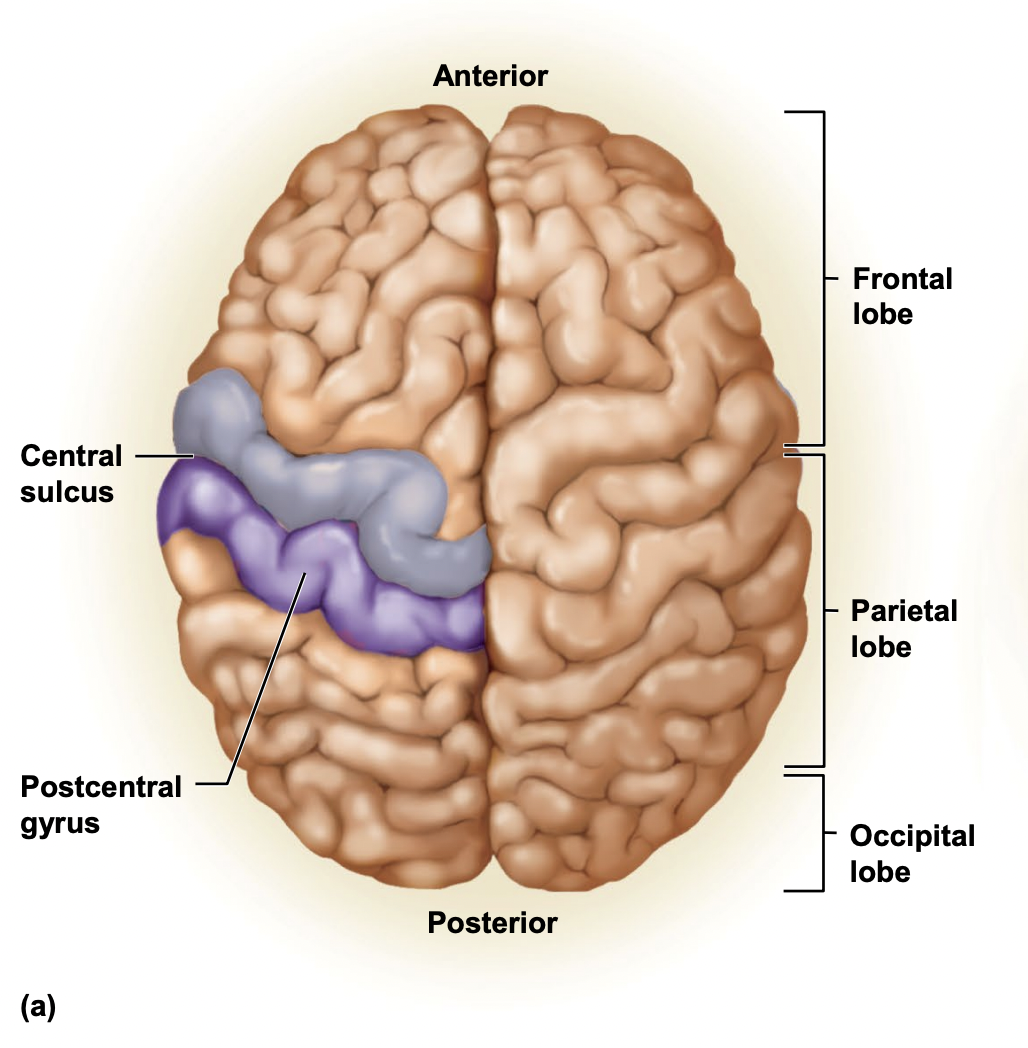
sulcus
A groove or furrow on the surface of the brain that separates adjacent gyri.
Gyrus
a ridge on the cerebral cortex, typically surrounded by sulci. It plays a role in processing sensory information and motor functions.
Motor (descending) pathways
carry motor signals down the spine
Neurons involved in motor pathways
Upper motor neuron and lower motor neuron
Upper motor neuron
located in brain (cerebrum, brainstem)
Lower motor neuron
located in the ventral horn of spinal cord gray matter
Purpose of upper motor neuron
can excite or inhibit lower motor neurons
Primary motor cortex
precentral gyrus
Spinal injury
Spinal cord trauma - paralysis:
Most common in 16-30yo males (high-risk behaviour)
Most commonly caused by car & motorcycle accidents, followed by sports injuries.
Complete severance (transection) of the spinal cord
interruption in pathways to the brain
During spinal shock
Flaccid paralysis below the site of injury & absence of reflexes
patient retains urines & faeces
Spinal shock passes
somatic reflexes reappear
through muscle & tendon reflexes (first in toes, then feet, then legs)
After spinal shock
the patient becomes incontinent because rectum and bladder empty reflexively in response to strech
End of spinal shock
Initial flaccid paralysis changes to spastic paralysis because spinal reflexes lack inhibitory control from the brain
Spastic paralysis
involved uncoordinated muscle spasms which can contort the limb