Gen Med - TBI
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
98 Terms
TBI peaks at which 3 age levels
- 1 to 2 years
- 15 to 24 years
- Elderly
TBIs ages 1-2 are often related to
Child abuse
TBIs in 15-24 are often related to
Risk taking
TBIs in elderly are often related to
Falls
A closed head injury often occurs when
Soft tissue of the brain is forced in contact with the hard, bony skill
In a closed head injury, there is focal injury to the
Cerebral hemispheres or brainstem localized to the area under site of impact
What is a coup-countrecoup injury
Damage to the opposite end of the brain during impact as the brain bounces off the inside of the skull
Grey matter contains
Neuron cell bodies and dendrites
White matter contains
Myelinated axons
Open head injury occurs when
The skull and meninges have been disrupted leaving the brain exposed
What are the mechanisms of injury of an OHI
- Penetrating missile injuries
- Scalp lacerations
- Compound fractures
- Usually focal brain damage
Acute management of a brain injury consists of
- Rapid triage
- Resuscitation
- Stabilization to prevent secondary spinal injuries
- Efficient transport
Level of consciousness
Glasgow coma score
Which signs are valuable in localizing brain stem damage and depth of coma
Oculomotor and pupillary
Anything greater than _ difference in size or asymmetry should be considered abnormal with pupillary signs
1mm
X-rays reveal
Skull fractures
CT scans reveal
Presence of hemorrhage, swelling, or infarction
MRIs allow for
Sensitive detection of mild TBI
PET scan can identify
Structural and functional consequences of mild TBI
EEC is most valuable for
Indicating seizure activities
EECs can be useful for predicting
Coma outcomes
Common complications of a TBI includes
- Pressure changes
Pressure change in the head is primarily due to
A lack of oxygen in brain tissue
Increased ICP is a result of
Swelling or intracranial hematoma
PTA on the glasgow coma scale is
Post traumatic amnesia
Normal ICP pressure is
4-15 mmHg
ICP pressure greater than _ is associated with increased morbidity
20 mmHg
Pressure changes are generally monitored in patients with
GSC of 7 or less or abnormal CT scan
Distortion of the brain can occur because
Fluid is contained in a rigid skull leaving no room for expansion
Increased intracranial pressure can lead to
Herniation of the brain
The most common herniation of the brain is the
Lateral tentorial membrane separating from the cerebral hemisphere from the posterior fossa
Compression of the brain stem and other structures can lead to
Paralysis and death
Pharmacological acute management of a TBI includes drugs that
Decrease ICP and BP
Elevated ICP greater than 20 mmHg is a significant predictor of
Poor outcome
Cerebral fluid volume can be controlled with
Mannitol to control blood volume
Cerebral edema can be treated with
Glucorticoids
Patients that have a TBI should keep their systolic pressure at a minimum of
90 mmHg
What drug is effective at maintaining systolic stability in TBI patients
Phenylephrine
What is a craniotomy
A removal of a portion of the skull so that the brain has room to swell
Pressure on brain tissue is created from
Swelling or hematoma
Perfusion refers to the
Perfusion in the brain tissue itself
What is perfusion
The passage of fluid through an organ or tissue
Intracranial hypertension can interfere with perfusion by
Lowering the cerebral perfusion pressure
Under normal circumstances cerebral perfusion pressure is maintained at
50-150 mmHg
Brain swelling can occur from
An increase in intravascular blood within the brain as a result of vasodilation and increased cerebral volume
Brain edema is
An increase in extravascular brain fluid
Compressive damage may occur when
The brain shifts from its normal symmetrical position
Brain shifting may cause
Compression of the brain stem, pituitary gland, or other structures in the brain
What are things to look for in TBI patients
- Arousal level
- Confusion or disorientation
- Changes in neurological status, posture, and tone
- Changes in bodily functions
- Monitor for signs of infection (open wound)
What are the clinical manifestations of a TBI
- Area specific
- Sensory impairments
- Abnormal tone
- Cognitive/behavioral impairment
- Balance/vestibular/coordination impairment
- Communication/speech impairment
- Visual-perceptual impairments
- Swallowing impairments
What functions does the frontal lobe control
- Voluntary movement
- Motor integration
- Expressive language
- Social functioning
- Inhibition of impulse
- Emotions
- Lack of initiative
- Short term memory
What functions does the temporal lobe control
- Hearing
- Smell
- Long term memory
- Receptive language
- Musical awareness
What functions does the parietal lobe control
- Sensation
- Comprehension of speech and reading
- Production of writing and calculation
- Awareness of spatial relationships
The occipital lobe is in charge of
Visual perception
The cerebellum is in charge of
Balance and coordination
The brainstem is responsible for
- Appetite
- Chewing and swallowing
- Hearing and balance
- Wakefulness
- Motor speech
- Upper intestine peristalsis
- Regulation of pulse, respiration, and BP
- Vision
- Eye and eyelid movement
- Smell
- Facial and neck muscle movement
- Facial sensation
- Taste
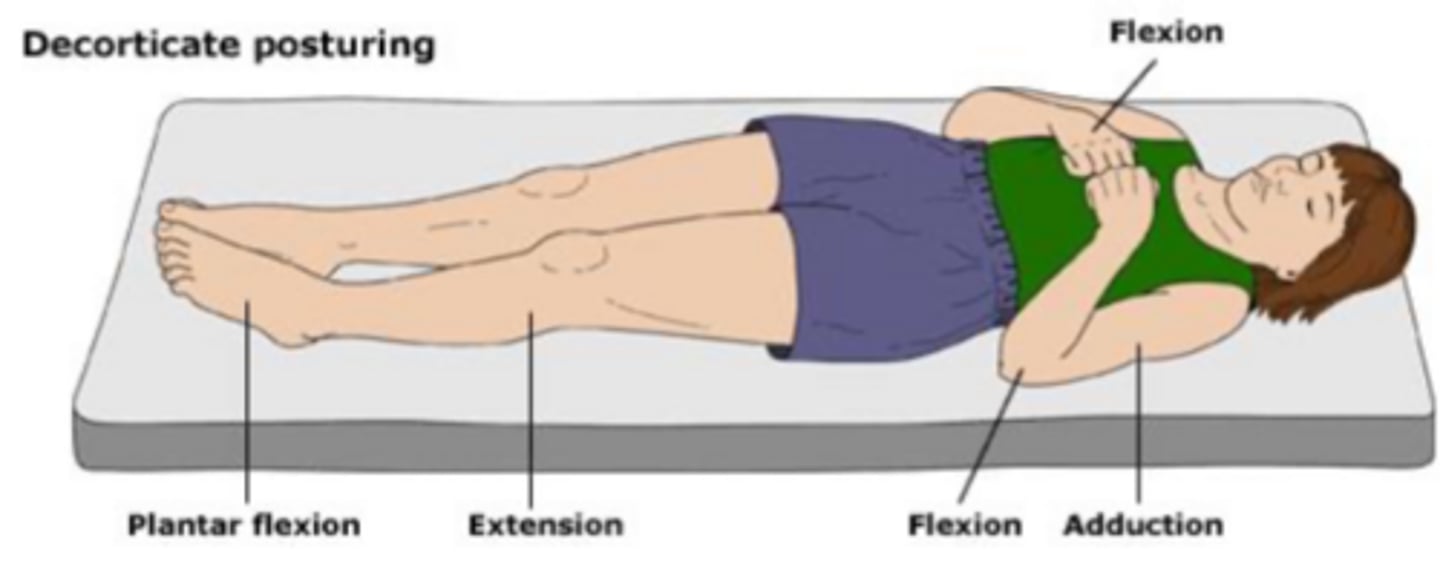
Decorticate positioning
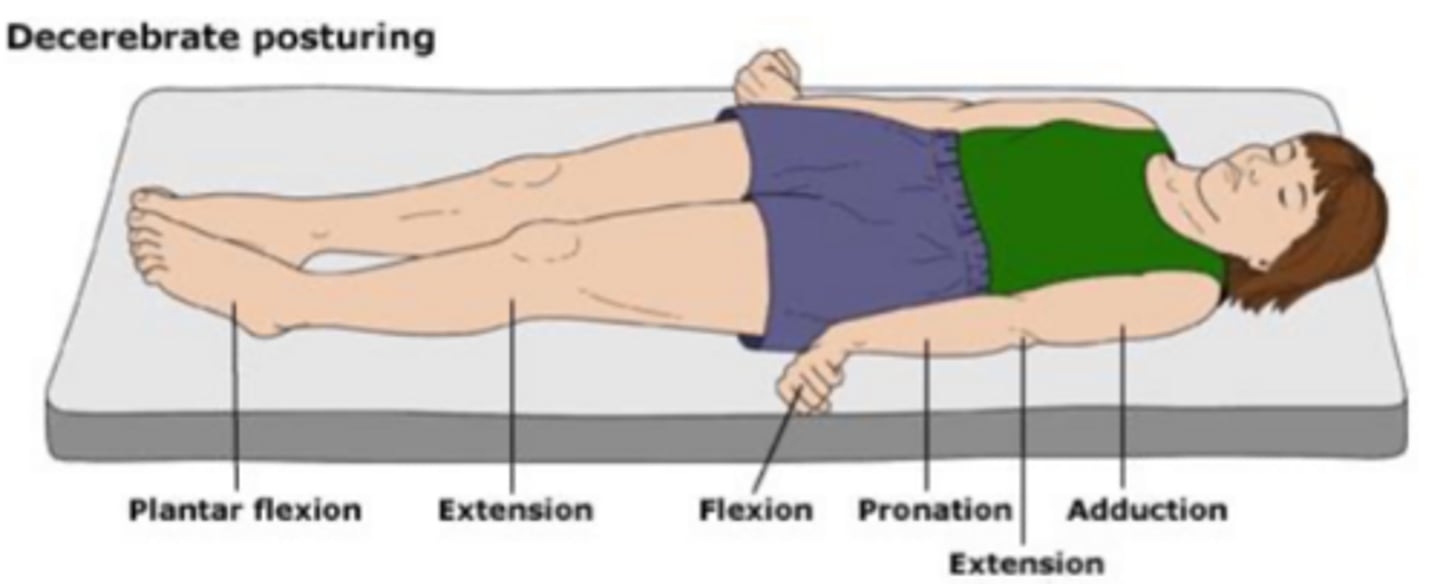
Decerebrate positioning
The glasgow coma scale is scored from
3-15
A GSC score of 8 or less indicates
Coma/severe head injury
A GCS score of 9-12 indicates
Moderate head injury, PTA>24 hours, LOC>30 min
A GCS of 12-15 indicates
Mild head injury, PTA<24 hours, LOC <30 min
Cognitive impairments include
- Problems with attention, memory, concentration, executive function
- Learning disorder, complex information processing, loss of abstract thinking and complex problem solving
- Confusion and disorientation
- Mood disturbances, depression, and anxiety
- Difficulty adjusting to environmental changes, erratic wandering, motor and verbal preservation
- Imitation of gestures, restlessness, refusal to cooperate
- Impulsiveness and hyperactivity
- Behavioral changes including irritability, agitation, acting out
- Sexual inappropriateness
- Lack of inhibition of social behaviors
- Emotional liability
- Confabulation
What is retrograde amnesia
The partial or total loss of the ability to recall events that occurred during the period immediately preceding the head injury
What is posttraumatic amnesia
The time lapse between the injury and the point where memory returns
What is anterograde memory
The ability to form new memory
Loss of _ is common in TBI
Anterograde memeory
Rancho levels of cognitive function ranges from
Level 1 to 10
Level _ of cognitive function is common in TBI patients
4
Level 1 of cognitive function indicates
No response; complete absence of observable change in behavior when presented with stimuli
Level 2 of cognitive function indicates
Generalized response; Generalized reflex response to stimuli, but may be the same regardless of type or location of stimuli
Level 3 of cognitive function indicates
Localized response; Demonstrates withdrawal or vocalization to painful stimuli and may respond differently to different stimuli
Level 4 of cognitive response indicates
Confused and agitated; alert and heightened state of activity, absent short term memory, non-purposeful movements, may cry and scream out of proportion to stimulus; aggressive behavior, and unable to cooperate with treatment efforts
Level 5 of cognitive response indicates
Confused-inappropriate; alert but not agitated, may become agitated to external stimulus, not oriented, impaired recent memory
Level 6 of cognitive function indicates
Confused-appropriate; inconsistently oriented, able to attend to highly familiar tasks in non distracting environment, vague recognition of staff, emerging awareness
Level 7 of cognitive function indicates
Automatic-appropriate; Consistently oriented, minimal supervision for new learning, able to attend to highly familiar tasks, carry over to new learning, initiates and carries out routines.
Level 8 of cognitive function indicates
Purposeful-appropriate; Consistently oriented, independently attends to familiar tasks, able to recall and integrate past and recent events, uses assistive memory devices to recall daily schedule
Level 9 of cognitive function indicates
Purposeful-appropriate; SBA on request; independently shifts back and forth between tasks and completes them, uses assistive memory devices, initiates and carries out familiar personal work, aware of and acknowledges impairments
Level 10 of cognitive function indicates
Purposeful-appropriate, Mod I; Able to handle multiple tasks simultaneously, independently procure and maintain assistive memory devices, independently initiates and carries out familiar work, anticipates impact of impairments
If sensory impairments are present in TBI patients, the pt and family should be educated on
Protecting the skin
TBi patients should be encouraged to attend to the
Involved side
Family and visitors should approach TBI patients on the
Involved side
TBI patients should get up on the
Involved side
When performing ROM exercises with TBI patients, give
Extra tactile input on the involved extremity
Which movements should have emphasis placed upon them in ROM exercises
- DF
- Knee extension
- Hip extension
TBI patients should be in _ as much as possible
Sitting or standing
Patients who have a TBI need _ on a regular basis
Orientation reminders
TBI injury severity is one of the main factors that determines
Outcome
What are factors that indicate a more favorable prognosis in TBI
- Absence of substance abuse
- Absence of previous TBI
- Higher education
- Stable work history
What condition might indicate brainstem damage and is associated with poor outcome
Loss of pupillary light reflex
What kind of deficits reflect cerebral damage consistent with severe cognitive deficits
Oculomotor
Within 7 days, the occurrence of _ is often related to poor outcome
Epilepsy
After the age of _, TBI patients have worse functional outcomes
40
Better TBI outcomes are possible is rehab is started
ASAP
PTA is better related to outcome than
Lesion size
What is a vegetative state
A persistent state characterized by reduced responsiveness associated with wakefulness
What is a severe disability
When the patient is conscious but requires 24 hour dependence
When assigning a level of cognitive function, it is necessary to
Observe an individual at different times of the day and in different settings