Topic 10 - Emotion
1/30
Earn XP
Description and Tags
guest lecture with Seth Winward
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
31 Terms
What is an emotion?
something of the body and of the mind
can be looked at as an evolved phenomenon that maximizes survival (evolutionary perspective) for reward-and-punishment circuits - conditioning
neural overlap between emotion and conditioning, but can’t all be conditioning since that’s not under conscious control
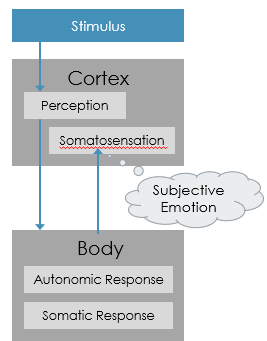
James-Lange Theory
says emotion is just a conditioned response
core idea is when we perceive some external stimulus and the feeling is perceived by somatosensory cortex, that’s where the subjective experience of emotion comes from
the response IS the emotion - we are sad BECAUSE we cry, we are angry BECAUSE our face gets red and not the other way around
Arguments about James-Lange Theory
evidence for:
pure autonomic failure: peripheral NS degenerates over time so patients can’t modulate physiological process via ANS - emotional bluntness
facial feedback hypothesis: mood will change by making an emotional expression suggesting emotional experience is caused by physical experience
botox cases: people with facial botox tend to report less intense emotional experiences after getting it
evidence against:
quadriplegic cases: can’t feel anything lower than the injury but still have regular emotional experiences
capgras syndrome: rare delusion in which people believe their family members have been replaced by imposters
physical damage prevents visual info from going to amygdala and hypothalamus and patient still has emotional response to parents and is scared of those seen as imposters
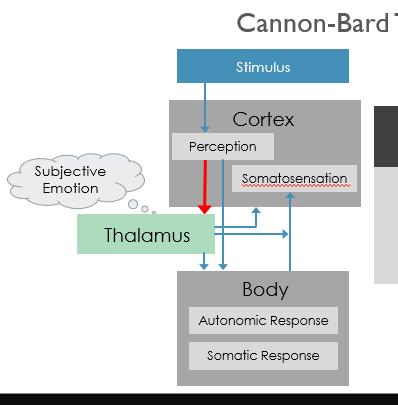
Cannon-Bard Theory
physiological change and associated emotion happen simultaneously
thalamus is where subjective emotion is processed and that is sent to the body and somatosensory cortex
based on animal neurophysiology where they would remove entire branches of the ANS without causing any change in emotional behaviours
removing cortex including somatosensory areas increased emotional behaviour which he attributed to removal disinhibiting activity in thalamus
Two-Factor Theory
Schachter and Singer induced physiological arousal with epinephrine injection with a different description of how the injection will make them feel
one group got accurate description
one got no description
one got wrong description
control group got no epinephrine and no description
talked to experimenter after injection who would either act rude or pleasant
researchers found people no explanation for how they felt were more likely to report their emotional state as same as experimenter - participants had same physiological processes attributed this to completely different emotions based on surrounding context
two-factor theory says stimulus is perceived and autonomic response happens
cognitive appraisal of physiological sensations gives rise to subjective emotional experience
Two-factor theory says …
our emotions are influenced by both our physiological state and the context of the environment surrounding us
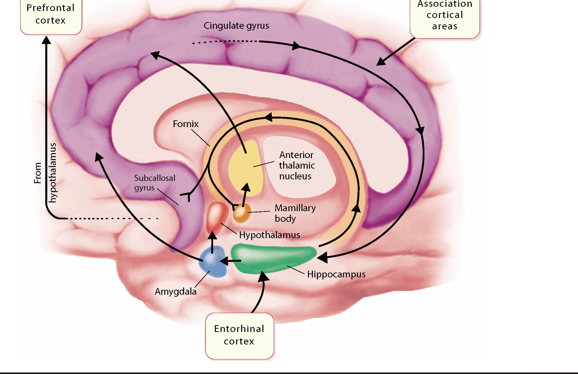
Subcortical Areas
limbic system is a primarily subcortical circuit that gets input from association and entorhinal cortex → cingulate gyrus and hippocampus respectively
limbic system is getting both sensory information and information from memory
after cingulate gyrus and hippocampus → amygdala → hypothalamus (other signals go through fornix and into mamillary bodies and the anterior thalamic nuclei)
hypothalamus → prefrontal cortex for basic emotional response → fornix, anterior thalamus, amygdala project back to cingulate gyrus which makes a loop
limbic system is NOT universal emotion center but is still important for emotion
Limbic System
subcortical structures are evolutionarily ancient and are not unique to humans, mostly in autonomic unconscious emotional responses
Kluver-Bucy syndrome: diminished fear response, low aggression, and no aversion to danger
was first seen in rhesus monkeys after bilateral lesions to medial frontal lobe (includes amygdala)
Amygdala and Fear Learning
amygdala is highly connected to other areas of brain and has receptors for neurotransmitters and hormones and has many nuclei
fear conditioning involves changes to lateral amygdala cells even if signals come from different brain regions like auditory cortex for loud noise and visual cortex for light - lateral amygdala cells react the same way
signals get projected from lateral to central amygdala then hypothalamus, etc for responding to stimulus
emotional conditioning doesn’t work without central amygdala
Severing pathway to lateral hypothalamus interferes with ___ fear response but not ____ fear response.
autonomic; behavioural
when LeDoux used fear conditioning paradigm with different brain areas - lateral hypothalamus and periaqueductal gray
when connection between central amygdala and lateral hypothalamus is severed, rates had appropriate behavioural fear response (freezing) but not autonomic response like no increased BP
therefore amygdala is not one-size-fits-all and different pathways are involved in different aspects of emotion
PAG in Brainstem
rats that got PAG lesions - when presented with conditioned stimulus, BP increased as you would expect for a healthy rat but without the behavioural response and autonomic parts of fear response
this shows that even tho behavioural and conditioned responses have amygdala, they have two separate pathways
amygdala is a choke point for fear processing, not fear center
3 Stages of Emotion
sensory processing - visual info comes to eyes and is sent to thalamus
low road (subcortical) - goes to amygdala for FAST unconscious response to dangerous stimulus → hypothalamus for sympathetic branch of ANS → HR increases, BP increases, muscles contract
high road (cortical) - conscious pathway through cortex where first thalamus info is processed from V1 → amygdala and cortical areas to think about your next move
Lesions to the Human Amygdala
patient SM had full complete bilateral lesions and specifically did not have subjective experience of fear and physiological responses to scary things were extremely blunted
couldn’t recognize fearful faces, draw a fearful face but was fine for other emotions
positive emotional responses were normal
no sense of personal space, doesn’t recognize situations as dangerous until too late (less situational awareness)
Cortical Role in Emotion
perception of emotion (interpretation)
expression of our own emotional state in face and tone
internal, subjective experience of our own emotions
purposes of this could be:
immediate response to a stimulus
influencing social behaviours such as tone of voice
communicating intent - emotions function as social behaviours e.g. giving someone a dirty look
subjective feelings - internal state of feeling something
Perception of Emotion
right lateral fissure is important for perceiving prosody and tone of voice
aprosidia: inability to comprehend someone’s tone of voice
Ekman faces are those that have the most universal emotions (anger, happiness, sadness, surprise, fear, disgust) - cross-cultural indicators of emotional states that are easily perceived and recognized by healthy participants
Prosopagnosia does not affect _____.
perception of facial expressions - even though they cannot identify whose faces are making those expressions
amygdala damage patients have difficulty recognizing all the basic emotions, especially fearful
amygdala damage patients don’t focus on eyes the way healthy people do
instructing people to attend to the eyes increases ability to recognize fearful faces back up to the level of a healthy participant
Expression of Emotion
RH has a dominance for emotional expressions so right side damage has difficulty perceiving others’ emotions and expressing their own
left side of the face is perceived as more expressive since contralateral control
with chimera stimulus, you see each side of the face mirrored to make its own face
participants rate faces made of two left halves as more emotionally intense than either the original faces or the faces of the two right halves
negative emotions are judged asymmetrically (left side is seen as more intense)
positive emotions tend to be judged symmetrically
Innate vs. Voluntary Expression
innate facial expressions are automatic in response to real emotion
voluntary facial expressions are consciously produced for any number of reasons
volitional facial paresis: difficulty in voluntary facial expression but can still do the innate ones in the case they are feeling the emotions, damage to motor cortex and subcortical connections
happens as damage to motor cortex and its connections, especially the parts of hypothalamus that are connected to cranial nerves
voluntary and innate expressions rely on different face nerves; the nerves in volitional paresis do NOT connect to Duchenne’s muscle, which is always involved in a genuine smile
emotional facial paresis has opposite symptoms
Emotional Facial Paresis
participants have no difficulty doing voluntary facial expressions but not when they are really experiencing emotion
damage to prefrontal cortex, thalamus, subcortical white matter in frontal lobe → connected to Duchenne’s muscle which is paralyzed
Expression of Prosody
affective prosody = emotional tone → perception and expression of this are localized to cortical areas surrounding the lateral fissure in the right hemisphere
propositional prosody is for semantic information
left hemisphere could be for propositional prosody, or for just language production areas incorporating prosodic cues that are processed in the right hemisphere
Experience of Emotion
Damasio and colleagues: studied patterns of neural activation for sadness, happiness, anger, fear
used PET scans to investigate neural activity
participants lie in scanner and remember emotionally intense moments of their lives with emotionally natural recollection of a regular day
used skin conductance, HR, and self-reports to confirm emotional response
Experience of Sadness
significant activation:
Bilateral anterior insula
Anterior cingulate cortex
Right basal forebrain
Right OFC
Dorsal pons
significant deactivation in posterior cingulate cortex
Experience of Happiness
significant activation:
right posterior cingulate
right anterior cingulate
left insula
left SII
significant deactivation in left anterior cingulate
basically the reversed pattern for sadness, and is lateralized
Experience of Anger
significant activation:
pons and midbrain
left anterior cingulate
right insula
significant deactivation in bilateral SII and right orbitofrontal cortex
Experience of Fear
significant activation in midbrain and left insula
significant deactivation:
right SII
hypothalamus
bilateral orbitofrontal cortex
Valence and Arousal
valence: positiveness or negativeness of emotional state
arousal: how strongly you feel positive or negative
right hemisphere is specialized for negative affect, left for positive
widespread LH damage → emotional lability (mood swings with little to no control over emotions)
widespread RH damage → euphoric indifference (very happy when it is not appropriate)
Mood Disorder Symptoms
adynamia: flat affect from lack of modulation of emotional expression (can be positive or negative emotions)
anhedonia: loss of pleasure from normally pleasurable things
have similar profile of symptoms, differentiated by whether actual emotional state matches
Depression Overview
defining symptoms are anhedonia, chronic sadness, hopelessness
other common symptoms:
changes in appetite
insomnia
lethargy
cognitive deficits like biasing memory and attention towards negative interpretations of things
low self-esteem
suicidal ideation
Depression and the Brain
dIPFC hypoarousal, disconnected from ACC so doesn’t regulate activity
subgenual cingulate cortex is hyperactive, involved in regulating body functions during rest
hemispheric asymmetries - right is more active, less decreased in left frontal lobe
amygdala activation persists in response to negative stimuli
ventral striatum hypoarousal
hippocampus is less active for encoding positive stimuli
Anxiety Overview
includes phobias, generalized anxiety, OCD, PTSD
key dimensions are anxious apprehension (worrying) and anxious arousal (panic) such as activation of sympathetic NS
Anxiety and the Brain
hyperactive amygdala since fear response to specific triggers compared to controls
HC smaller in PTSD since flashbacks and memory loss comes from stress hormones that are released that destroy HC tissue
ventromedial prefrontal cortex hyperactive to threat so doesn’t regulate amygdala as well
ACC overactive at rest and during threat since it monitors action
anxious apprehension associated with left frontal cortex therefore speech centers
anxious arousal associated with posterior right cortex