Cognitive Neuroscience Exam #1
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
96 Terms
2 Kinds of Brain Cells
1) Neurons: transmit electrical signals and do information processing (~100 billion)
2) Glia cells: non-electrical supporting, cells (more than half of the brain’s volume)
Neurons
Specialized cells for the processing and transmission of information
Occurs through electrical and chemical communication (only cells that communicate like this)
Cell body, dendrites, axon, and myelin sheath
Shape varies by function
Dendrites
Antennas that receive information from other neurons
Contain many branches (dendric tree)
Also may have little bumps called dendritic spines (result of learning something)
Axon
Sends information to other neurons
Typically the longest part of a neuron
Myelin Sheath
Insulates the axon (bumps in diagrams)
Helps transmission of signals
Made up of a type of glia
Fatty, white
Make up the white matter of the brain
Fiber tract: groups of axons going to the same place
Myelination has a developmental course
Disruptions/damage can lead to neurological disease (e.g., multiple sclerosis)
Glia
Supporting cells
Critical to:
Modulating communication between neurons
Supporting connections between neurons
Guide developing neurons
Removing dead neurons & and help with reorganization when there is brain damage
Blood Brain Barrier
No blood IN the brain
Keeps a protective barrier to keep toxins out
Glia help get nutrients from the blood to the neuron
Neural Communication
Neural transmission inside the cell (via electrical changes)
Dendrites (mostly) receive information
Collects in the soma
Information is sent down the axon to the axon terminals
Sends to other cells via electrical changes in the cell which in turn activates the synapse (the connection to other neurons)
Communication between cells (via chemical transmission)
Cell Membrane
Separates the inside of the neuron from the extracellular fluid
The fluid inside and outside the neuron are filled with ions (charged atoms)
The inside concentrations are different from the outside concentrations
Electrical Signals
Cell membrane keeps some ions inside the cell, and some outside
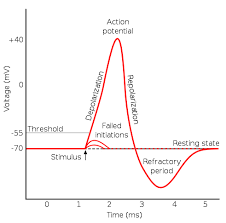
When a neuron is at rest, the inside is negatively charged compared to the outside of the neuron
Resting potential (-70 mV)
When a neuron receives activity from another cell it can affect the concentration of ions
Input from other cells can either open or close channels that allow certain ions in or out
The change in ions due to this connection change the electrical charge of the neuron
Action Potential
neuron firing, or “spikes”: change in charge
If the connection sends +ions in the cell (Na+), it becomes more positive
If positive enough (-55 mV) threshold of excitation occurs
The neuron “fires”
Sending the charge, rapidly to a peak of +40 mV
Depolarization
Repolarization- potential moves back to resting potential
Hyperpolarization- briefly becomes more negative
Once started, neuron cannot fire again until back to resting state
Some connections can make the cell more positive (sending +ions into the cell)
Some connections can make the cell more negative (sending -ions into the cell)
Hyperpolarizing the neuron
Taking it further away from having an action potential (inhibition)
“All or nothing”
Was the threshold of excitation reached?
Magnitude isn’t different with stimuli, but rate of firing is
Neuron to Neuron Communication
Transmission between cells is chemical- neurotransmitters
Released by presynaptic cell (axon)
Across the synaptic cleft
Received by the receptors on the postsynaptic neuron
Opening channels that either depolarize the neuron or hyperpolarize the cell
End result is postsynaptic neuron either having an action potential or not
Based on the neurotransmitter passed and whether there is enough signal to pass the threshold of excitation
In the end, all behavior boils down to this
Nervous System
Peripheral Nervous System (anything outside of brain and spinal cord)
Central Nervous System (most relevant to this class)
Each vertebrae covers a section of the body
Damage can result in lack of sensation in or motor control for the body areas served by the spinal cord at damage or below
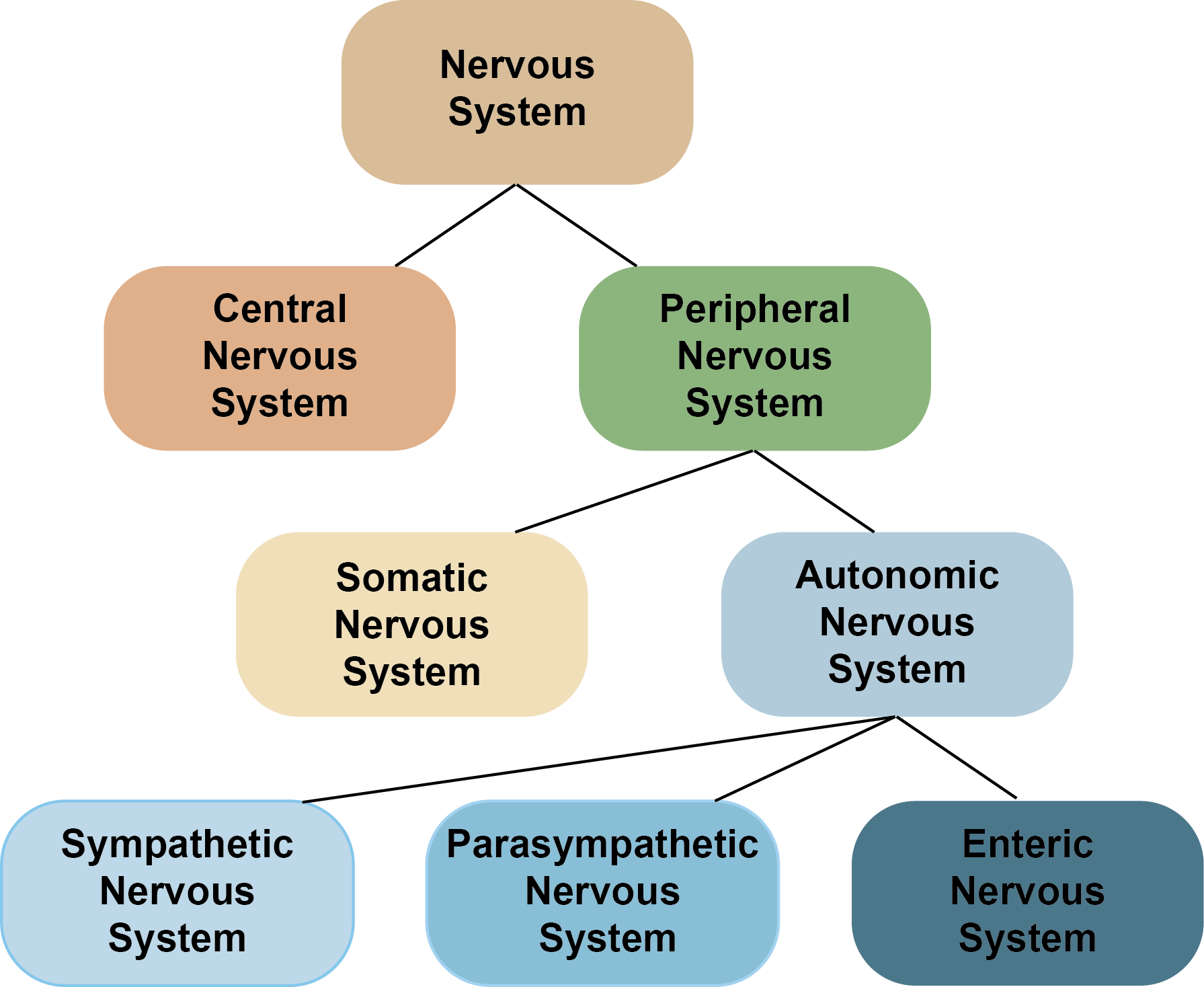
Peripheral Nervous System
Somatic NS: controls muscles, sends sensory information to the brain
Autonomic NS: made up of sympathetic nervous system (fight or flight) and parasympathetic nervous system (rest and digest systems) as well as new enteric nervous system (gut/brain axis)
Central Nervous System
Most sensory information (e.g. touch, pain) relay through the spinal cord
All motor commands from the brain are sent to muscles via the spinal cord
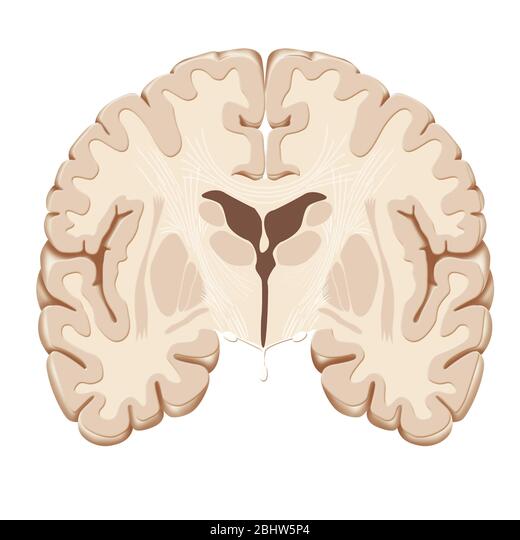
Main Tissues of the Brain
Gray matter= neuronal cell bodies
White matter= axons, myelin, and glia cells
Represents the axonal connectivity of the brain
Most notable fiber tract: corpus callosum
Within hemispheres, between hemispheres, and between cortical and subcortical regions
Ventricles= hollow chambers filled with cerebrospinal fluid (CSF)
CSF resembles blood plasma, but there’s no blood because of the blood-brain barrier
4 main ventricles
Has direct implications for traumatic brain injury (TBI)
Meninges
Membranes that surround the brain and spinal cord
Protect the CNS
Meningitis= inflammation of the meninges
Sagittal Plane
Bisects the body into right and left halves
Coronal Plane
Divides the body into front (anterior) and back (posterior) regions
Horizontal Plane
Divides the brain into upper and lower parts (also called “transverse” or “axial” plane)
Anterior
Head end (also called “rostral”)

Posterior
Tail end (also called “caudal”)

Dorsal
Top part (also called “superior”)
Ventral
Bottom part (also called “inferior”)
Distal
Far part of brain
Proximal
Near part of brain
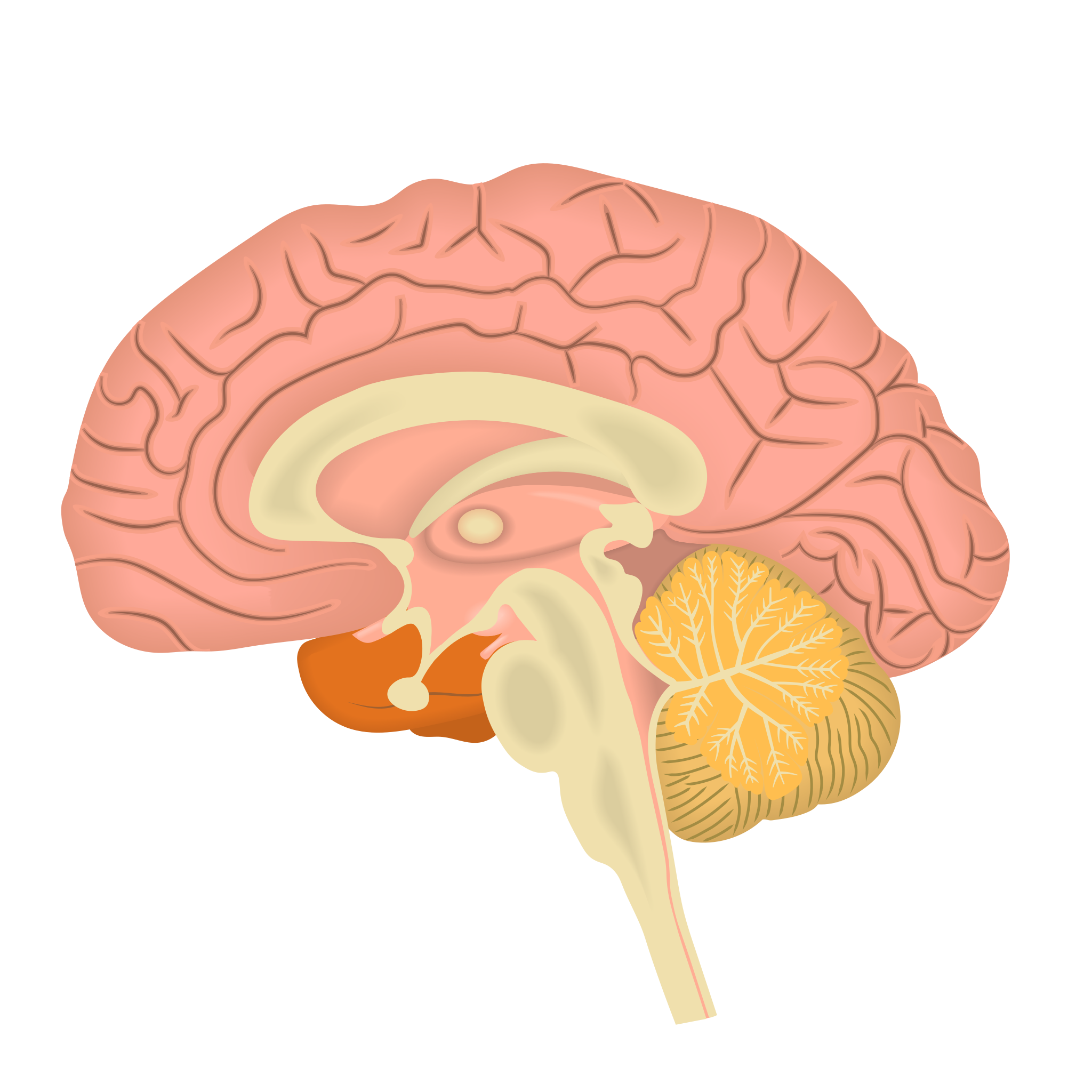
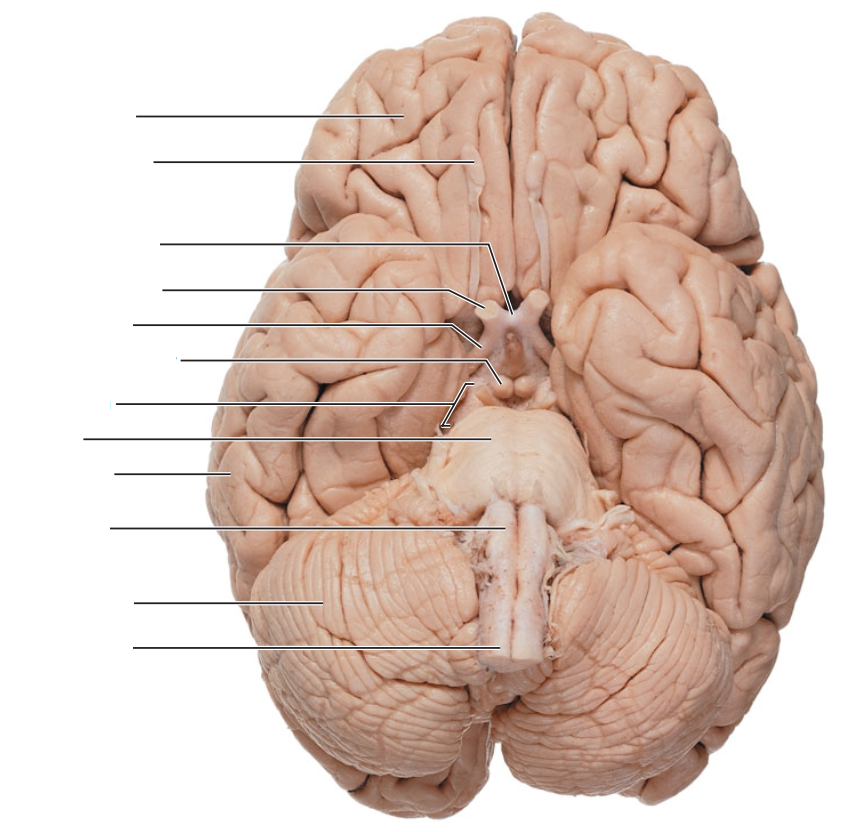
Brain Stem and Hindbrain
All part of brain stem, critical to survival, rough sensory processing, motor tracts, and cranial nerves
Medulla
Pons
Midbrain
Cerebellum
Medulla
Sits on top of spinal cord
Pretty critical to basic functioning
Respiration, heart rate
Arousal (via reticular activating system)
Motor tracts
Pons
Sits on top of medulla
Lots of connective pathways
Balance and eye movements
Sleep cycles
Supplier olive: important stop in the auditory pathway
Midbrain
Sits on top of pons
Some cranial nerve action
Visual and auditory orienting mechanisms
Cerebellum
Important for movement (tone/balance, muscle guidance and control)
Learned movement
Controls the timing aspect of movement
Involved in cognition at large
Contains all inhibitory neurons and about ⅓ of neurons in the whole brain
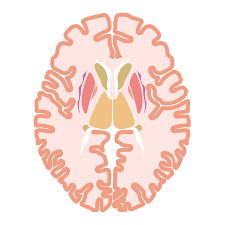
Subcortical Structures
Hypothalamus
Thalamus
Basal Ganglia
Limbic System
Hypothalamus
Maintains equilibrium via endocrine system (hormonal system)
Eating thirst, body temperature, etc.
Thalamus
Gateway to cortex
Relay center for almost all sensory and motor information
Divided into different regions that subserve pathways for different systems
Basal Ganglia
Collection of nuclei
Dopamine nuclei
Related to movement and implicit/autonomic memory
Highly connected to frontal lobe
Limbic System
Collection of structure (amygdala, hippocampus, cingulate cortex)
Important for relating the organism to its environment based on current needs to the present situation, based on previous experience
Implicated in emotions, learning, and memory
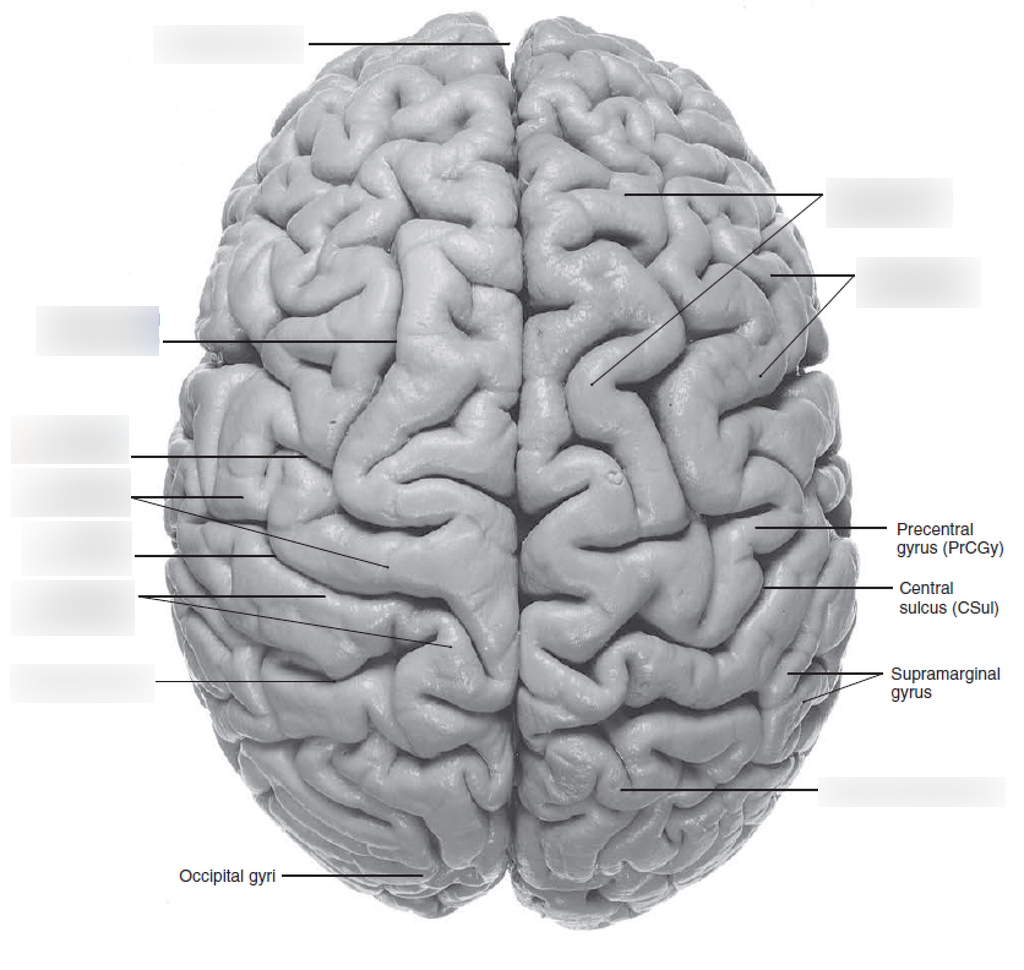
Cerebral Cortex
sulci= grooves, gyri= bumps, fissure= deep sulci
Folds increase surface area
Sulci and gyri are very stable across individuals and species
That’s why atlases work
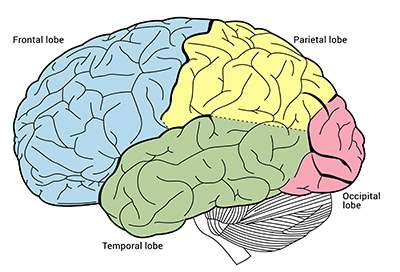
The cortex is divided into four lobes/cortexes:
Frontal (most anterior region)
Parietal (region between the frontal and occipital lobe)
Occipital (posterior region, visual processing)
Temporal (lateral region, auditory, visual, semantic and language processing)
Major Landmarks: Central Sulcus, Sylvian Fissure, and Longitudinal Fissure
Primary Cortex
Primary visual cortex
Primary auditory cortex
Somatosensory cortex
Primary motor cortex
Associate Cortex
Non-primary cortex
Typically doing higher level processing (learning, planning, memory, etc.)
Can be unimodal (one sense) or multimodal (multiple senses)
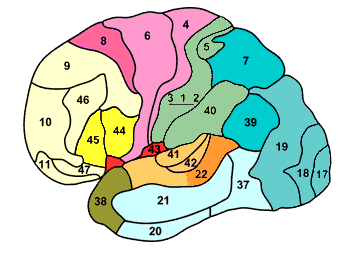
Brodmann Areas
Different regions of cortex have been demarcated by histological examination of the cellular micro-anatomy aka cytoarchitectonic maps (~50 regions)
Direct Neuroimaging Methods
Directly measures neuron activity
Indirect Neuroimaging Methods
Measuring something that correlates with neuronal activity, e.g. fMRI
Limitations of Neuroimaging
The physical properties of the recording system
The physiological constraints of the brain
Images of brain activity only have meaning when using the correct experimental design and interpreted using the correct analysis
Lesions
Lesions are a result of traumatic brain injury, surgical resection, strokes as a likely reason, and disease
Gold standard of learning about brain-behavior relationships
Studying the impaired, we can learn about the unimpaired
Can determine cause and effect
Strengths of neuropsychology are establishing causal relationships (changes in behavior due to changes in cortex)
Brain Lesion Studies
Single case studies (provides great insight, but does it generalize?)
Group case studies (more support of general mechanism, but difficult to find multiple patients with similar lesions)
Group can be heterogenous
Lesion can be heterogenous (size, severity, isolated damage)
Double Dissociation
Normally derived from 2+ single cases with complementary profiles of strengths and weaknesses
Used to infer the two tasks/stimuli use separate neural/cognitive resources
Weaknesses of Brain Damage Studies
Damage is largely dictated by vasculature (strokes)
Damage is typically large
Size and shape depend on injury
Not specific to anatomical or functional boundaries
Functional deficits are rarely selective
Individuals may experience cortical reorganization
Limits the extent to which we can generalize from specialized populations
Moreover, still making conclusions about what can’t be observed, only observing regions critical to behavior (not the whole network of regions), and the brain may compensate
Lesions limited to the patients that present to you (most other methods you can design experiments and test hypotheses)
Transcranial Magnetic Stimulation
TMS
Transient and safe disruption of local neuronal activity
Scrambles neuron firing
“Virtual lesions”- causal link
Provides both information about “where” and “when”
Important to have a control site
Two types: single-pulse TMS and rapid TMS (rTMS)
Can makes claims of causality, but can only get lateral surface of the brain and have to already know where to look for an effect
Transcranial Direct Current Stimulation
tDCS
9v battery
Stimulated anodal (positive) electrode- increase activity
Stimulated with cathode (negative) electrode- decrease activity
Less intense and less focused than TMS
Single Unit Recording
Measuring the action potential of neurons
Recording the changes in electrical potentials through an electrode inserted through the brain
Highly invasive- animal studies
Typically intracellular recordings
Electrocorticography
ECoG
Electrode implantations in humans- done for medical reasons only
Epilepsy- seizures may be induced by aberrant neural activity in a focal region
May be able to relieve symptoms by resecting that region- last resort
Intracranial Electrodes
Not just passive recorders
Can stimulate too!
“If this neuron/area is stimulated, we expect to see a change in X behavior”
Penfield pioneered brain stimulation: testing for local, critical function “eloquent cortex”
Therapeutic means: deep brain stimulation for Parkinson’s, tremors, etc.
Neurophysiology
Recording directly from neurons!
Great temporal and spatial resolution
Both passive measurement and active manipulation
Electroencephalography
EEG
Measures electrical activity that is readable from the scalp
Omnibus recording technique
The potential from a single neuron is too small to be picked up
Measures populations of neurons with synchronized potentials & oriented similarly
High temporal resolution (ms) but poor spatial resolution
Magnetoencephalography
MEG
Measures magnetic field activity that is readable from the scalp
High temporal resolution (ms) but poor spatial resolution (MEG has better spatial resolution than EEGs though)
Event Related Potentials
ERPs (EEG and MEG signal)
Evoked response as a function of task
Takes the average of MANY trials
Identifiable peaks and troughs in electrical activity
Strange convention: up=negative
Are measured based on their amplitude
E.g. the P1- the first “major” positive waveform measured over lateral occipital cortex
Attending to specific region of space modulates the amplitude, but not latency, of the contralateral P1
Oscillations
EEG and MEG signal
Steady state measures of ongoing waves of EEG activity over a period of time
Frequency= the speed of the peaks and troughs
Looking at the power of different frequency bands
Power analysis (which frequency bands are the strongest and when)
Time frequency analysis (frequency bands can indicate different types of cognition)
Source Localization
Hard to know where the source of the signal is coming from
Inverse problem- many sources can lead to the same EEG response
EEG and MEG Pros and Cons
Advantages
Direct measure
Noninvasive
Has excellent temporal resolution (ms)
Disadvantages
Requires large populations of neurons to be synchronized
Has poor spatial resolution (on the order of cm)
Localization of source can be complicated (MEG better than EEG)
CAT Scan
Structural
Derivative of X-rays
Good at seeing fluid or different tissue mass in the brain
Positron Emission Tomography
Records emissions of radioactivity from injected radioactive chemicals
Can tag certain molecules (e.g. look at neurotransmitters)
Can look at metabolism of neurons (e.g. glucose consumption)
Three Types of Data from MRI
MRI Structural Data
fMRI Functional Data
Diffusion Weighted Imaging (DWI, structural)
MRI Structural Data
Different tissue types (grey matter, white matter, CSF)
Each tissue has different physical properties under MR imaging
Static- a snapshot of the brain
Very high resolution
Types of analysis
Look for damage
Size of region
Grey matter thickness
Diffusion Weighted Imaging
White matter connections in the brain
Integrity of myelination (e.g. MS)
“Looking at flow of water in the brain, and how it is different in different tissues”
Color (hue)= direction of the highest diffusion
Brightness= degree of anisotropy
Looking at uniformity.integrity of direction
Tractography
Good for looking at connections in the brain
fMRI
fMRI signal= Blood Oxygen Level Dependent (BOLD)
We are looking at blood, not looking directly at neural activity
Oxygenated and deoxygenated blood have different magnetic response times
basic model of relationship between BOLD fMRI and neuronal activity correlational (not causal)
Two things have massively improved over the years:
Spatial resolution (field strength [Tesla] and more advanced protocols)
Sophistication of analysis and design techniques (partly due to all low hanging fruit already picked)
fMRI Pros and Cons
Advantages
Great spatial resolution ~mm
Can image the whole brain
Don’t need to preselect where to measure
Non-invasive
Can design hypothesis driven experiments
Disadvantages
Poor temporal resolution
Indirect measure of brain activity
Looking at correlations not causality
Some individuals cannot participate (e.g. anyone with magnetic implants, such as pacemakers)
Some individuals do not like to participate: it’s a confined environment (claustrophobia and VERY loud)
Must lay still for ~1 hour
Very expensive (~$1000 a subject)
fMRi signal is slow
Hemodynamic response function (change in BOLD signal over time)
Temporal resolution of fMRI signal is mostly limited by the sluggishness in the hemodynamic response to stimulus presentation
Types of fMRI Analysis
Whole brain analysis
More exploratory
Region of interest analysis
Pick a priori region of brain to investigate
Subtraction Method
fMRI analysis method involving averaging together all the images acquired during the 'on' phase of the task, and subtracting the average of all the “off” images
Adaption Method
fMRI analysis method where region is selective for specific stimulus
Multi Variate Pattern Analysis
MVPA
fMRI univariate contrasts and adaptation designs look at the average activation across a region
Looks at the pattern of activity voxel-by-voxel
Look at the similarity in the pattern of activity to learn about how information is processed and presented in the brain
e.g. through correlation
More similar- the more evidence they relate to the same function/representation of the region
Functional Connectivity
fMRI analysis method showing correlation between time series from different regions; infer communication between regions
Brain Reading
Brain response can be used to predict which object is seen or imagined from a limited set (e.g. face v. house, bottle v. shoes)
However, can only be done if experimenter pre-tests the participants on these items (to know where to look in that particular person)
Think about what the comparison is
Reconstruction
fMRI Pitfalls
Reverse Inference
Not a 1:1 relationship of brain and behavior
Individual Differences
Group averages are sometimes misleading
Lots of individual variability
Default Mode Network
Areas of the brain that were more active at “rest,” or more tuned in to internally generated thought
Can use that as a tool to examine and understand brain function
Tasks and default network are anti-correlated
“Baseline is greater than task, rather than task greater than baseline”
Can use the default network and resting activity to explore brain function, especially across different populations
Hierarchy of Action
Lowest level of movement= reflexes
Highest level of movement= voluntary planned action based on goals and intentions
More basic cognitive mechanisms in action include:
Object recognition
Locating an object in space
Linking object with limb positions and motor commands (sensory-motor transformation)
Knowledge of the present state of the body (somatosensation) and position of limbs in space (proprioception)
Selecting a specific movement (direction, force etc.)
Generating the movement
Monitoring the progress and outcome of the action (feedback)
Higher cognitive mechanisms include:
The goals, plans and intentions of an individual
Stored semantic knowledge of objects and their uses
Stored motor programs for specific objects (e.g. lifting cups) and schemas for familiar situations (e.g. making tea)
Motor Neurons and Reflexes
Reflex- quickest movement to control movement
Stretch reflex, signalling goes through spinal cord (not up to brain)
Regulates the length of the muscle
Allows things like posture stability to be maintained without involving the cortex
Number of muscle fibers a neuron innervates relates to precision of movement (less fibers= less precision)
Motor Tracts
Motor complex movements signals sent from the brain via motor tracts
Organization of the tracts is meaningful of how our brain executes movement
Lateral corticospinal tract: and medial corticospinal tract:
Lateral Corticospinal Tract
Distal limb movements (arms, fingers, legs, foot, etc.)
Fine motor control
Cell bodies in primary motor
Contralateral control- crosses at the medulla
Medial Corticospinal Tract
Trunk and proximal limb muscles
Postural control, bilaterally constrained movements (e.g., walking, bending)
Contralateral control and Ipsilateral control
Cortical Motor Regions
Primary Motor Cortex (M1)
Supplementary Motor Complex
Premotor areas
Frontal eye fields
Anterior Cingulate
R Inf. Frontal Cortex
Parietal Lobe
Primary Motor Cortex
Executes all voluntary movements of the body
Somatotopically organized and crossed (left hemisphere= right side of the body)
Stimulation results in movement
Cortical magnification
Might be organized by behavior rather than body
Damage
Weakness or hemiplegia (the loss of voluntary movement on the contralateral side of the body)
Primary motor neurons have a preferred direction
Fire a little less for nearby directions; a lot less for very different directions
Other information coded (not sure how these are coordinated):
Force
Torque
Trajectory and distance
Cortical Magnification
The amount of cortical space given to body part is not with respect to the size of the body part, but the precision and extent of movement
Population Vector
Problem: Many neurons in M1 fire for a single movement, although they may have many different preferred directions.
How to know where to go? (Most active neuron?)
But movement is very precise and the preferred direction is quite broad…
Solution: Population vector
Take the summed activity
Very precise direction
Motor Plan
An abstract representation of intended movement
The brain generates this entire plan of action before movement commences rather than creating the plan in a step-by-step manner as actions are being performed
Implemented via supplementary areas
Supplementary motor area (SMA)
Premotor cortex (PMC)
NOT primary motor cortex!
SMA and PMC modulate activity in primary motor to execute commands to move the muscles
Supplementary Motor Cortex
Plays a role in planning, preparing, and initiating movements
Both contralateral and ipsilateral control of M1, and also feeds into contralateral SMC
Damage results in bimanual coordination impairment
Can’t use hands independently
Motor planning
Active before action
Active for a specific sequence
Not active for repetitive movements
Complex movement
Sequential movements
Coordination between limbs
TMS reduced ability to perform sequenced motor program
Deals with spontaneous well-learned actions that don’t place strong demands on the environment
Initiated by internal goals
May be involved with more domain general sequential processing
Numerical processing, working, memory, musical processing, language
Premotor Cortex
SMC → PMC → M1
Dorsal region: integrates motor commands with sensory cues
Ventral region: integrates with manipulating specific object
How it’s actually done. Moving from abstract representation of movement (SMC) to more concrete commands (PMC)
Ex./ wanting to spread cream cheese on bagel to actually determine how the hand, fingers, arm, etc. will perform the task
Frontal eye fields
Voluntary eye movements
Distinct from reflexive eye movements (midbrain- superior colliculus)
Mirror neurons
Mirror Neurons
Respond to observed as well as self-enacted actions
Part of action comprehension
Basis of learning via imitation, and understanding action of others
Foundation of communication?
Embodied cognition
Anterior Cingulate
Most involved when an action is novel or requires cognitive control
Such as when a well-engrained response must be overwritten
Involved in regulating the consequence and correcting
Stroop task
May modulate or override activity during simple motor tasks (most posterior)
May modulate the selection of movements
May modulate more complex motor actions or become active when a high degree of conflict exists
Posterior → anterior
Gradient of going from more simple to more complex (most anterior)
Prefrontal Lobes in Action
Involved in coordination of cognition generally (both external actions and internal thoughts)
Involved in selection and maintenance of goals and responses
Damages to this region does not impair physical movement but actions become inappropriate or disorganized
Perseveration (action repeating)
Utilization of behavior (act impulsively on irrelevant objects)
Parietal Cortex
Integrates sensory information with movement
Spatial maps, and spatial map translation (e.g., into hand centered coordinates)
Overlaps with “where” or “how” visual stream
Overlaps with our somatosensory cortex
Preprioceptive information: sensory information received from internal sensors in the body, such as that about the position of body parts relative to one another
Kinesthetic information: actual movement of body parts
Feedbacks to premotor and primary motor cortices to correct and adjunct movement
Largely left hemisphere
Bilateral control
Damage (or TMS) leads to:
Adjusting movement
Misguided actions (e.g. misreach)
Grasping problems
Impairment of generating a mental model of movement (e.g.pantomime, or imagining)
Apraxia
An inability to perform skilled, sequential, purposeful movement that cannot be accounted for by disruptions in more basic motor processes (e.g. muscle weakness)
Usually a result of brain damage or trauma (usually left)
Thought of as high order problem
Bilateral
Low level motor intact (e.g., grasping an object)
Ideational/Conceptual and Ideomotor
Controversy over whether these are two distinct disorders, and one is just more severe
Ways to categorize apraxia
Typically a result of damage to the parietal or frontal cortex
Can be a result of the connections between frontal and parietal and M1
But really can be any of our motor regions, cortical, subcortical which would determine the type of impairment
Spatial processing difficulties: RH parietal
Language, control of left hands: damage through corpus callosum
Visual feedback needed: requires different regions
Ideational Apraxia
Inability to form a mental image of intended movement
Issue with choosing correct action and the correct course of actions
Inappropriate use of objects
Impaired transitive gestures (object-related actions)
Ideomotor Apraxia
Disconnection between the idea of the movement and its execution
More pronounced for actions not initiated by interactions with external objects
More pronounced for more abstract than concrete actions
Pantomime impaired
Cerebellum in Action
Posture and stability
Timing associated with coordinating muscles
Planning of movements
Learning new skills
Sensory motor integration and feedback
Modulating effect on movement
Damage= degrading motor abilities
Ipsilateral control
Organized for trunk/posture vs. limbs
Damage means hard to coordinate movement, especially across multiple joints and with sensory feedback (ex./ dysarthia and cerebellar ataxia)
Learning
Prism glasses
Recalibration impaired
Sensorimotor learning
Forward model
Predict sensory consequences of motor actions, but does compute an error signal for future performance
Timing device that provides a clock for events
Timing of initiation and cessation of aspects of the movement
Timing of discrete events (not continuous movements)
Affects temporal perception across domains (not just motor)
Basal Ganglia in Action
Also called Striatum
Collection of nuclei
Basal ganglia loops= multiple pathways of basal ganglia involvement
Highly connected to the frontal cortex
Highly organized within different areas of BG
Highly concentrated of the cells bodies generating the neurotransmitter dopamine
“Setting” the motor system with regard to posture
Motor planning
Important for initiating or stopping voluntary movements
Controlling the timing of and switching between motor acts
Skill learning
Acting as an autopilot for well-learned sequential movements
Implicit learning
Motivated movement with respect to reward
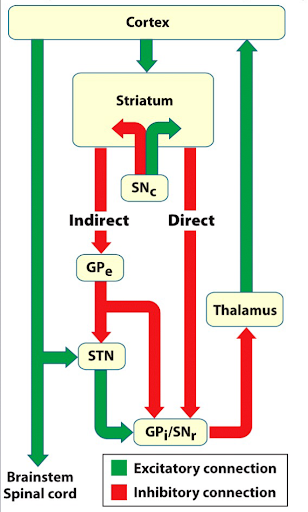
SNc site of dopamine
Intricate excitation and inhibition
Overall output is to inhibit movement
Direct (fast) pathway- promote movement (less inhibition on thalamus)
Indirect (slow) pathway- inhibit movement (more inhibition on thalamus)
“Gatekeeper”
Initiation of actions
Strong inhibitory baseline keeps system in check
Allows cortical representation of movement to become activated without triggering movement
As a motor plan gains strength, the inhibitory signal is deceased
Parkinson’s Disease
Lack of dopamine
Hypokinetic: absence of voluntary movement
Posture
Later stages develop delusions, paranoia, and memory issues
Lack of inhibition through the direct pathway
Lack of excitation to motor cortex