5. Angle Closure Glaucoma - Management of Glaucoma Summer 2026
1/175
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
176 Terms
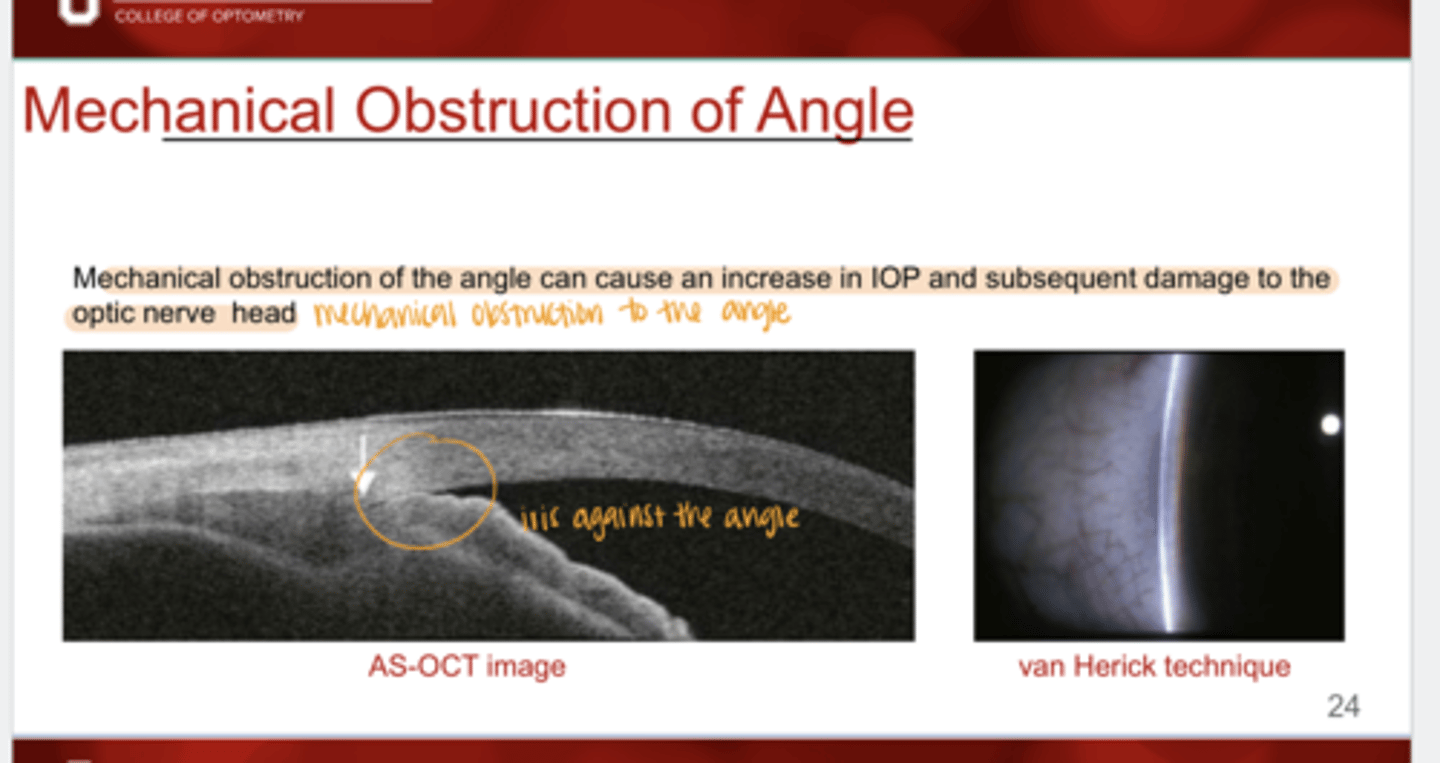
What can mechanical obstruction of the angle cause?
an increase in IOP and subsequent damage to the ONH
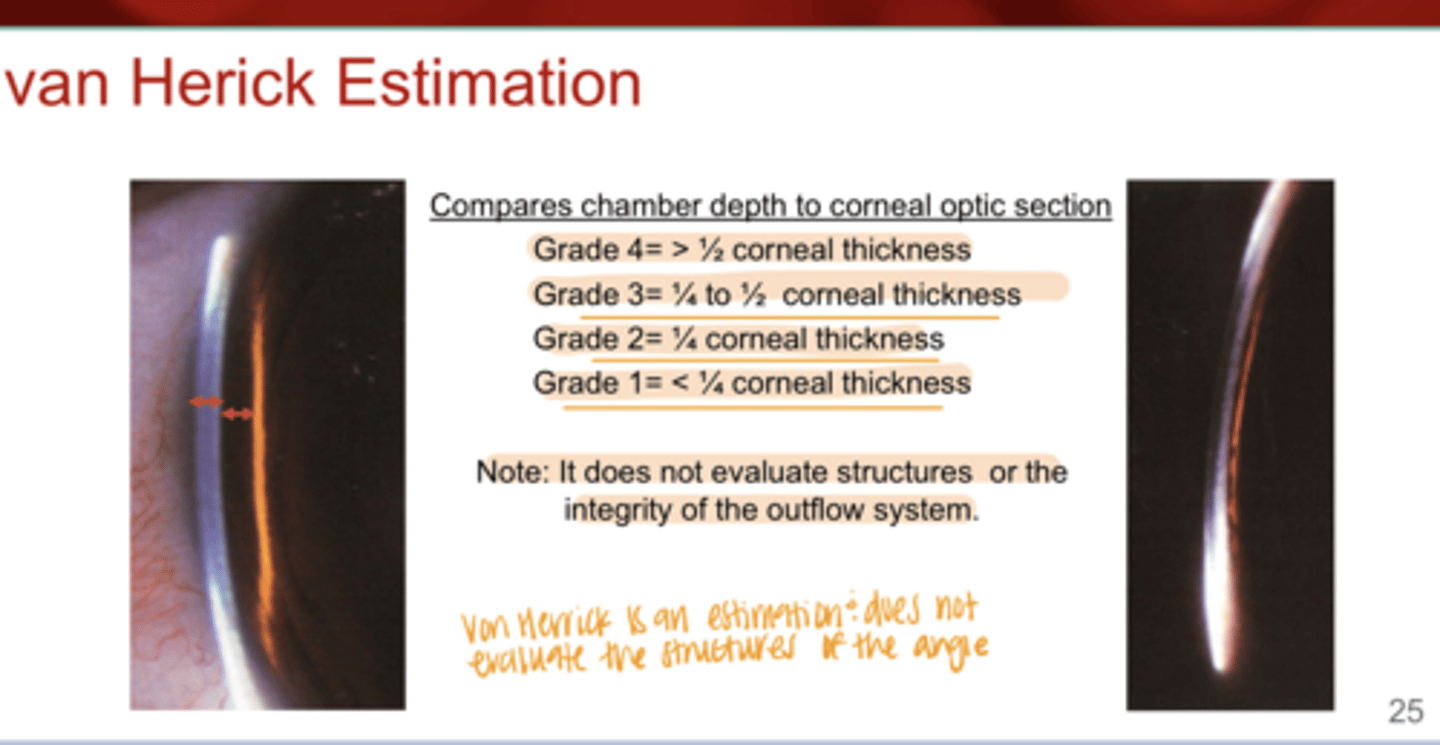
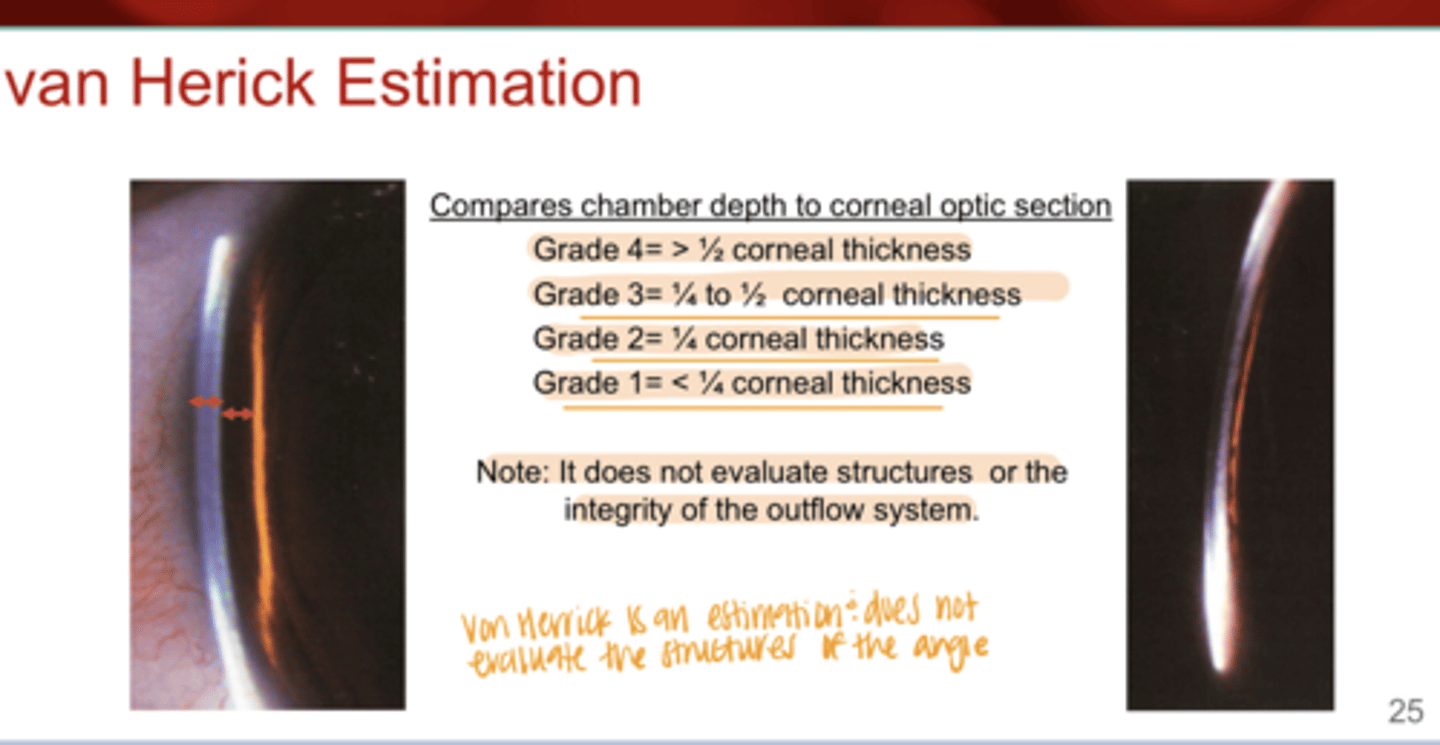
What is the function of van Herick angle estimation?
compares chamber depth to the corneal optic section
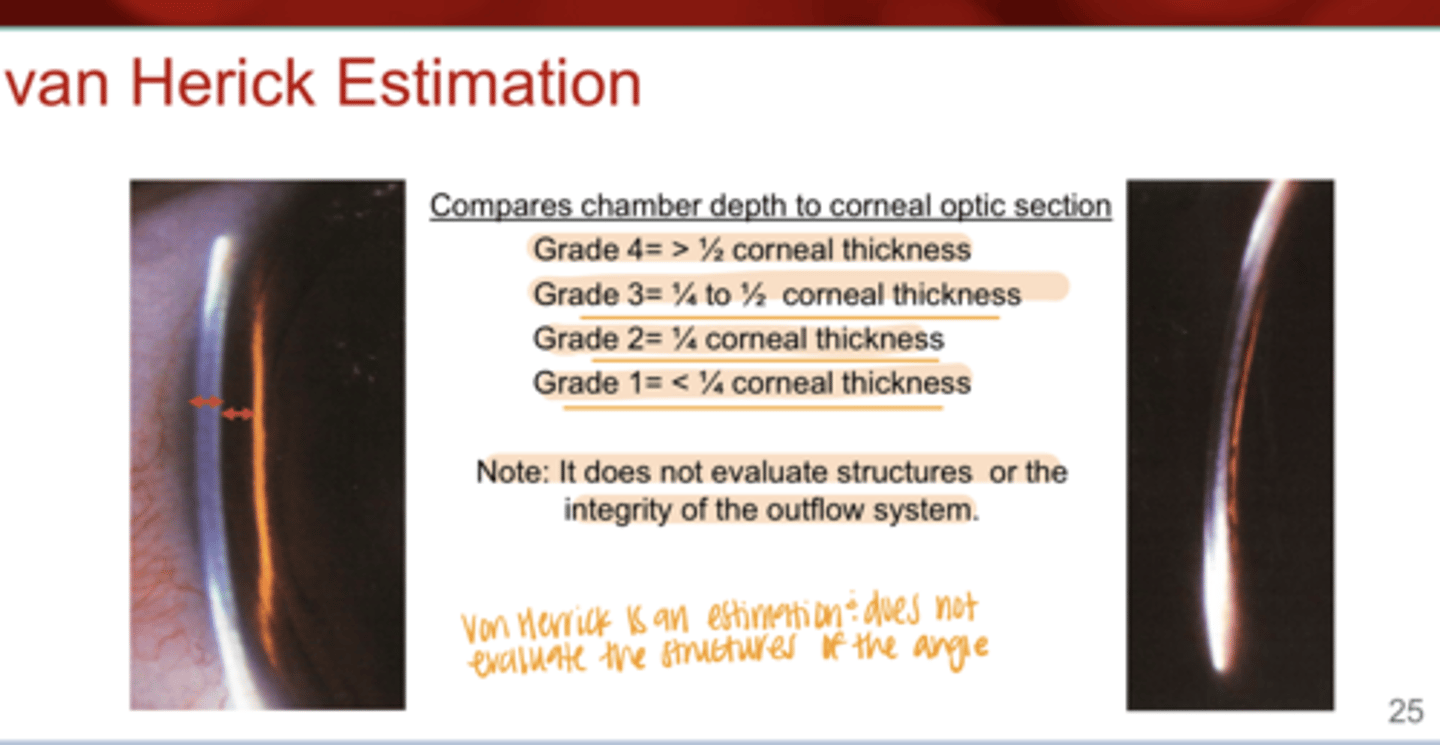
What is a "Grade 4" van Herick angle?
>1/2 the corneal thickness
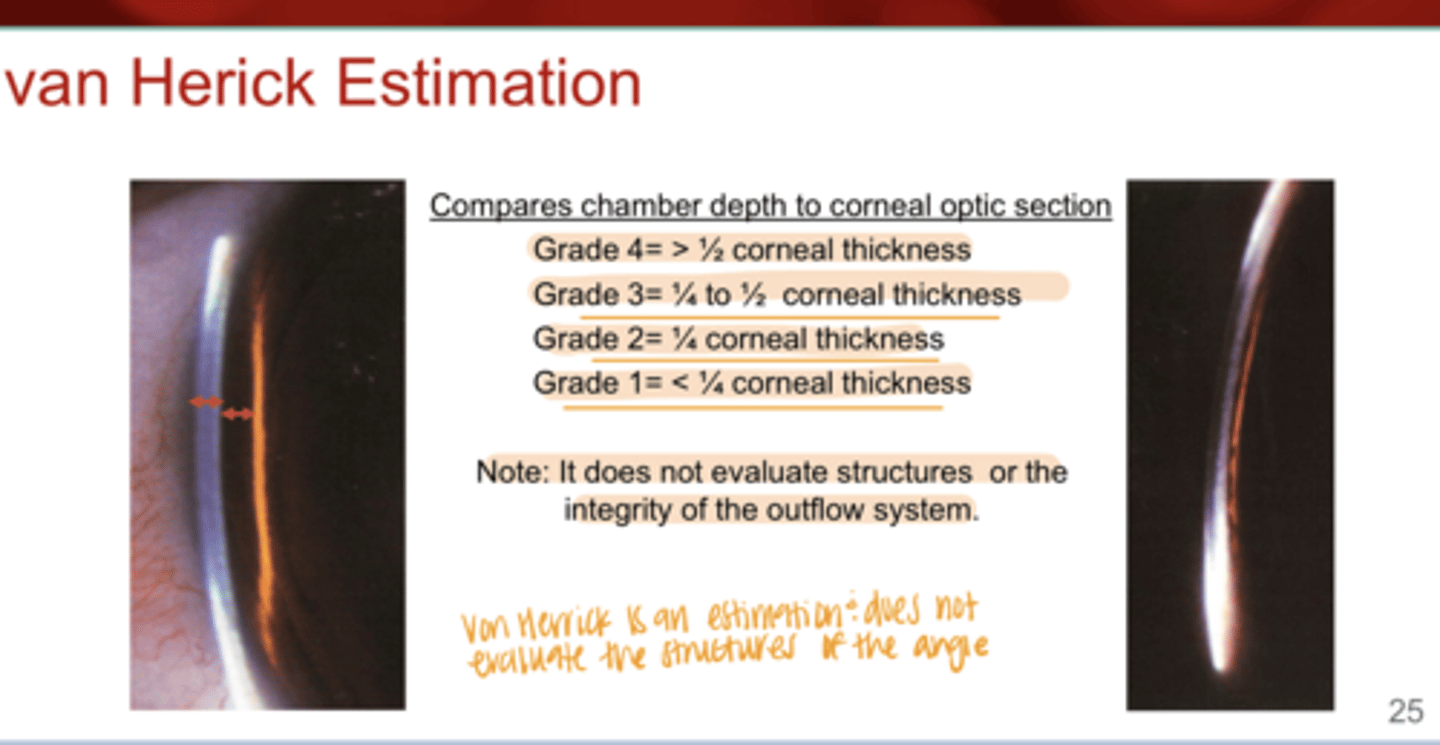
What is a "Grade 3" van Herick angle?
1/4 to 1/2 corneal thickness
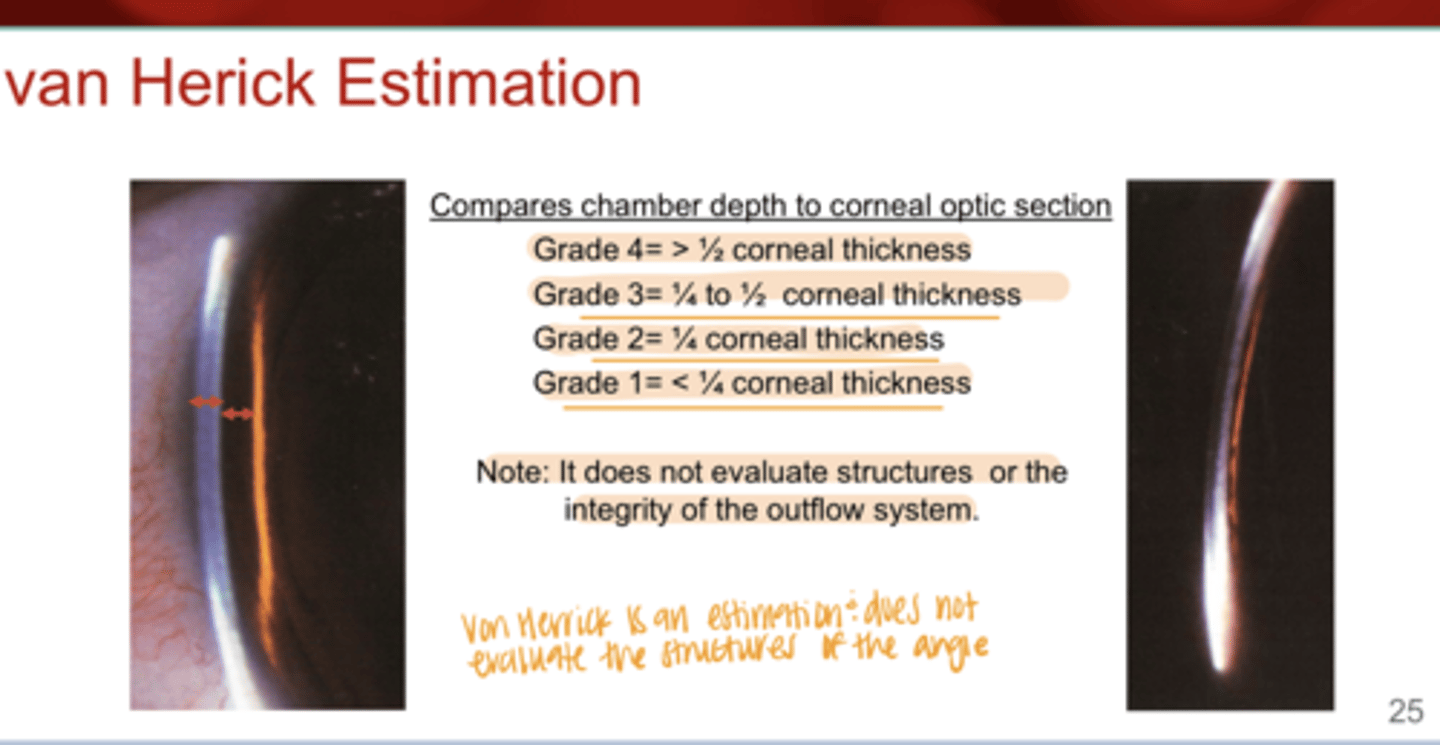
What is a "Grade 2" van Herick angle?
1/4 corneal thickness
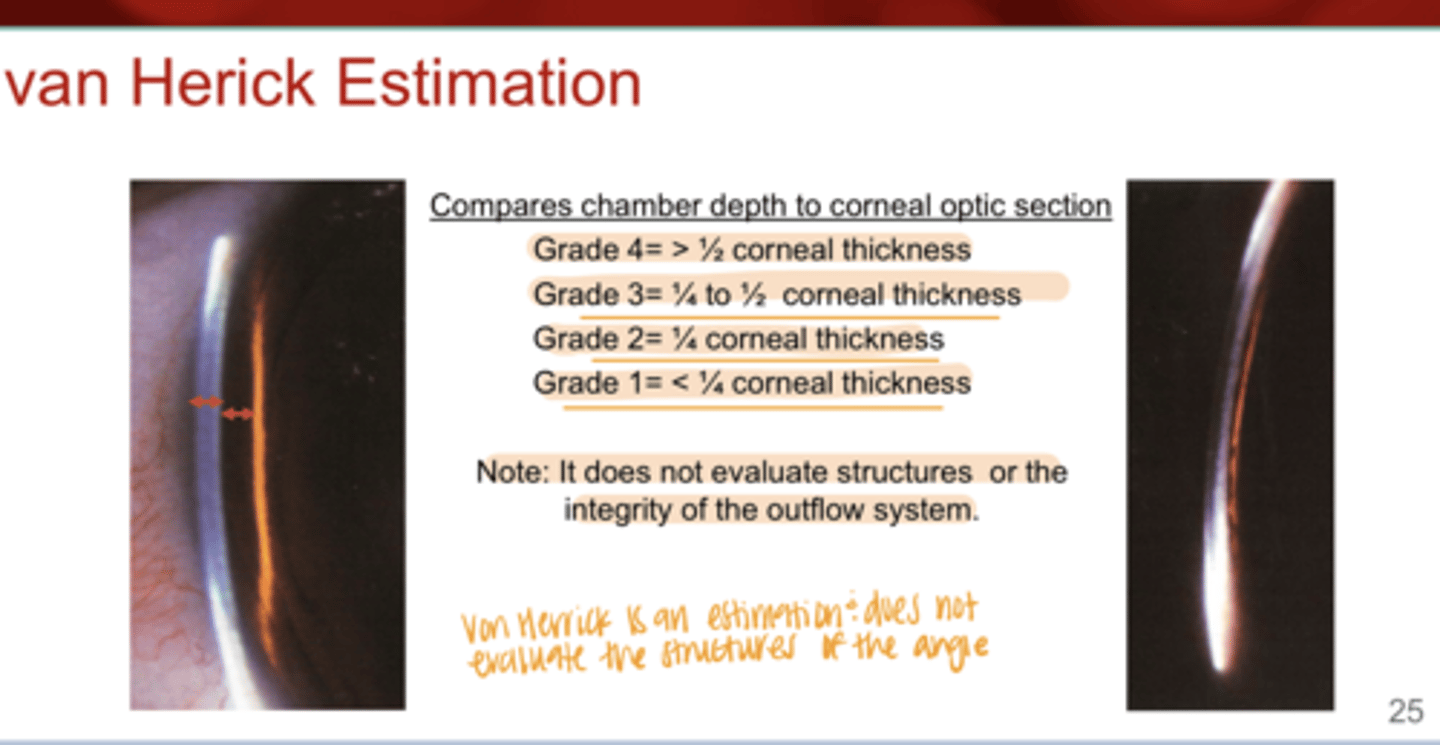
What is a "Grade 1" van Herick angle?
<1/4 corneal thickness
True or False:
van Herick angle estimation evaluates angle structures & integrity of the outflow system
False -- it does not do this
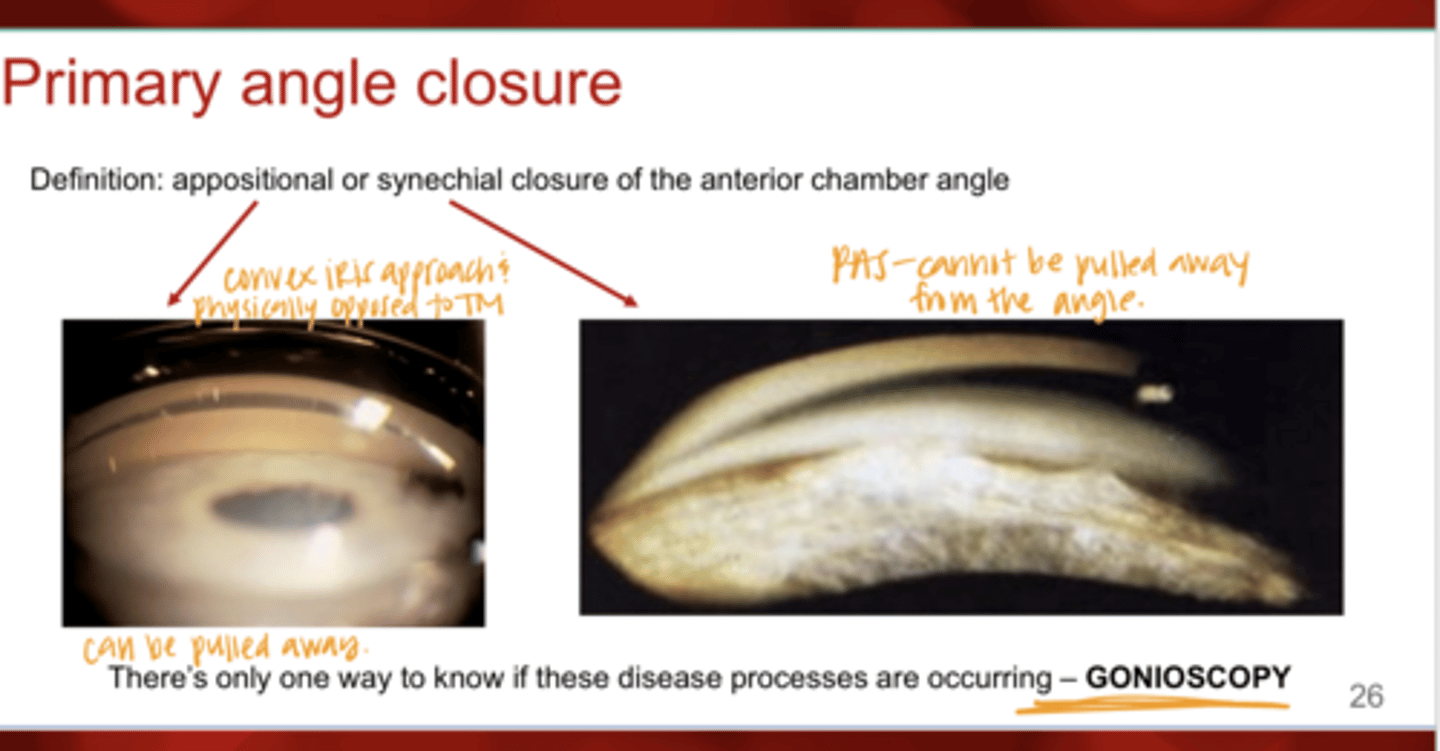
What is primary angle closure?
appositional or synechial closure of the anterior chamber angle
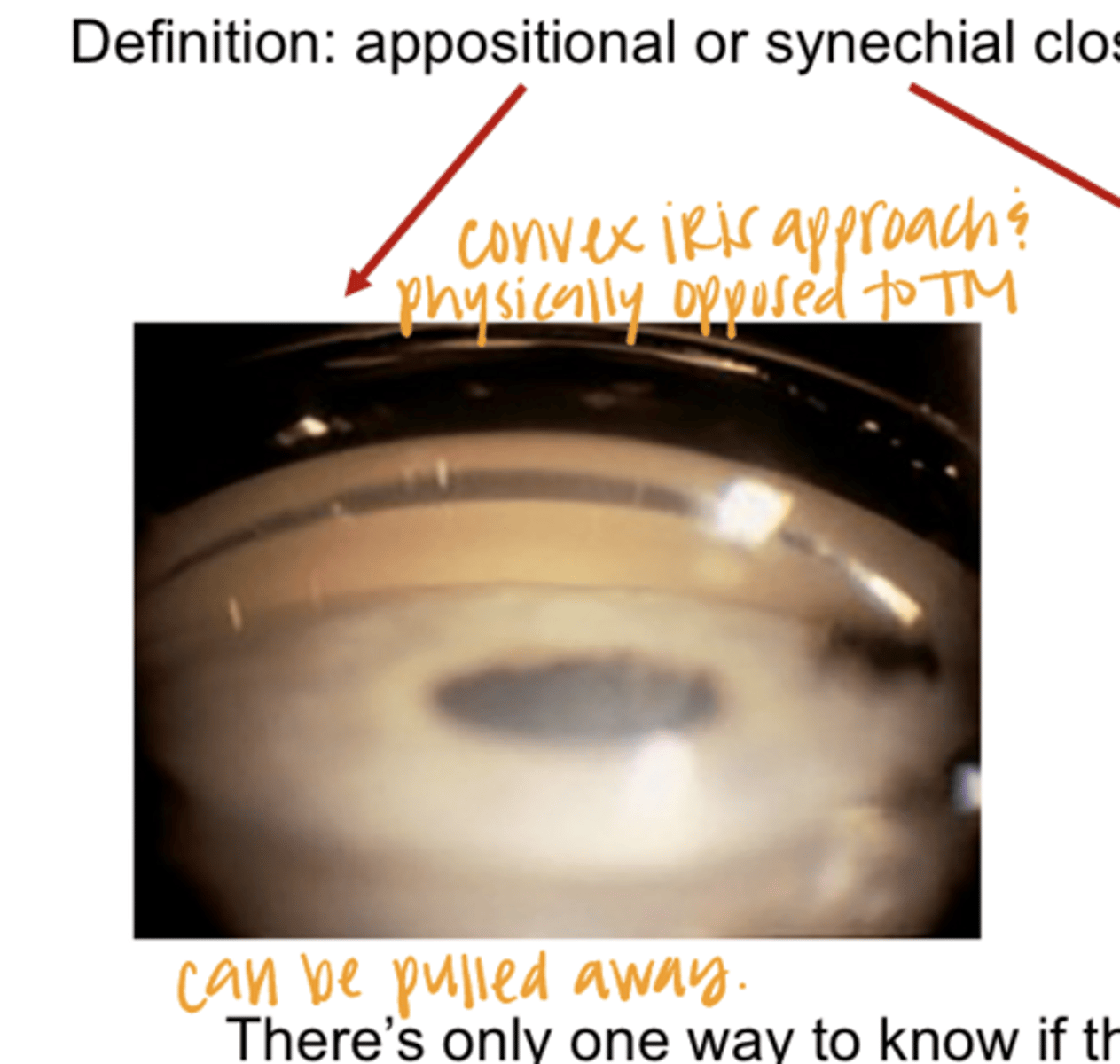
Convex Iris Approach -- Iris Opposed to the TM (Pic)
Convex Iris Approach -- Iris Opposed to the TM (Pic)
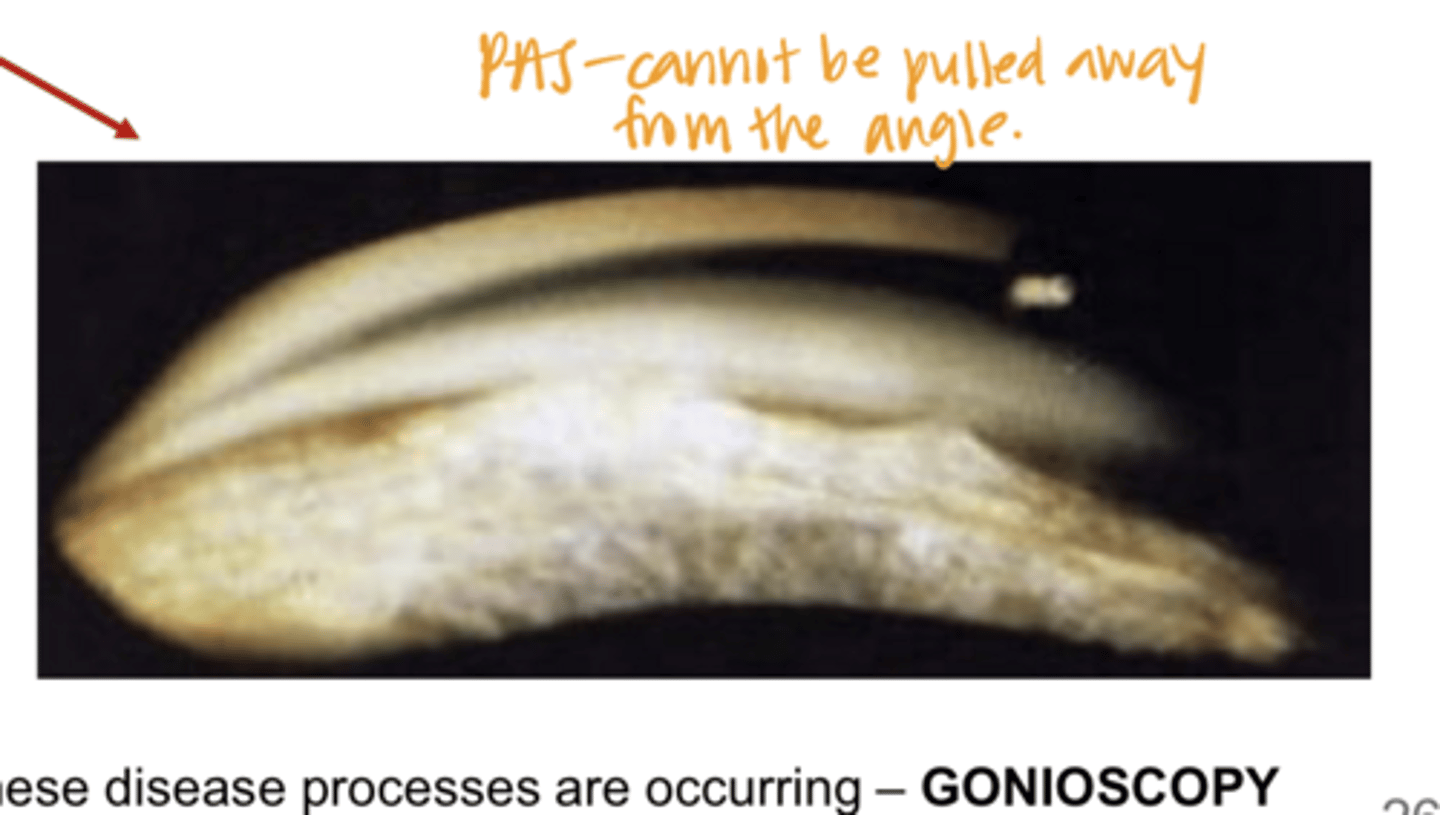
Peripheral Anterior Synechiae -- Cannot be Pulled Away from the Angle (Pic)
Peripheral Anterior Synechiae -- Cannot be Pulled Away from the Angle (Pic)
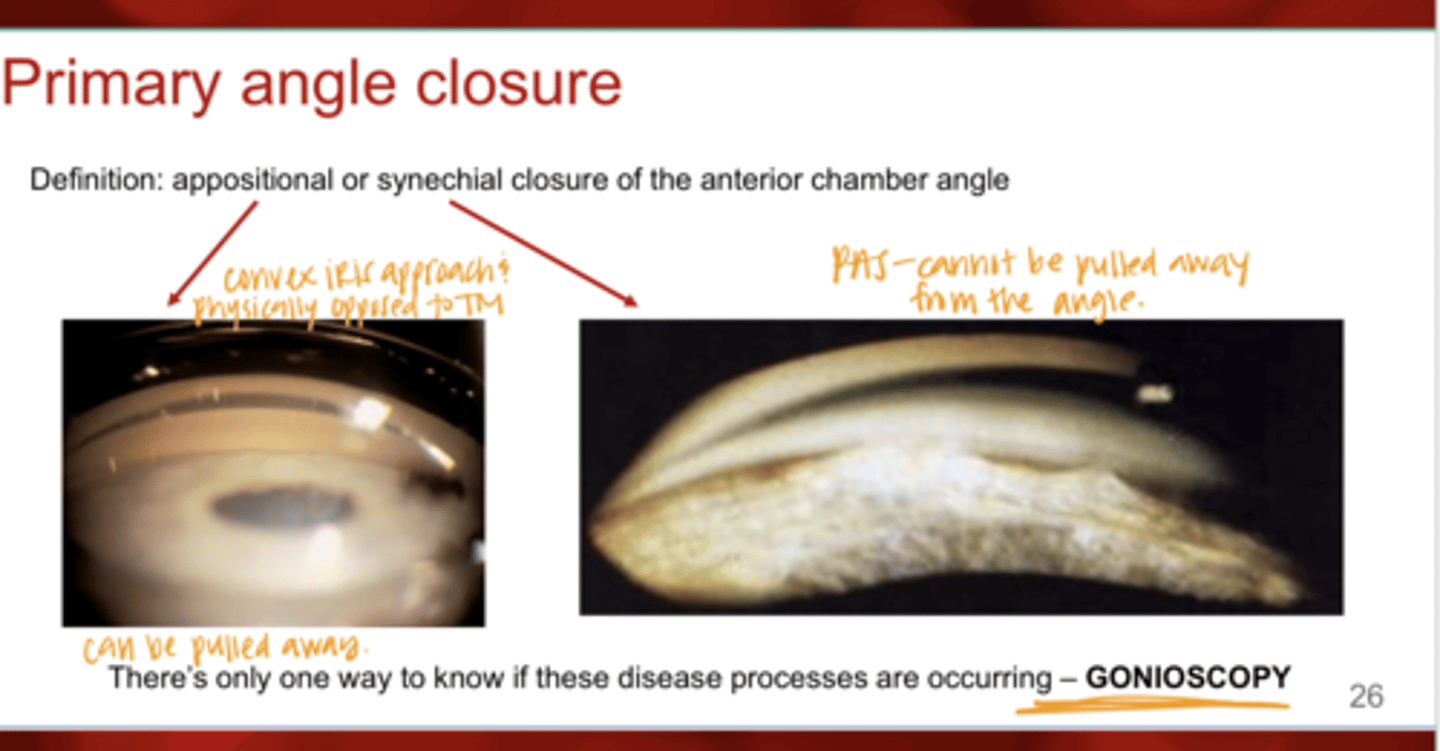
There is only one way to know if primary angle closure or PAS is occurring, what is this?
gonioscopy
Why should you perform gonioscopy?
-Determine the extent of the drainage structures that are open
-Determine the configuration of the angle and iris approach
-Determine the degree of pigment, which can help to categorize the disease process
-Differentiate Open Angle, Closed Angle, and Plateau Iris
What are the forms of secondary glaucoma that can be observed with gonioscopy?
-pigmentary glaucoma (PDS)
-uveitic glaucoma
-neovasc glaucoma
-pseudoexfoliation glaucoma (PXE)
-traumatic glaucoma
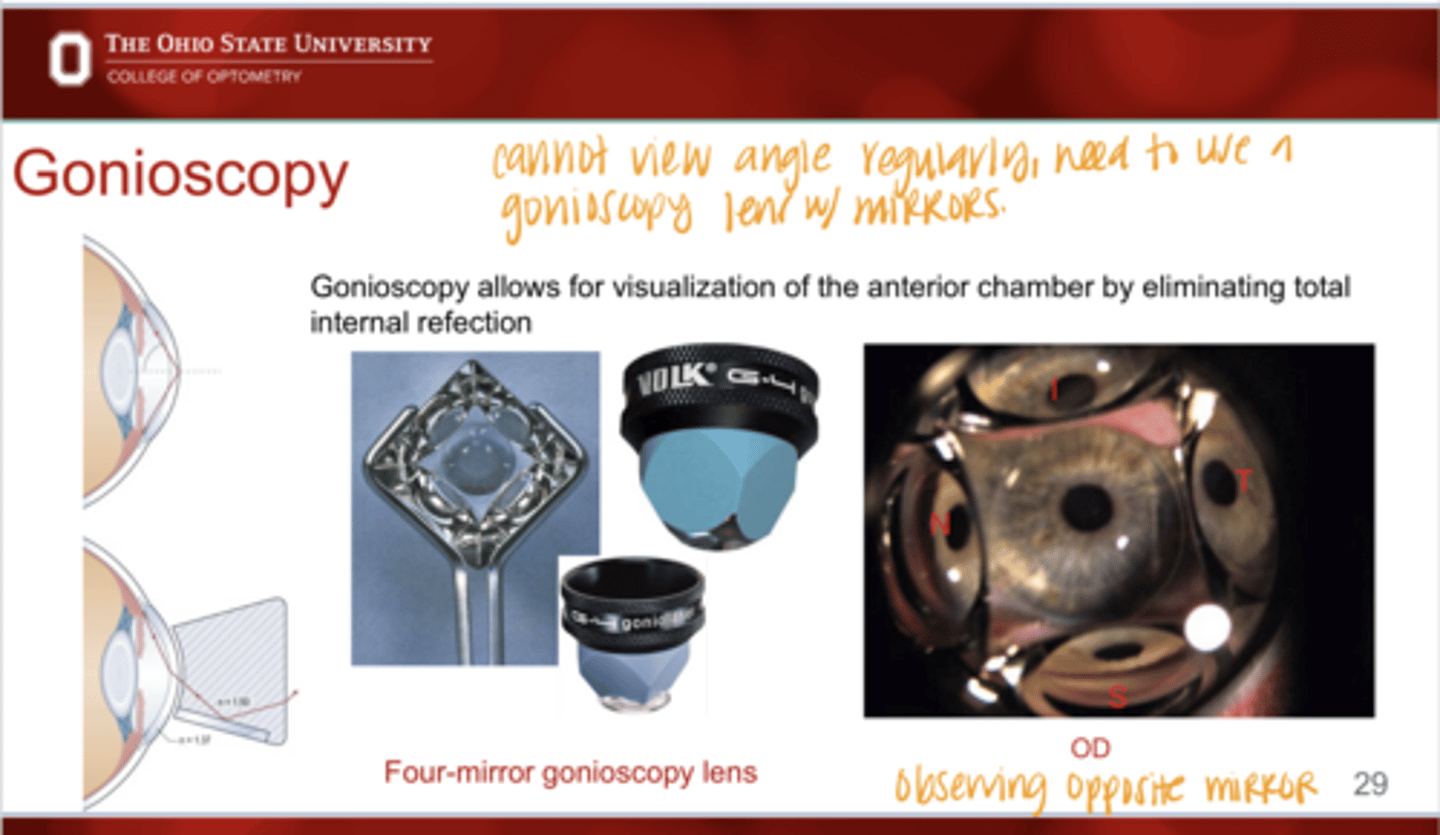
What does gonioscopy allow for?
visualization of the anterior chamber by eliminating total internal reflection
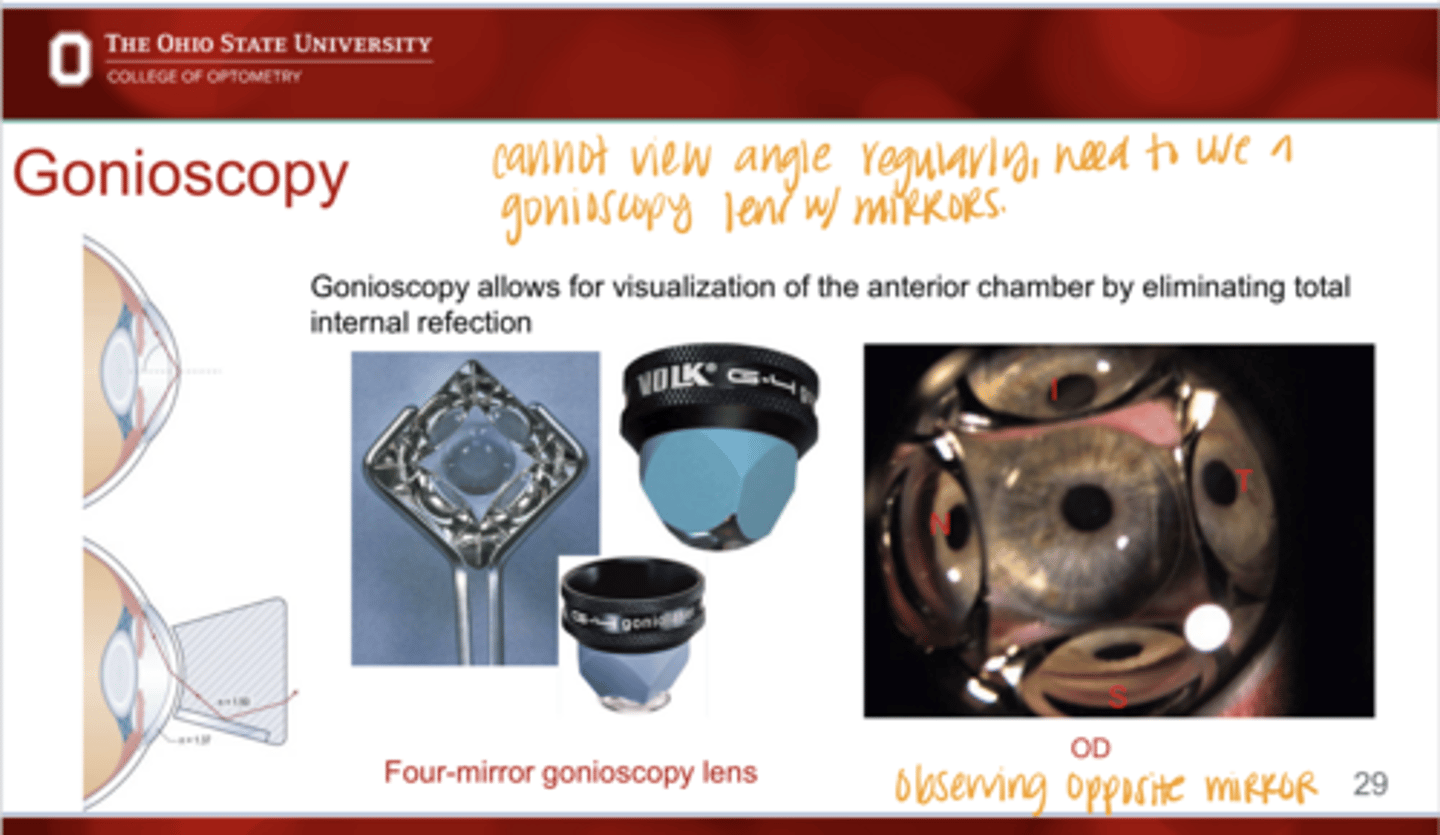
Four Mirror Gonioscopy View (Pic)
Four Mirror Gonioscopy View (Pic)
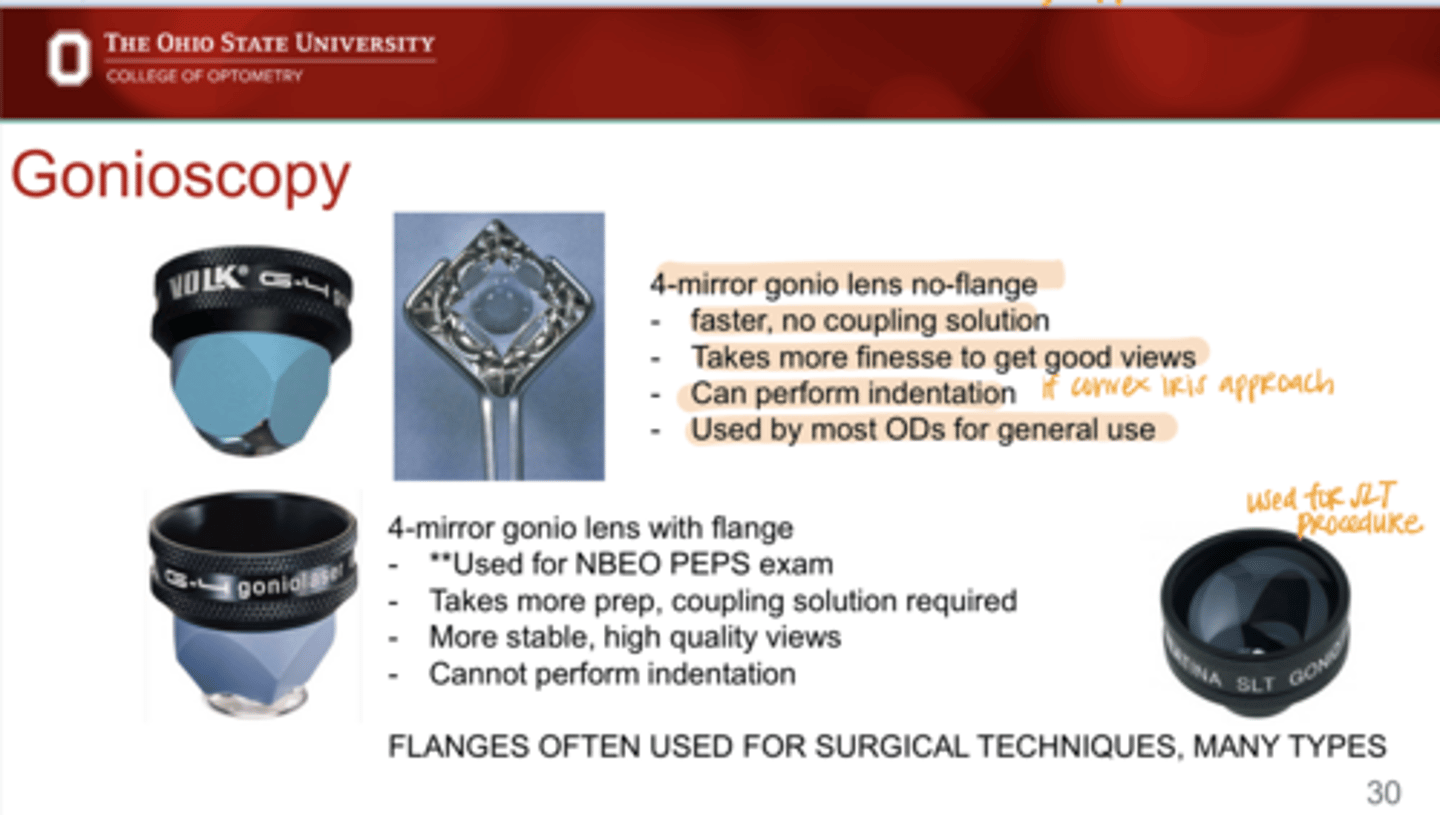
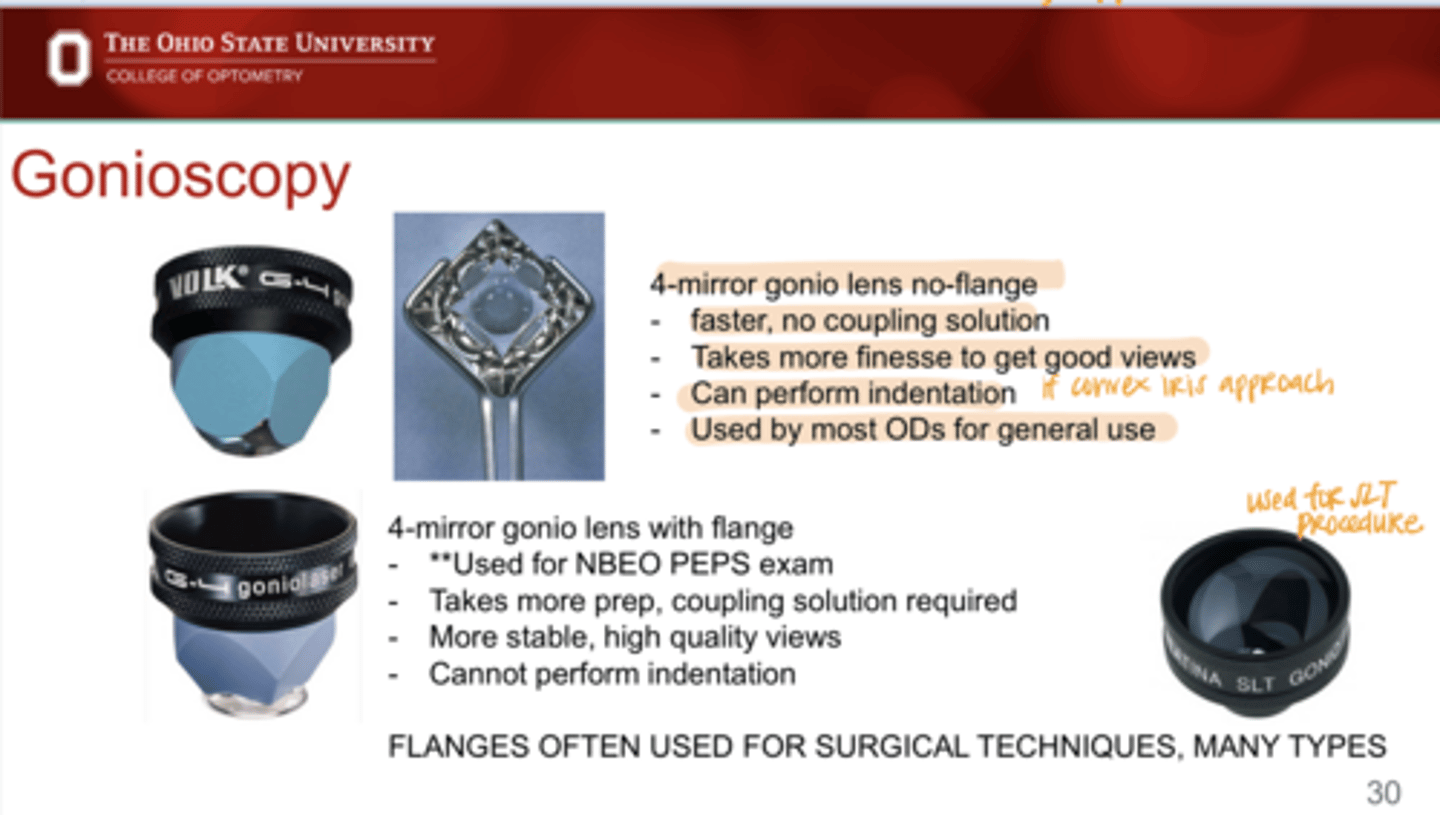
What are the benefits of 4 mirror gonio lens w/ no flange?
-faster
-no coupling solution needed
-can perform indentation gonioscopy
-used by most ODs for general use
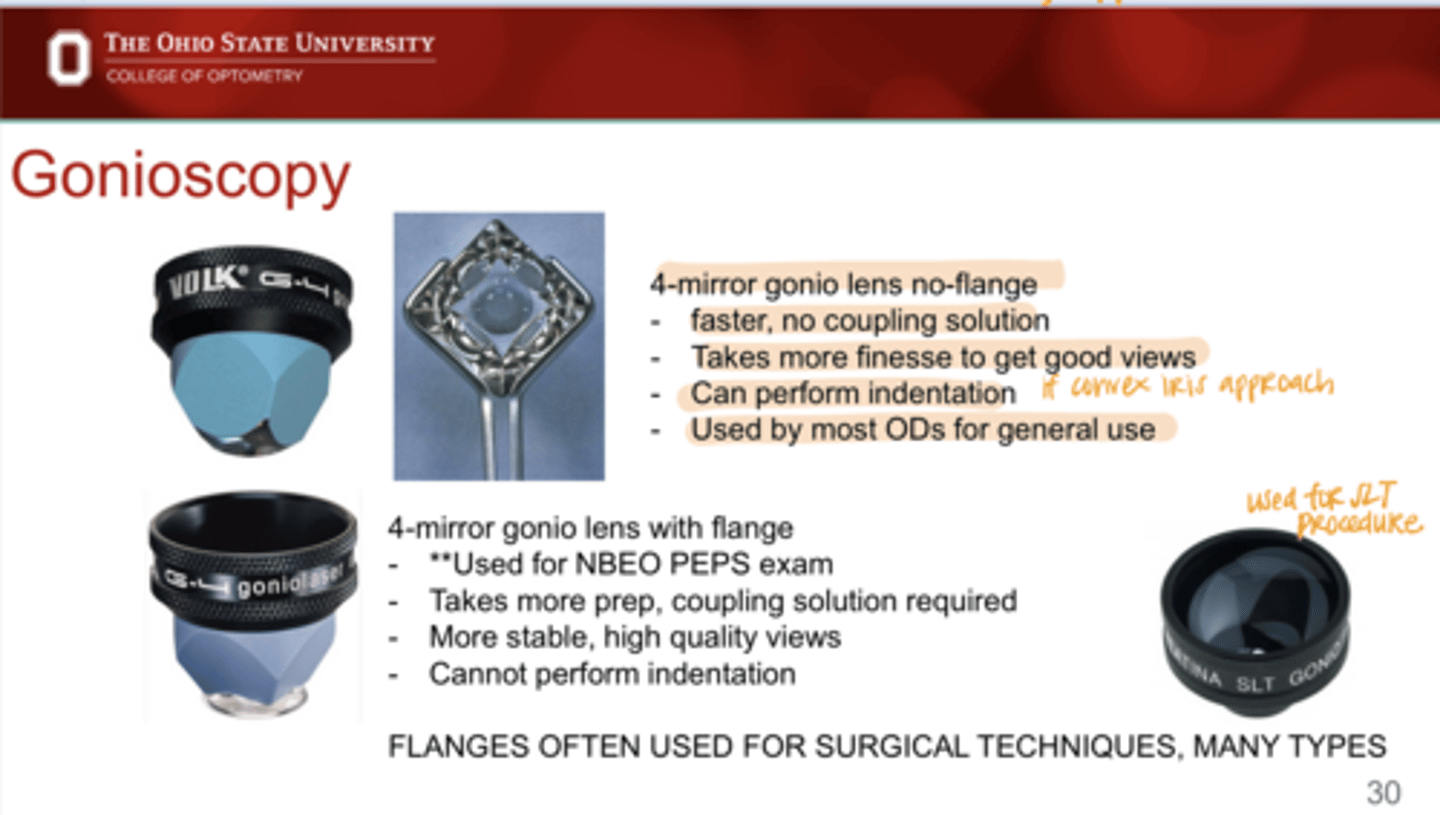
What are the disadvantages of 4 mirror gonio lens w/ no flange?
takes more finesse to get good views
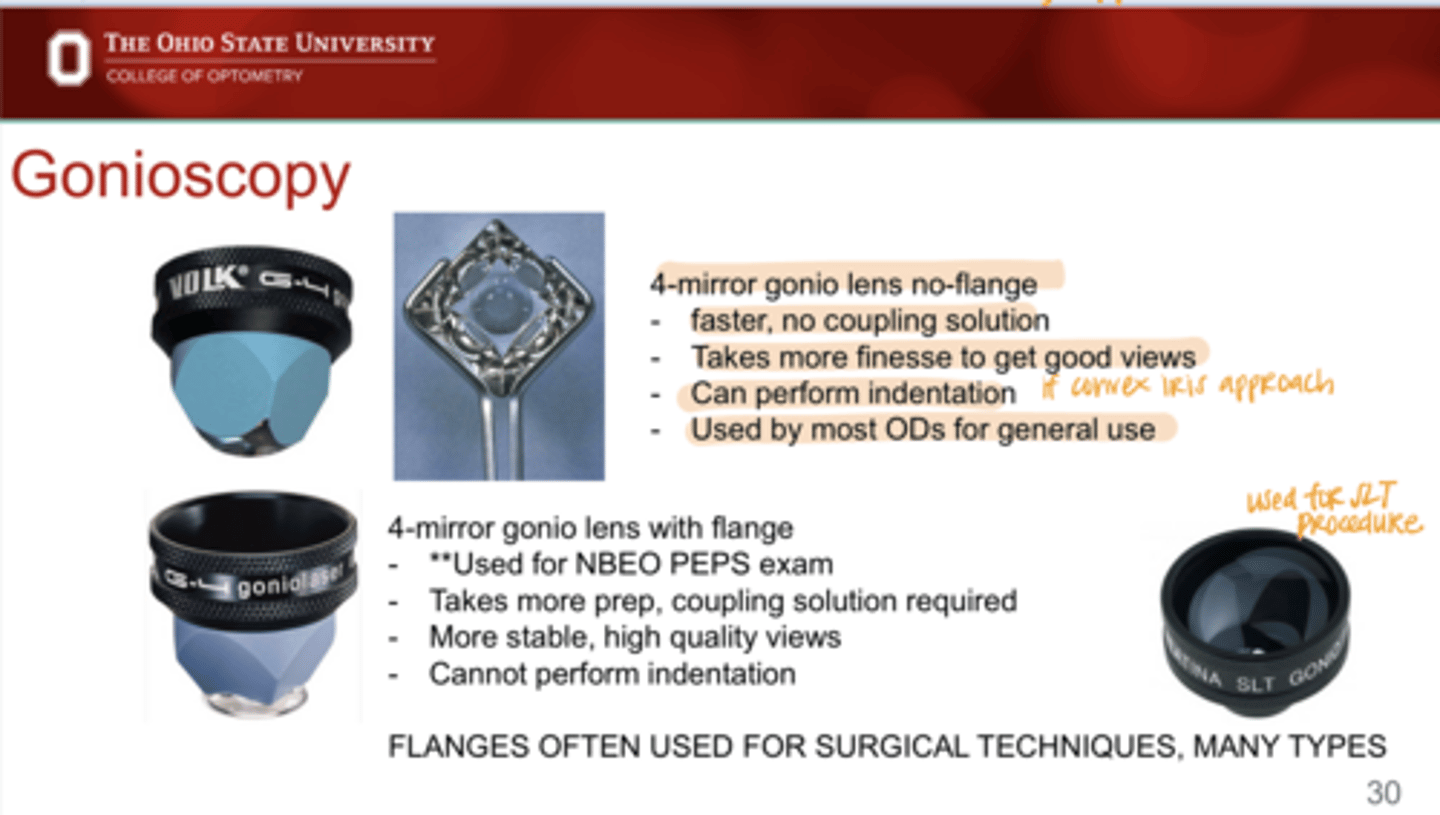
What are the benefits of 4 mirror gonio lens w/ flange?
-more stable
-more high quality views
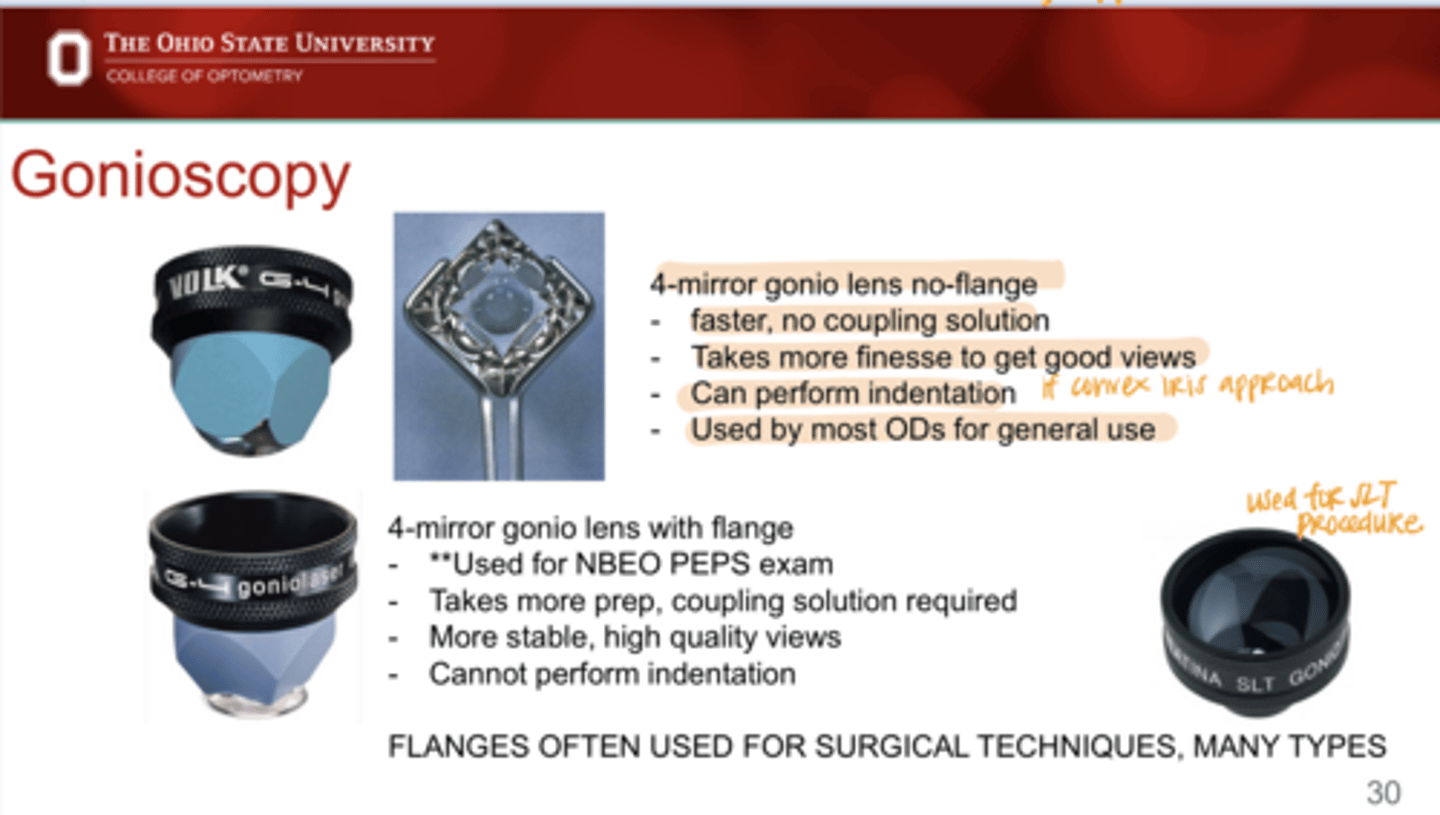
What are the disadvantages of 4 mirror gonio lens w/ flange?
-takes more prep
-coupling solution required
-cannot perform indentation
_____ can often used for surgical techniques
Flanges
During gonioscopy, you should be mindful of _______
-illumination of the room
-illumination of the slit lamp beam
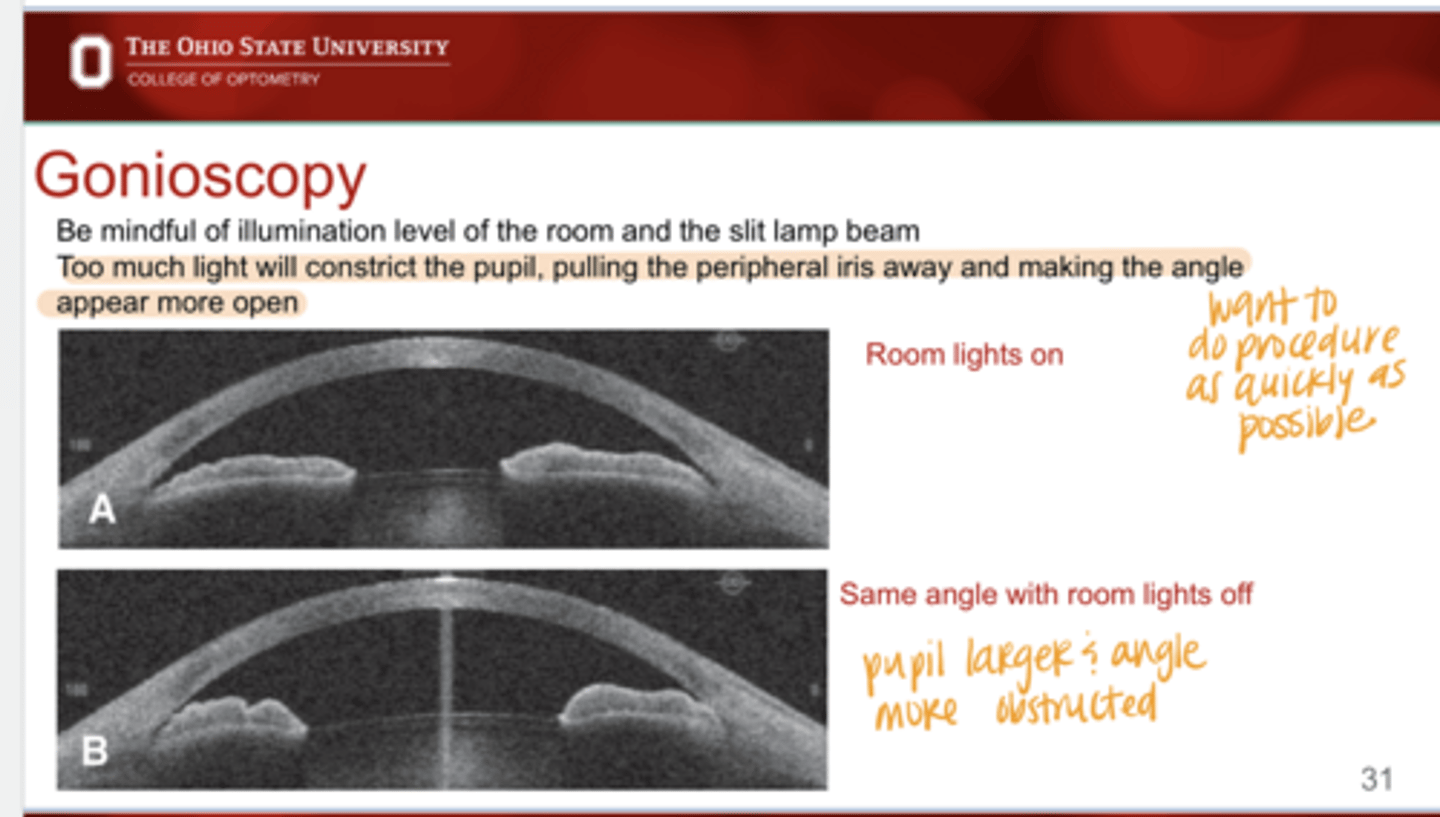
Why should you be mindful of illumination of the room and slit lamp beam when doing gonioscopy?
With too much light, the pupil will constrict. This may pull the peripheral iris AWAY from the angle structures and make it appear more open that it is.
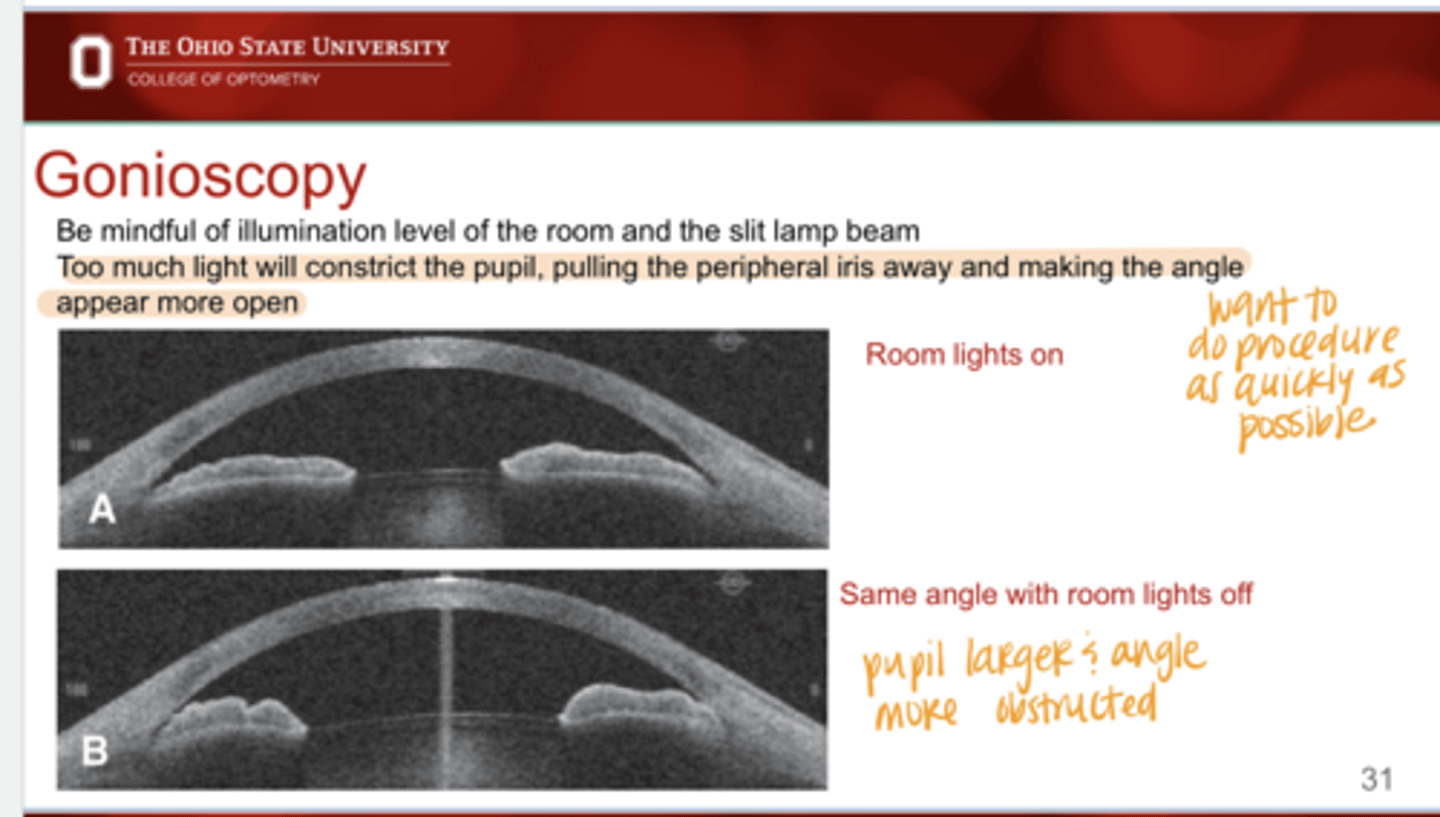
Iris Configuration with Room Lights On and Off (Pic)
Iris Configuration with Room Lights On and Off (Pic)
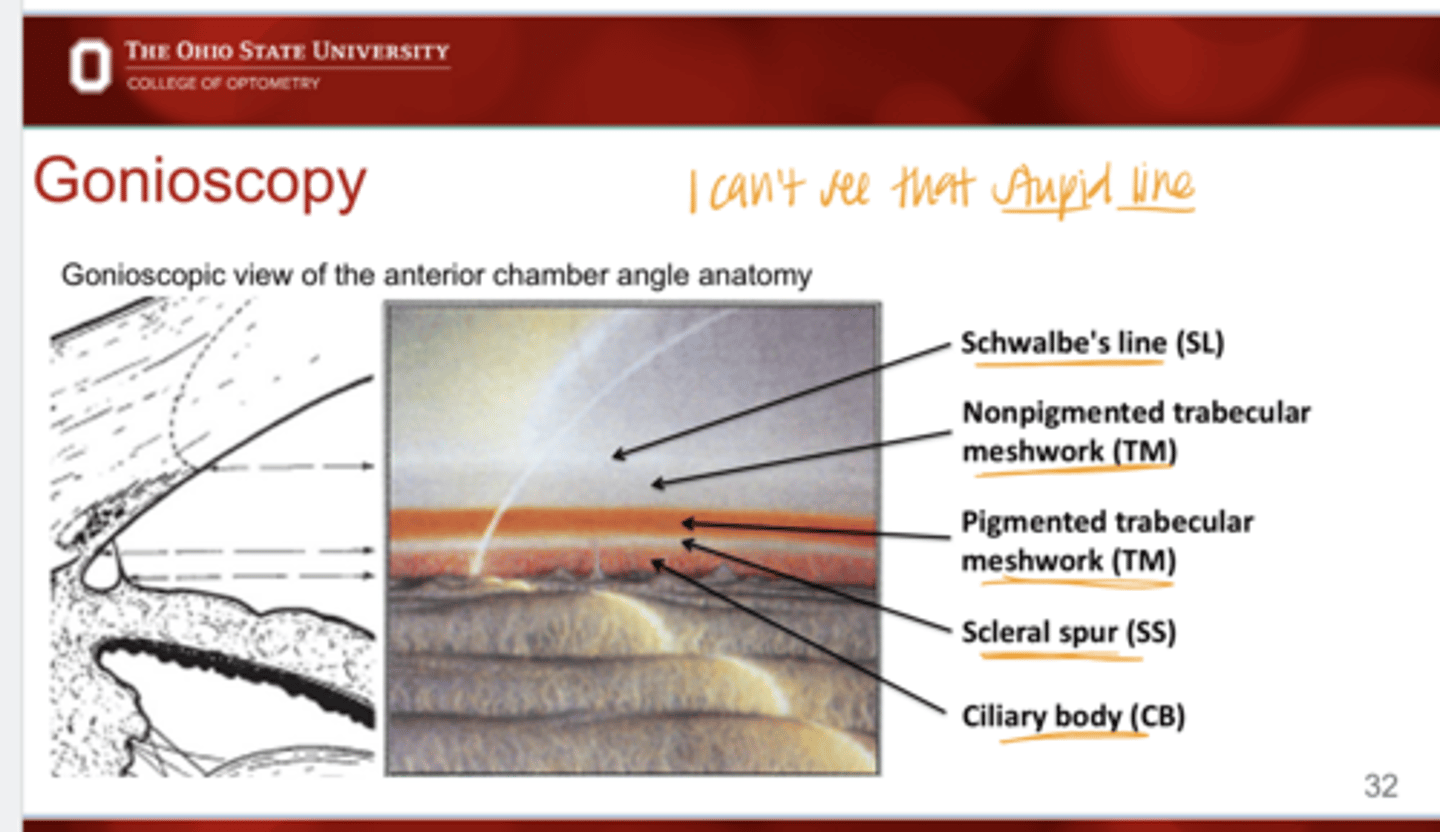
Gonioscopic view of the Anterior Chamber Anatomy
-Ciliary body
-Scleral spur
-TM Pigmented and Nonpigmented
-Schwalbe Line
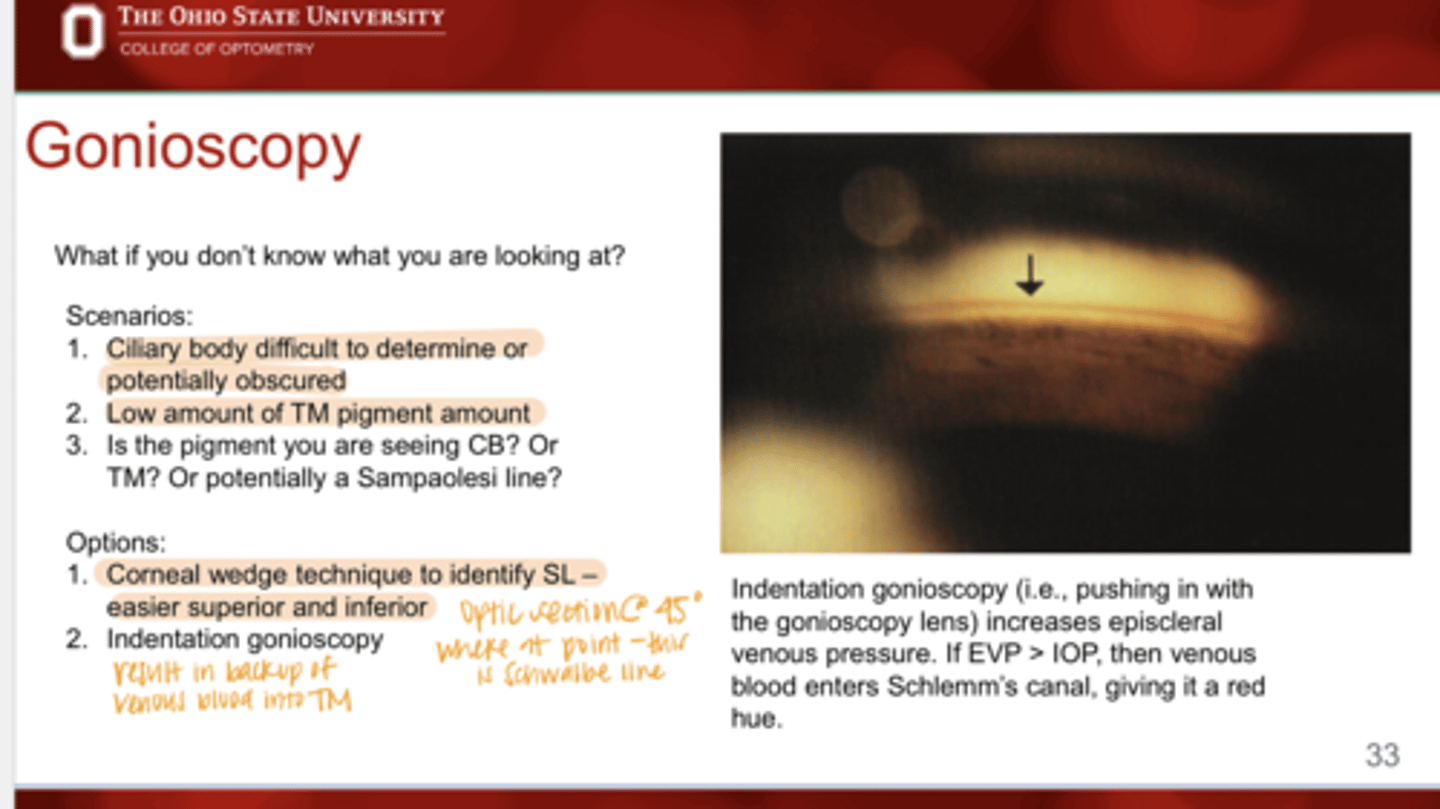
If you DO NOT know what you are looking at on gonioscopy, what options do you have?
1) Corneal wedge technique to identify Schwalbe's Line in superior and inferior views. Optic section will be at 45º.
2) Indentation gonioscopy
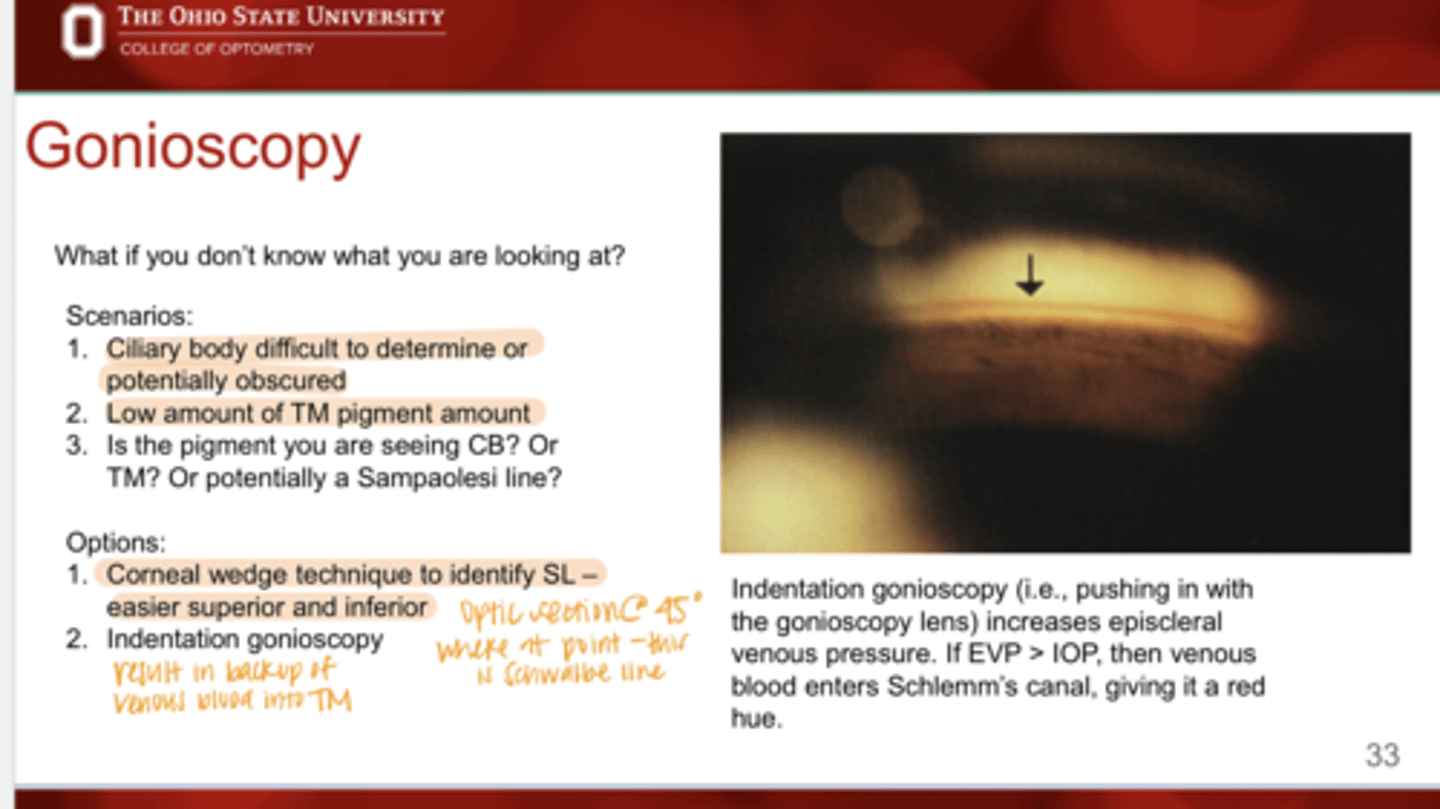
How to perform Indentation gonioscopy?
Pushing in with the gonioscopy lens to increase episcleral venous pressure. If EVP > IOP, then venous blood enters Schlemms canal and gives it a red hue.
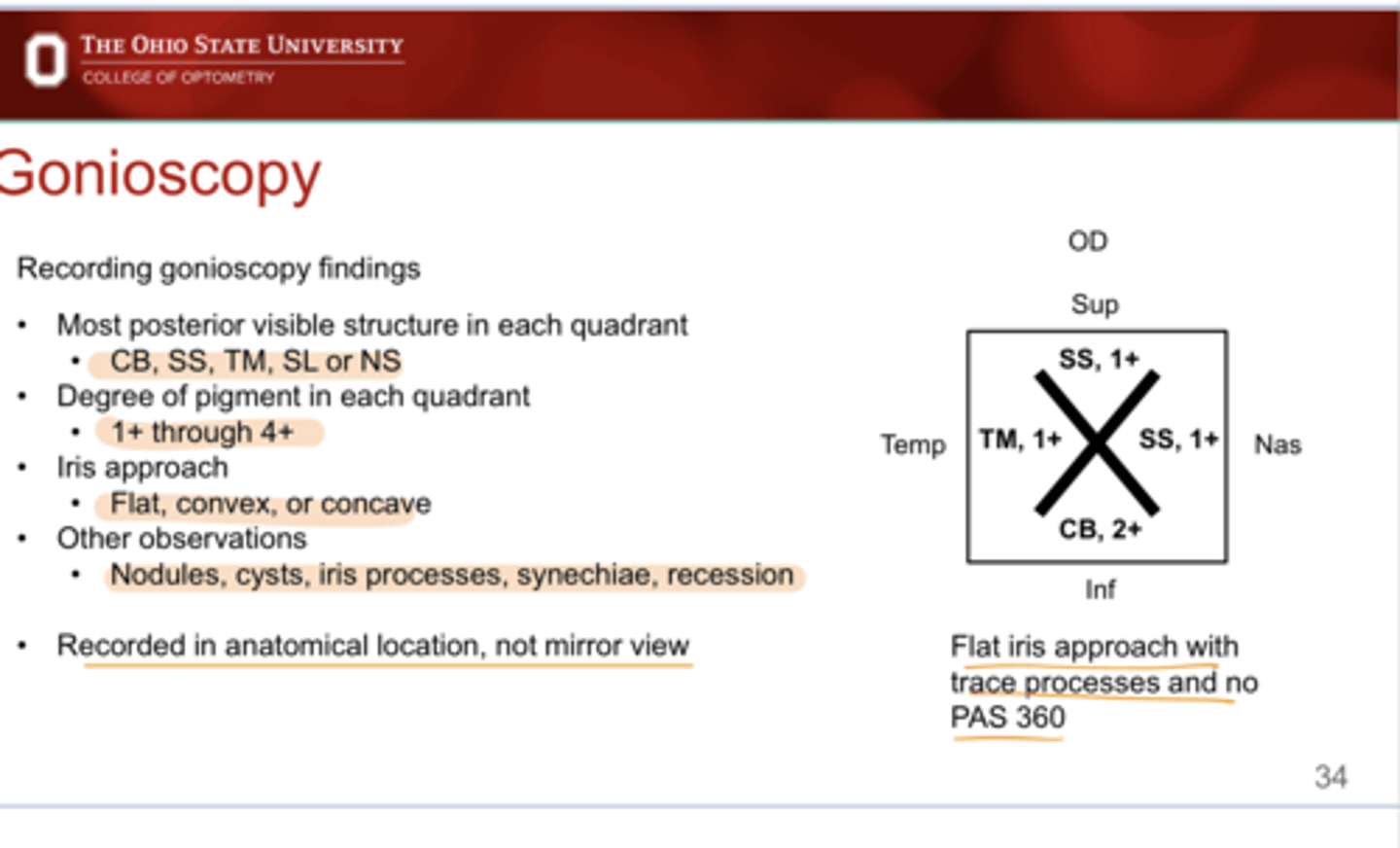
How to record gonioscopy findings?
-Most posterior structure in each quadrant
-Degree of pigment in each quadrant
-Iris approach
-Notable observations
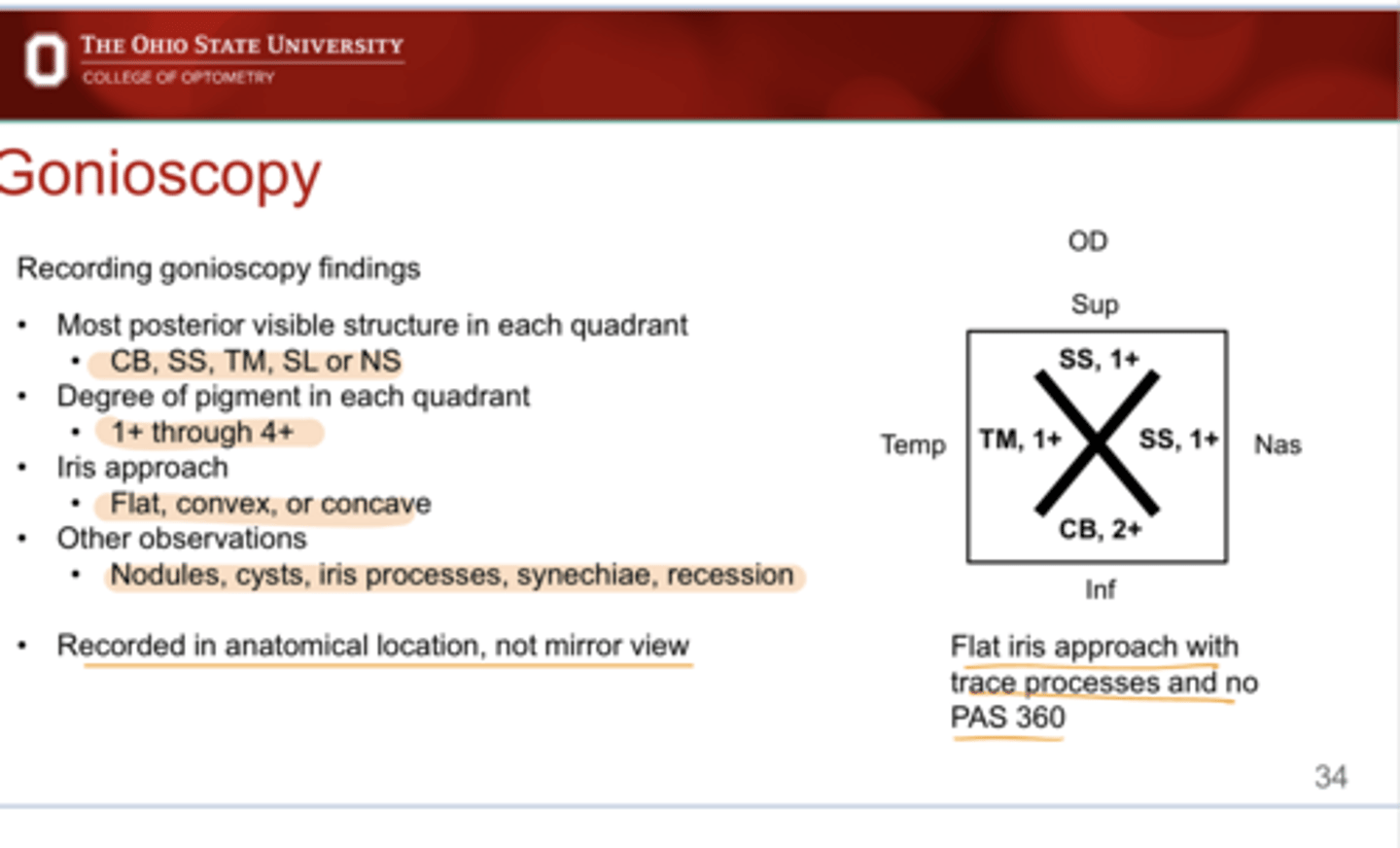
Recorded Gonioscopy Findings -- Flat Iris Approach with Trace Processes and No PAS 360 (Pic)
Recorded Gonioscopy Findings -- Flat Iris Approach with Trace Processes and No PAS 360 (Pic)
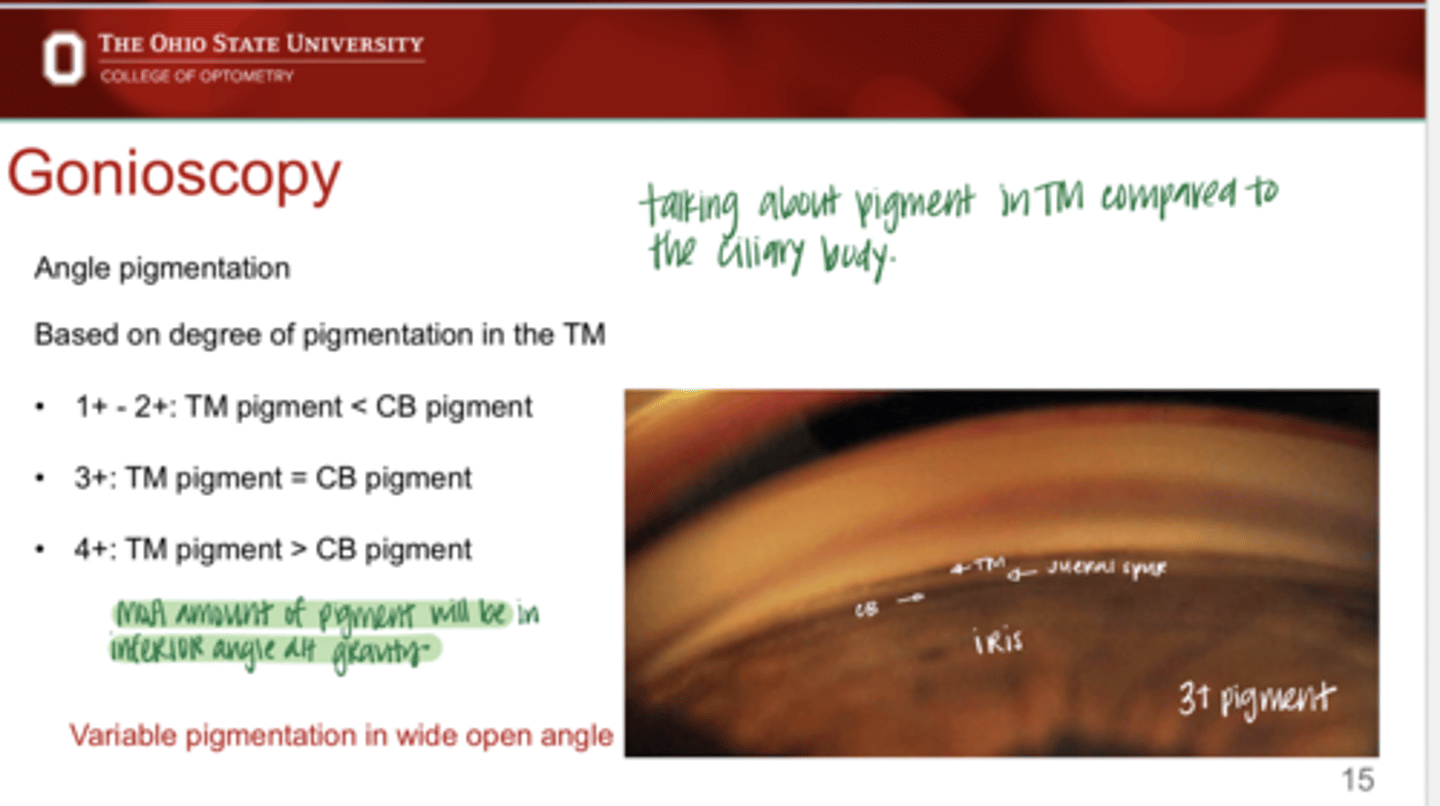
Angle pigmentation grading is based on pigmentation in the ______
TM
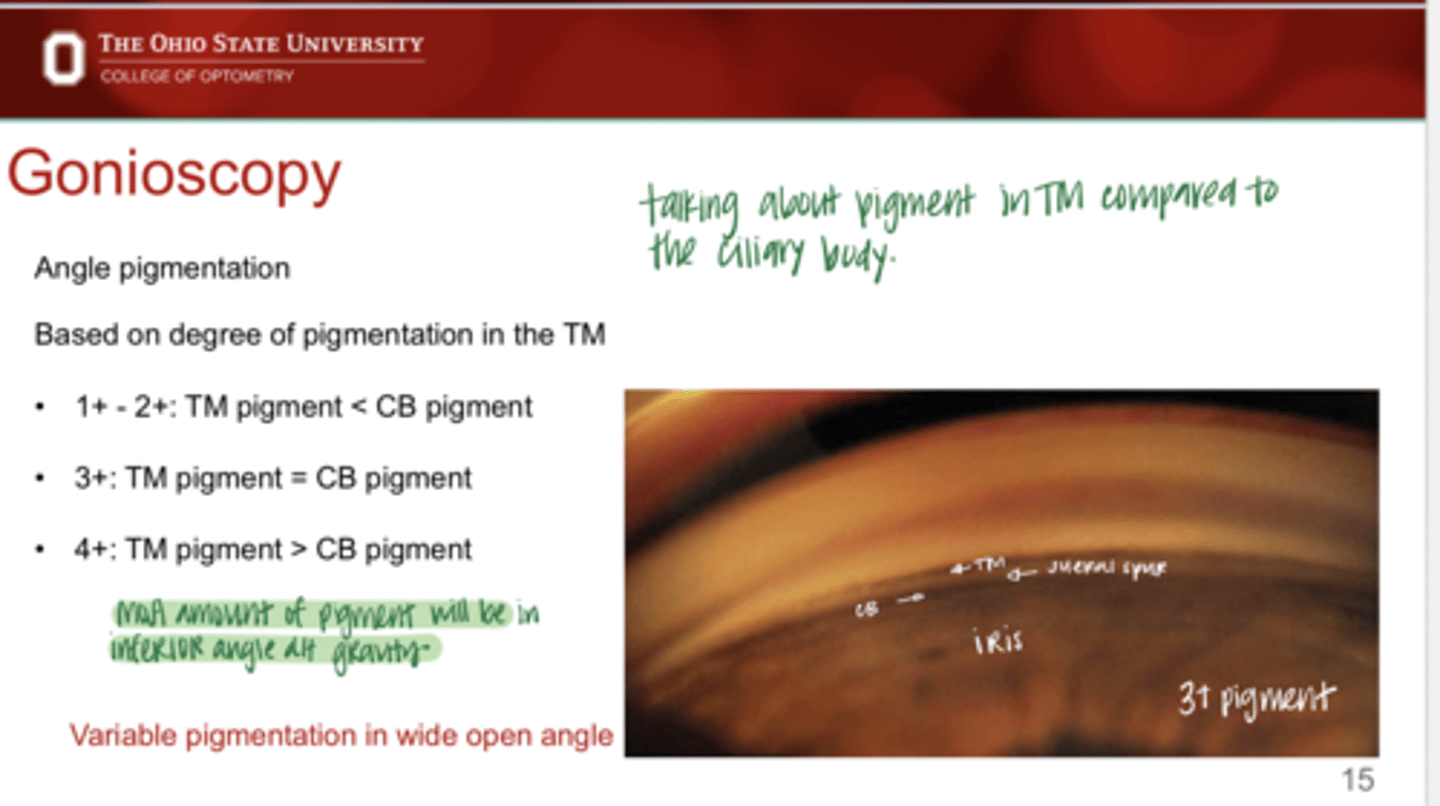
Grading Pigmentation in the Angle
TM pigment < CB pigment
1+ or 2+
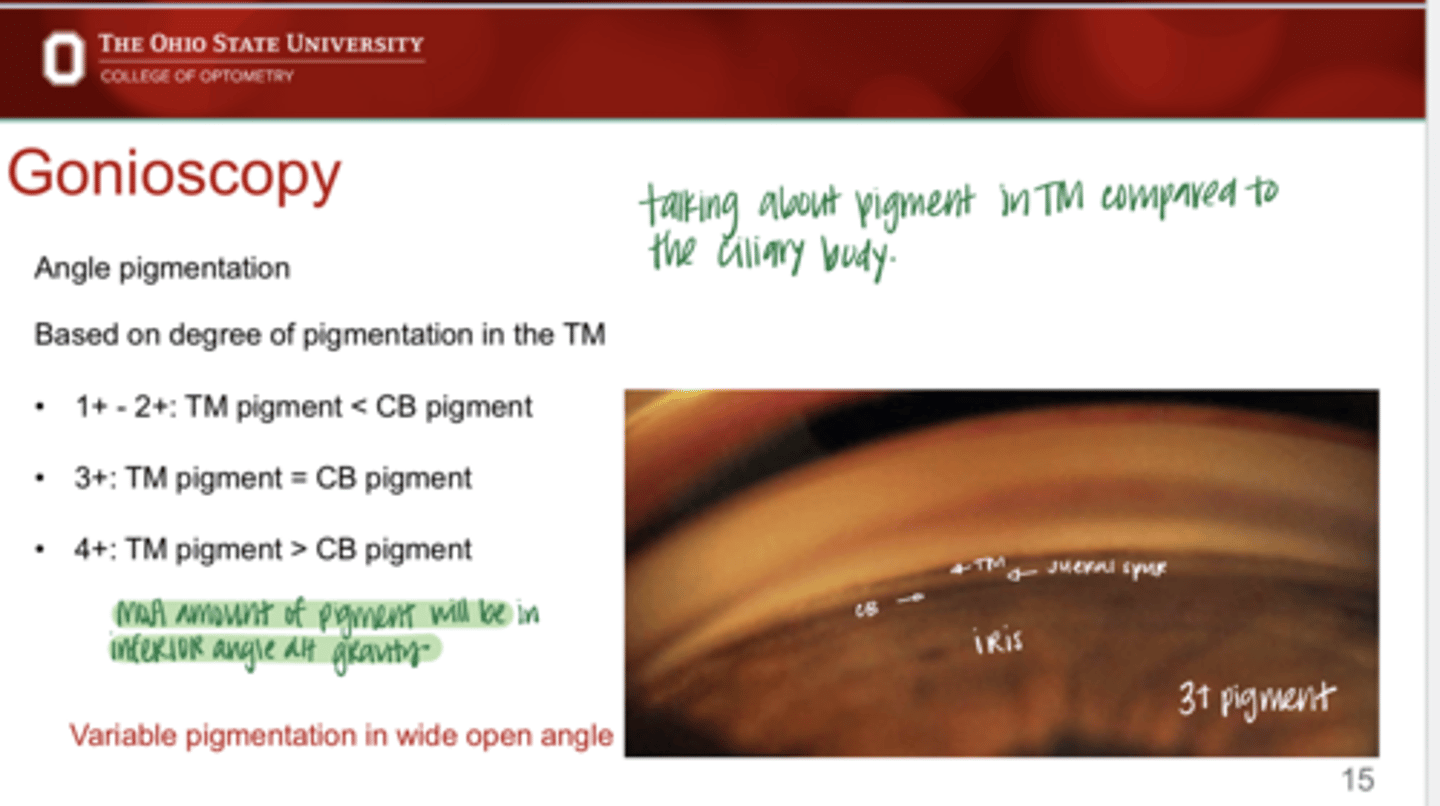
Grading Pigmentation in the Angle
TM pigment = CB pigment
3+
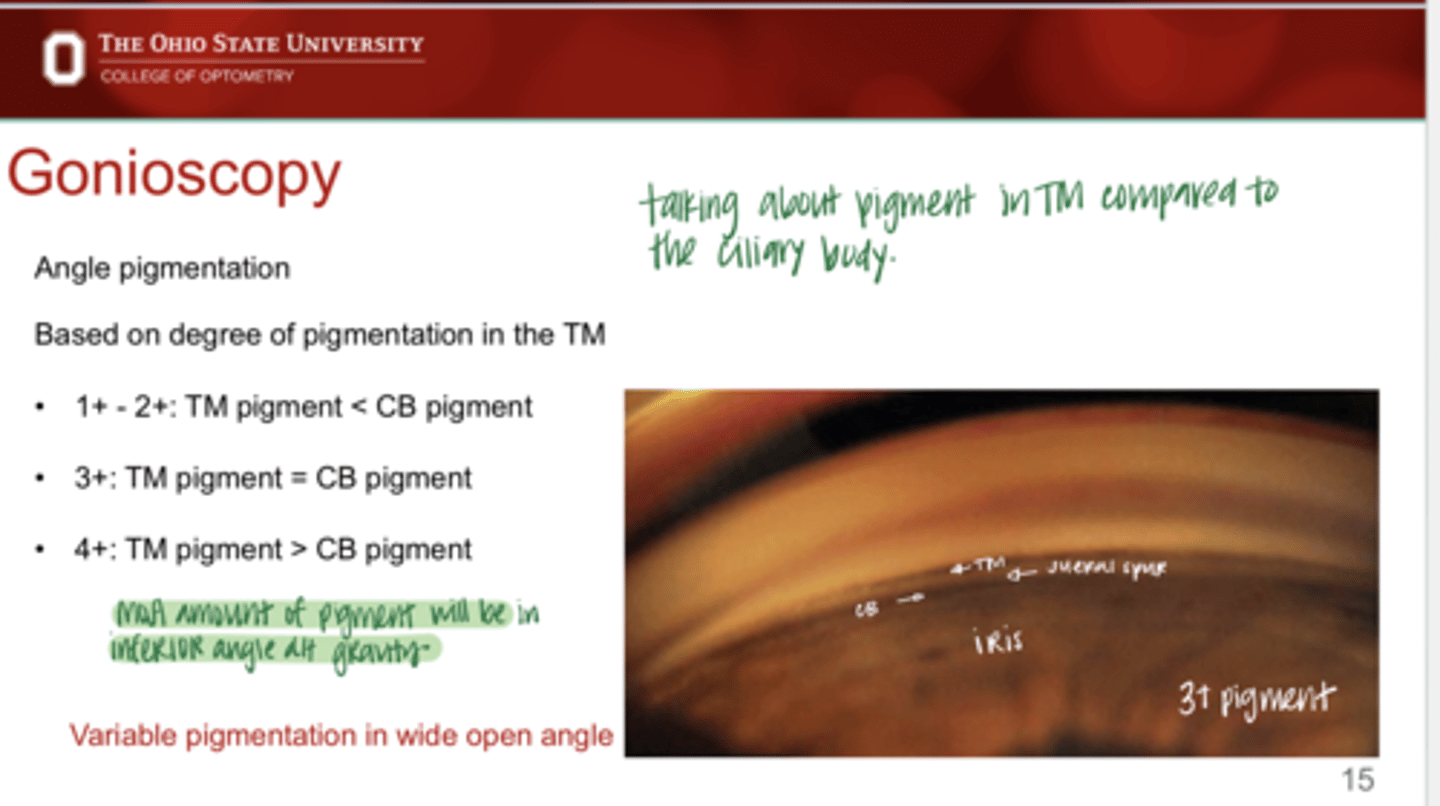
Grading Pigmentation in the Angle
TM pigment > CB pigment
4+
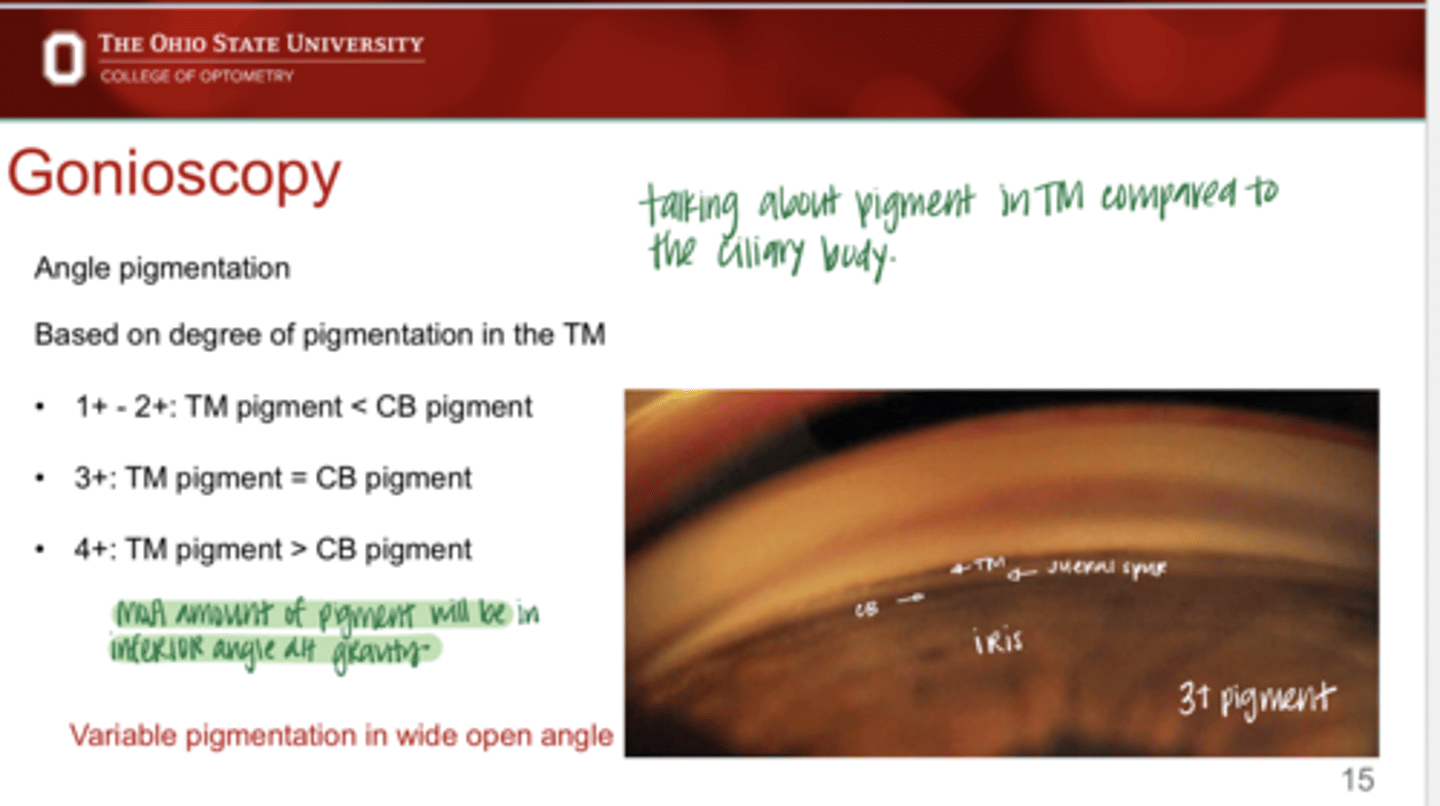
The most amount of pigment will likely be in the _____ angle
inferiori
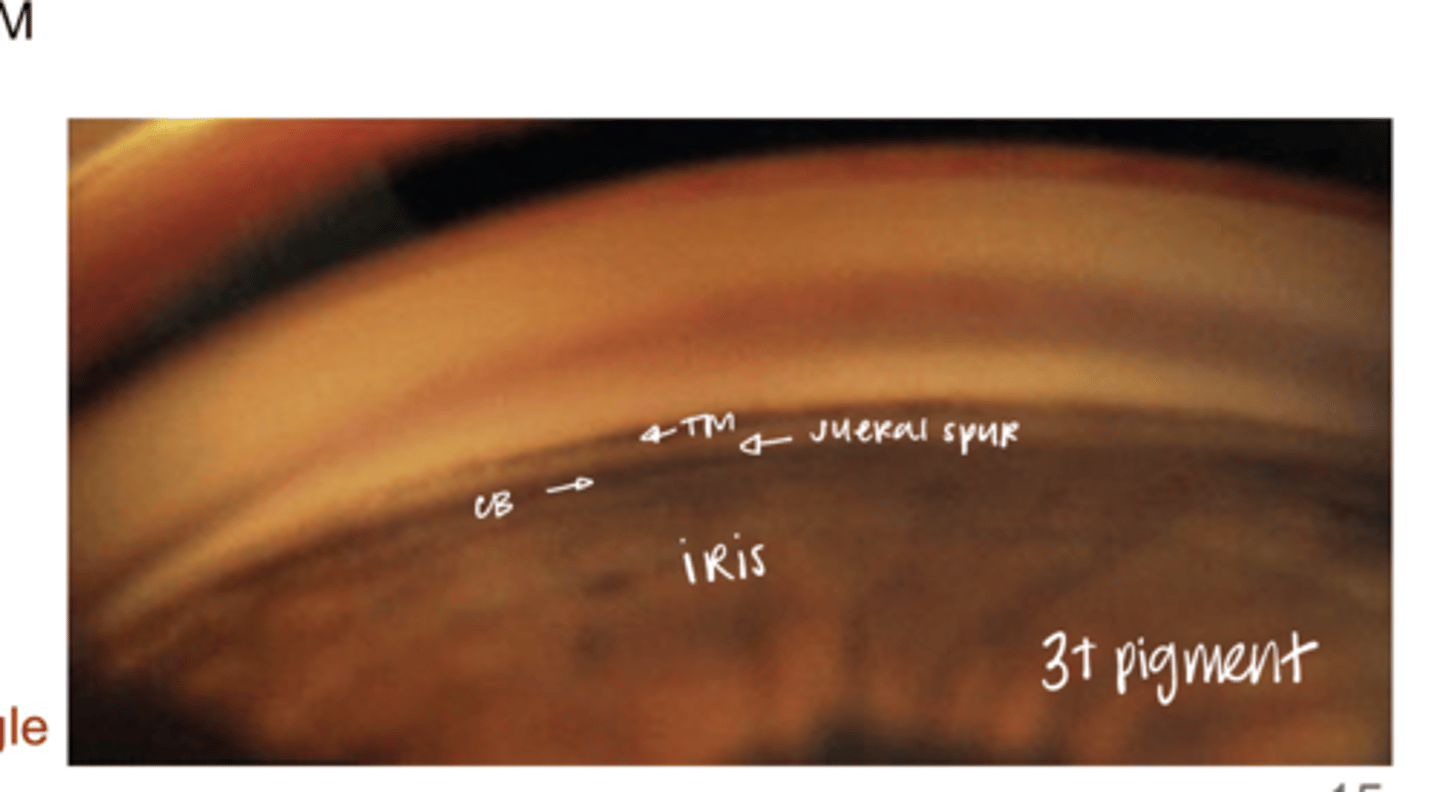
Grade 3+ Pigment in Open Angle (Pic)
Grade 3+ Pigment in Open Angle (Pic)
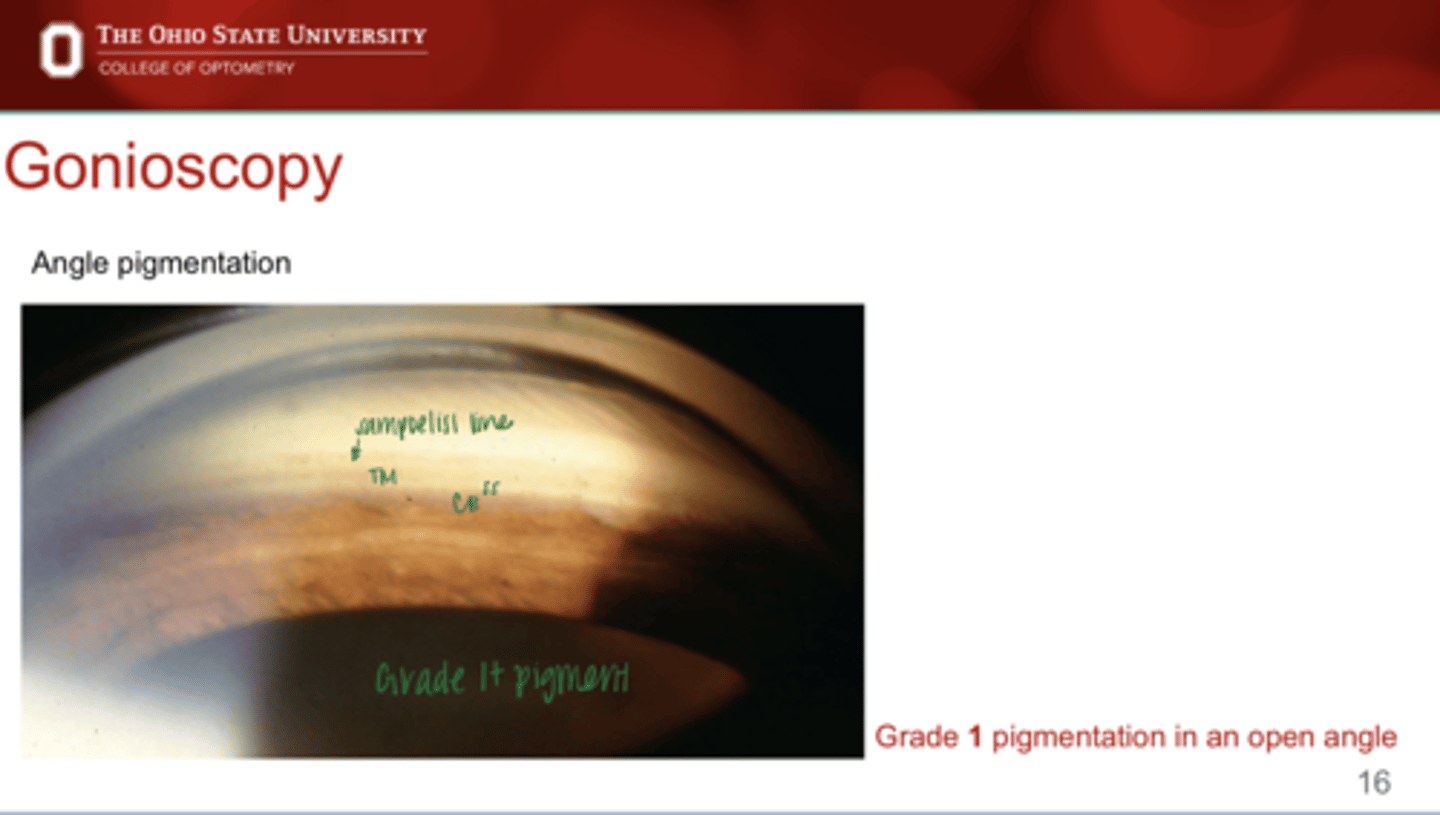
Grade 1+ PIgment in Open Angle (Pic)
Grade 1+ PIgment in Open Angle (Pic)
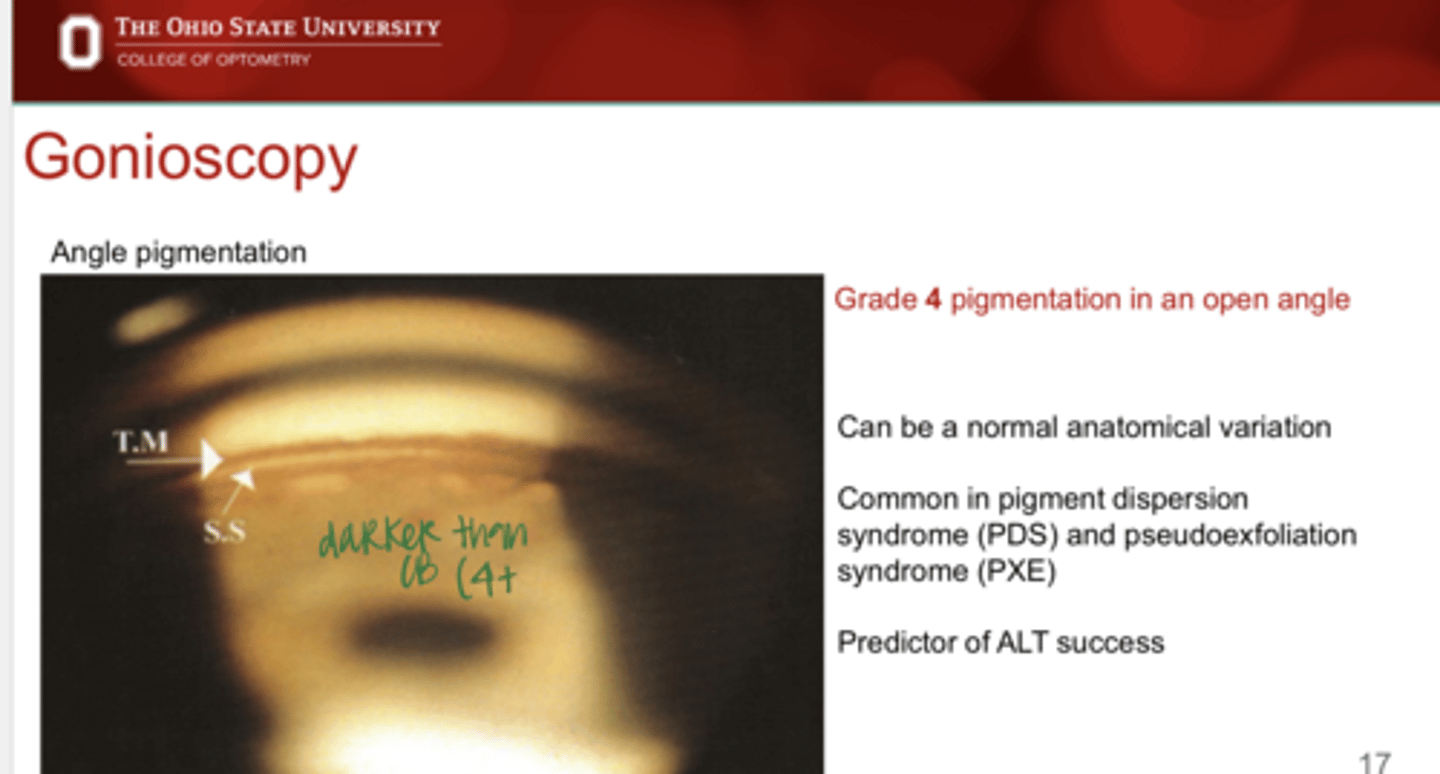
Grade 4+ Pigment in Open Angle (Pic)
Grade 4+ Pigment in Open Angle (Pic)
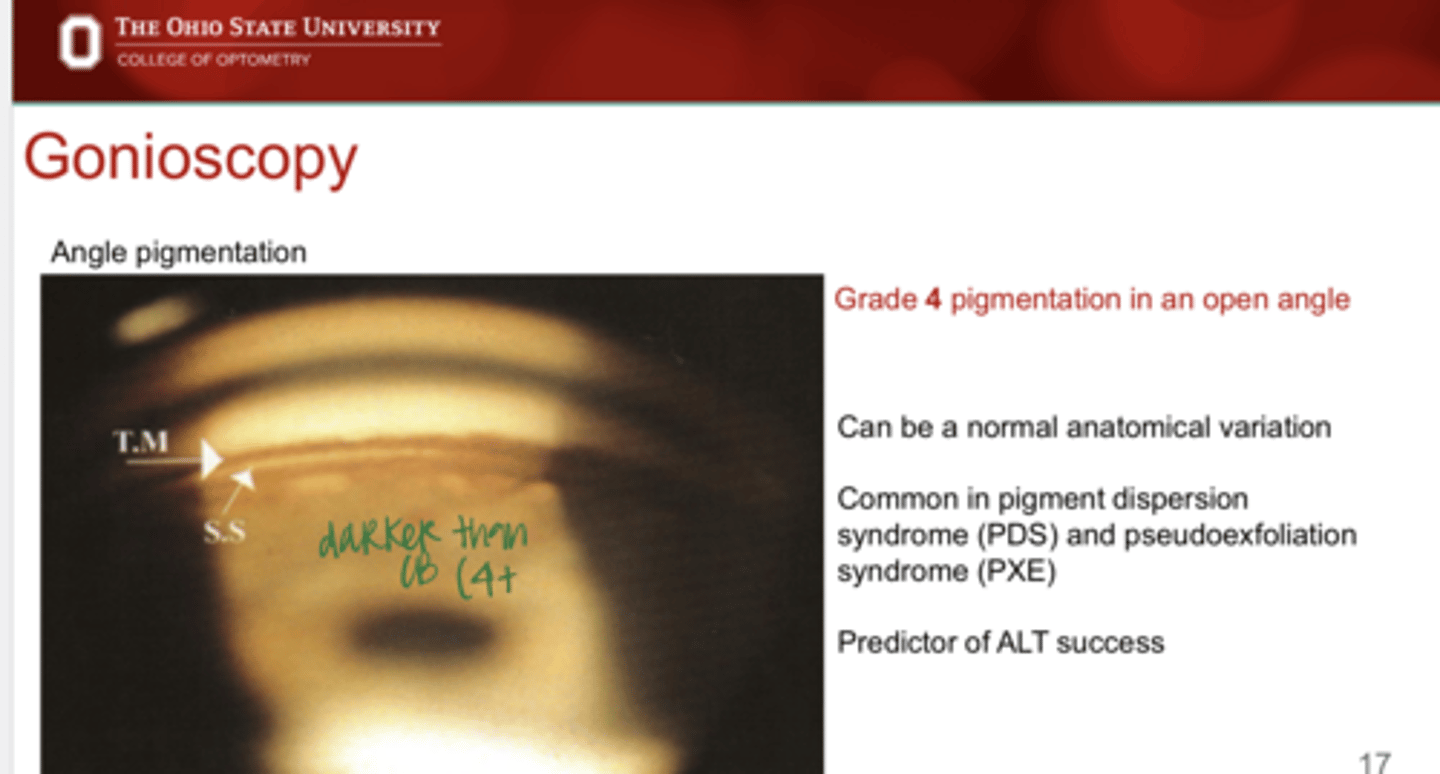
Can angle pigmentation be a normal variation?
Yes
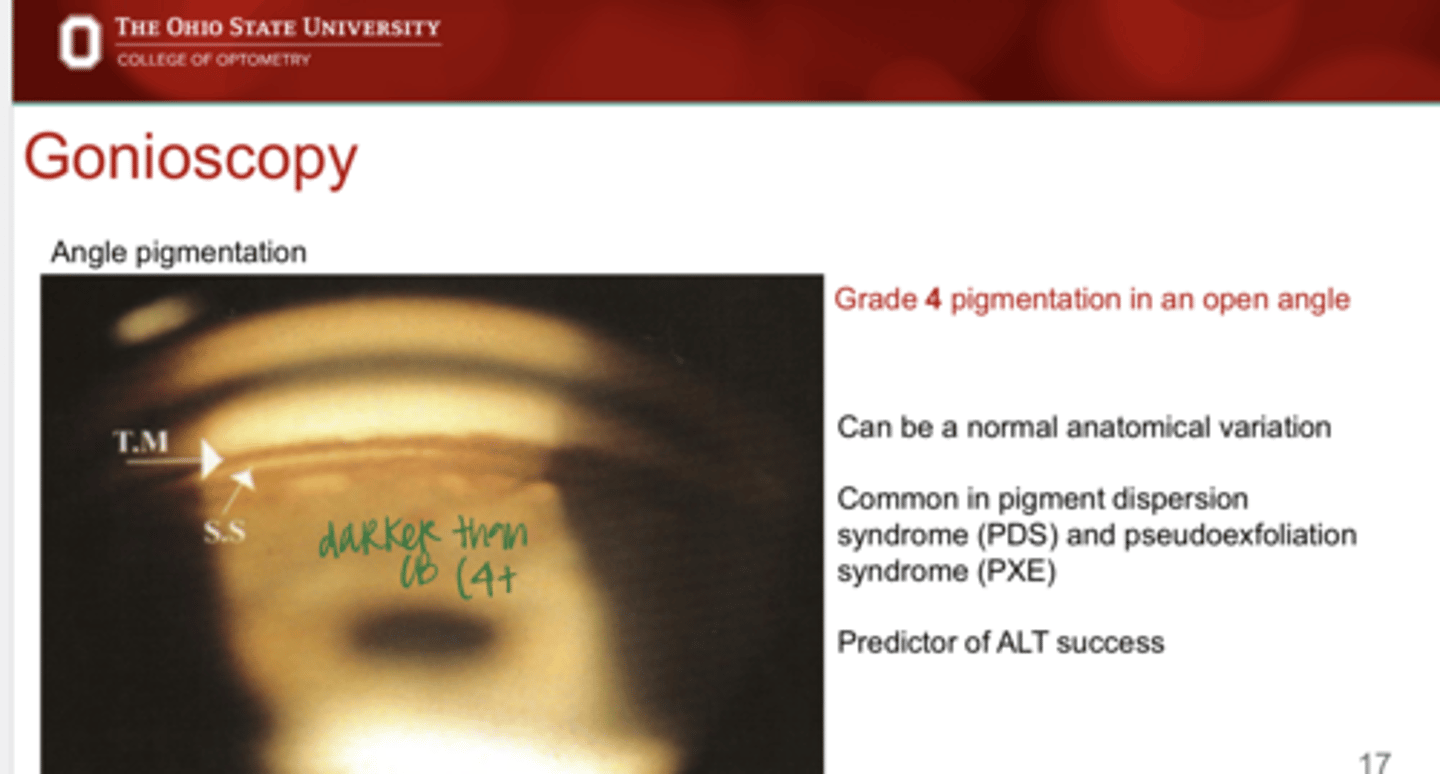
High levels of pigment in the angle is common in what conditions?
-Pigment dispersion syndrome (PDS)
-Pseudoexfoliation syndrome (PXE)
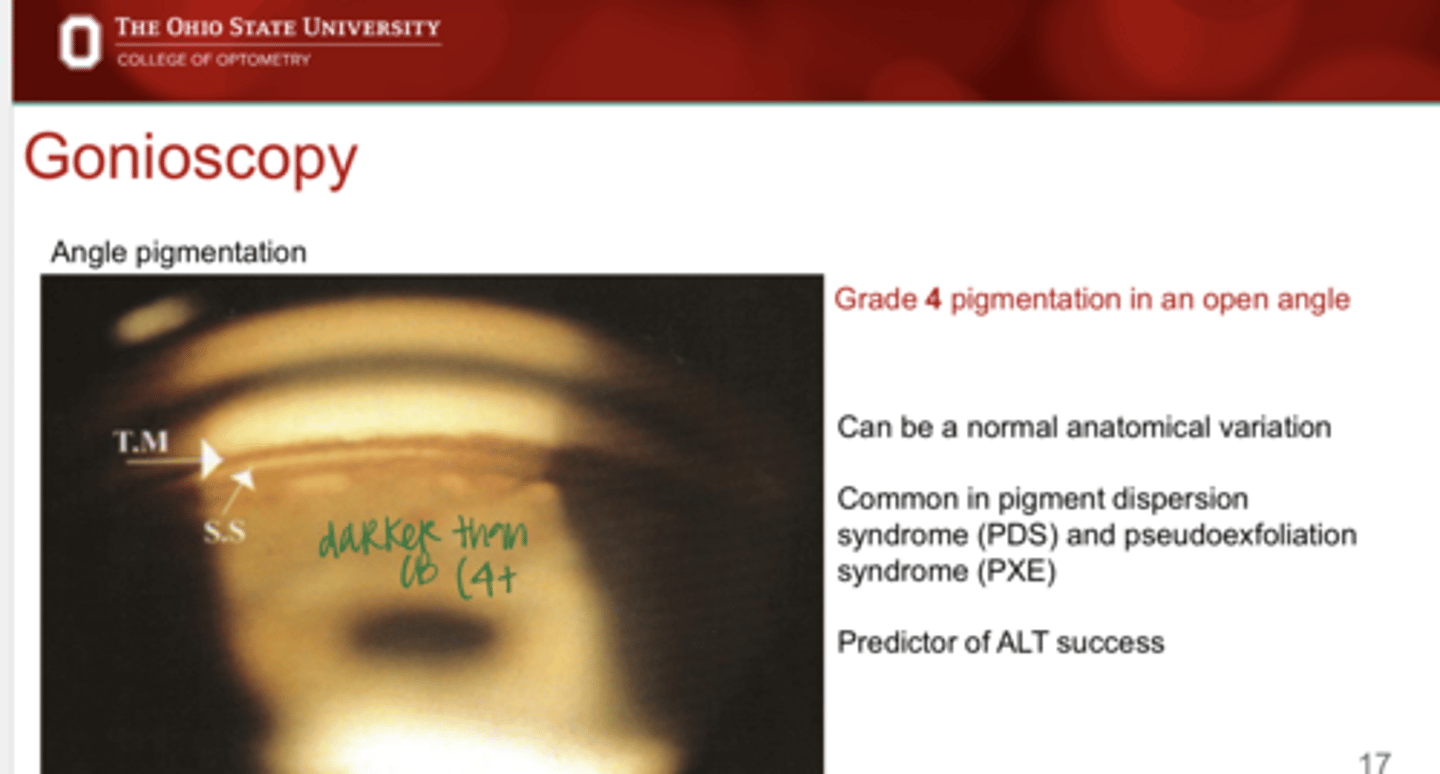
Levels of pigment in the angle is a predictor of ____ success
ALT
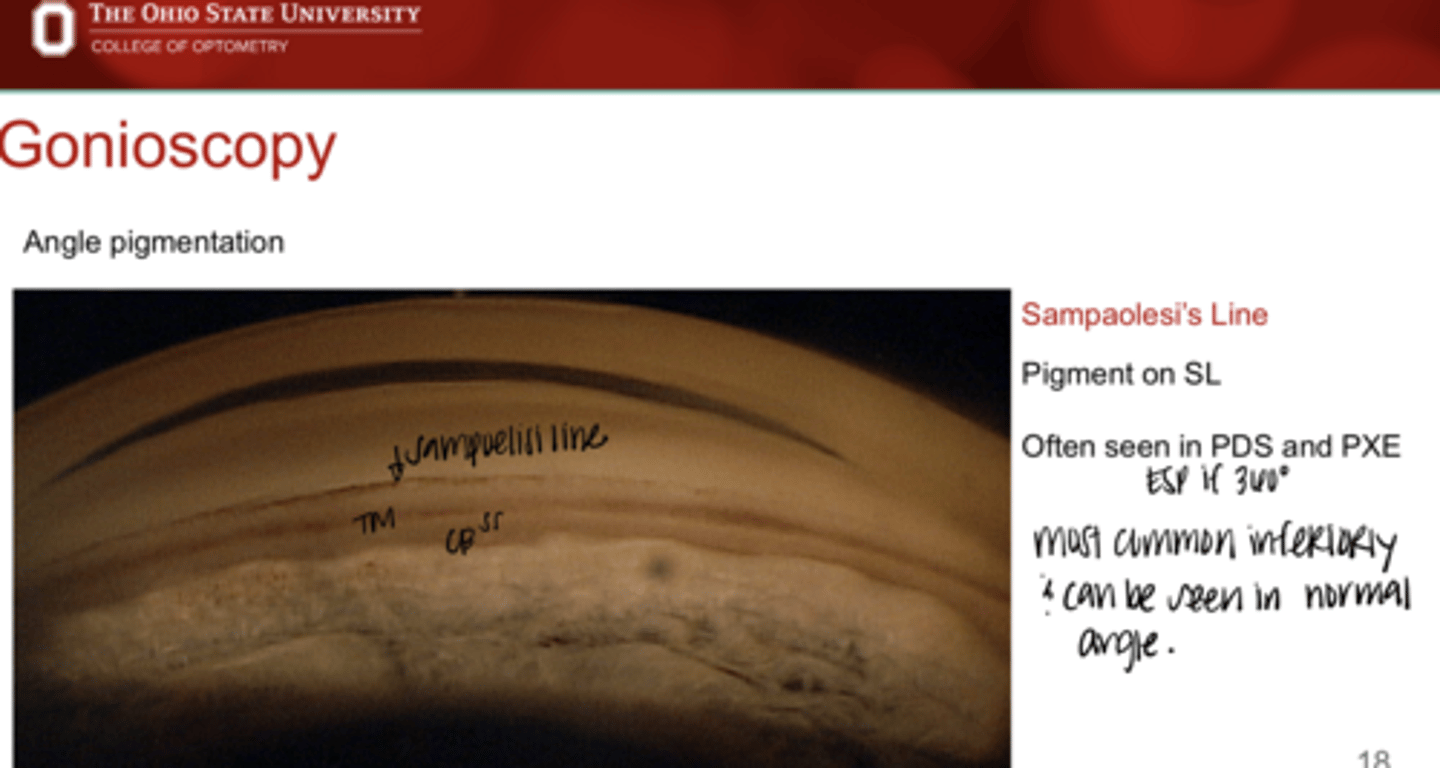
What is Sampaolesi Line?
pigment on Schwalbe's Line
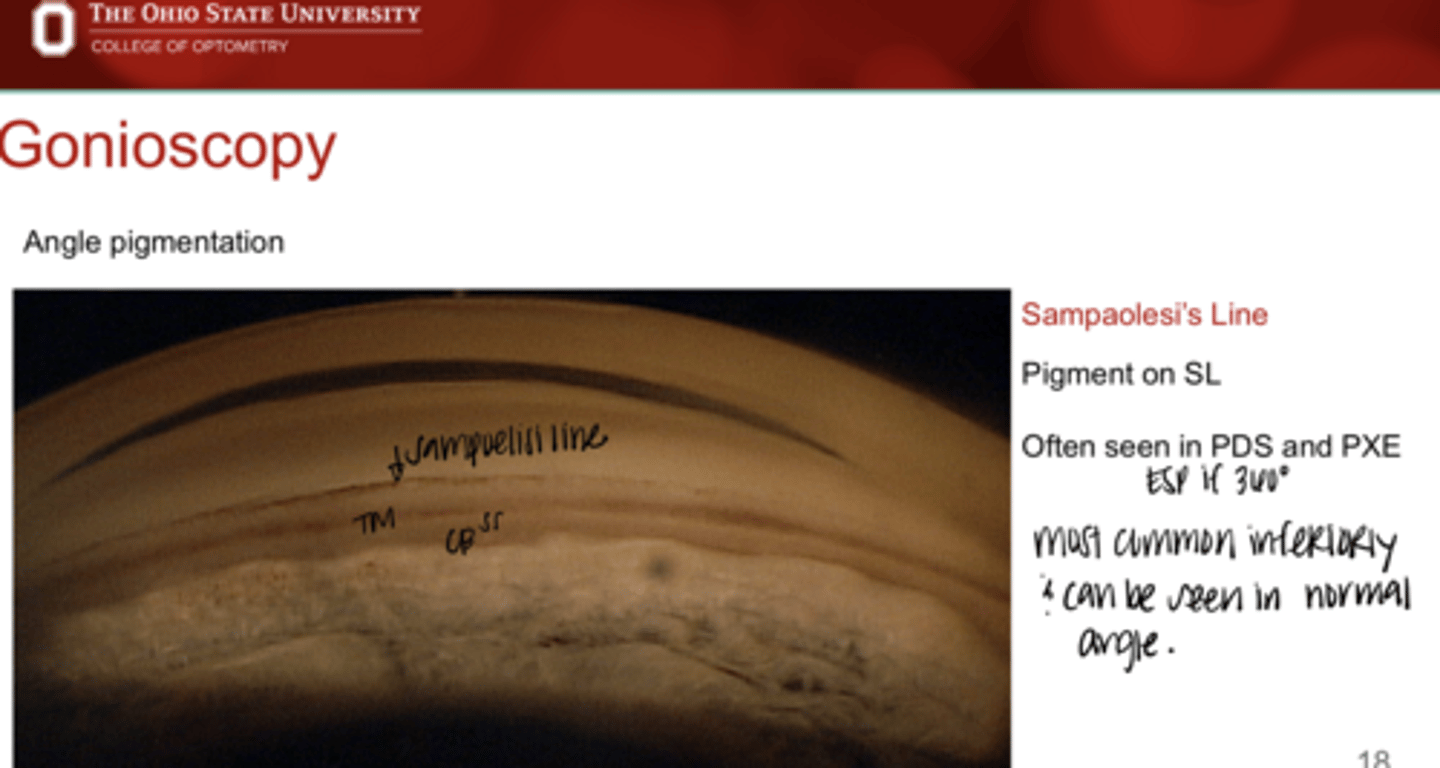
When is a Sampaolesi Line often present (conditions)?
-PDS
-PXE
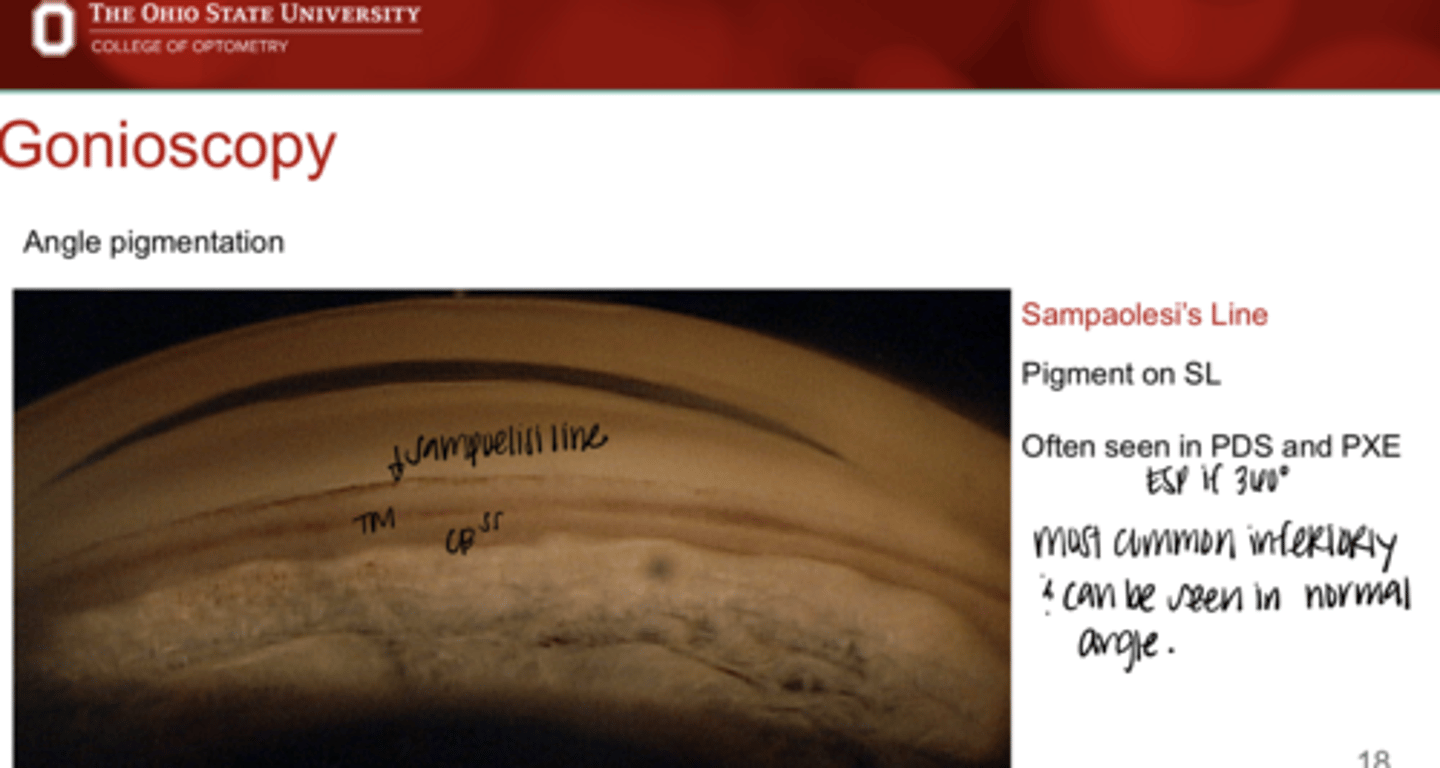
Where are Sampaolesi Line most commonly found?
inferior
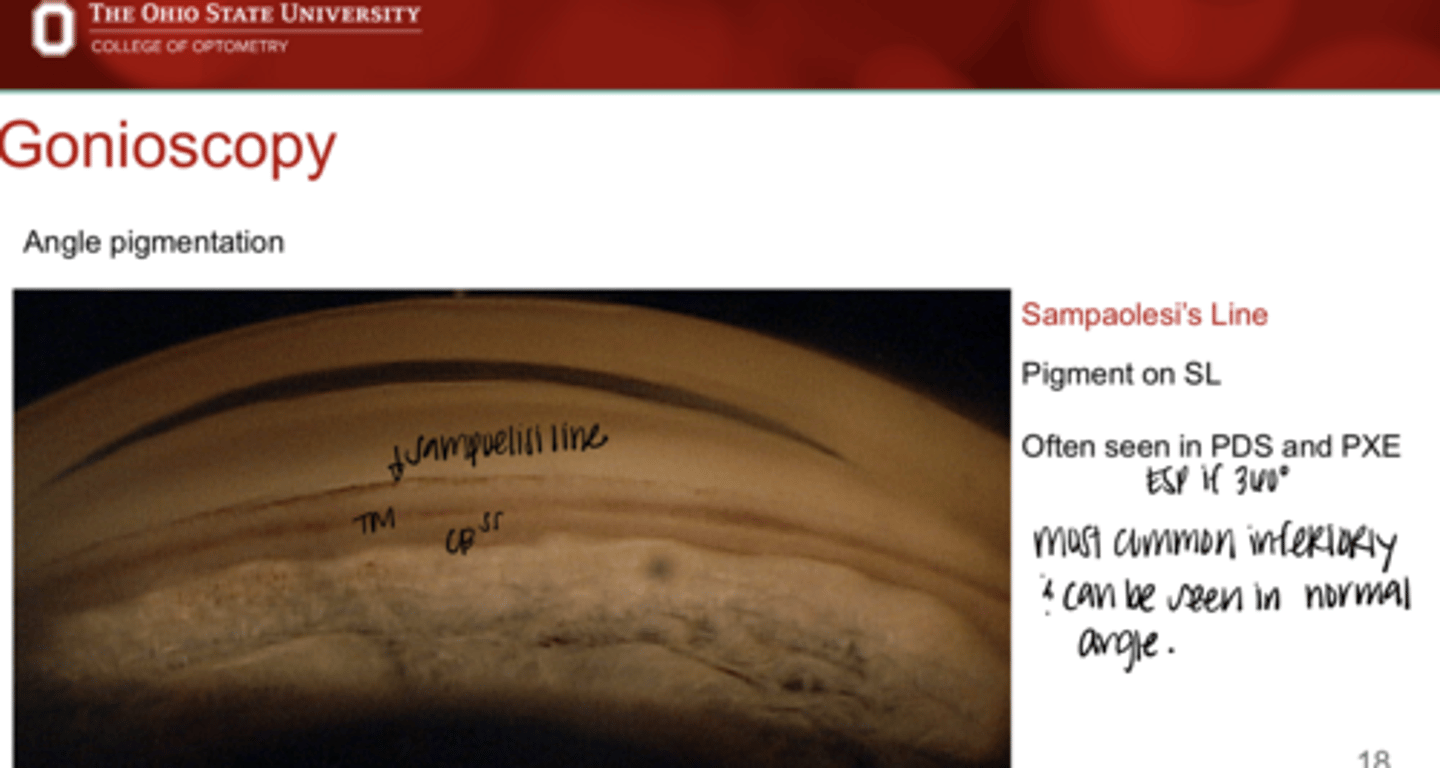
Can a Sampaolesi Line be found in a normal angle?
Yes
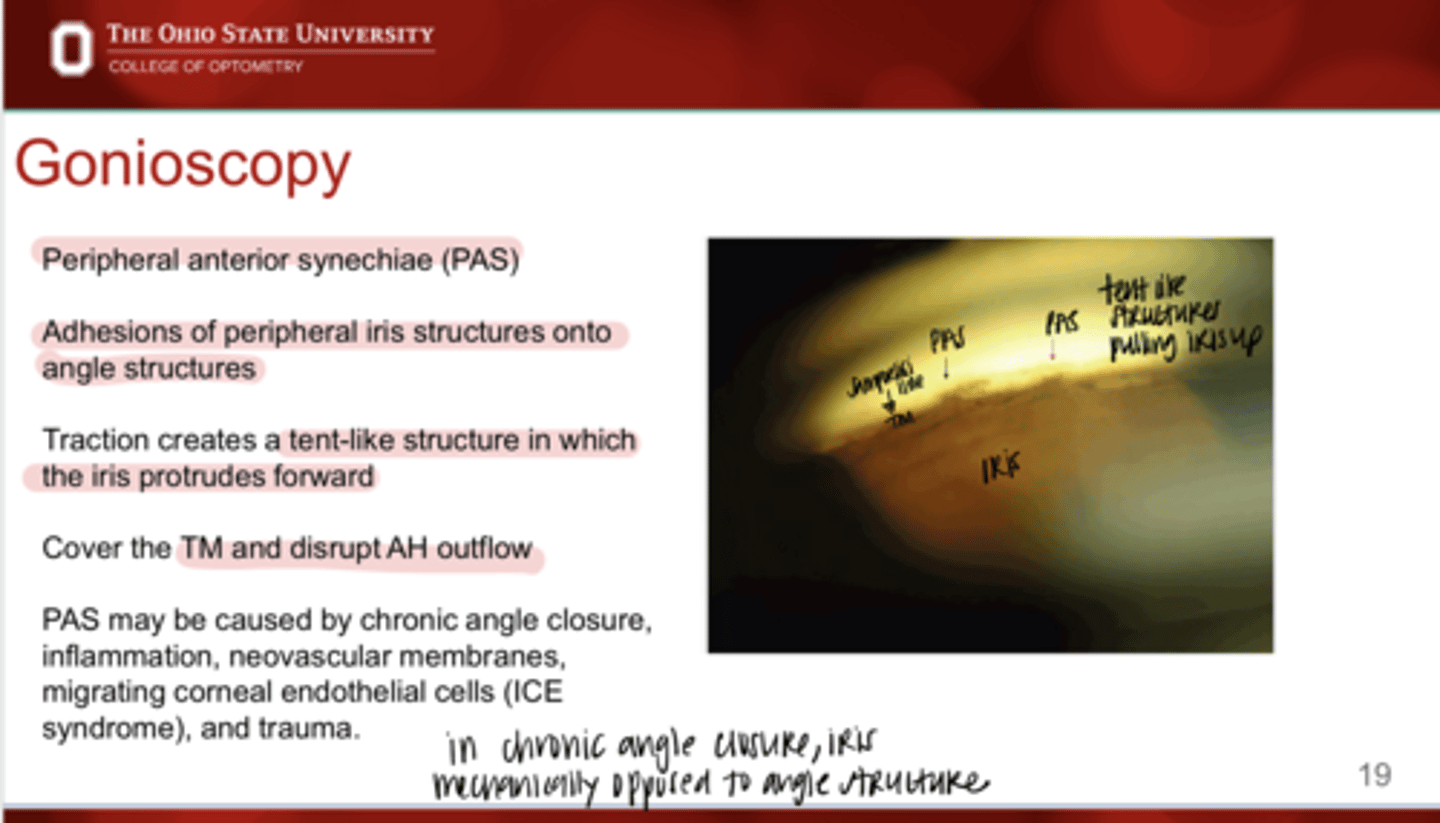
What is a peripheral anterior synechiae (PAS)?
adhesions of peripheral iris structures onto the angle structures
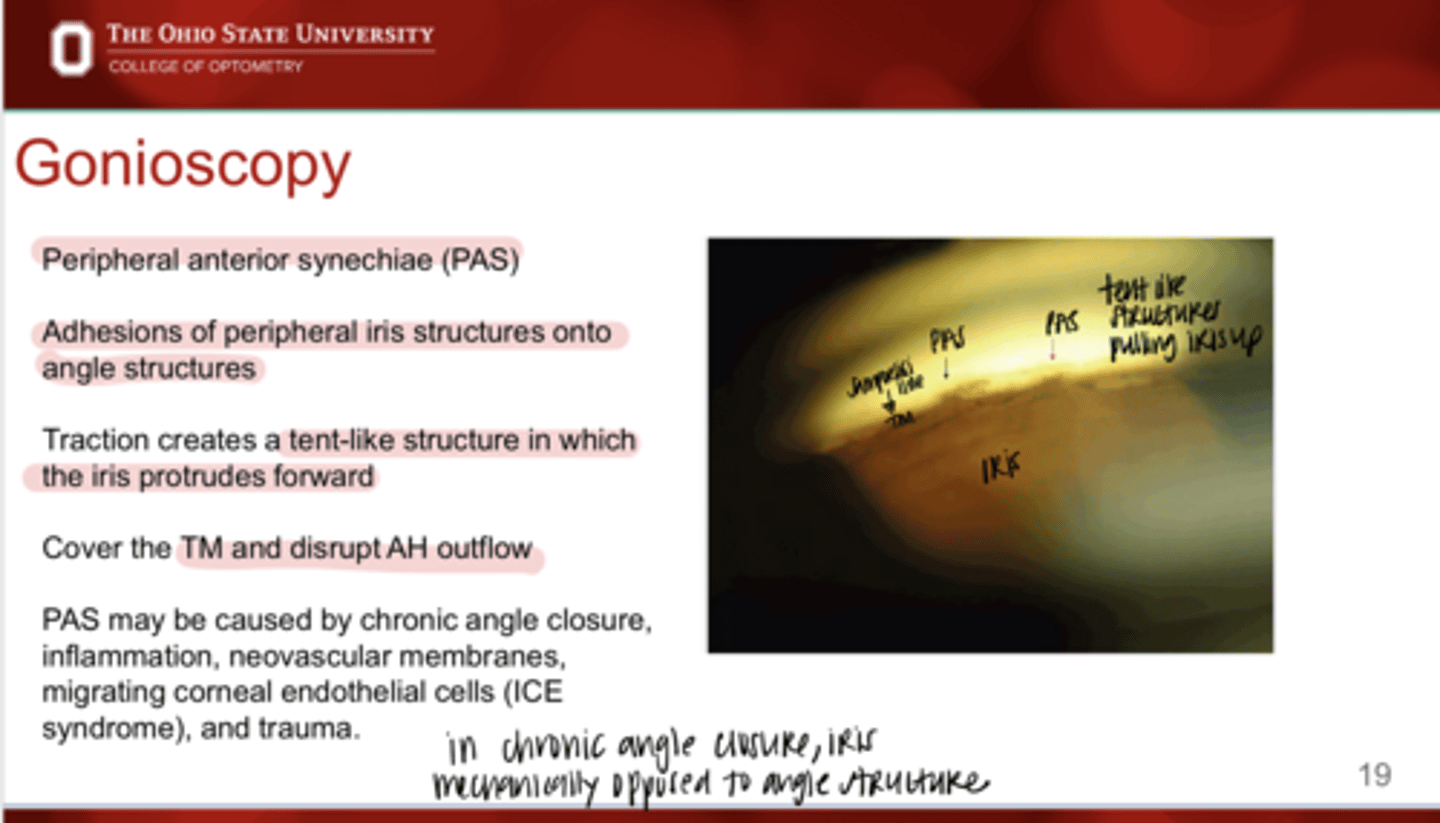
Traction from PAS creates what?
tent like structure that pulls the iris forward
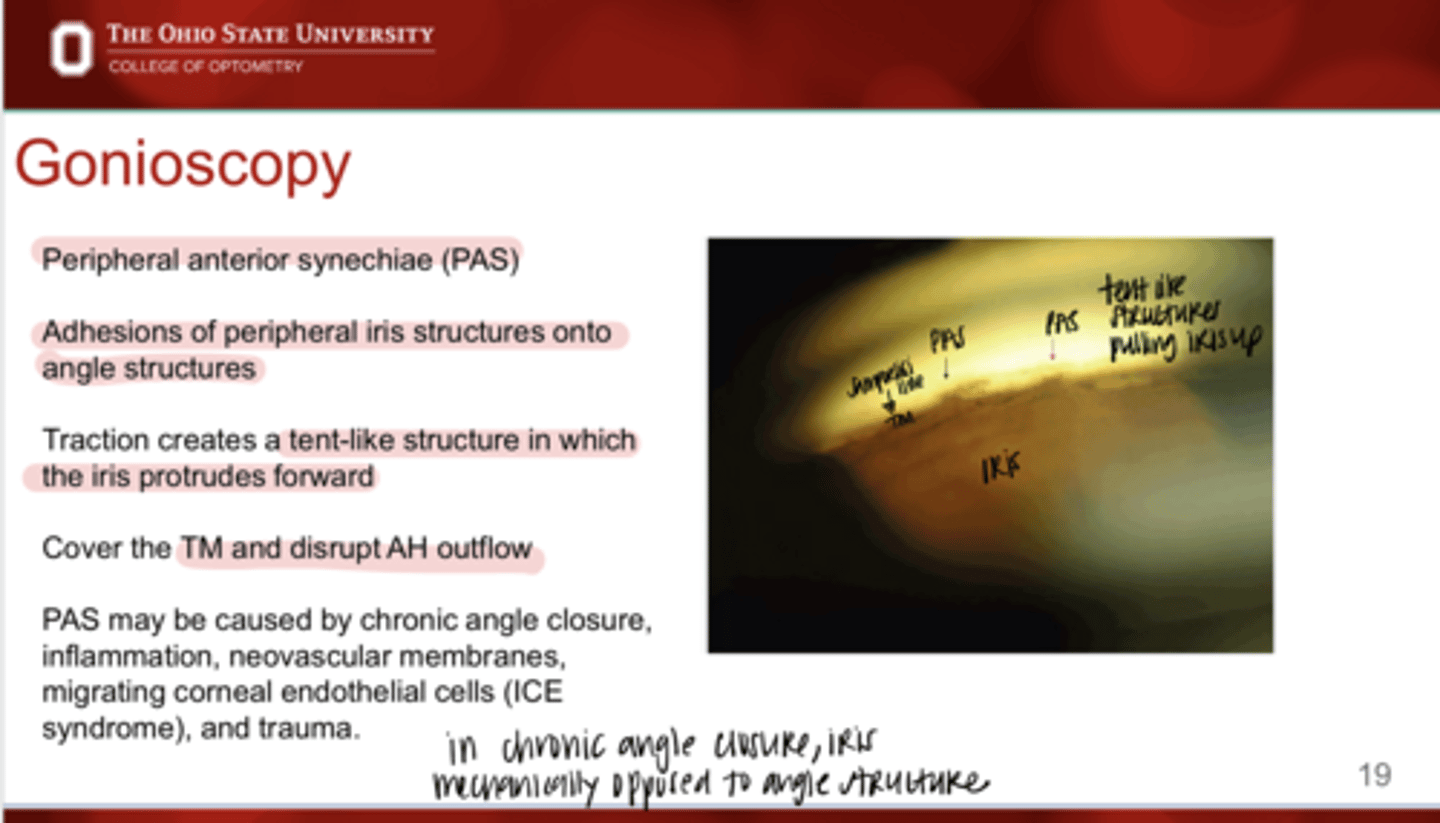
PAS will cover what angle structures?
TM
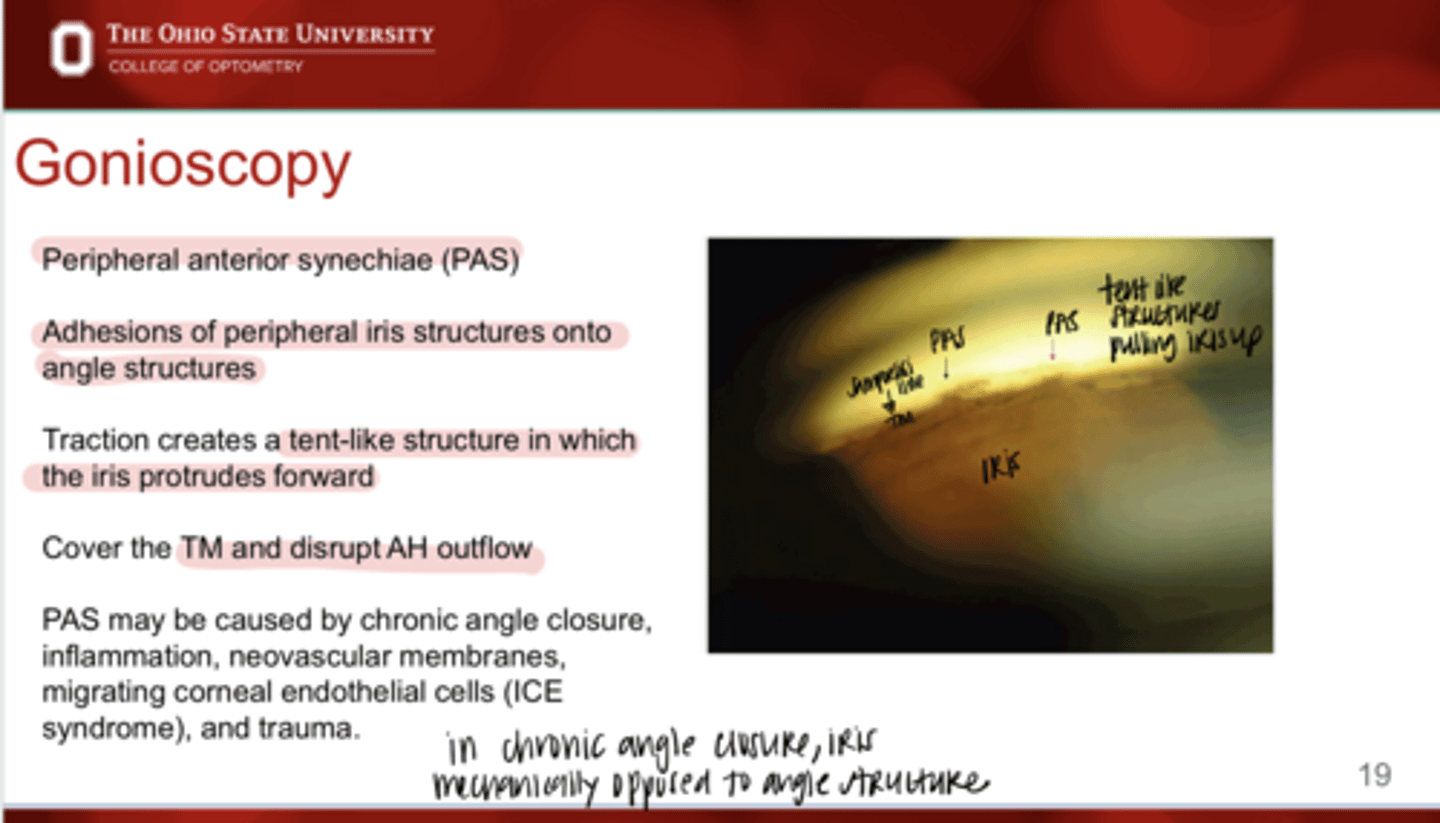
PAS will disrupt what?
aqueous outflow
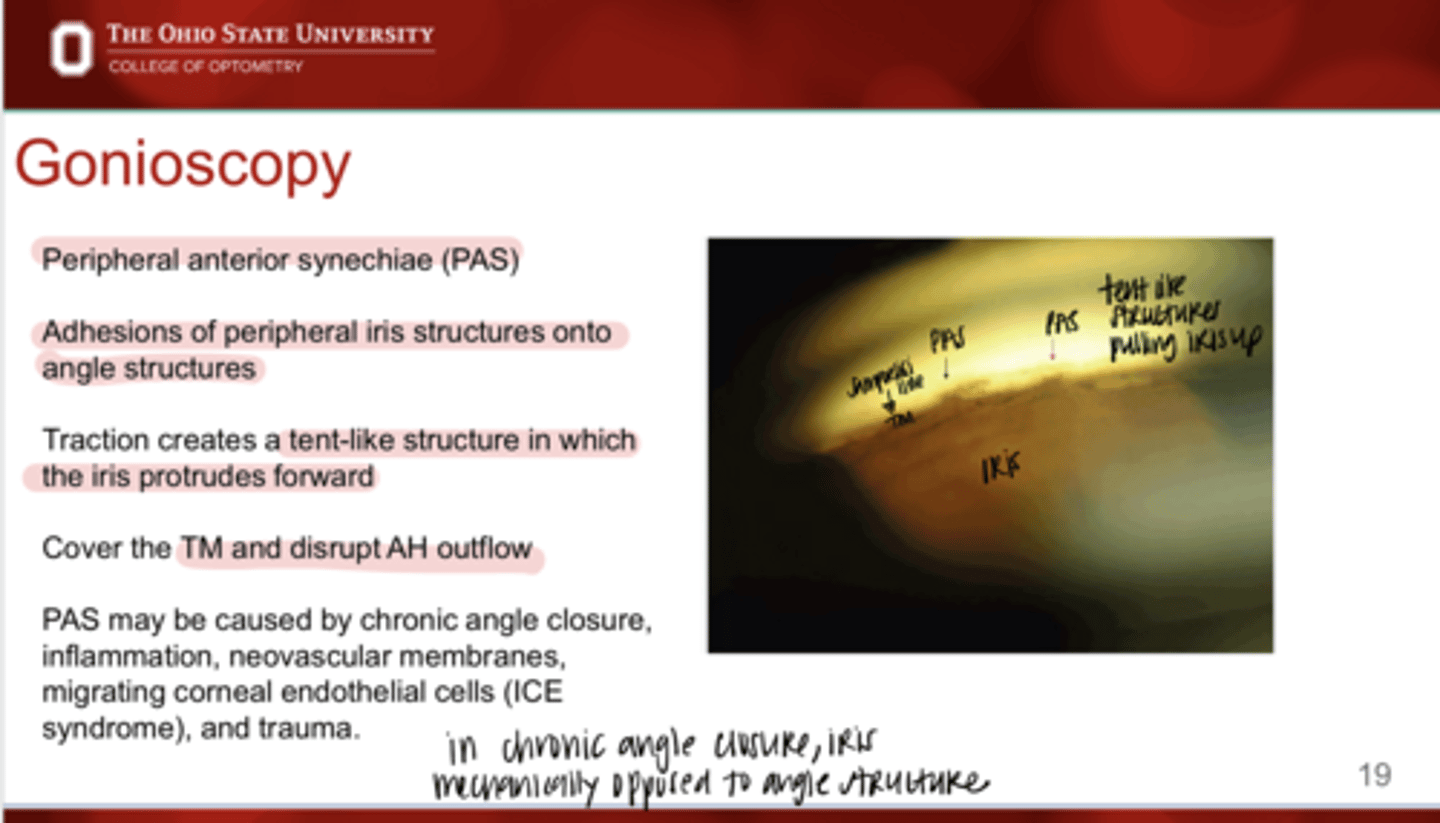
PAS may be caused by what?
-chronic angle closure
-inflammation
-neovasc membrane
-migrating corneal endothelial cells (ICE)
-trauma
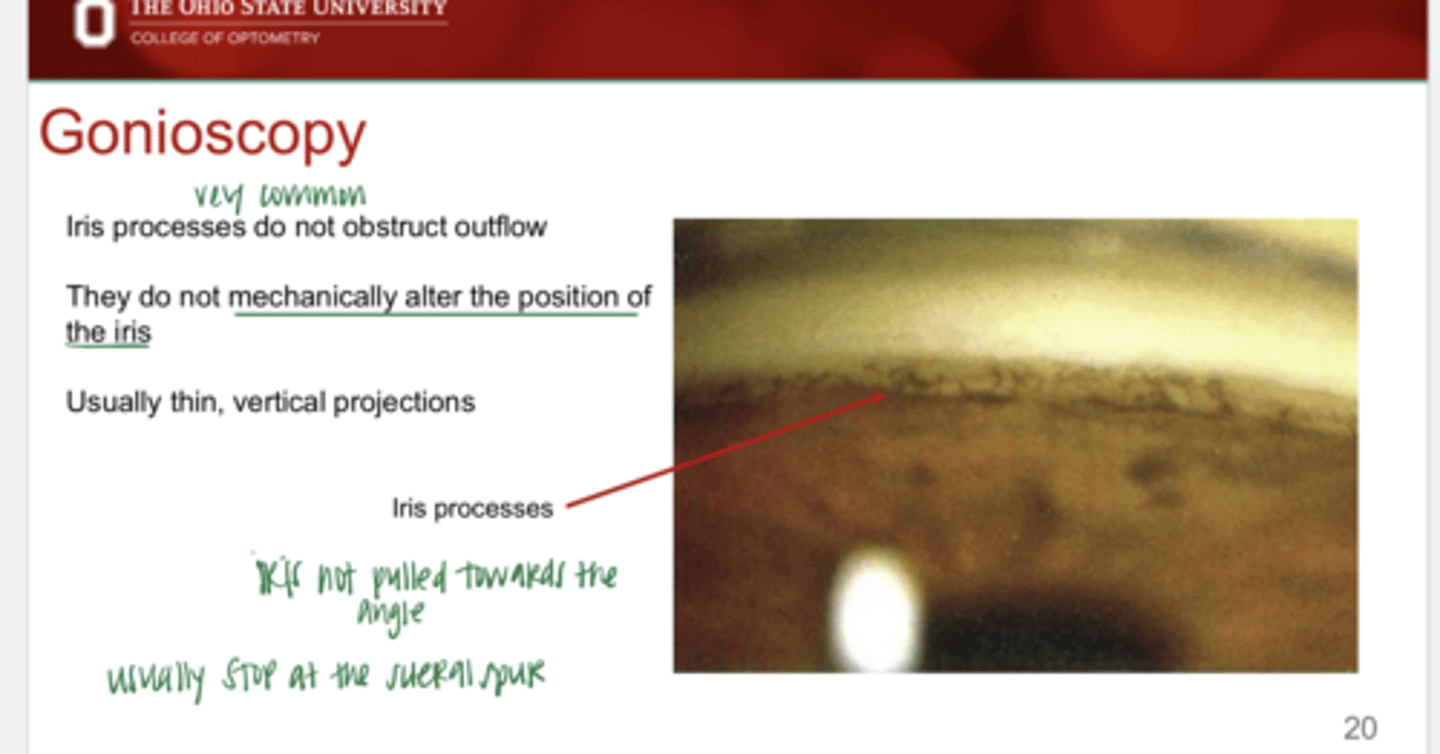
Are iris processes common?
Yes
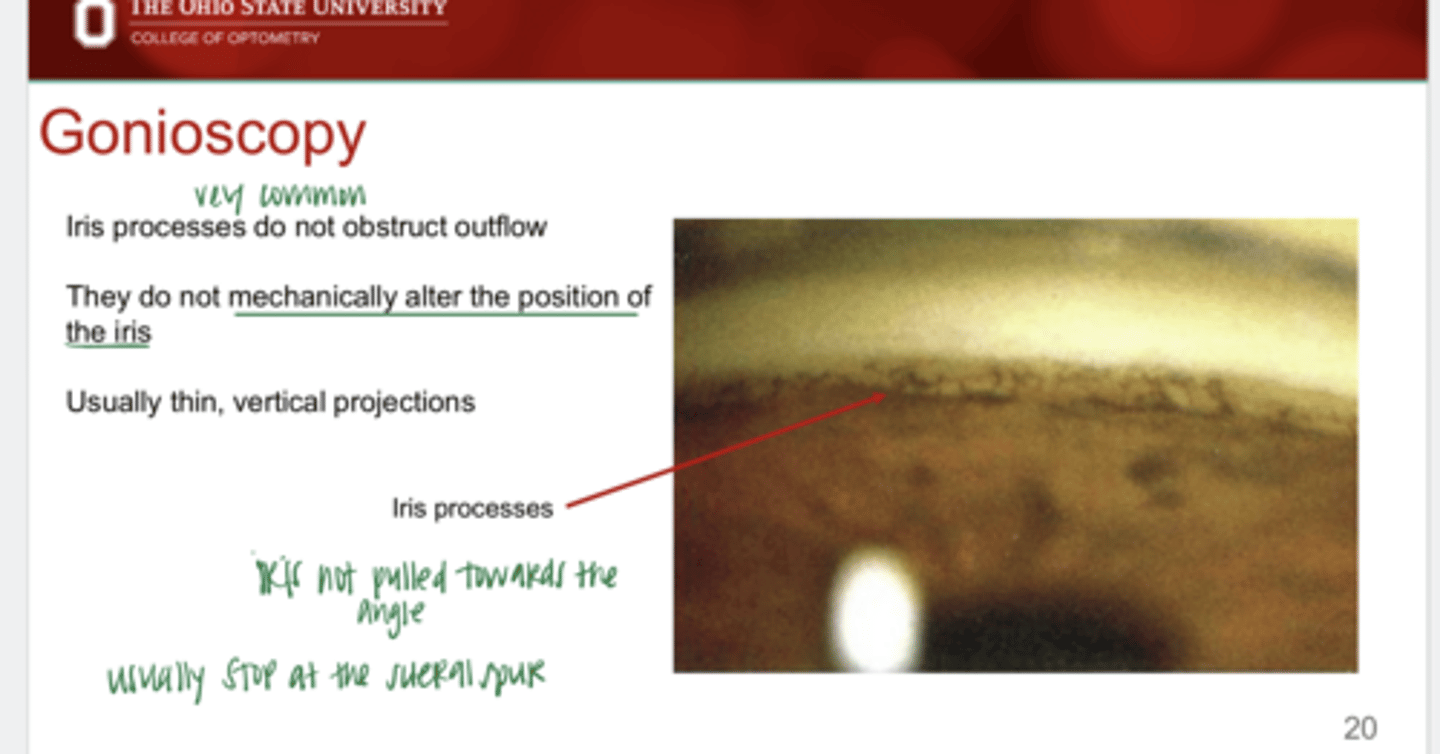
Do iris processes obstruct outflow of aqueous?
No
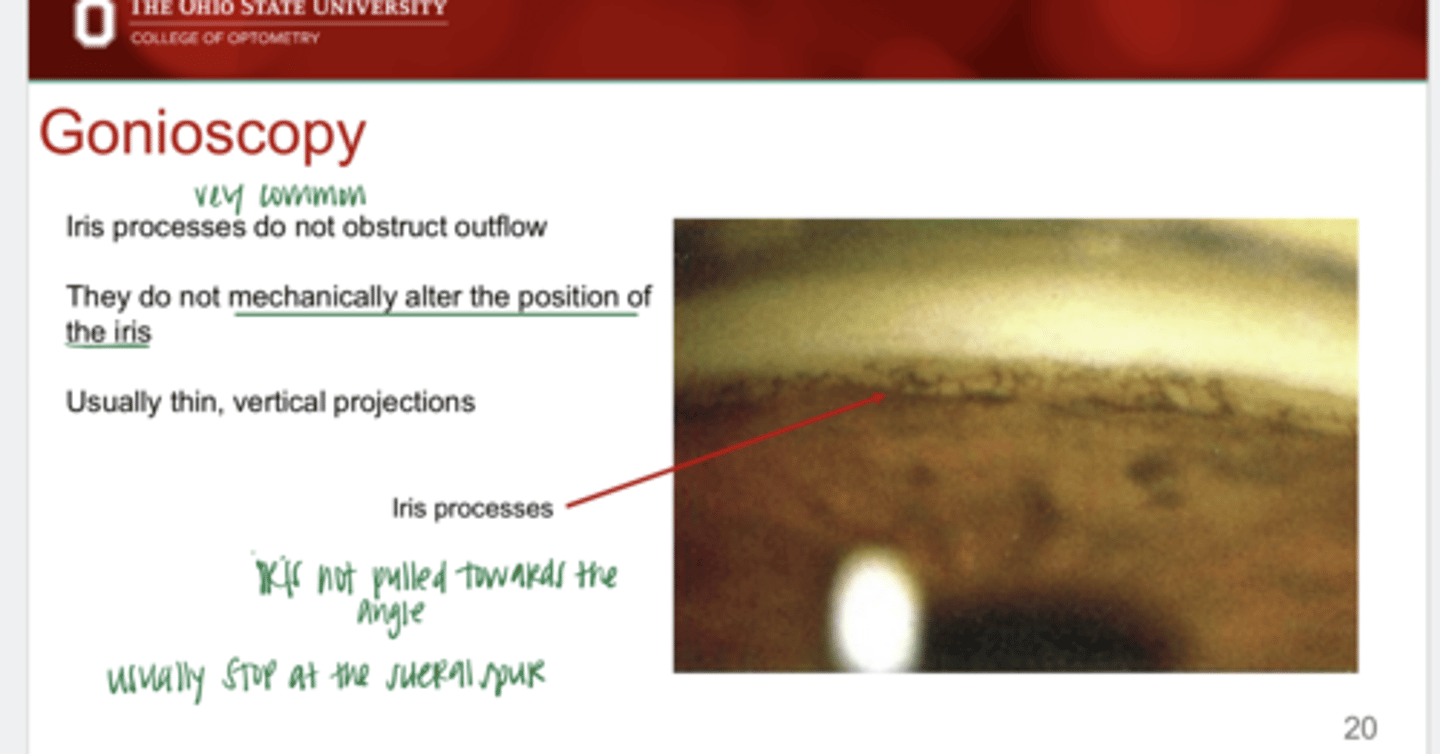
Do iris processes mechanically alter the position of the iris?
No
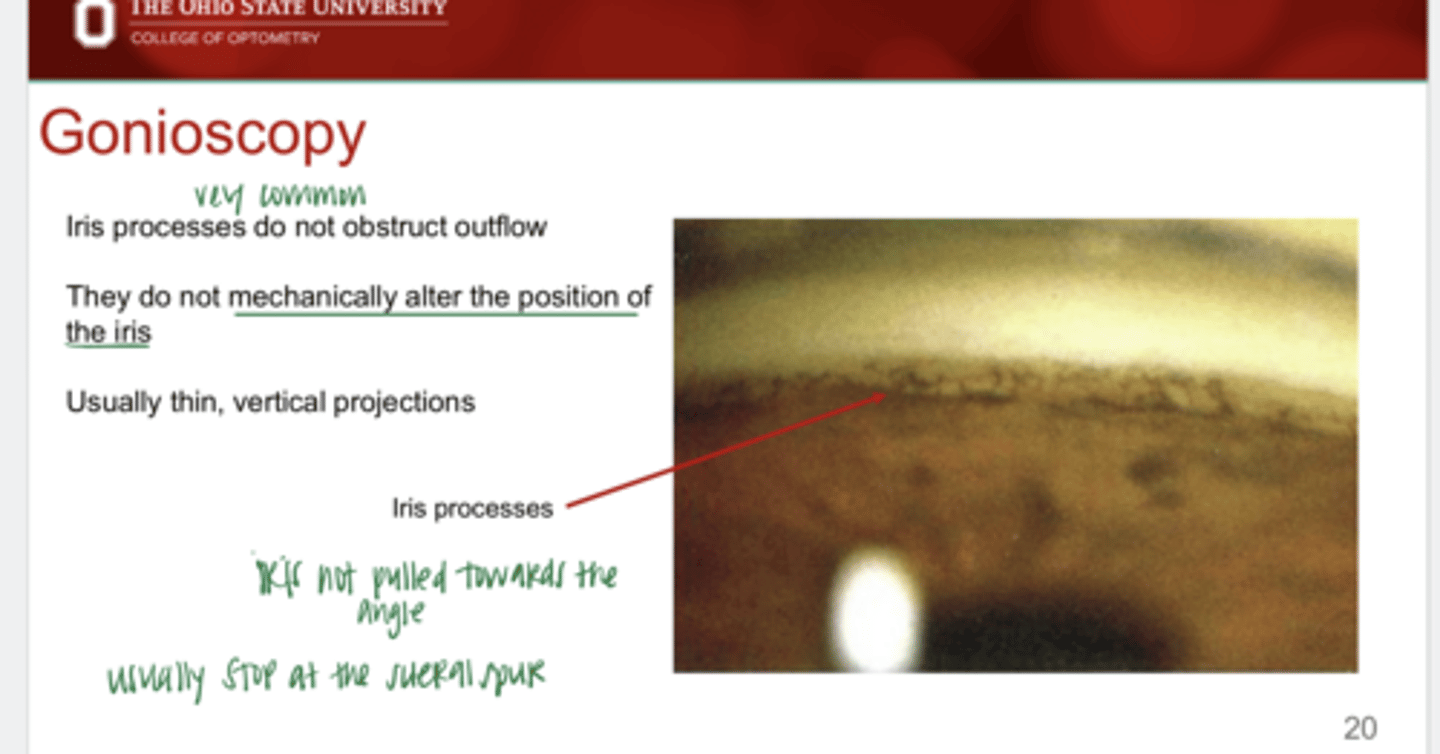
What is the appearance of iris processes?
thin, vertical projections
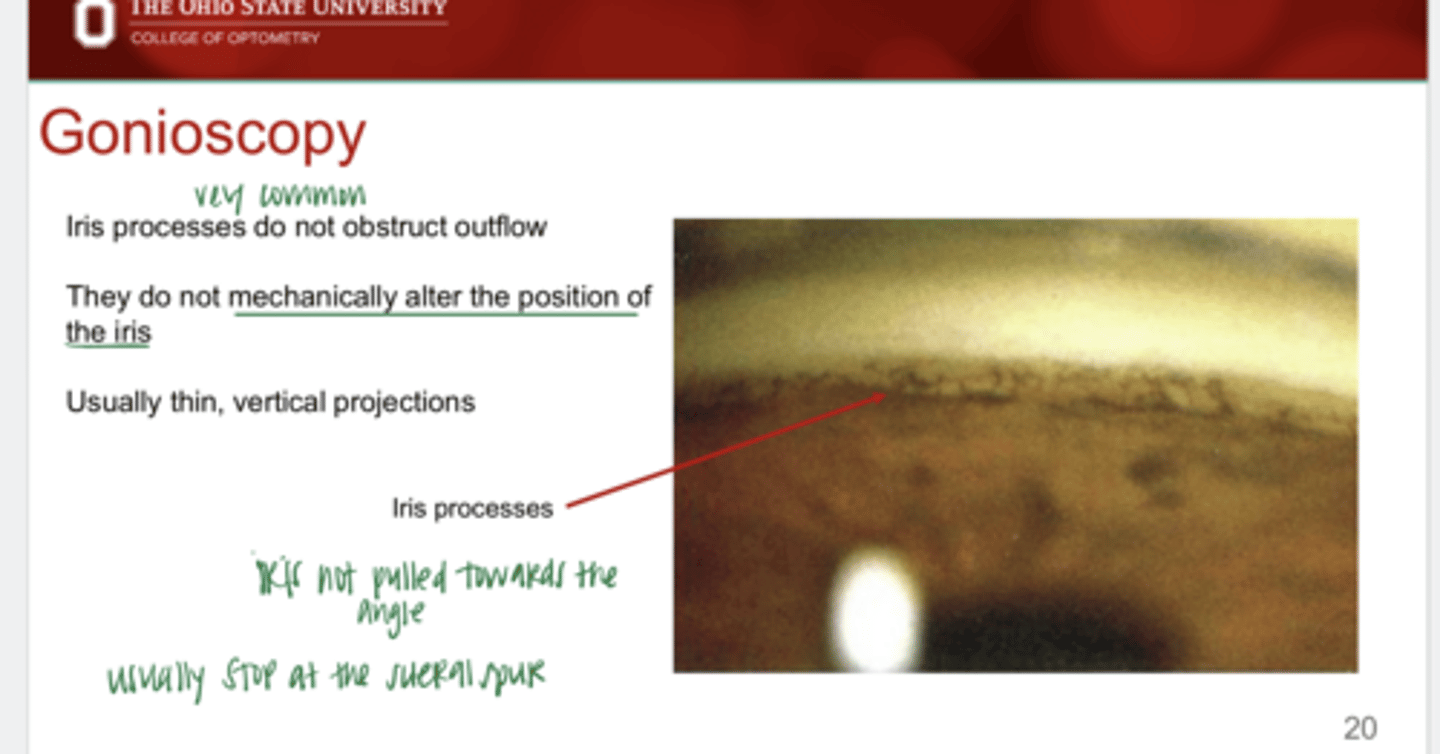
Iris processes usually stop at what angle structure?
scleral spur
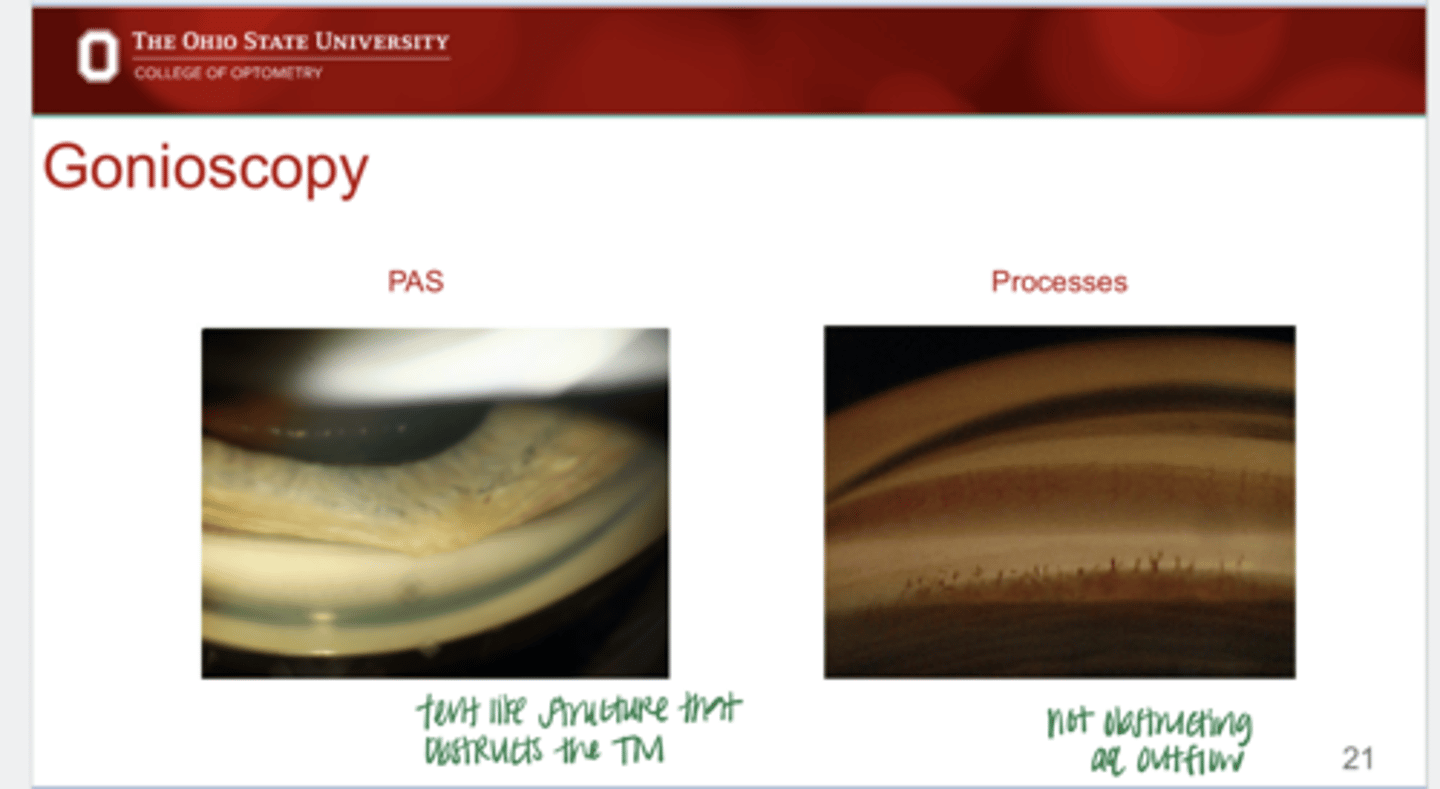
PAS v Iris Processes (Pic)
PAS v Iris Processes (Pic)
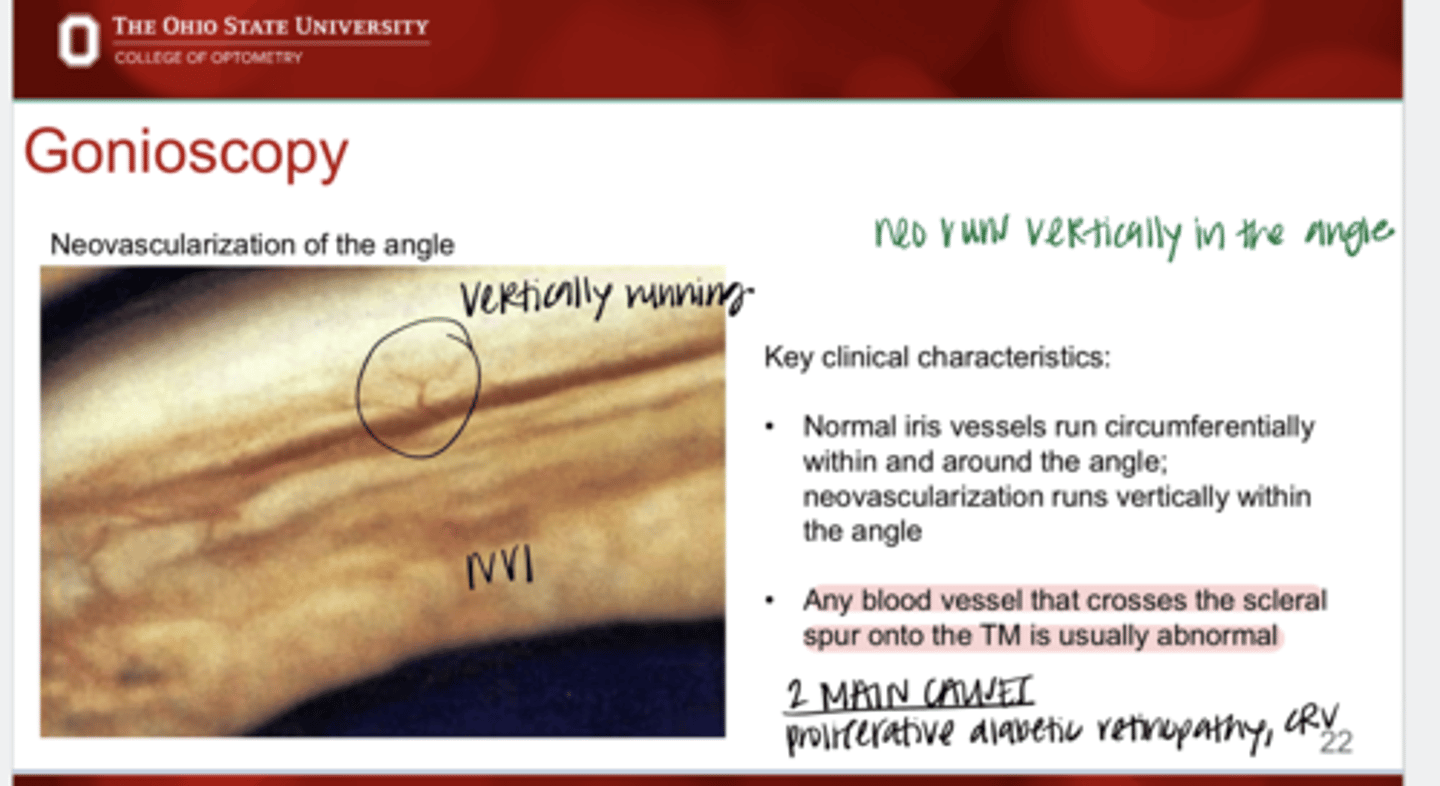
What are the key clinical characteristics of neovac of the angle?
runs vertically within the angle
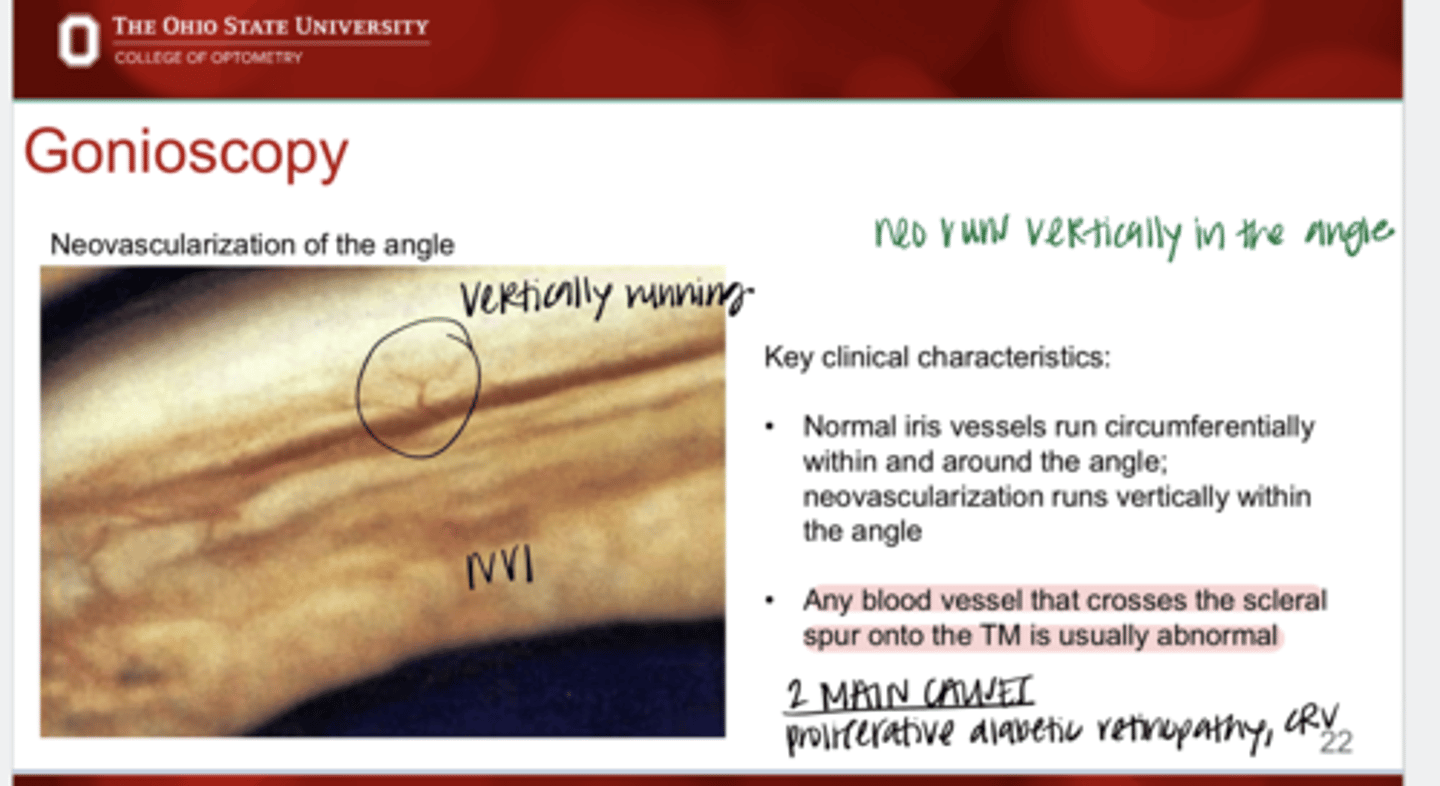
Do normal iris vessels run vertically?
No -- they run circumferentially within and around the angle
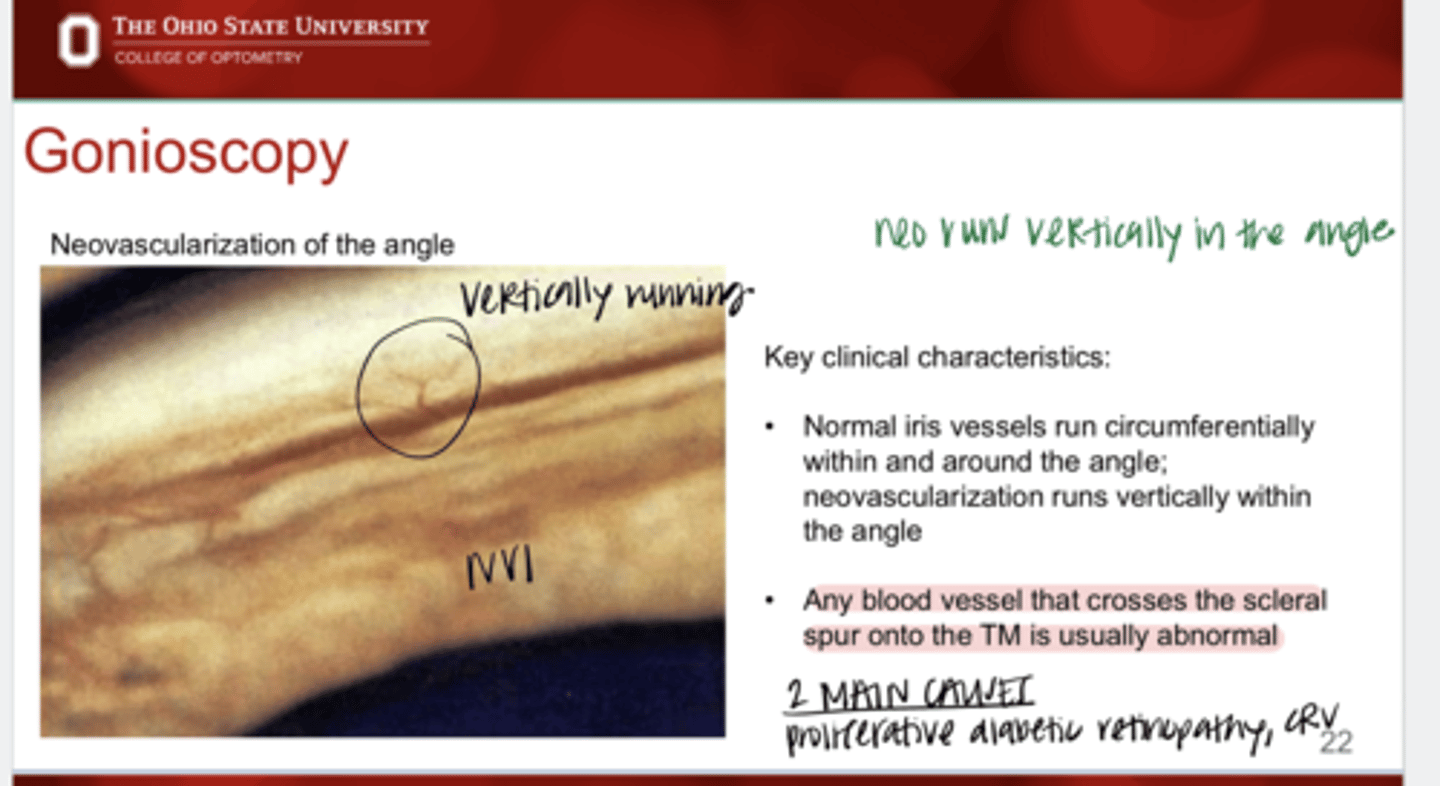
True or False:
Any blood vessel that crosses the scleral spur onto the TM is usually abnormal
true
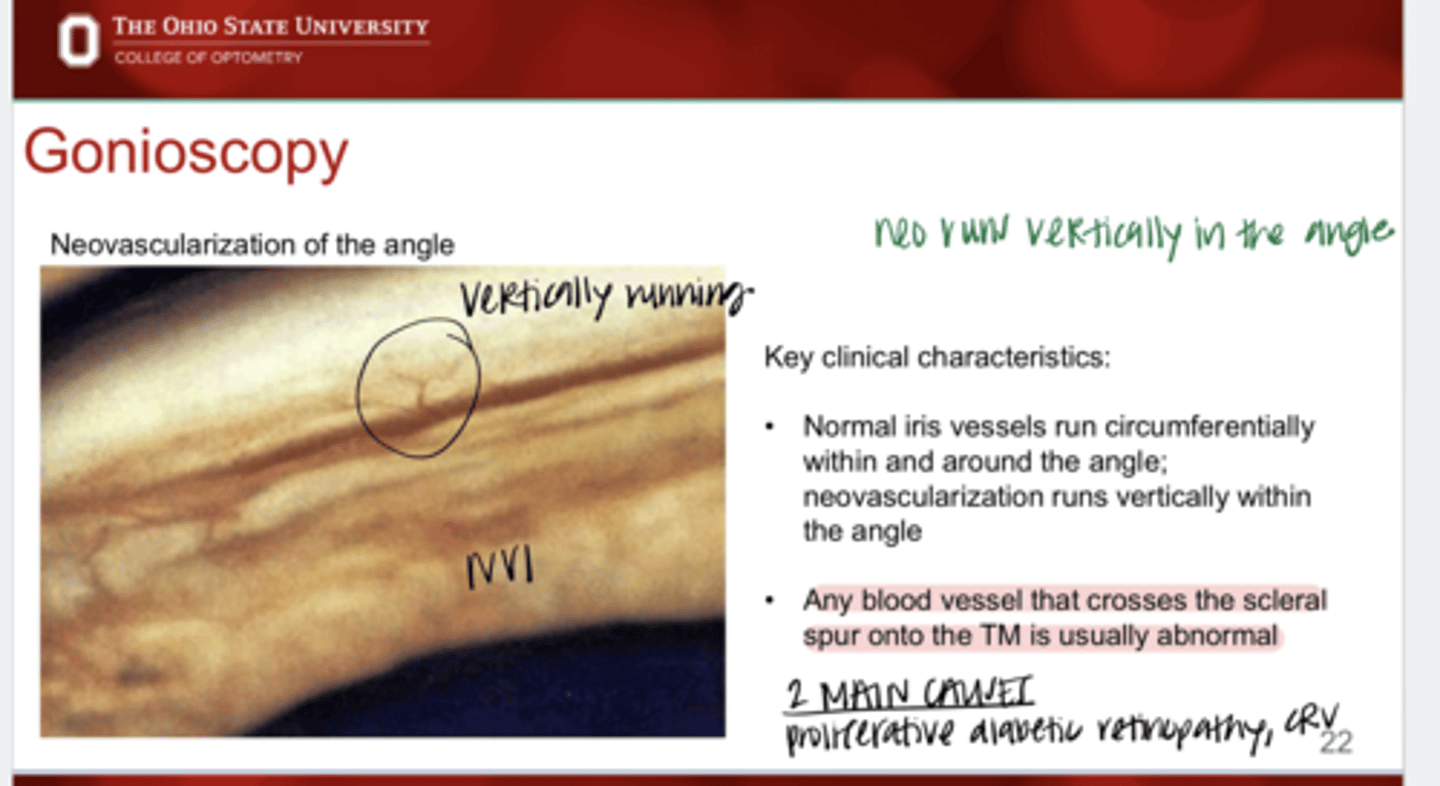
What are the 2 main causes of neovasc of the angle?
proliferative diabetic retinopathy and CRVO
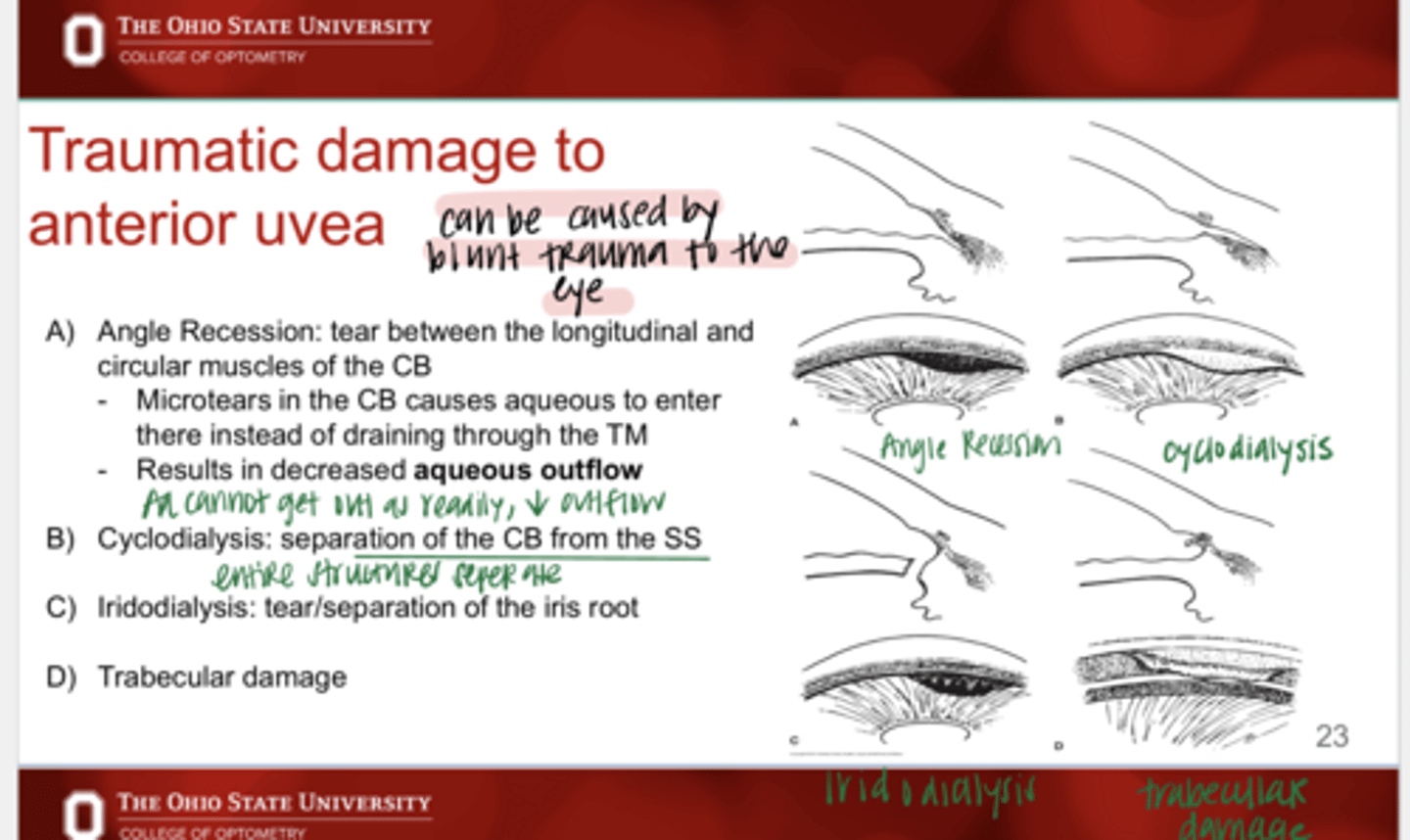
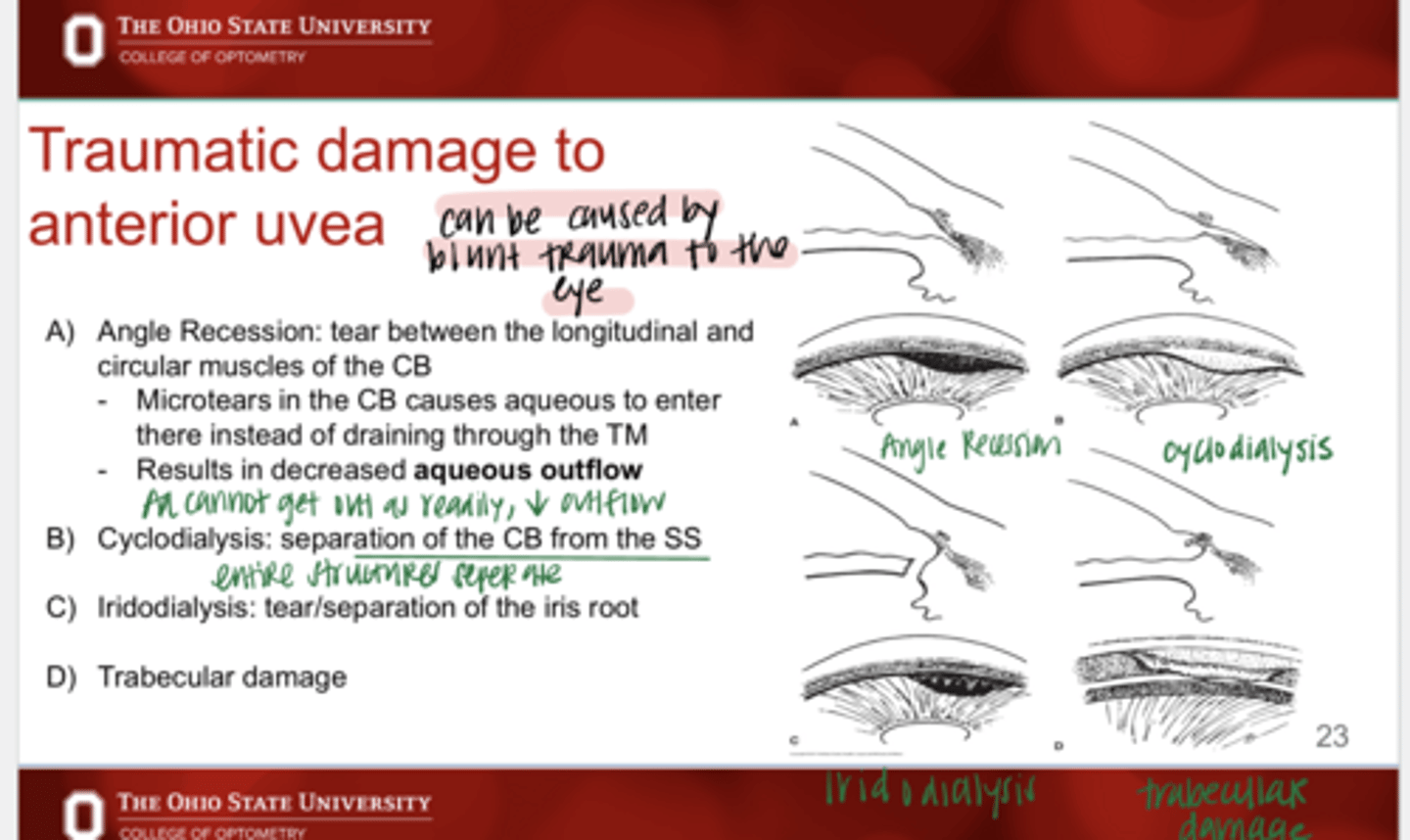
What are the 4 effects of traumatic damage to the anterior uvea?
1) Angle recession
2) Cyclodialysis
3) Iridodialysis
4) Trabecular damage
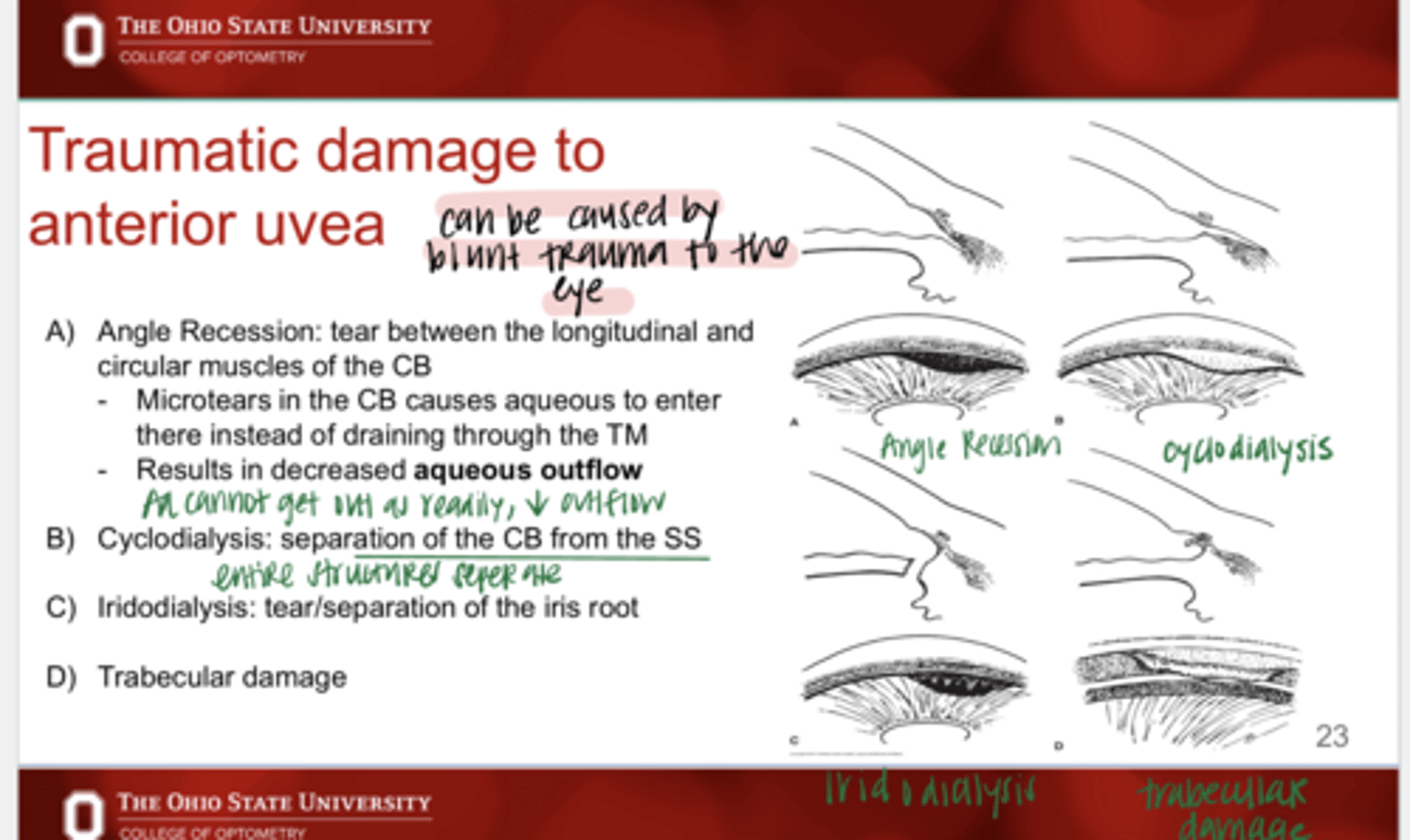
What is angle recession?
-tear between the longitudinal and circular muscles of the CB
-microtears in the CB causes aqueous to enter there instead of going through the TM
What does angle recession result in?
-microtears in the CB causes aqueous to enter there instead of going through the TM
-decreased aqueous outflow
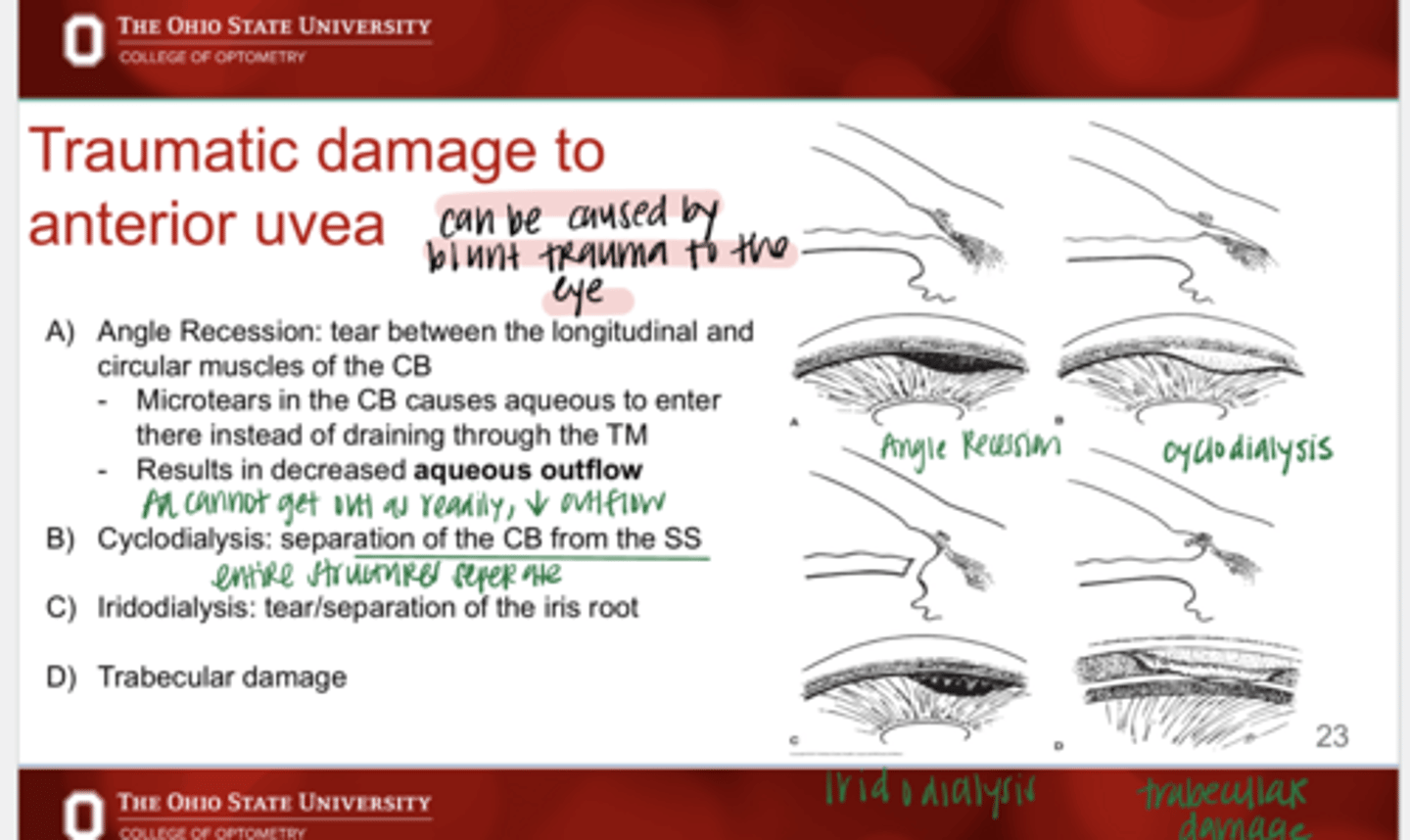
What is cyclodialysis?
separation of the CB from the SS
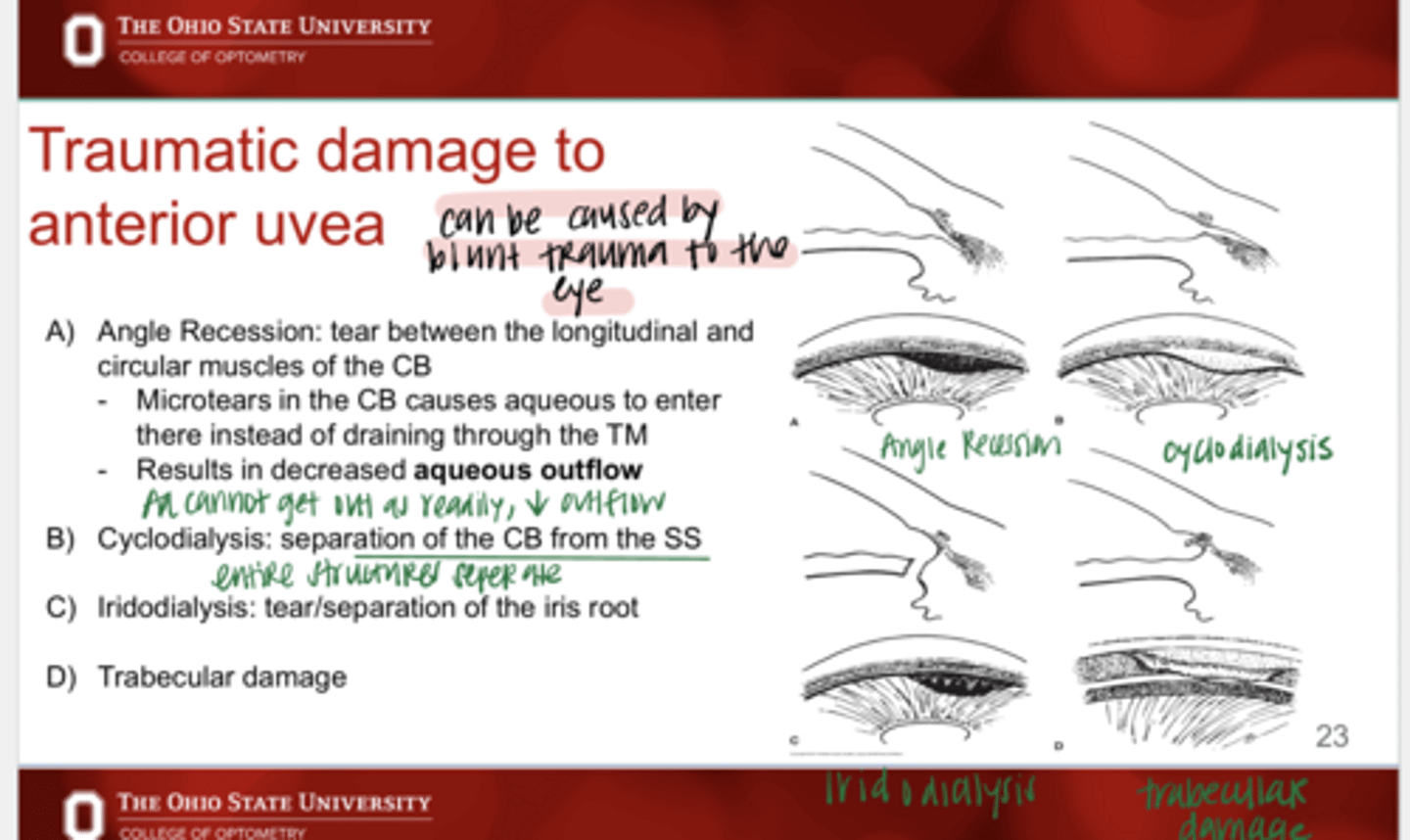
What is iridodialysis?
tear/separation of the iris root
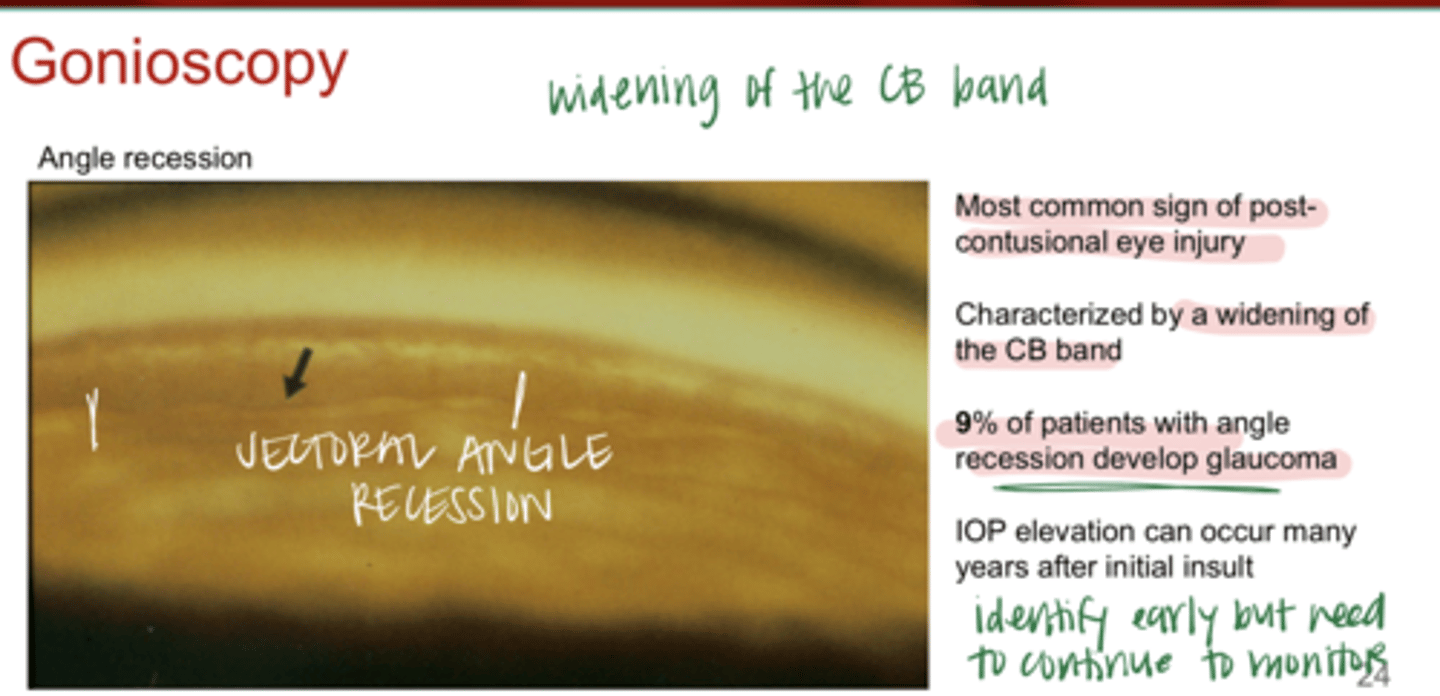
What is the MOST COMMON sign of post-contusional eye injury?
angle recession
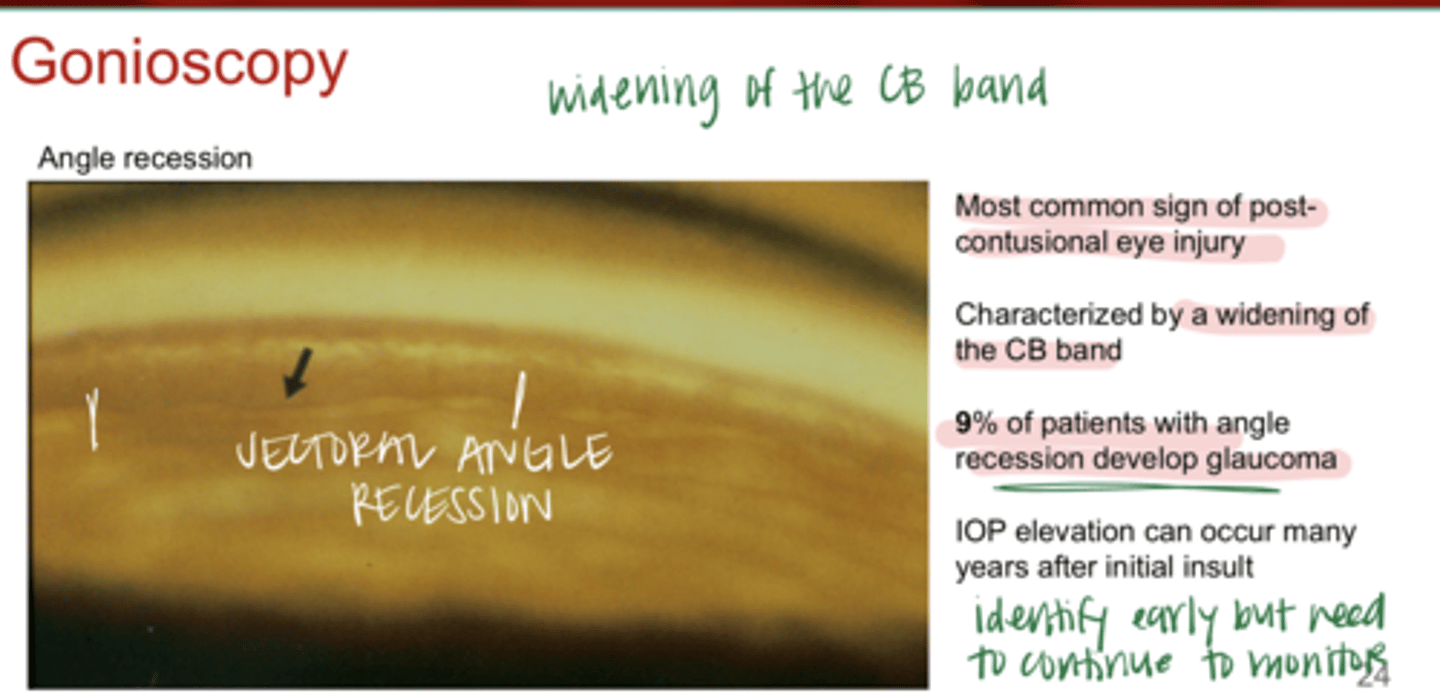
What is angle recession characterized by?
widening of the CB band
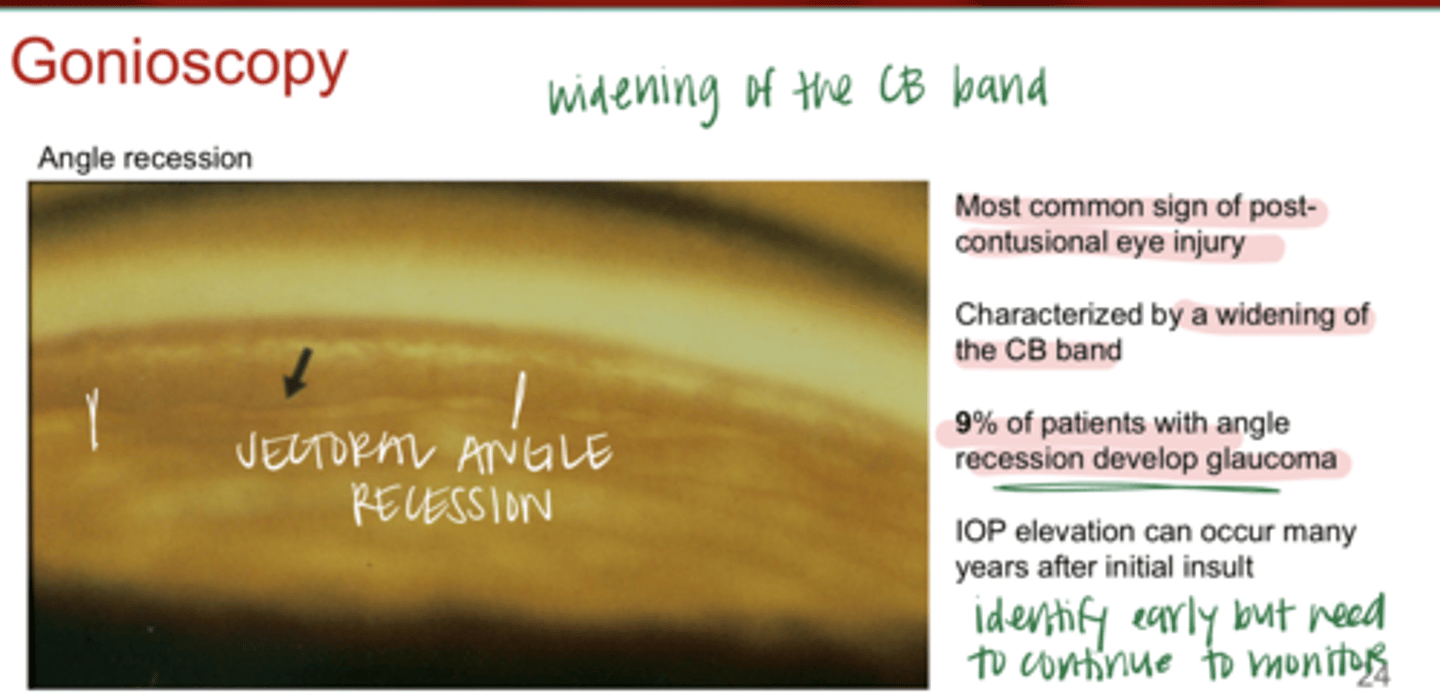
___% of patients with angle recession will develop glaucoma
9
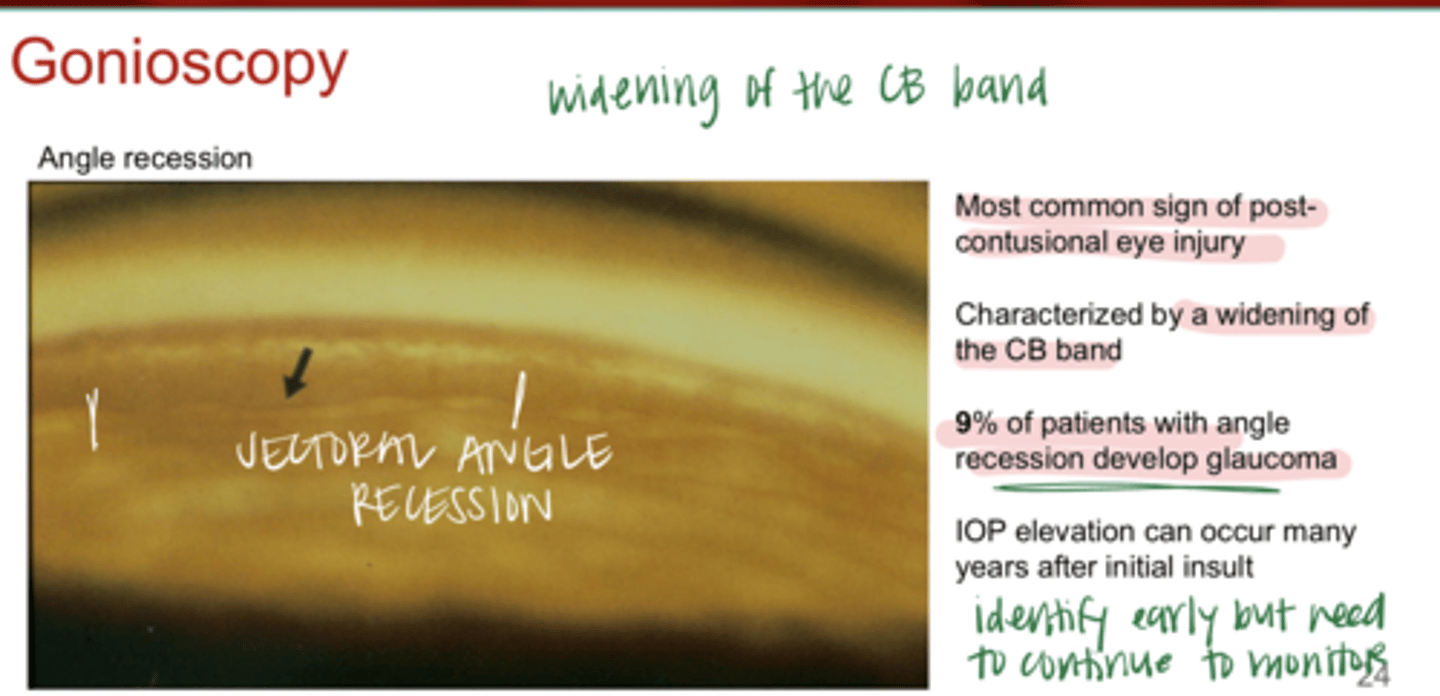
True or False:
IOP elevation can occur many years after the initial insult causing angle recession
true
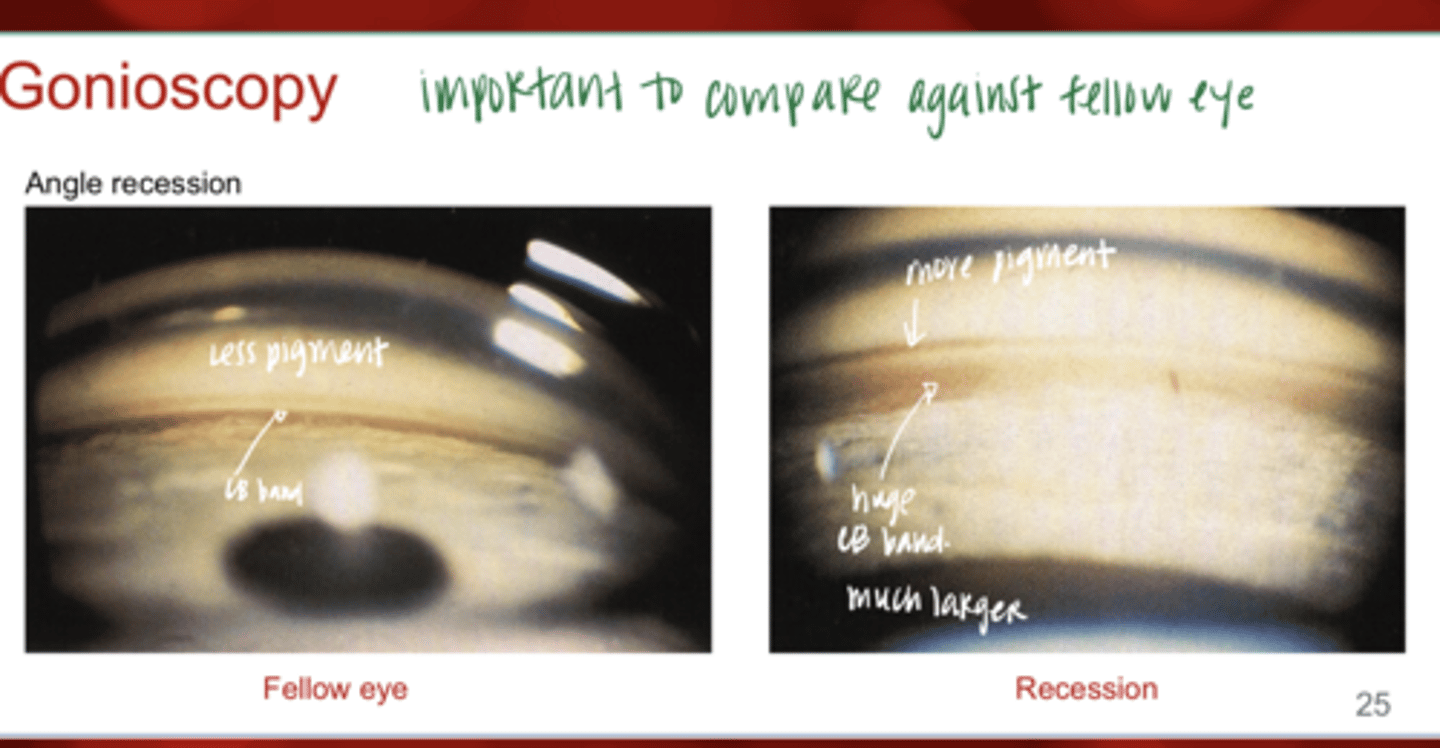
Angle Recession -- Important to Compare to Fellow Eye (Pic)
Angle Recession -- Important to Compare to Fellow Eye (Pic)
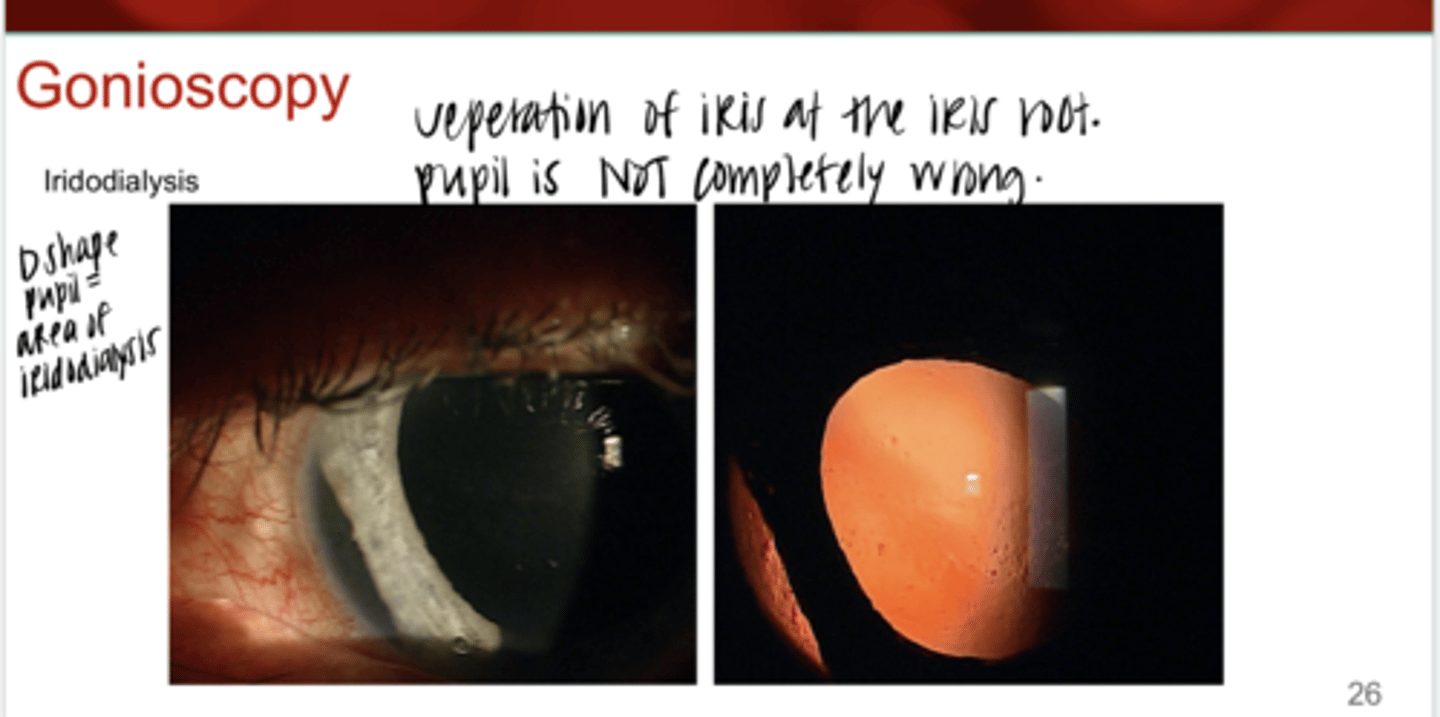
Iridodialysis -- Separation of the Iris at the Iris Root (Pic)
Iridodialysis -- Separation of the Iris at the Iris Root (Pic)
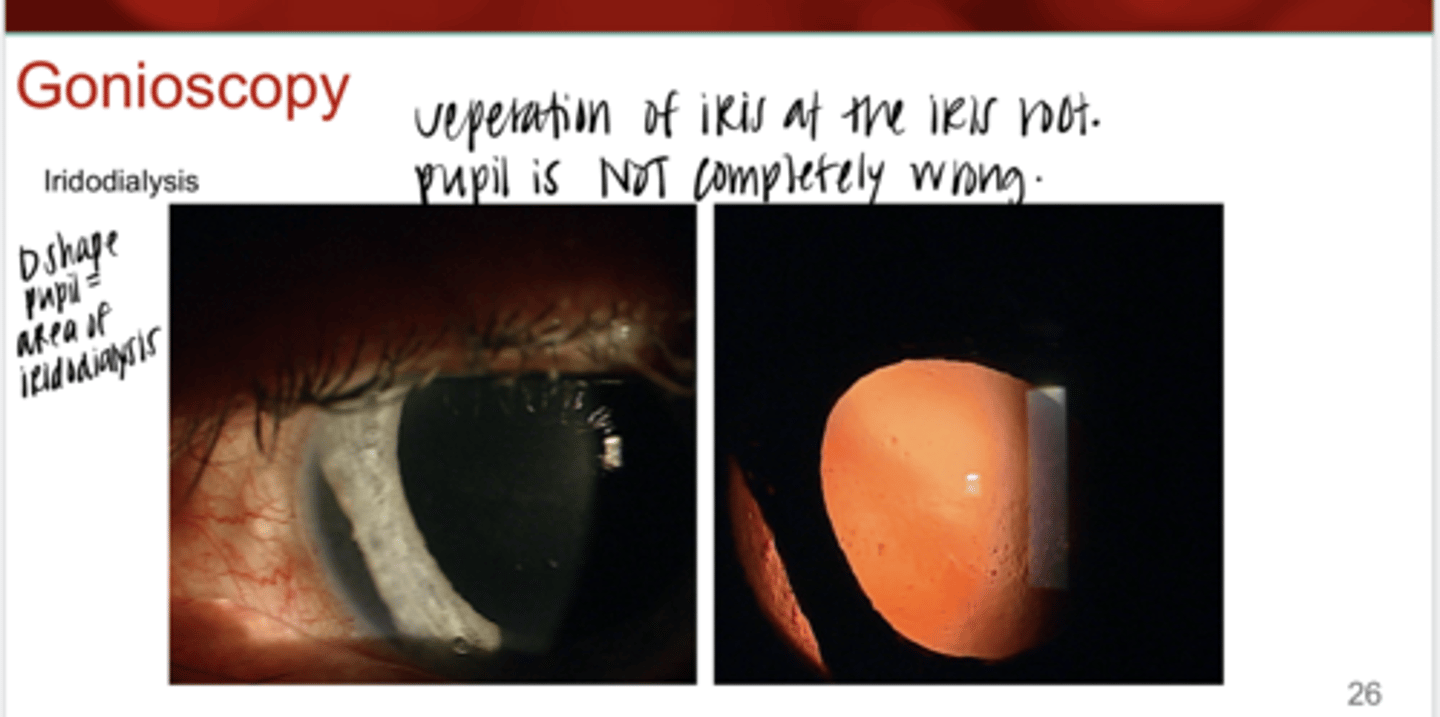
Iridodialysis will result in a ____ shaped pupil
D
True or False:
All instances of angle obstruction will result in damage to the optic nerve
false
Most forms of angle closure glaucoma are ____ and _____
chronic; incomplete
Angle obstruction is usually ____ and/or _____
sectoral and/or intermittent
Are the symptoms of angle closure glaucoma common?
No symptoms are rare -- usually no pain
Pain (symptoms) of angle closure are usually with ____ episodes of angle closure
acute
What are the stages of angle closure?
1) Primary angle closure suspect
2) Primary angle closure
3) Primary angle closure glaucoma
4) Acute angle closure
5) Plateau iris configuration
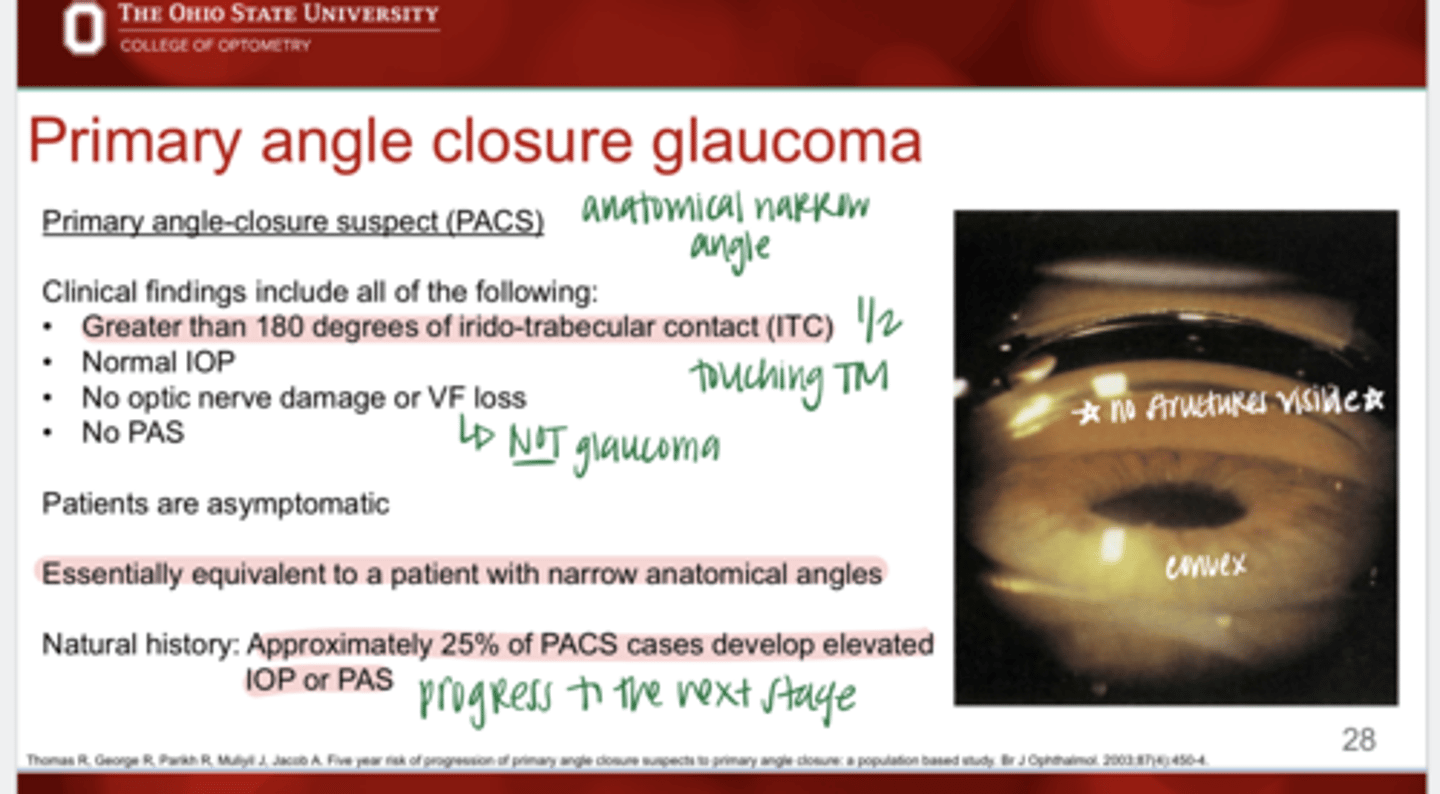
Clinical findings in a patient that is a Primary angle closure suspect?
-Greater than 180º of ITC
-Normal IOP
-NO PAS
-No optic nerve damage or VF loss
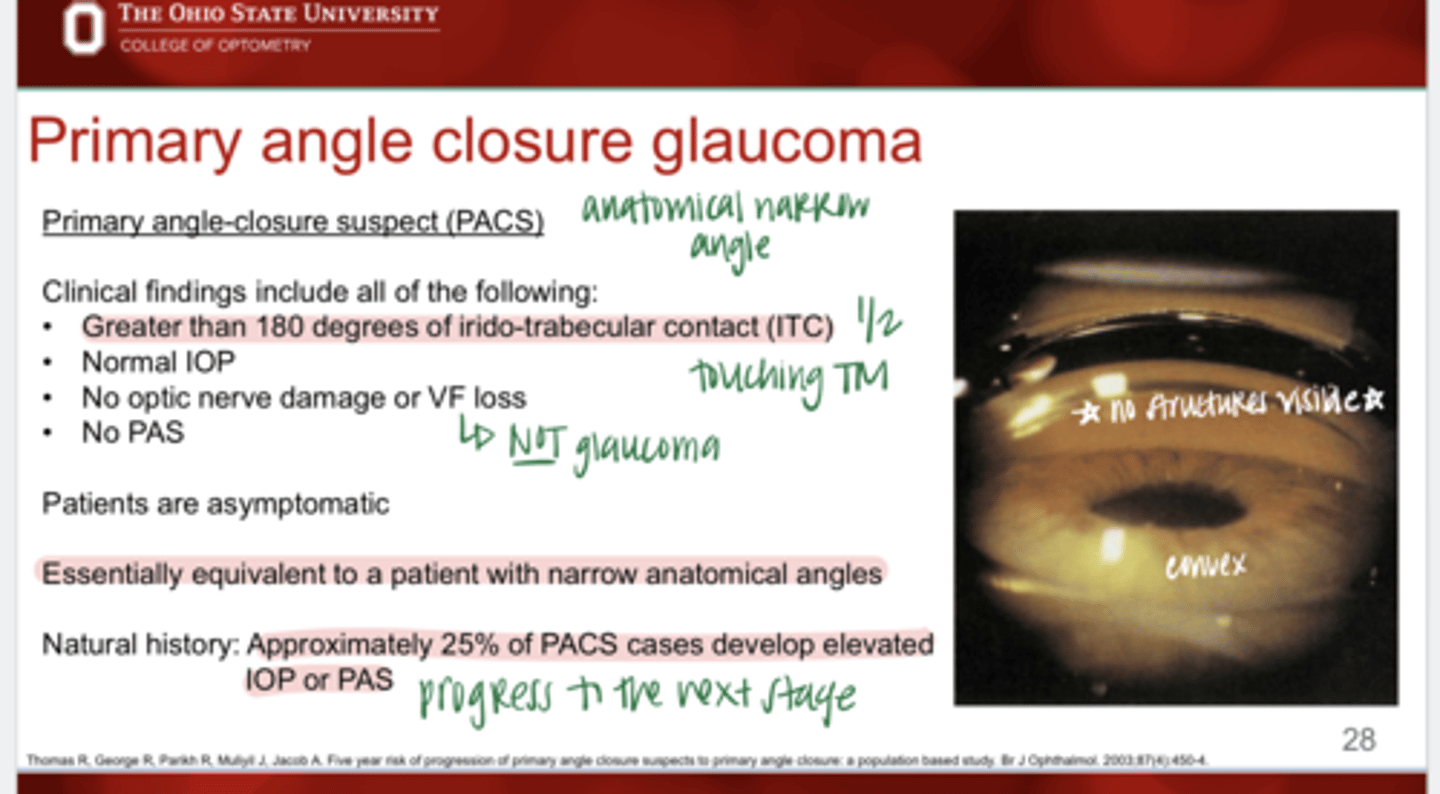
Primary angle closure suspects are (symptomatic/asymptomatic)?
asymptomatic
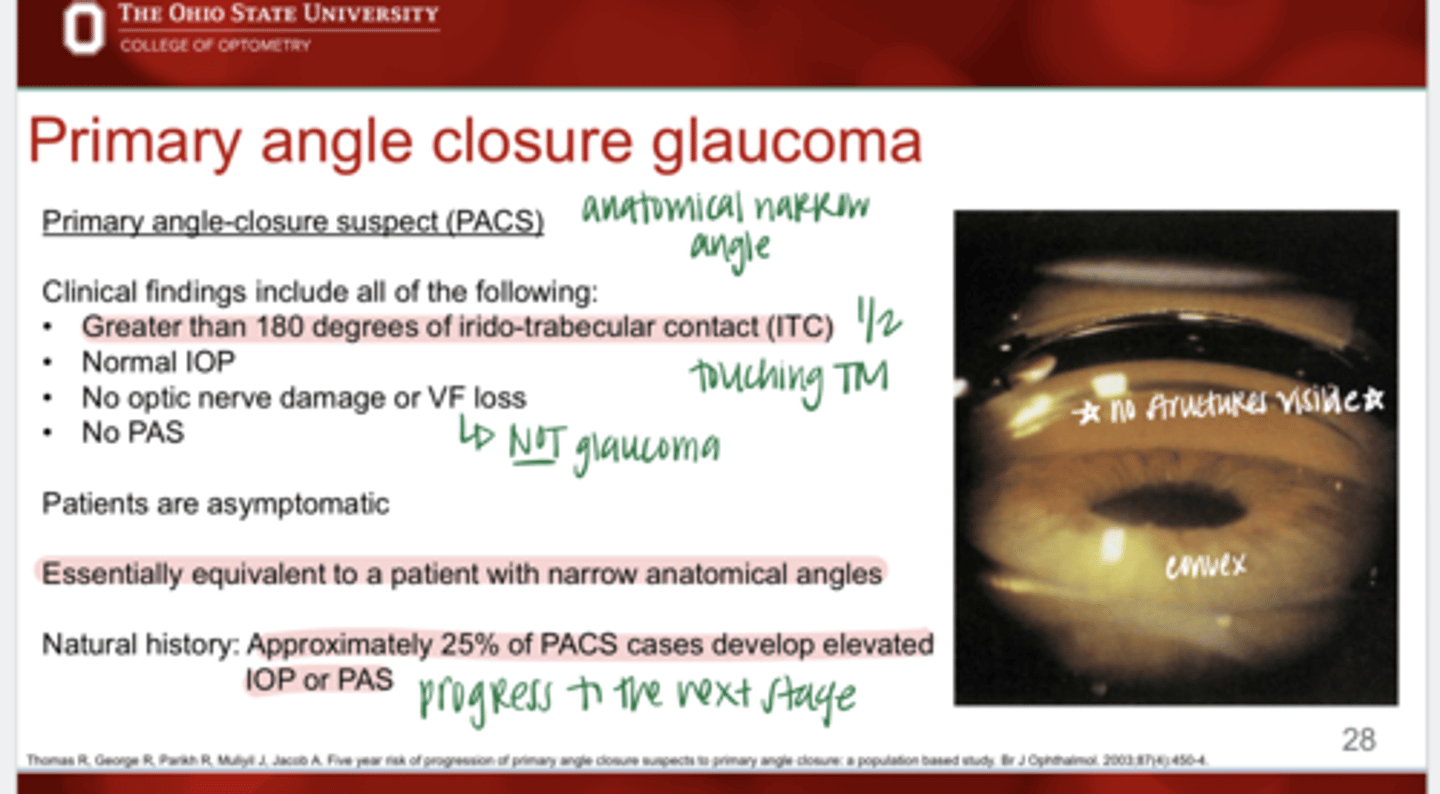
Primary angle closure suspects are essentially equivalent to a patient with ________
narrow anatomical angles
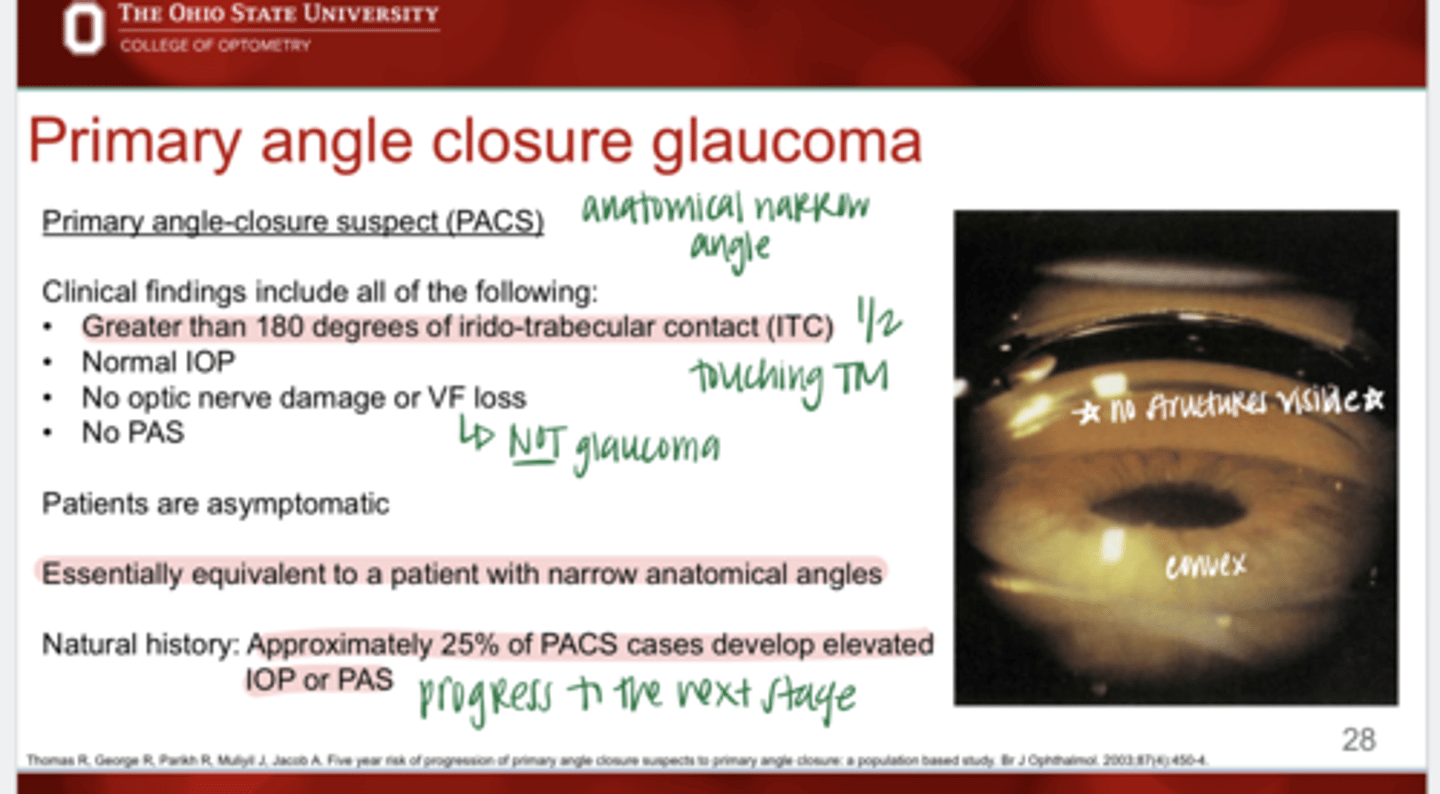
Approx ____% of Primary angle closure suspects will develop elevated IOP or PAS and progress to the next stage
25
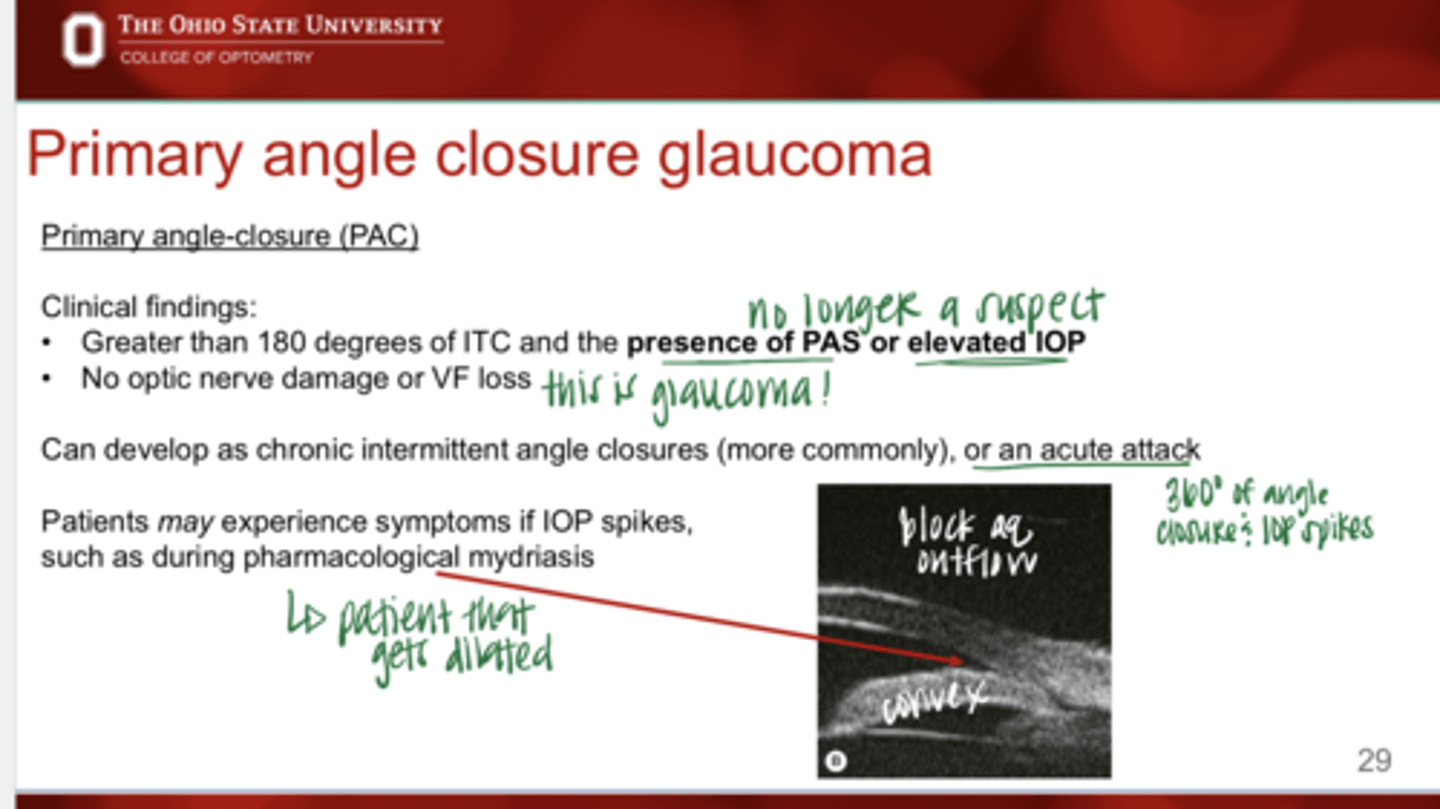
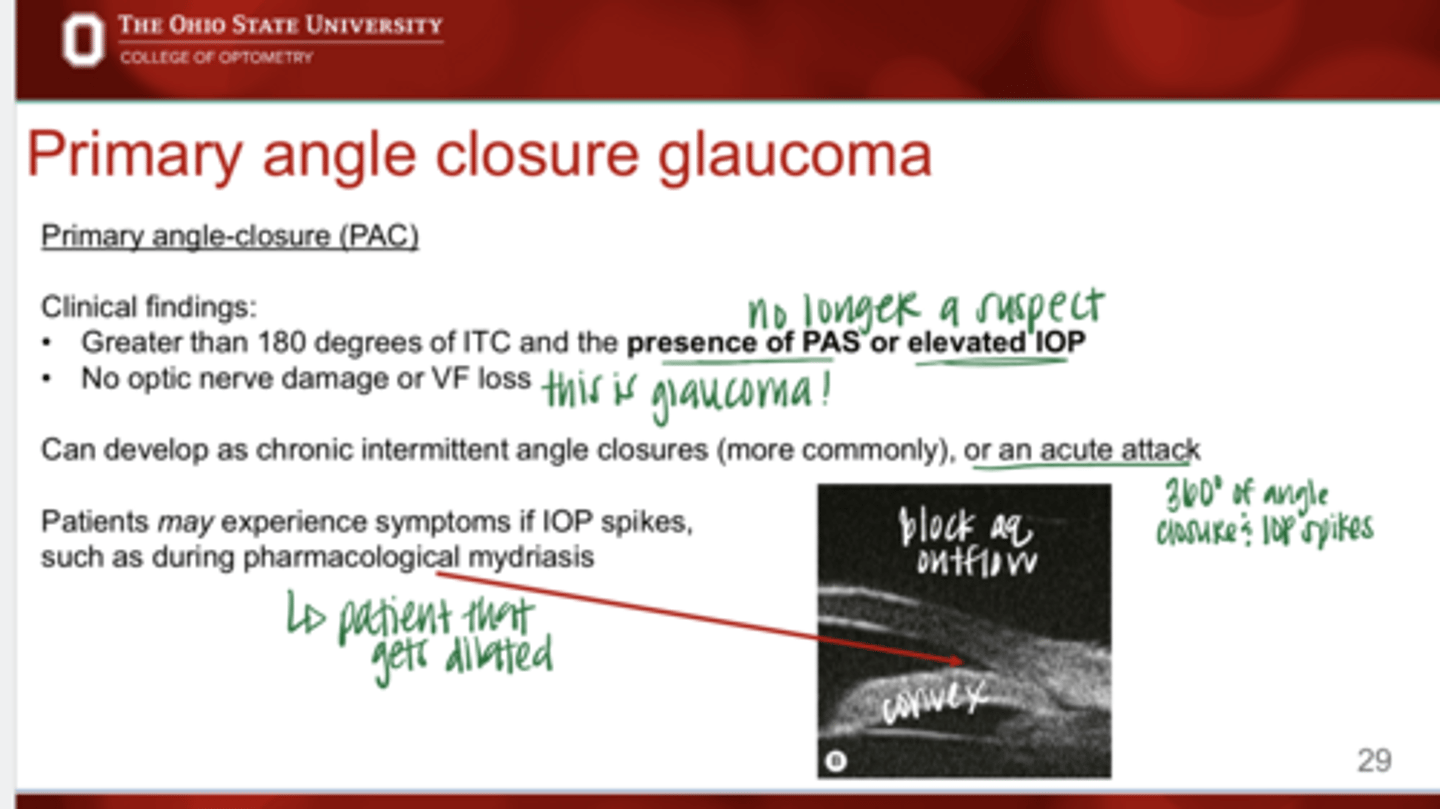
Clinical findings in a patient that is a Primary angle closure?
-greater than 180º of ITC
-presence of PAS or elevated IOP
-No optic nerve damage or VF loss
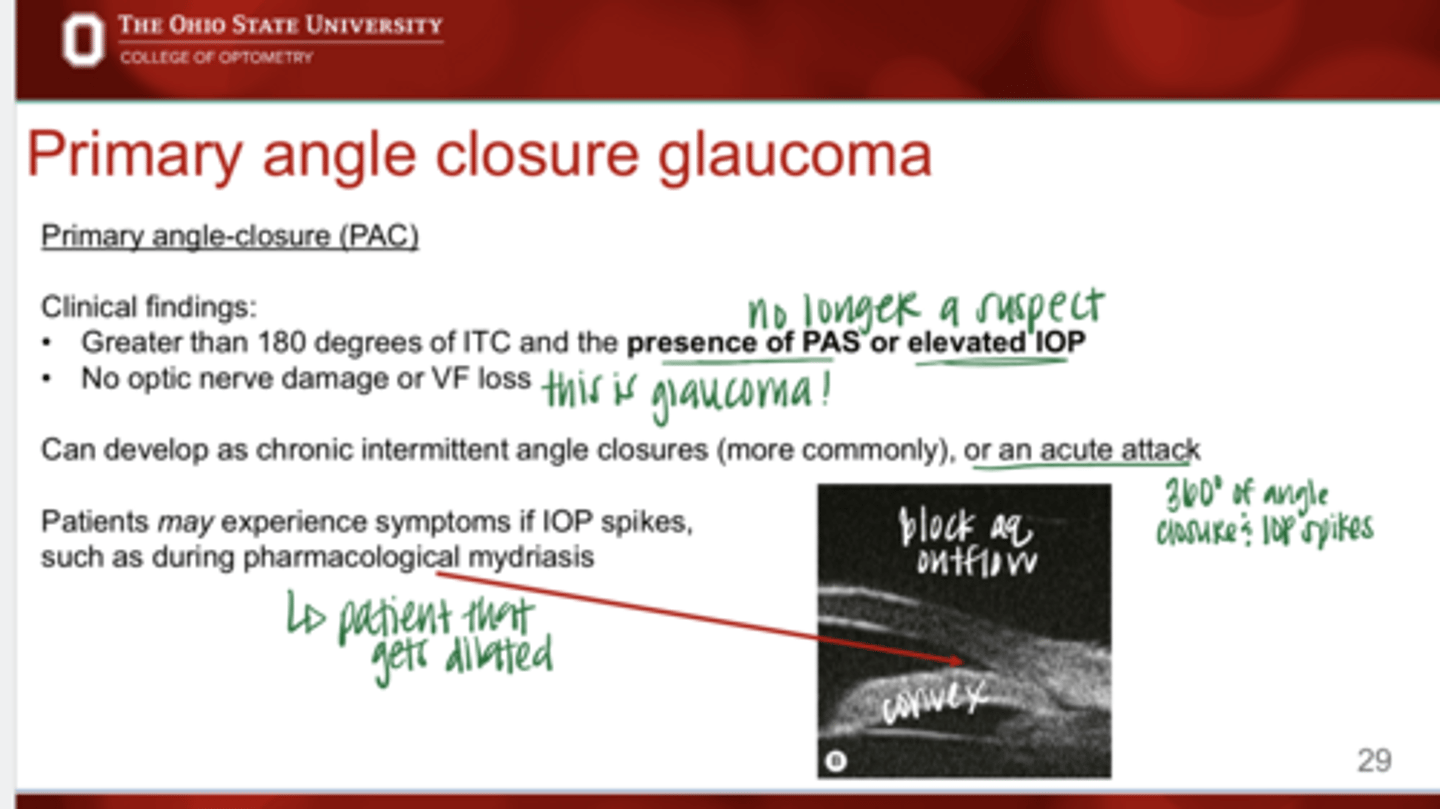
Can primary angle closure develop as chronic intermittent angle closure or as acute attacks?
Yes
Which is more common?
chronic intermittent angle closure or as acute attacks
chronic intermittent angle closures
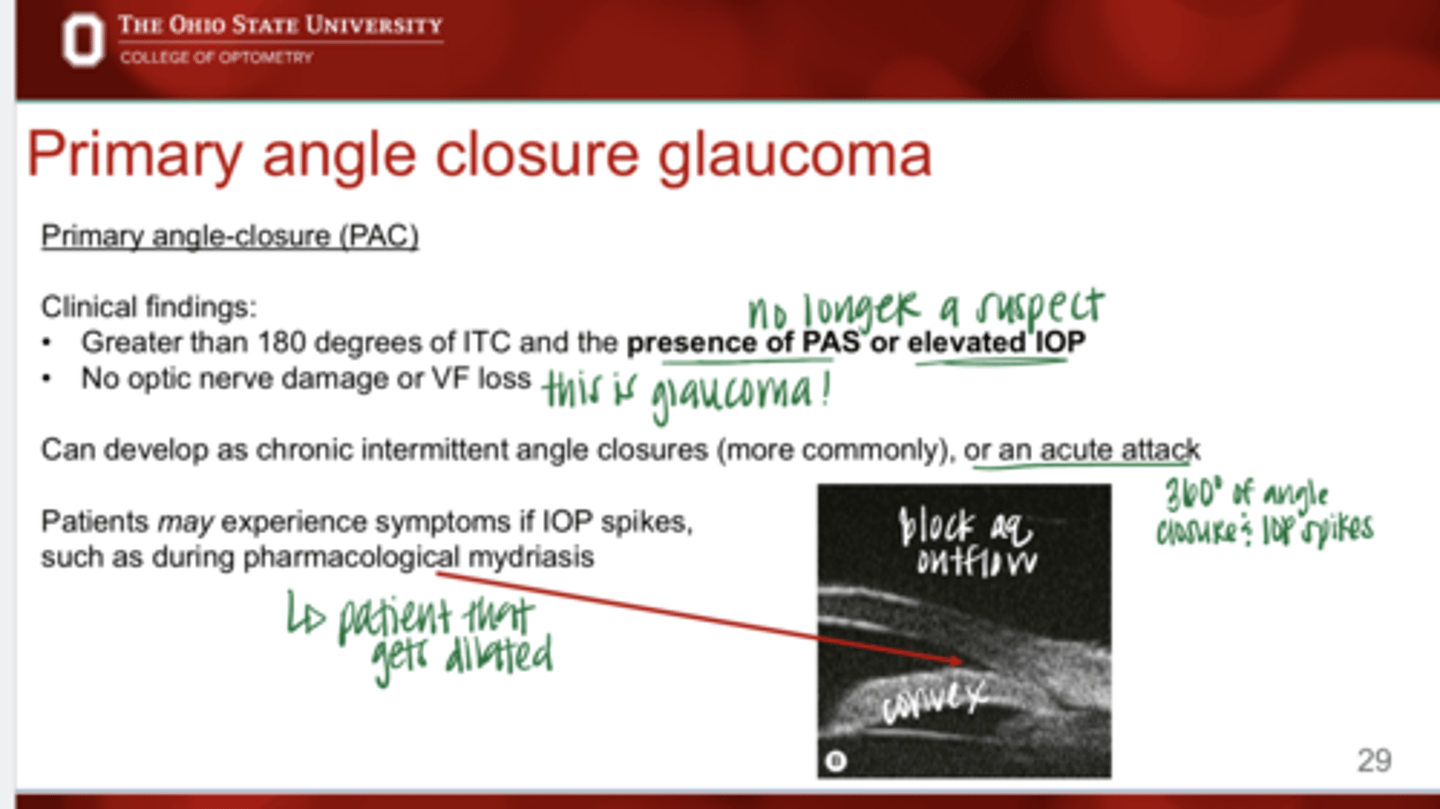
Can patients experience symptoms with primary angle closure?
Maybe -- if IOP spikes such as during pharmacological mydriasis (dilation)
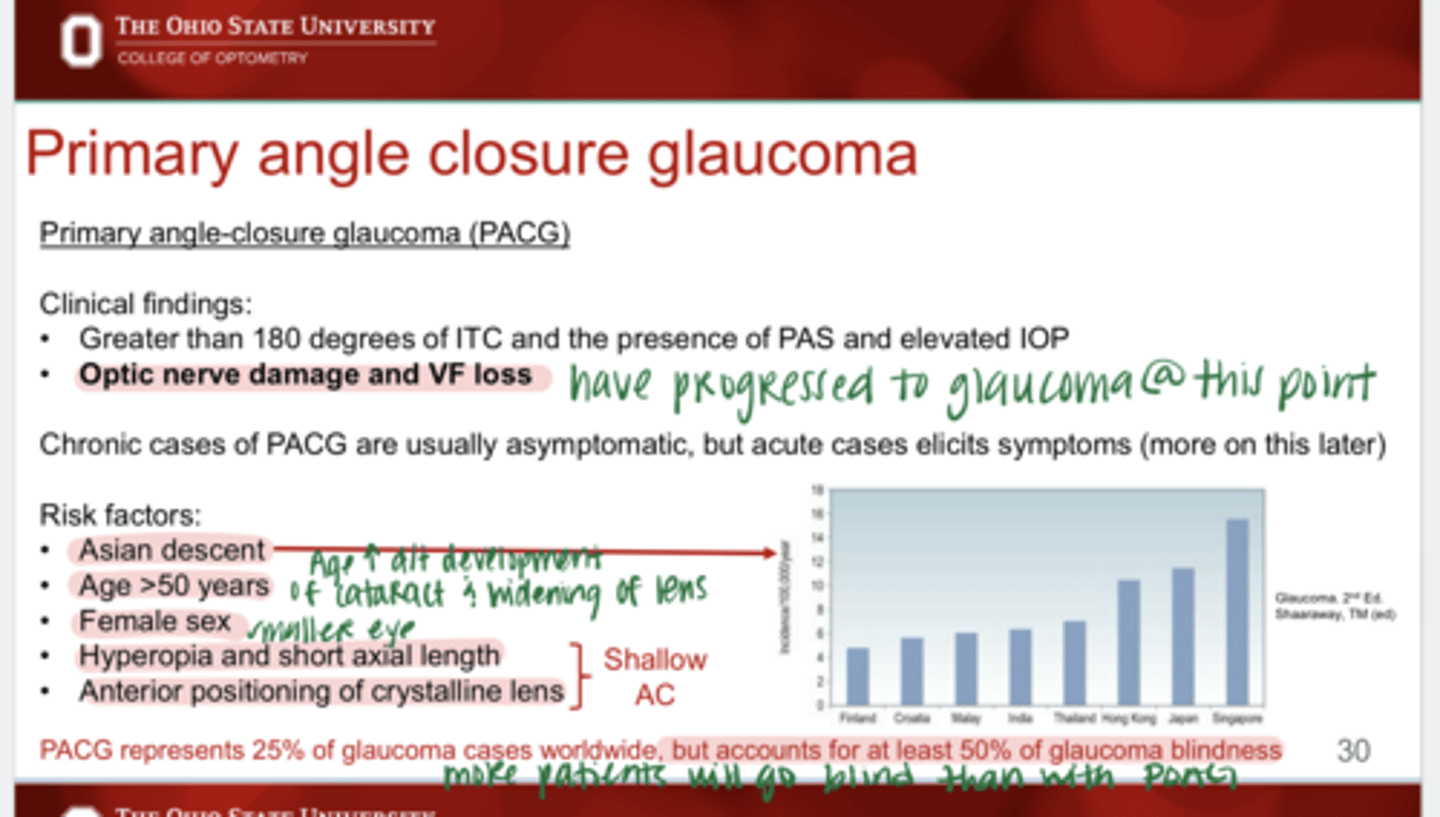
What are the clinical findings of primary angle closure glaucoma?
-greater than 180º of ITC
-presence of PAS or elevated IOP
-optic nerve damage or VF loss
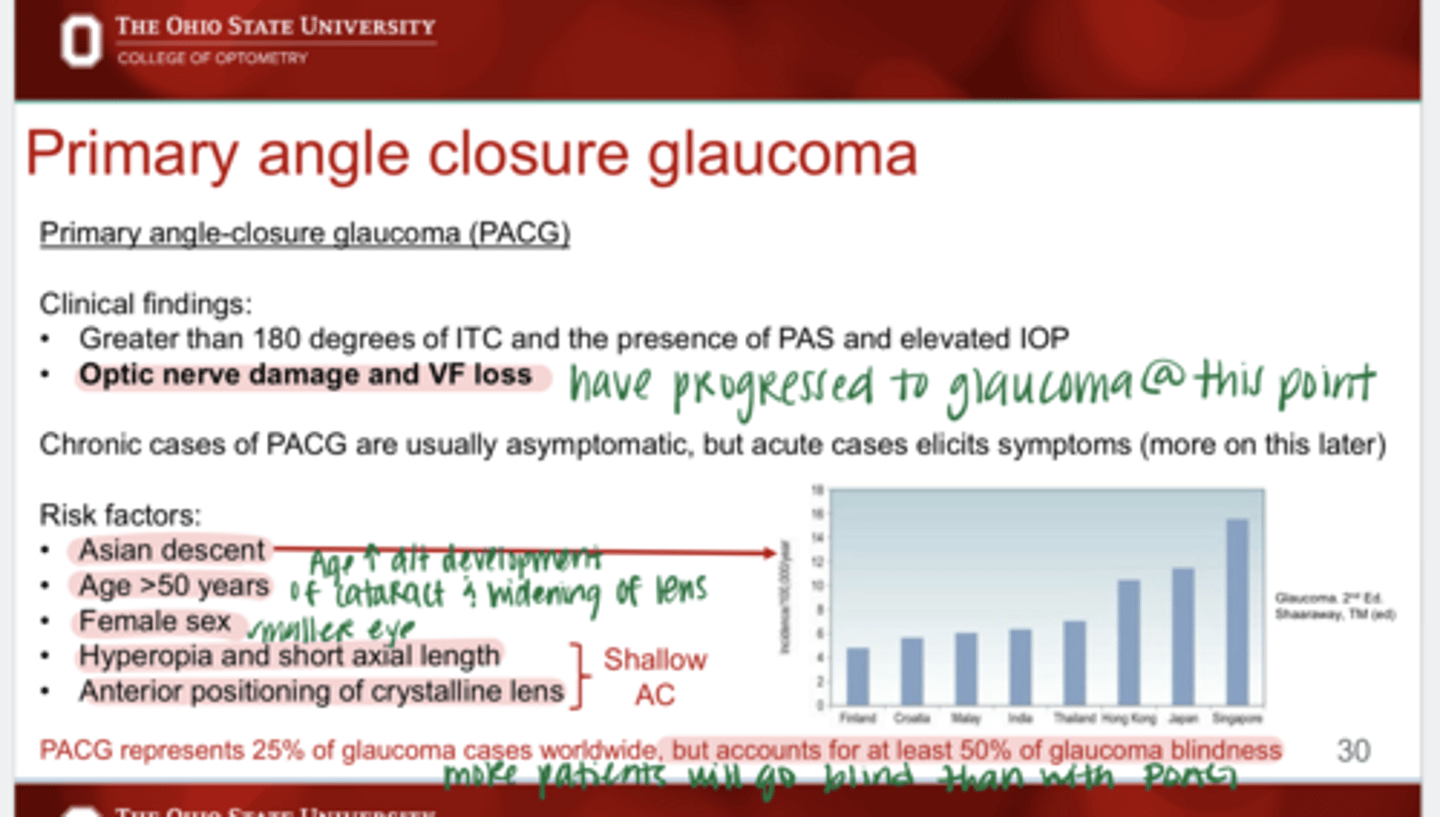
Chronic causes of PACG are usually ______
asymptomatic
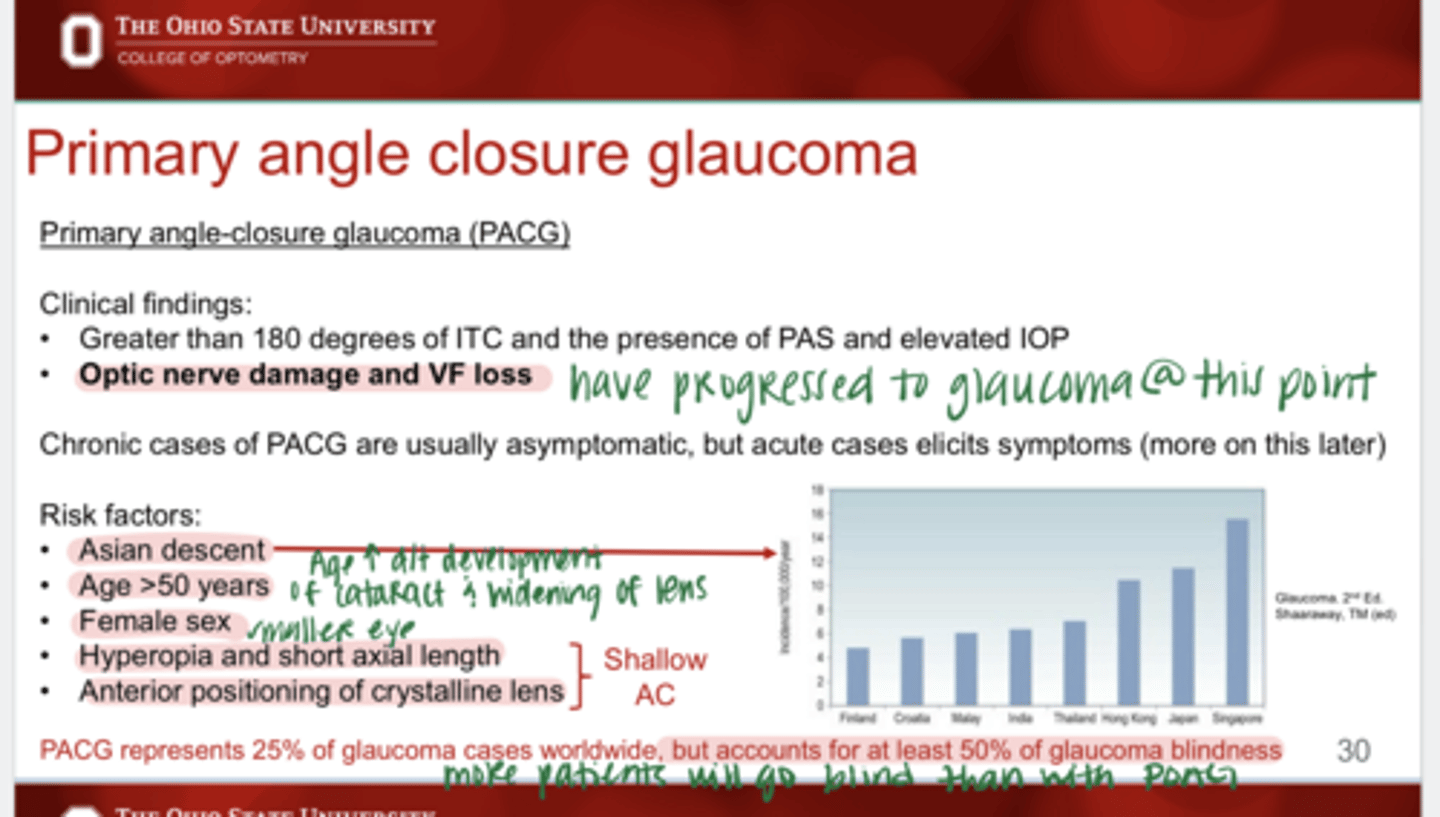
Acute cases of PACG elicit ______
symptoms
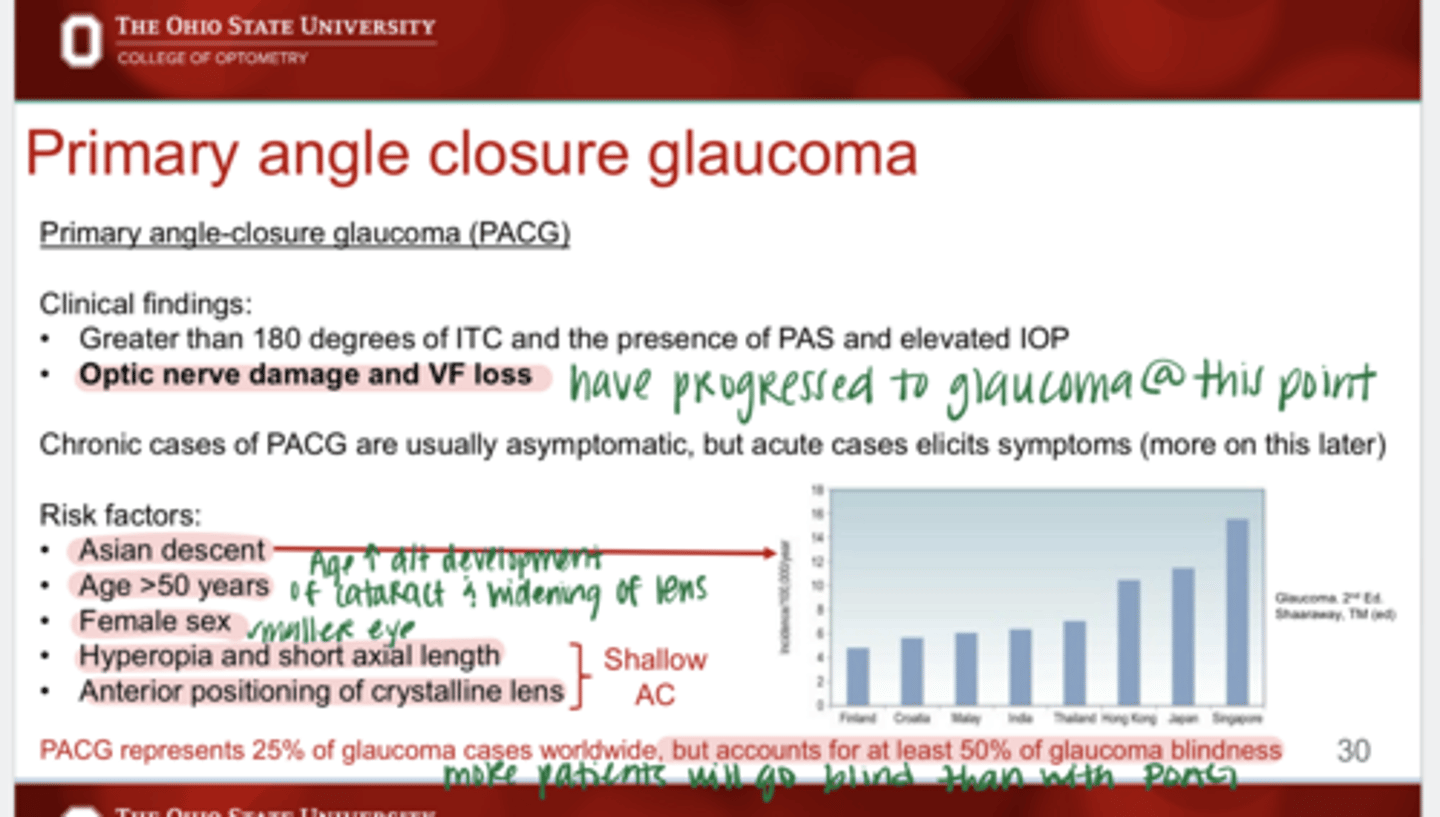
What are the risk factors for PACG?
-Asian descent
-Age >50
-Female > male
-Hyperopia
-Short axial length
-Anterior positioning of crystalline lens
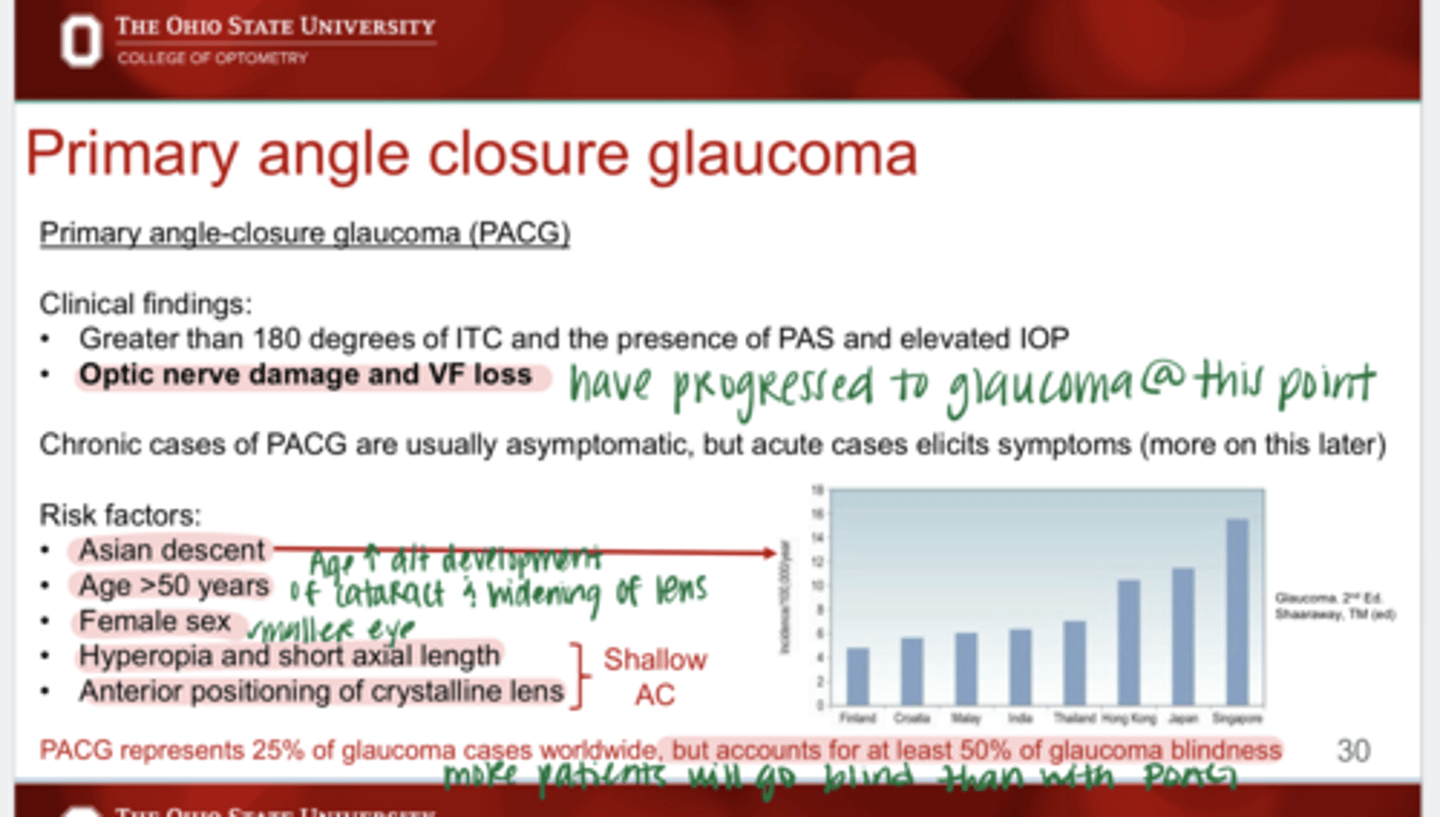
PACG represents ____% of glaucoma cases worldwide
25 -- less than POAG
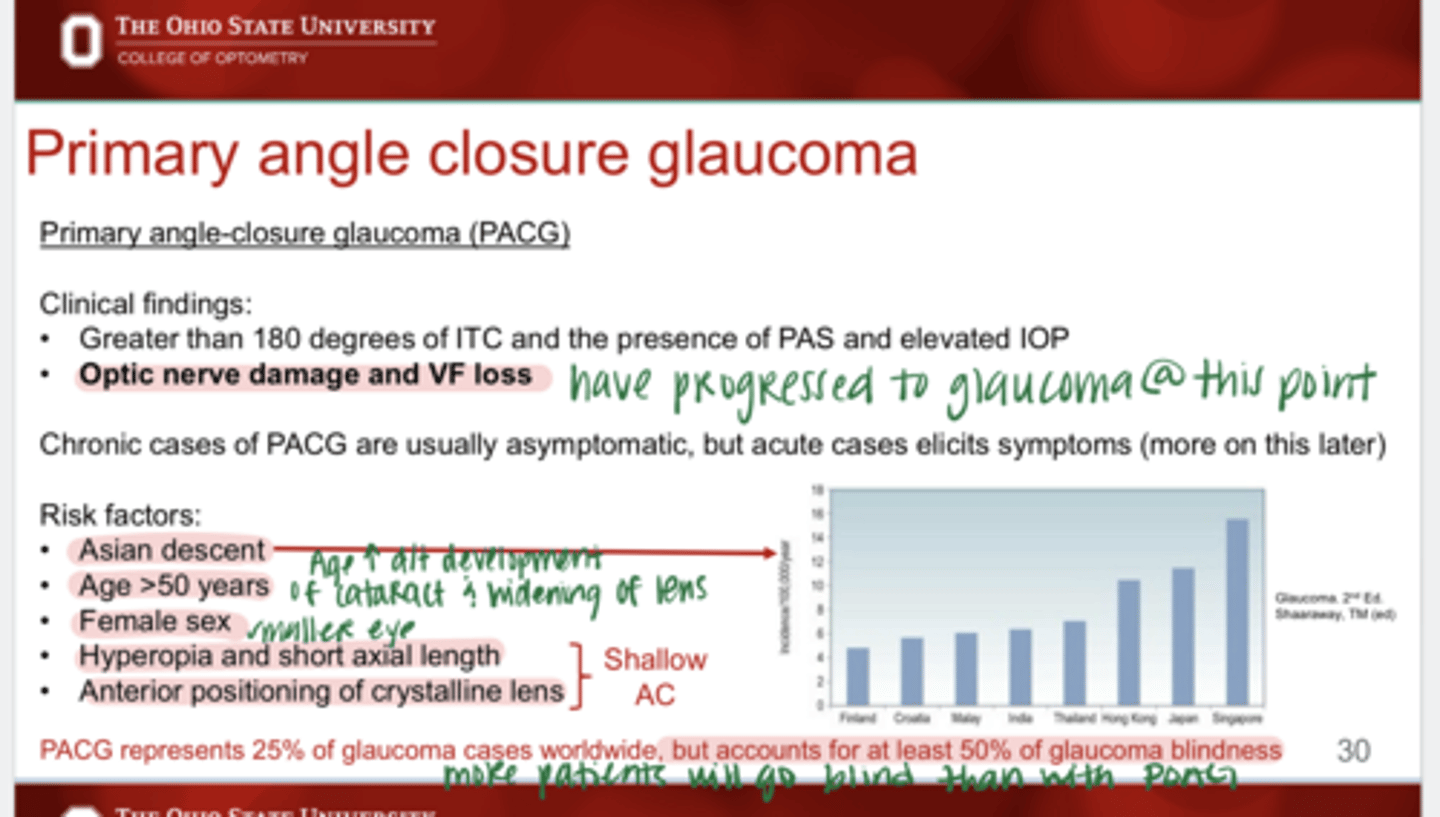
PACG accounts for ____% of glaucoma blindness
50 -- more than POAG
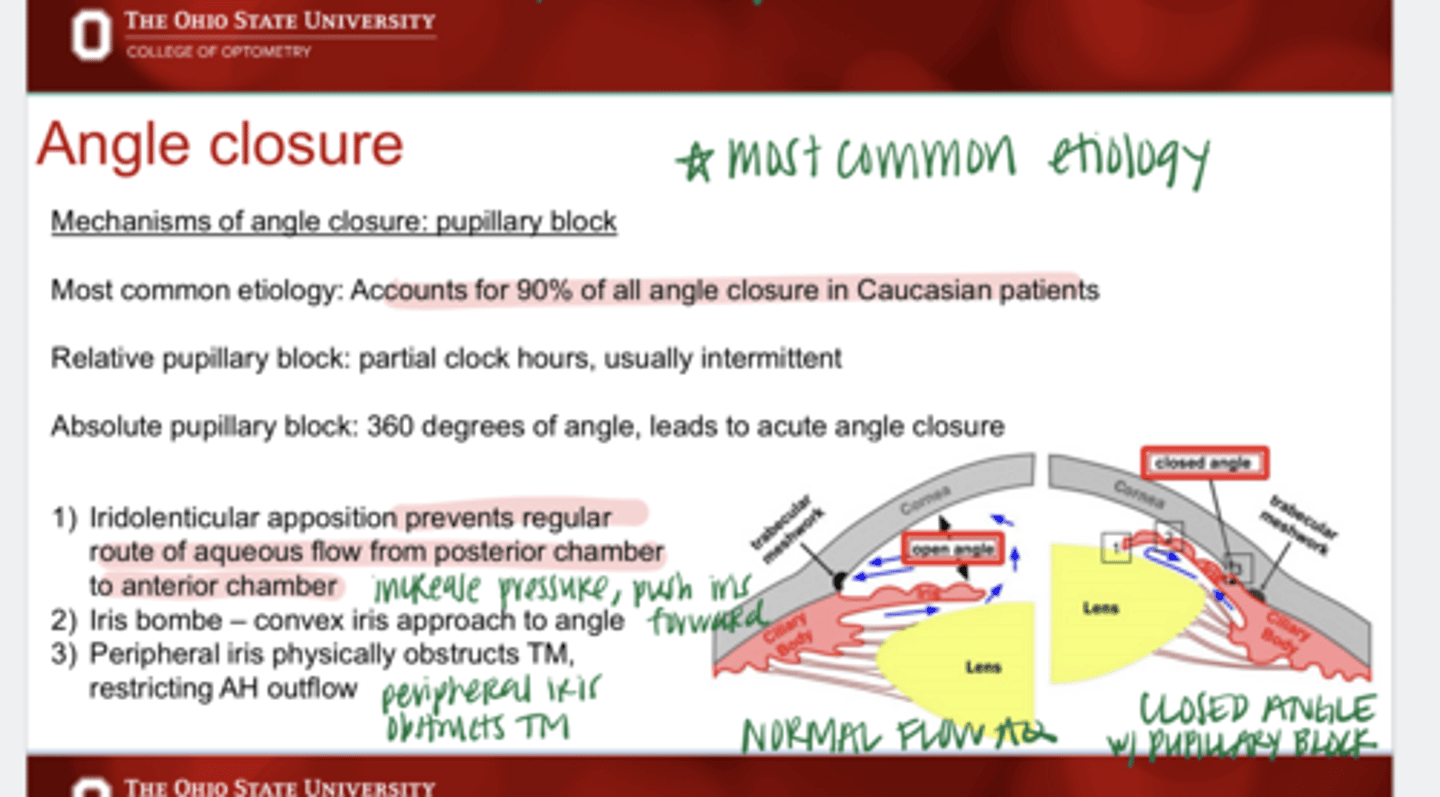
Pupillary block accounts for ____% of angle closure in Caucasian patients
90
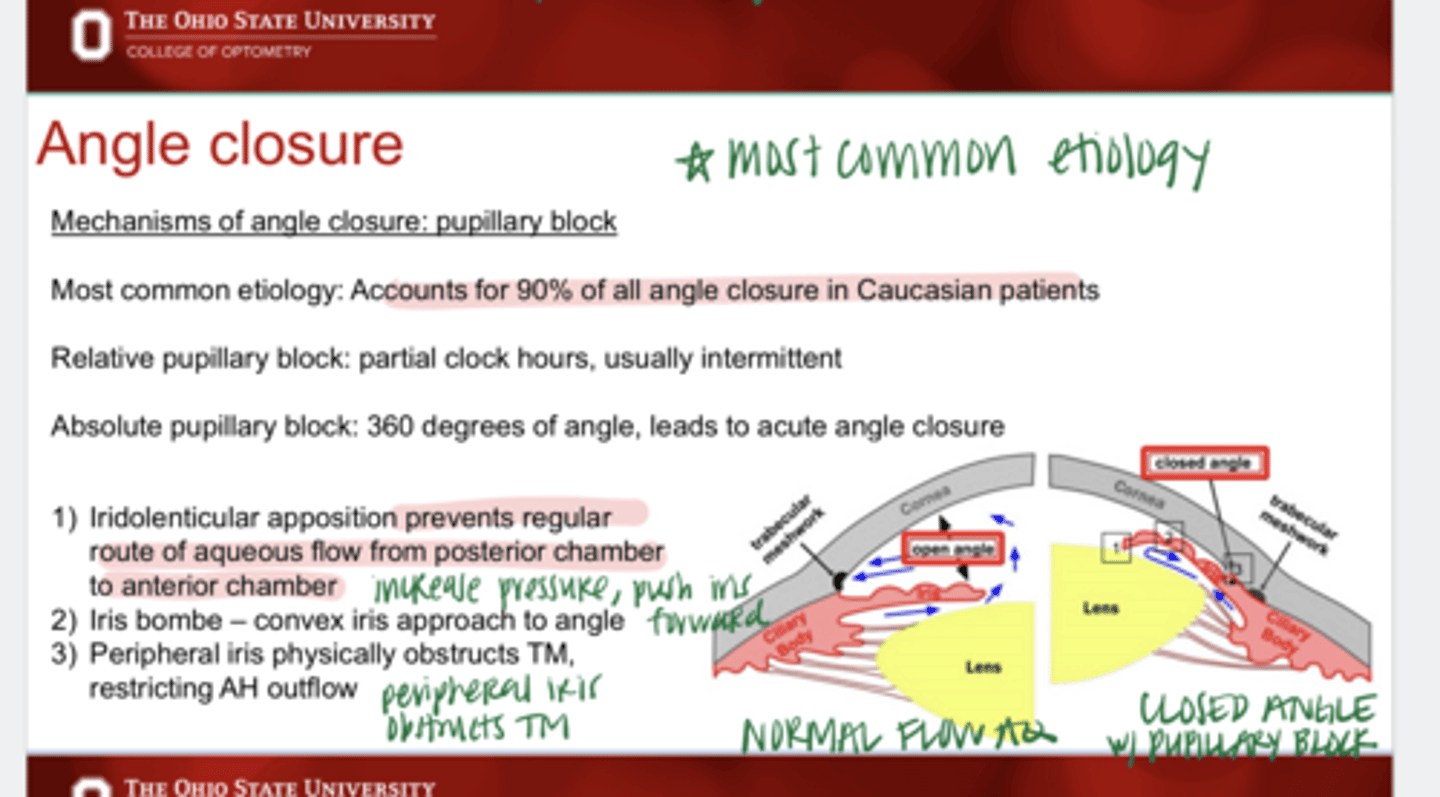
What is the most common etiology of angle closure in Caucasian patients?
pupillary block
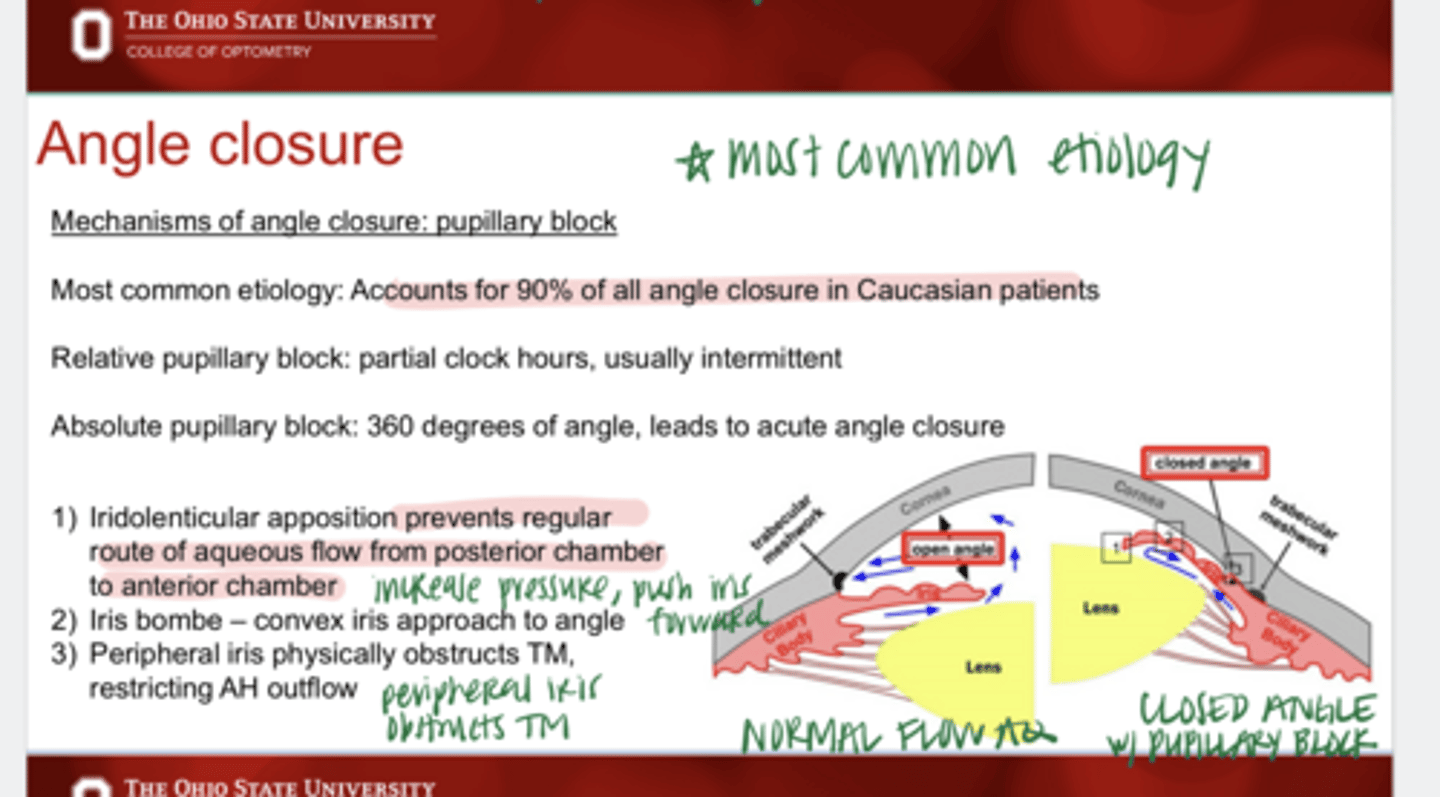
What is a relative pupillary block?
partial clock hours, usually intermittent
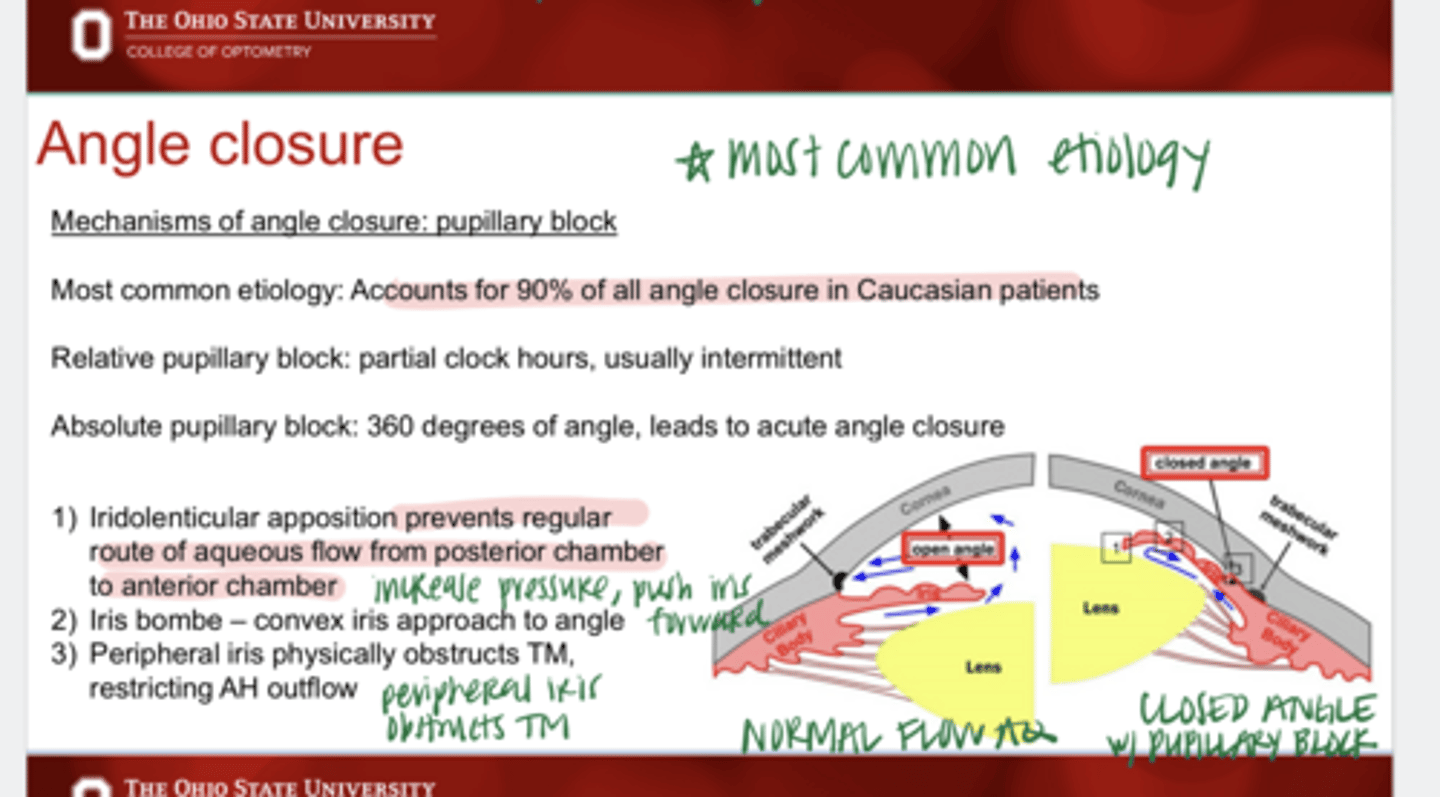
What is an absolute pupillary block?
360 degrees of block, leads to acute angle closure
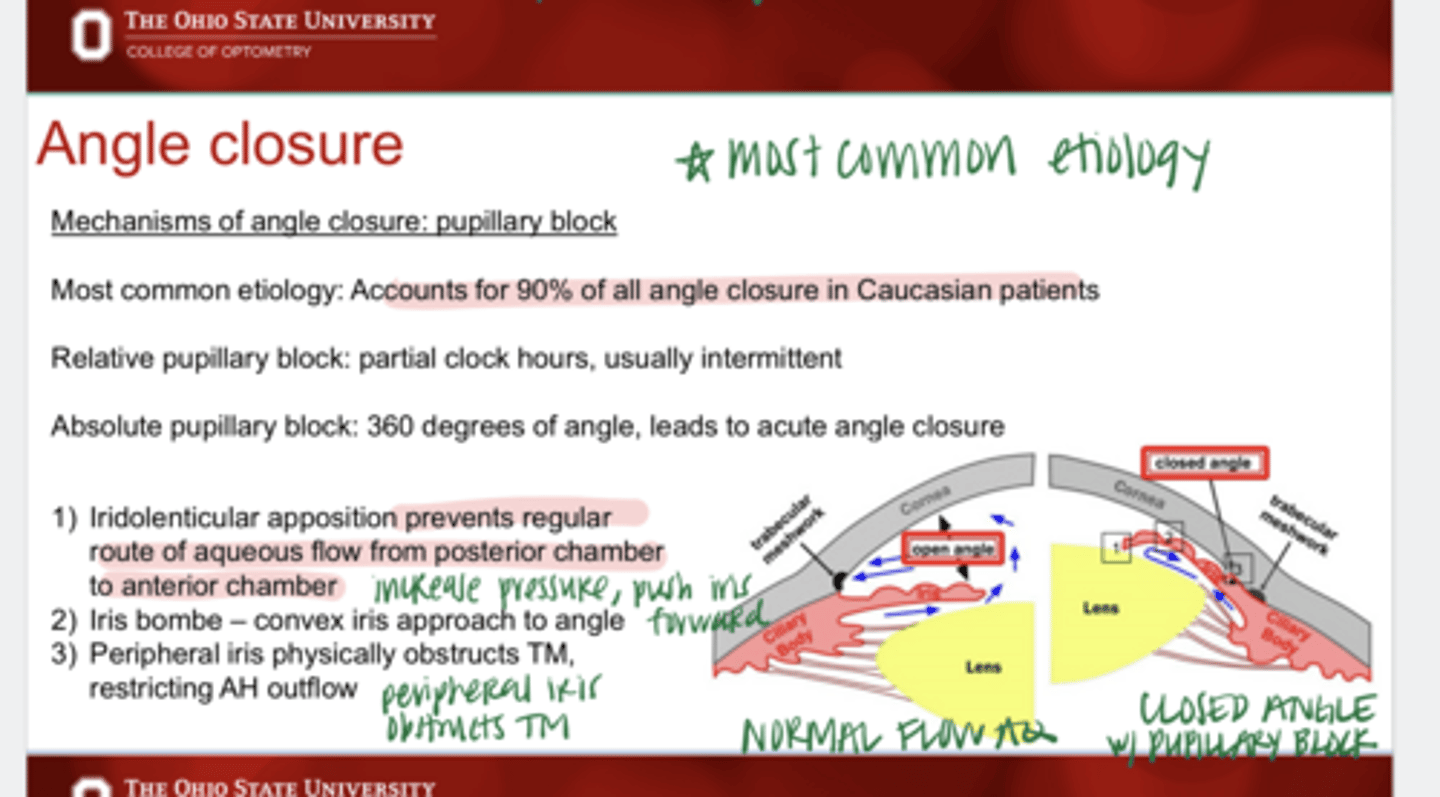
What is the pathophys of pupillary block?
1) Iridolenticular apposition prevents regular route of aq. flow from the posterior chamber to the anterior chamber
2) Iris bombe -- convex iris approach to angle
3) Peripheral iris physically obstructs TM, restricting AH outflow

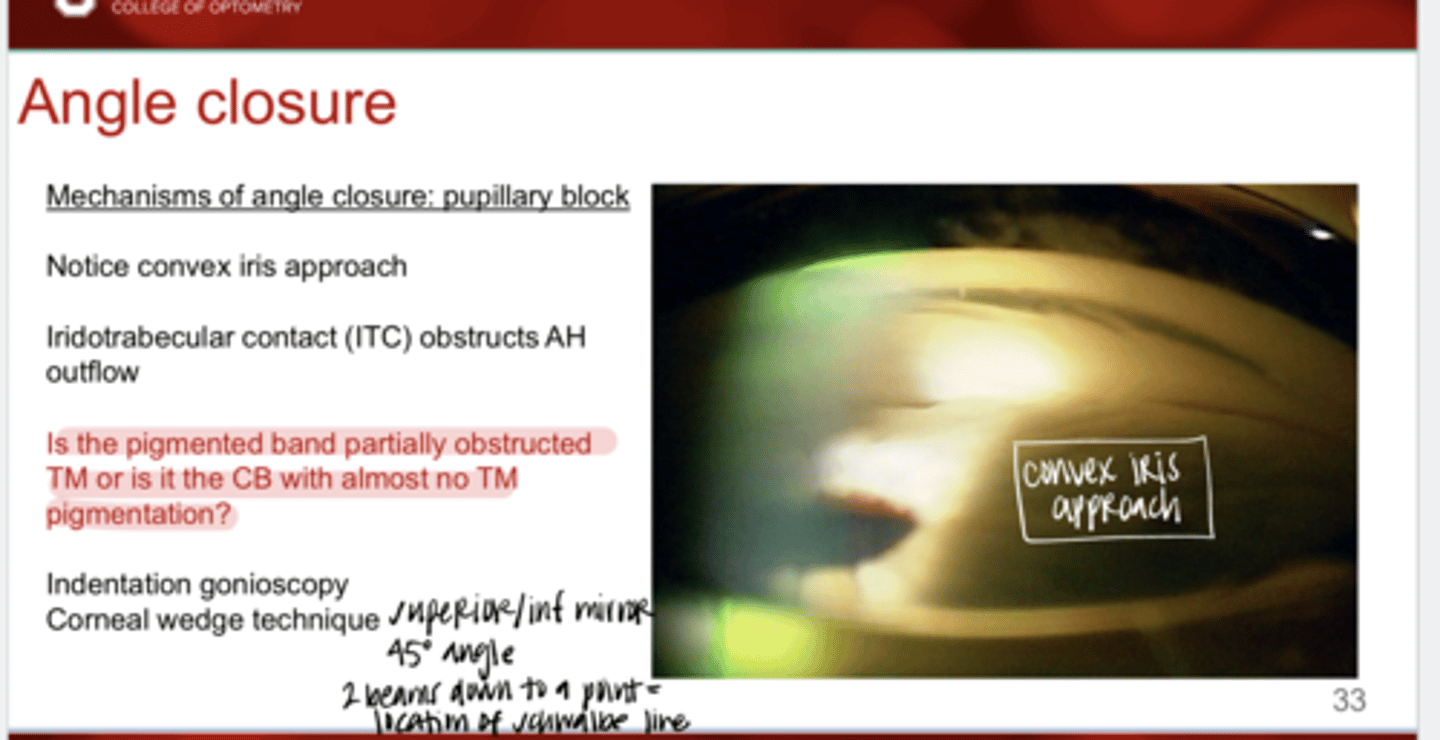
Iris Bombe -- Convex Iris Approach (Pic)
Iris Bombe -- Convex Iris Approach (Pic)
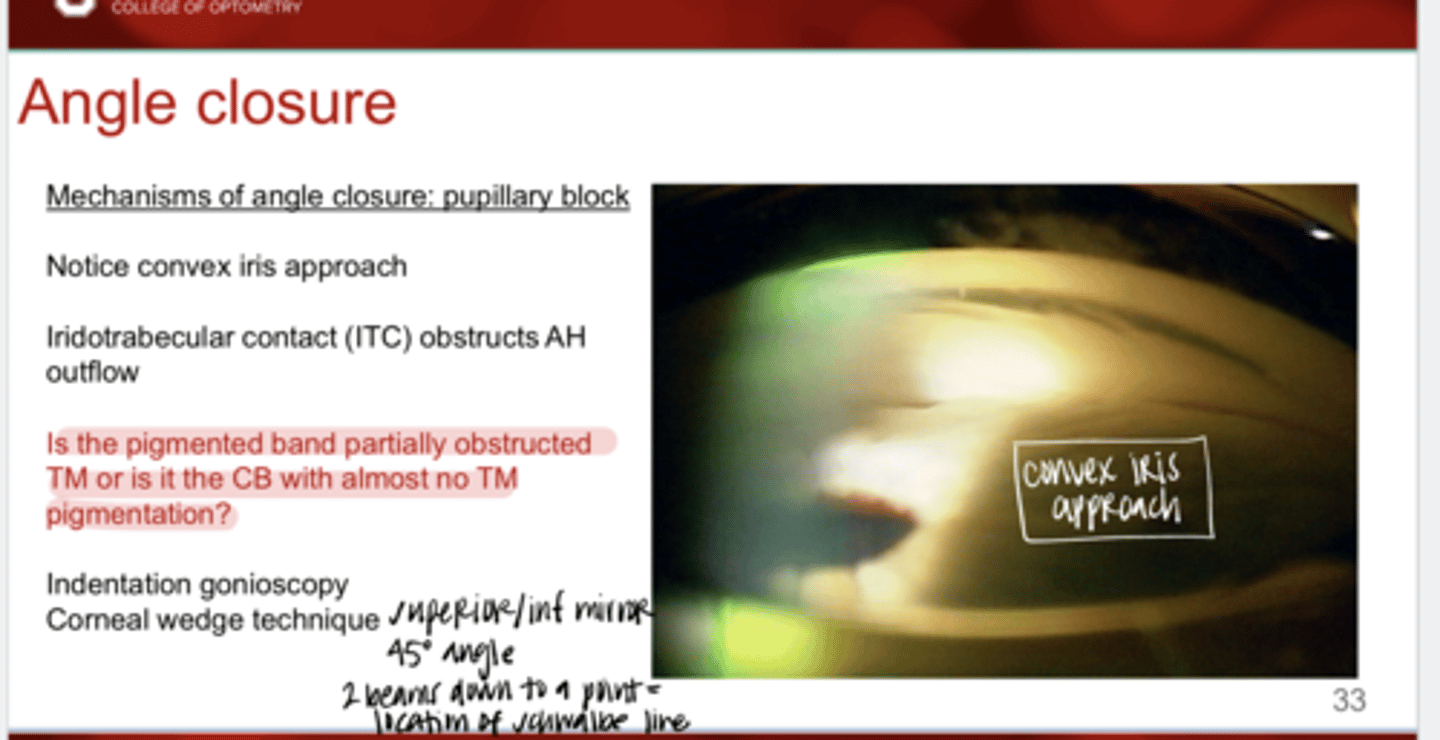
When there is ITC present and iris is physically obstructing outflow, how can you be sure the pigmented band you see is TM vs CB?
-indentation gonioscopy
-corneal wedge technique
Indentation gonioscopy is performed with what form of 4 mirror?
w/o flange
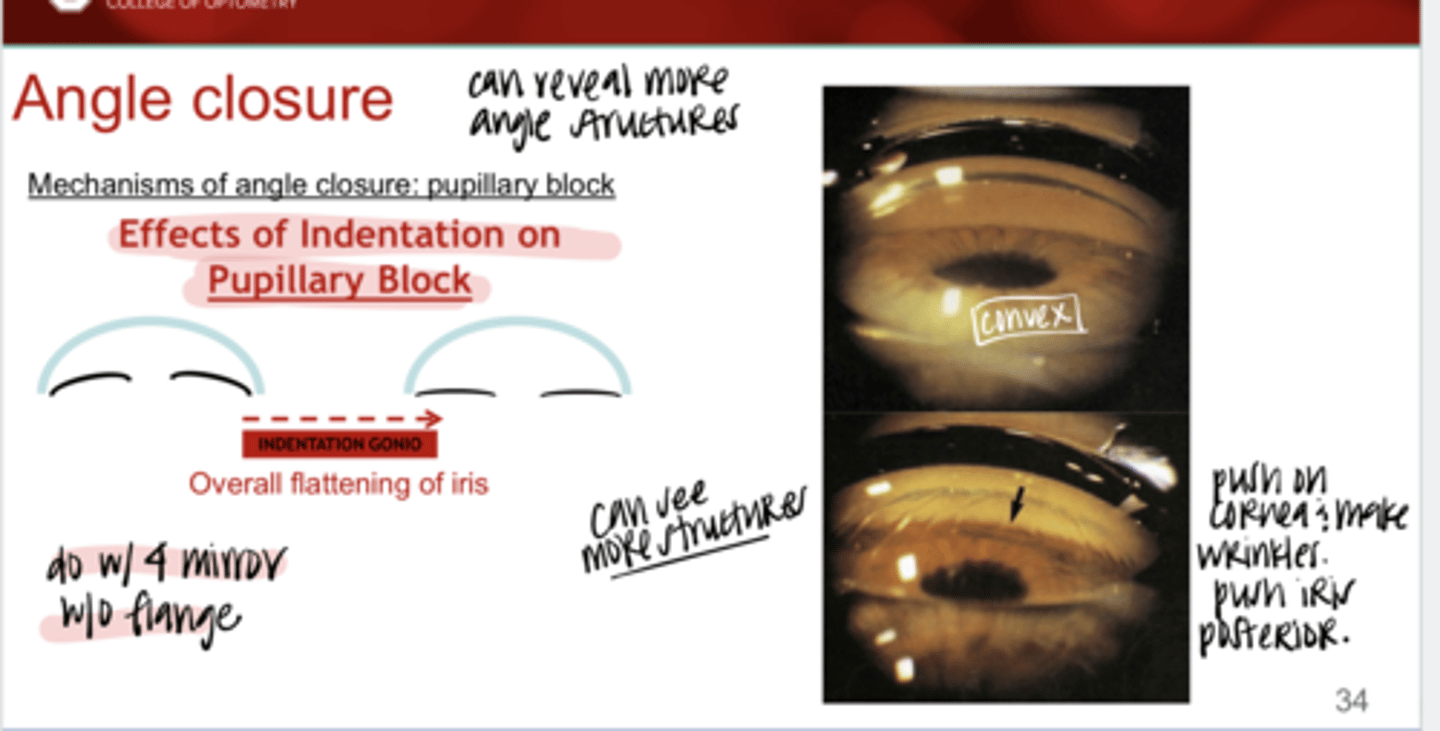
How to perform indentation gonioscopy w/ angle closure?
Push on the cornea w/ the gonio lens. Push the iris posterior & more structures will come into view. Leads to overall flattening of the iris.
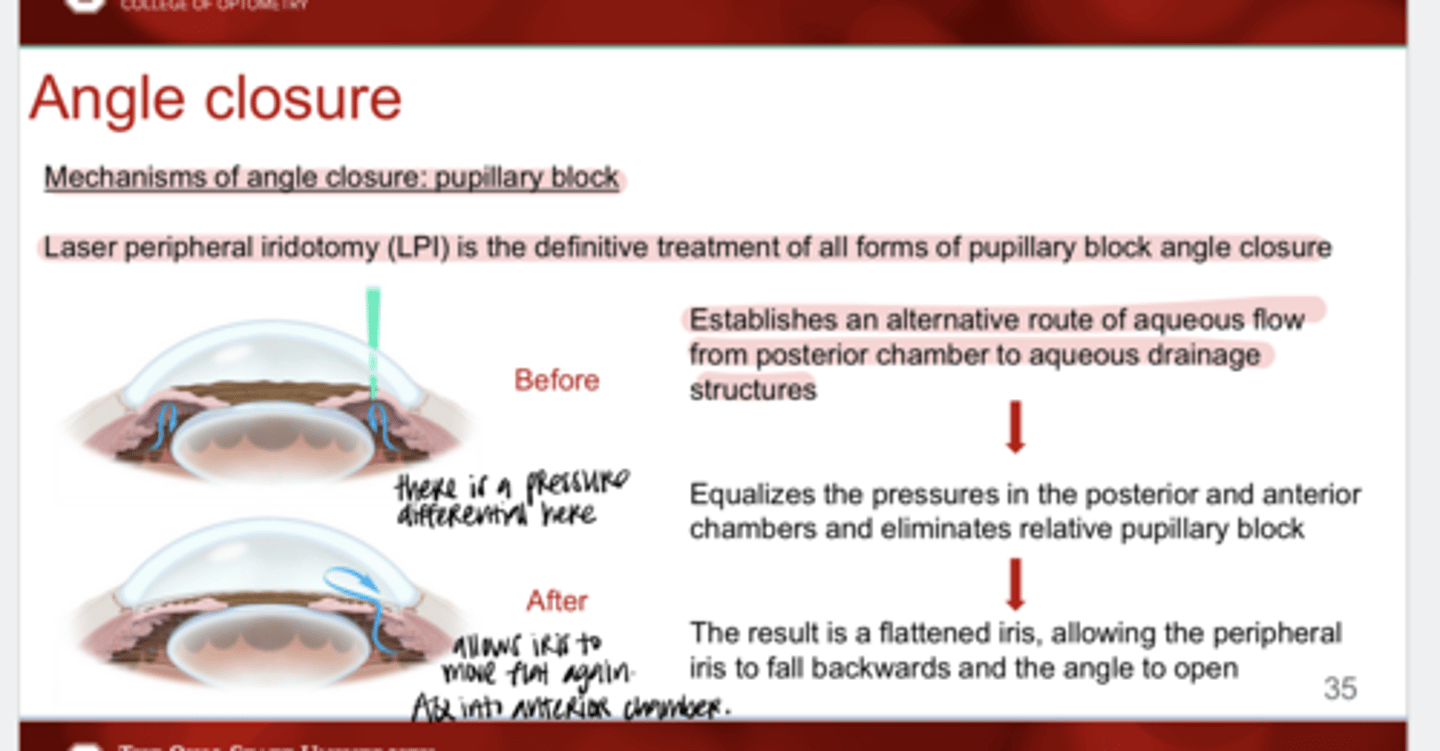
What is the definitive treatment for all forms of pupillary block angle closure?
LPI