Case 3: Rana Osmen - Obstruction/Croup
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
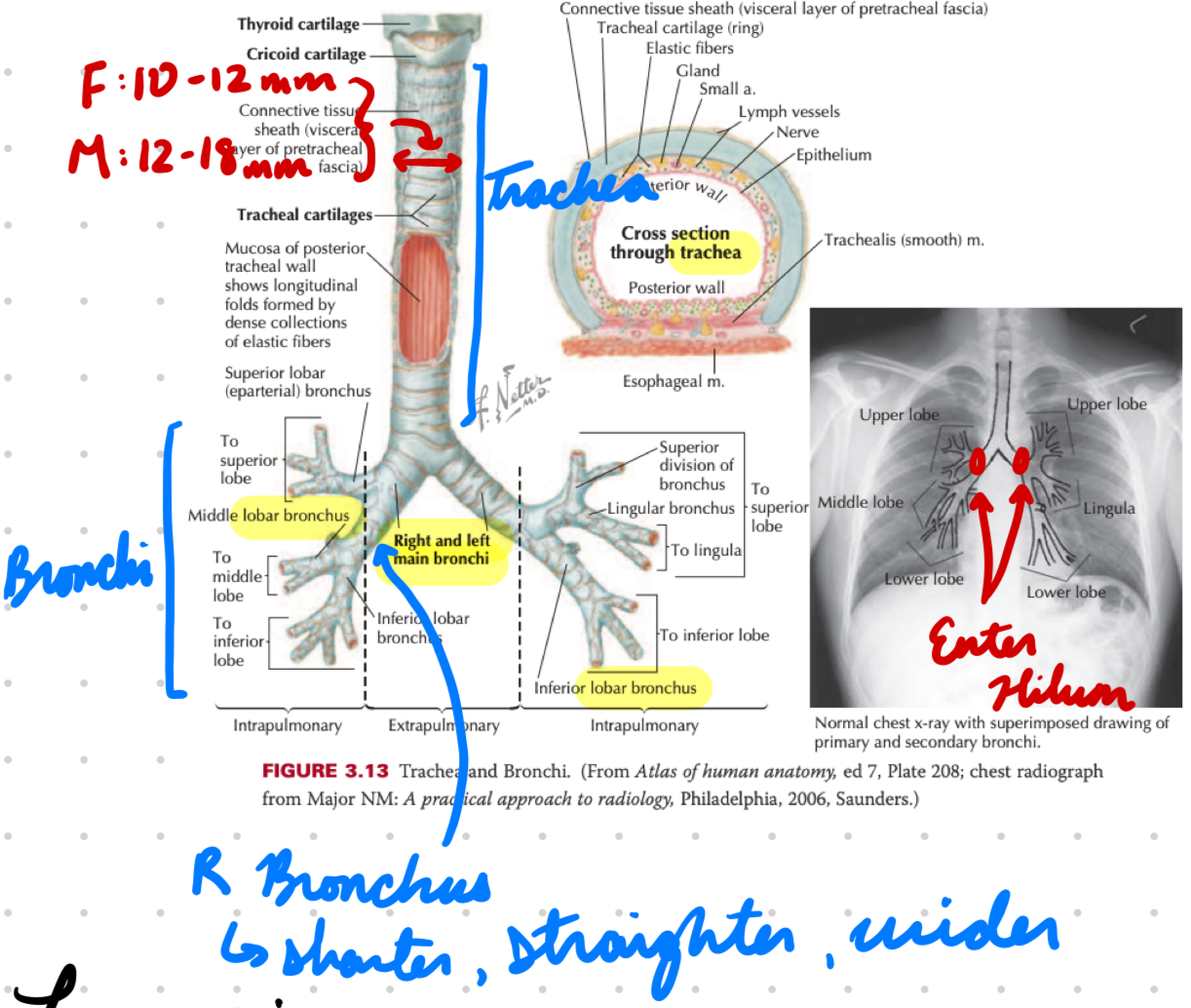
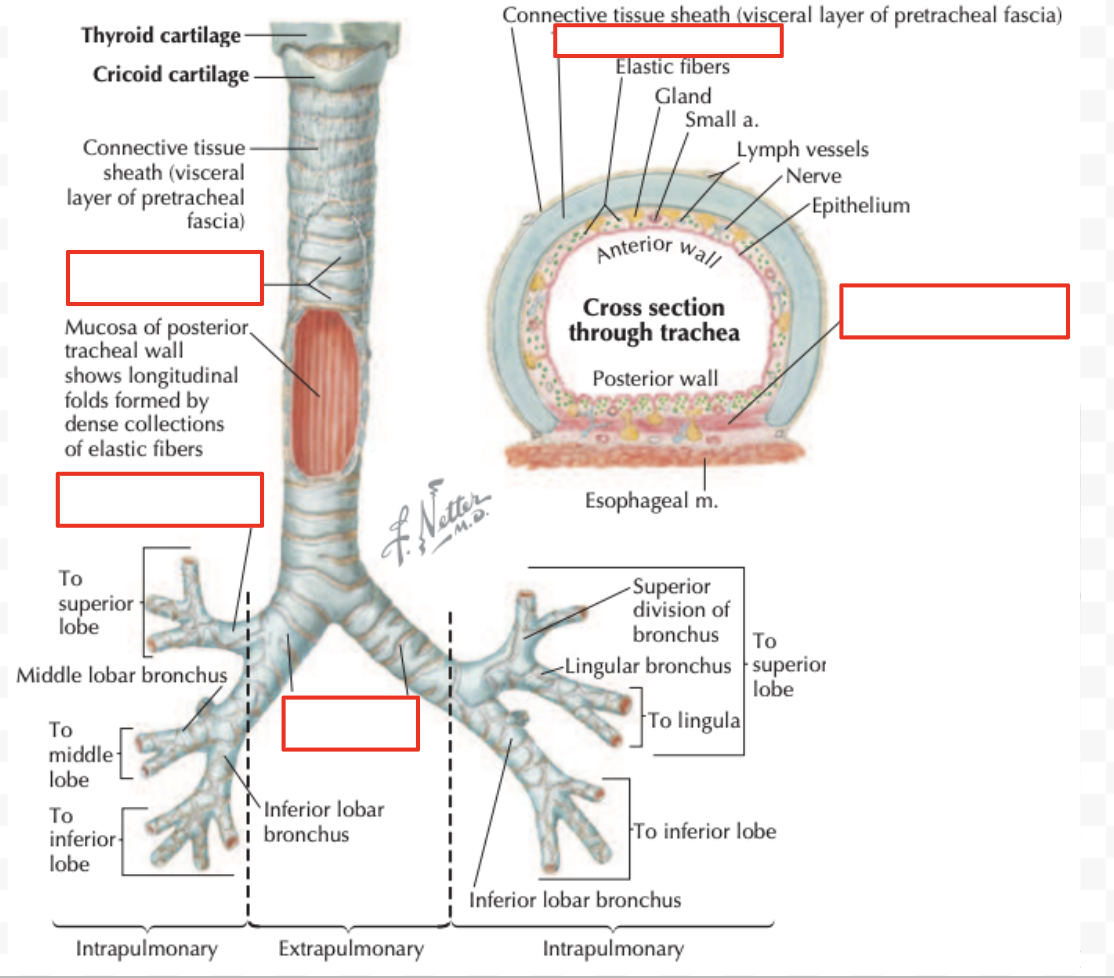
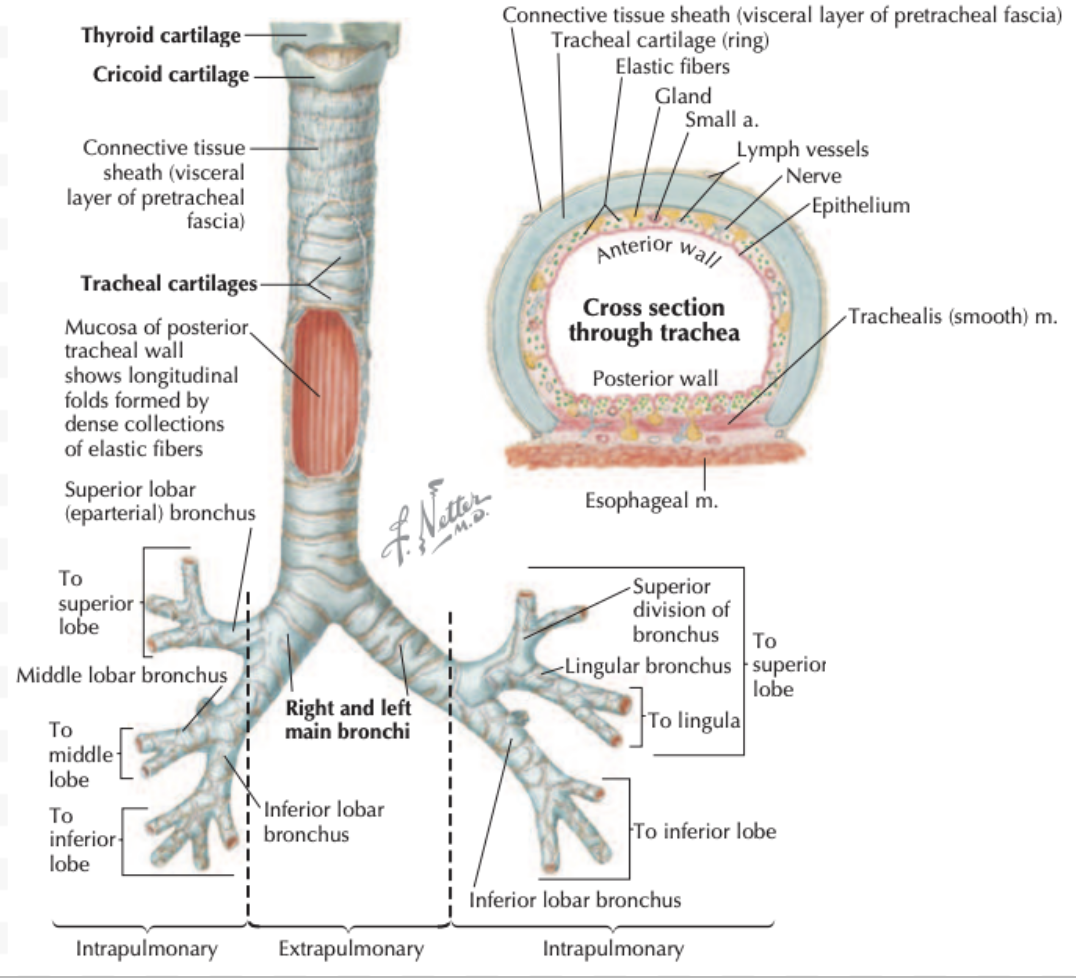
LRT: Trachea
Anterior to esophagus
Held open by C cartilage rings
Trachealis muscle at back (against esophagus)
LRT: Bronchi
Trachea divide at carina into right and left main bronchi
Enter hilum
Right bronchus shorter, wider, more vertical
Easy aspiration
Bronchi Divisions
Main bronchi → Lobar (secondary) bronchi → Tertiary bronchi → Divide until terminal bronchioles → Respiratory bronchioles
Cartilage to smooth muscles moving down
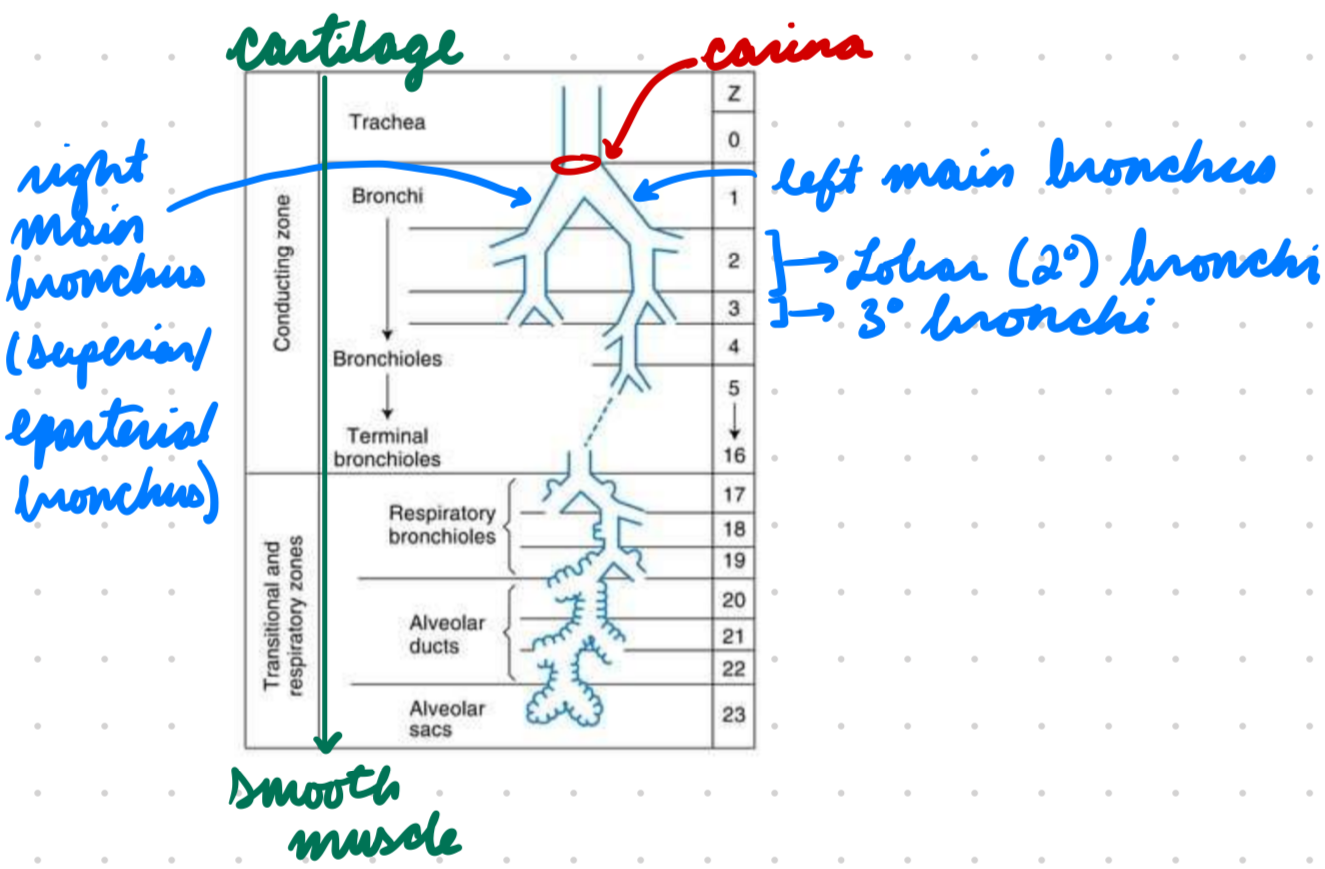
LRT: Alveoli
Alveolar ducts and sacs budding from respiratory bronchioles
Respiratory zone (gas exchange)
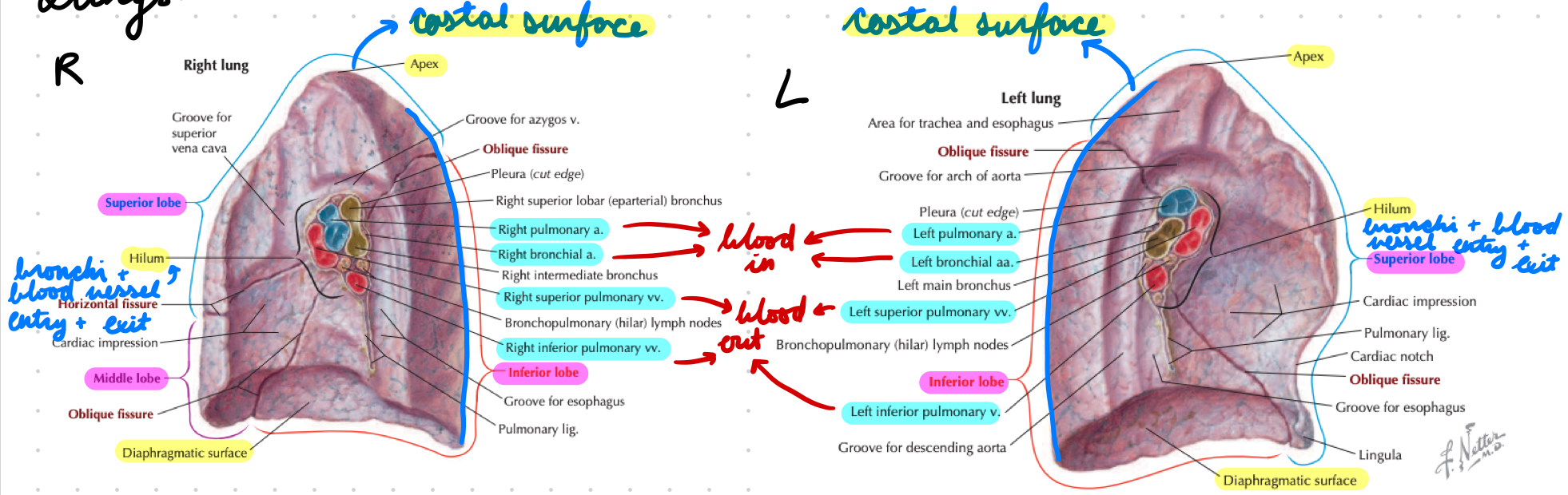
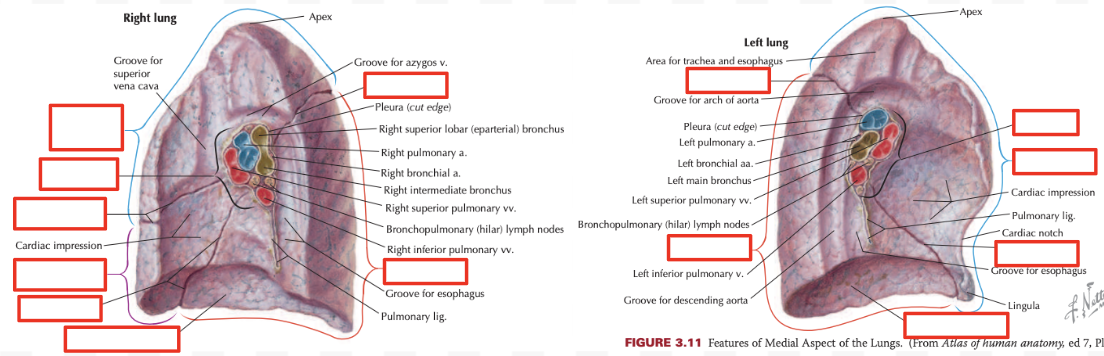
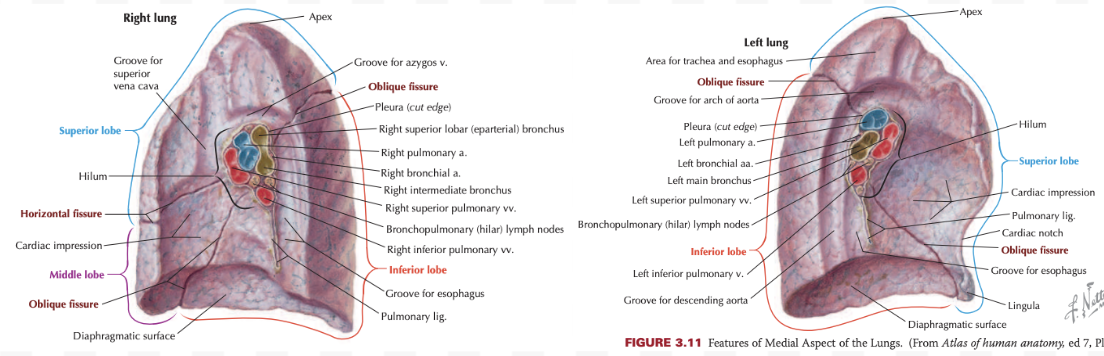
LRT: Lungs
Right: Bigger, 3 lobes
Left: Smaller, 2 lobes
Extend to 6th costal cartilage (rib)
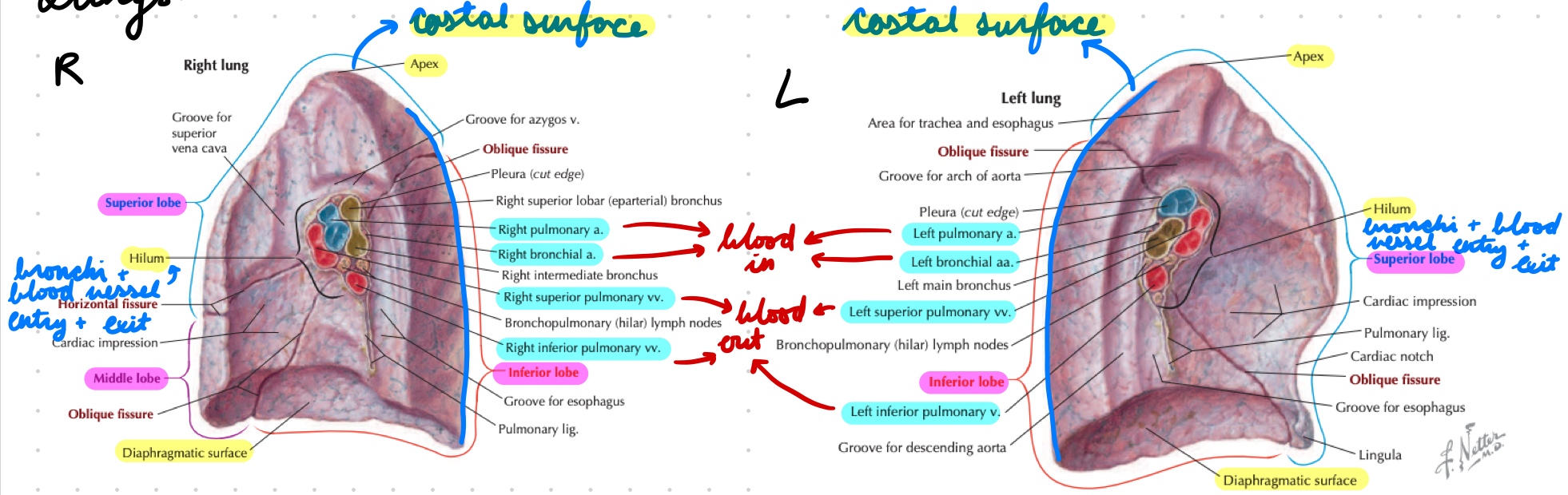
Lung Surfaces
Apex: Top of superior lobes, above clavicles
Hilum: Middle, attach to mediastinal structures
Costal: Outer, convex part
Diaphragmatic: Bottom, contact with diaphragm
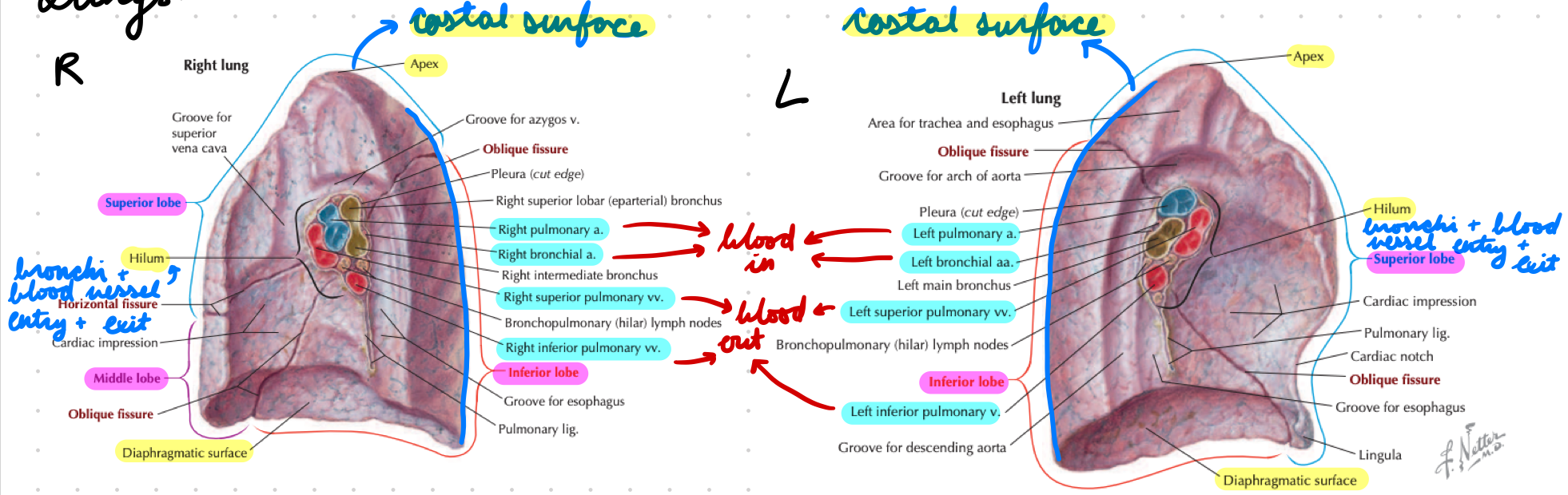
Lung Fissures
Right:
Oblique: Between superior, middle, and inferior lobes
Horizontal: Between superior and middle lobes
Left:
Oblique: Between superior and inferior lobes
Lung Innervation
ANS
Sympathetic bronchodilator fibres
Parasympathetic bronchoconstrictor fibres
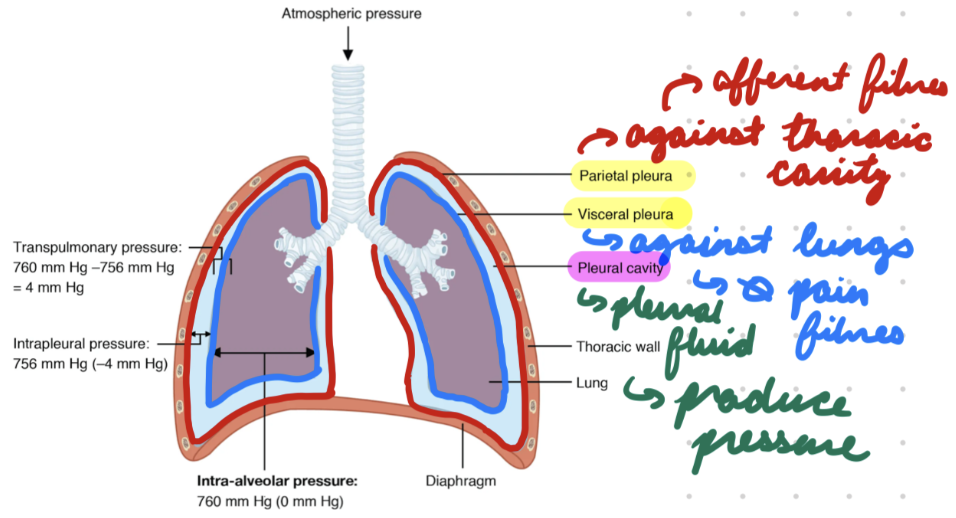
Pleura
Visceral
Parietal
Visceral Pleura
Around lungs (touching)
Left + right
Few/no pain fibres
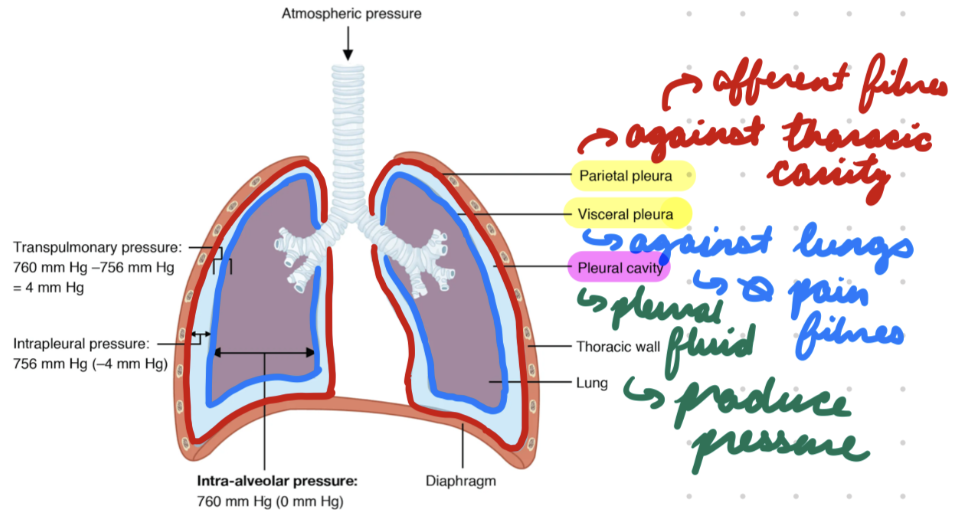
Parietal Pleura
Line outer cavity (not touching lungs)
Afferent fibre innervation
Extend to 9th costal cartilage (ribs)
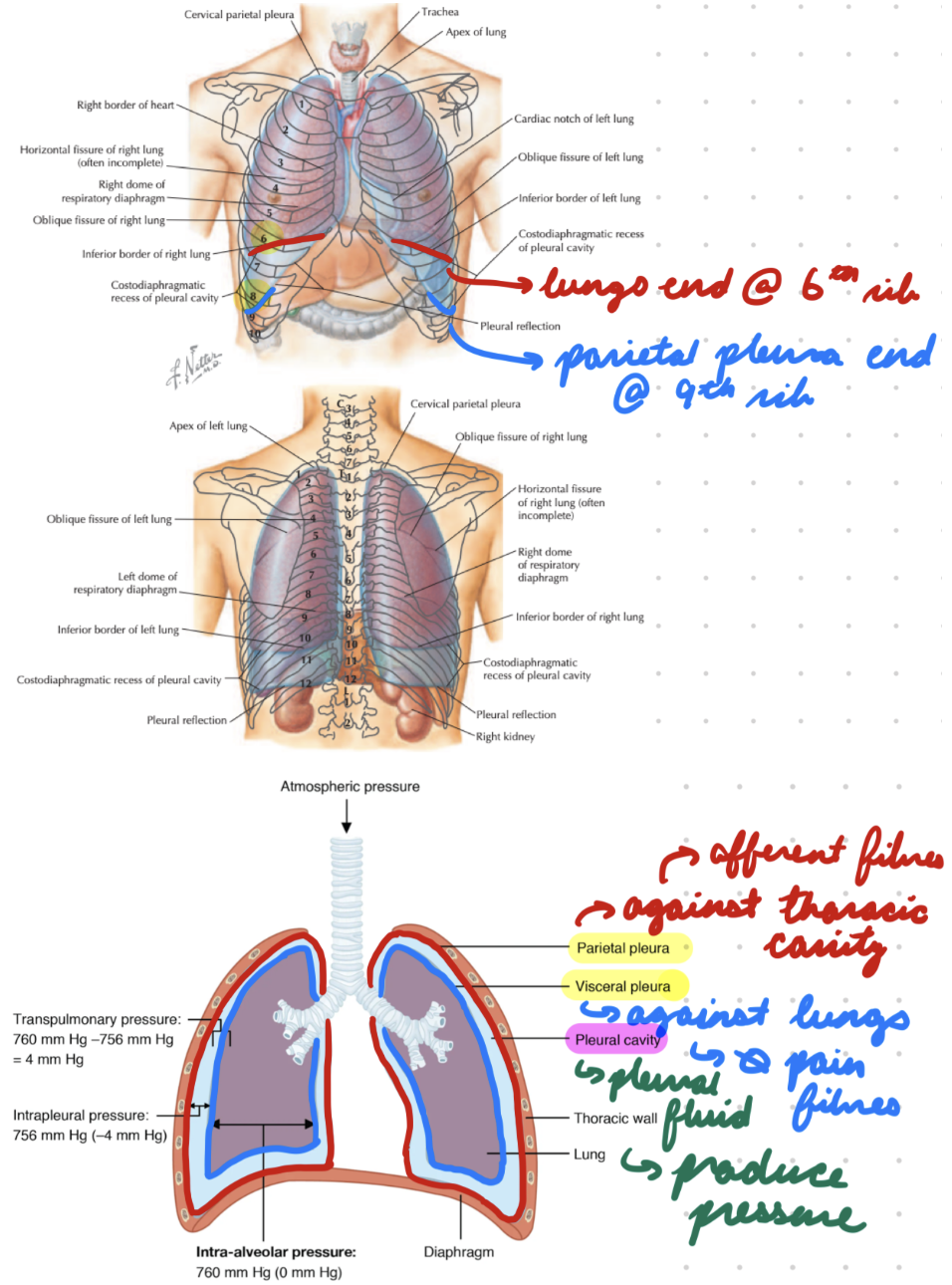
Pleural Spaces/Cavities
Contain lungs + lubricating serous fluid
Mediastinum
Middle space between pleural spaces
Pleural Pressure
Negative pressure (< -4 mmHg)
Fluid suction into lymphatic channels decrease pressure in pleural space
Hydrostatic force hold lungs open to thoracic wall
Pleural Pressure: Inspiration
Chest expansion pulls lungs outwards = Increase negative pressure
Air enters lungs
Pleural Pressure: Clinical Importance
Trauma (lung punctures) = Air entering intrathoracic space = Increase pressure = Prevent breathing
Pleural Fluid
Mucoid/serous fluid in pleural cavity produced by parietal pleural capillaries
Lubricate pleural cavity for lung movement
Decrease friction with chest wall
Transpulmonary Pressure
Alveolar P - Pleural P = Elastic force in lungs (recoil pressure)
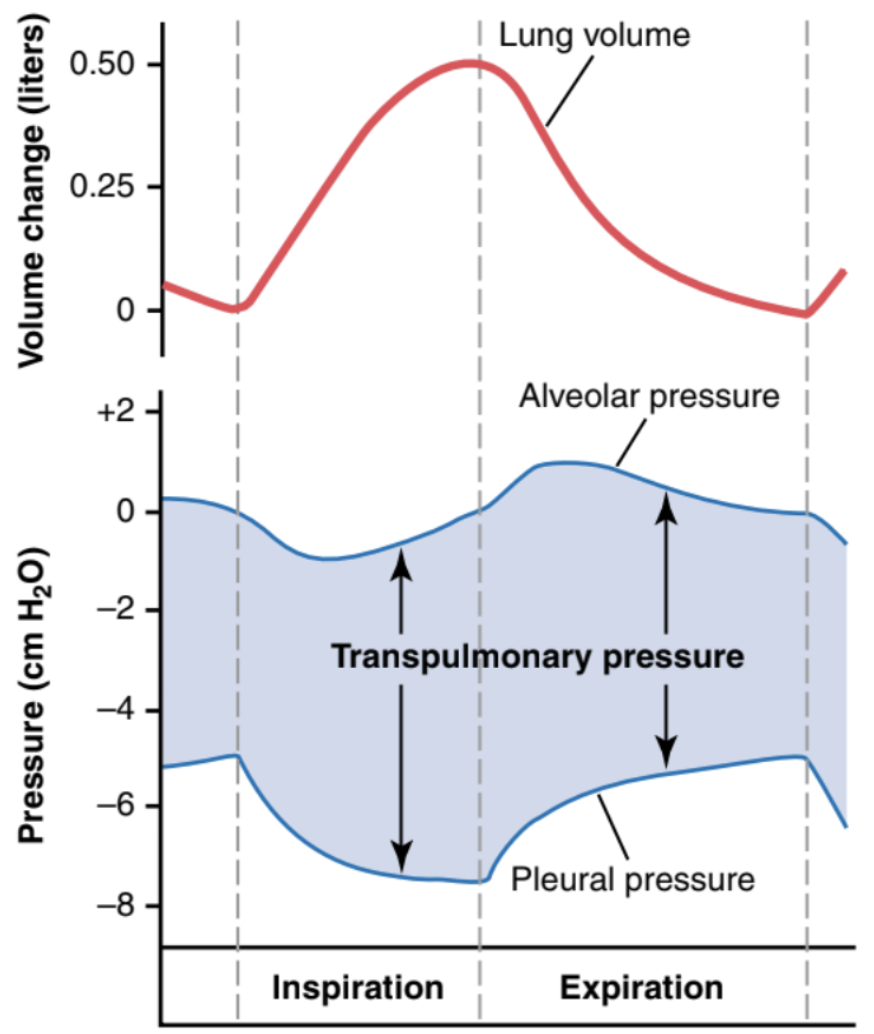
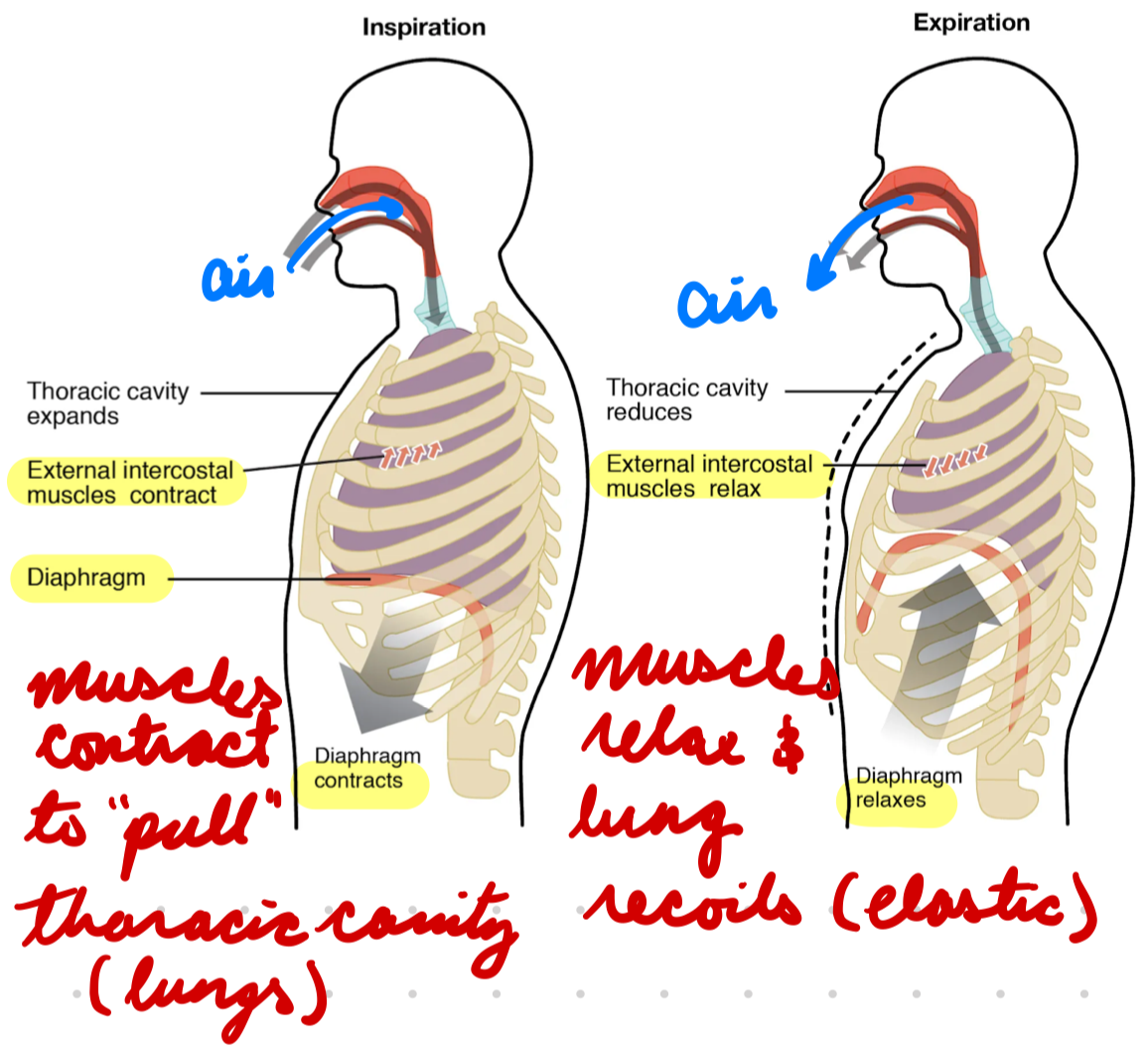
Respiratory Cycle
Negative-pressure breathing
Inspiration: Diaphragm, external intercostal, scalene muscles contract to pull lungs down/out = Increase alveolar volume
Alveolar P decreases (< atmospheric P)
Air enters lungs (P gradient)
Expiration: Diaphragm, external intercostal, scalene muscles relax to compress lungs (elastic recoil) = Decrease alveolar volume
Alveolar P increases (> atmospheric P)
Air leaves lungs (P gradient)
Pulmonary Resistance
Airway resistance + pulmonary tissue resistance (overcome with pleural fluid)
R = 1/r^4
Diameter decrease = resistance increase
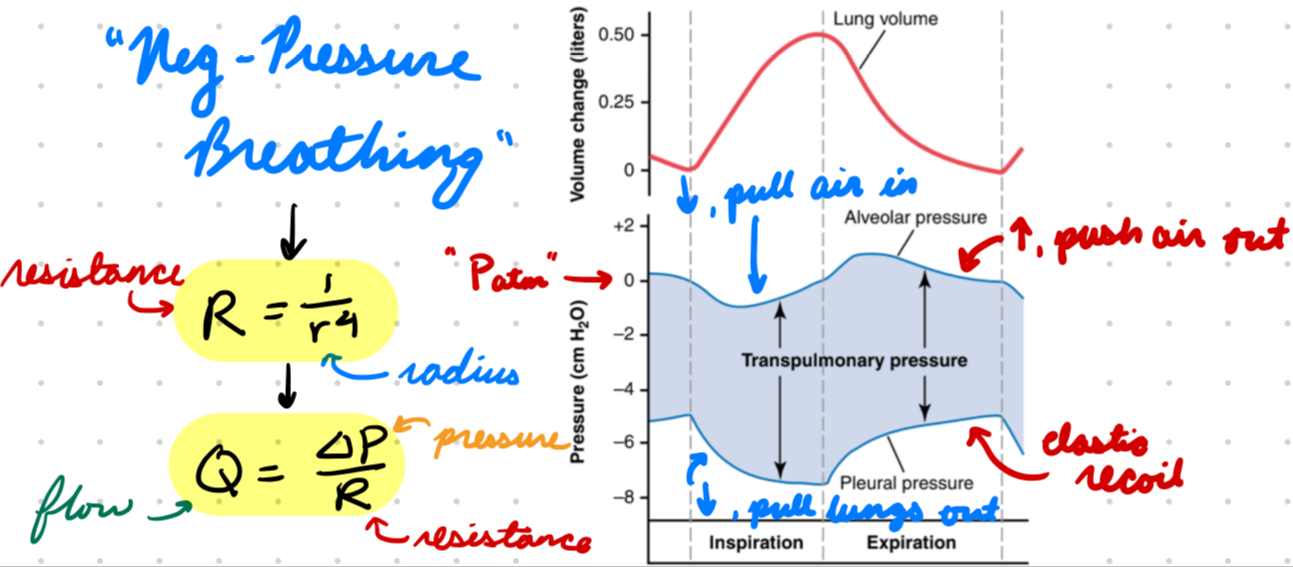
Flow
Flow = Pressure difference/Resistance
Decrease airway diameter/radius from obstruction = Increase resistance = Decrease airflow

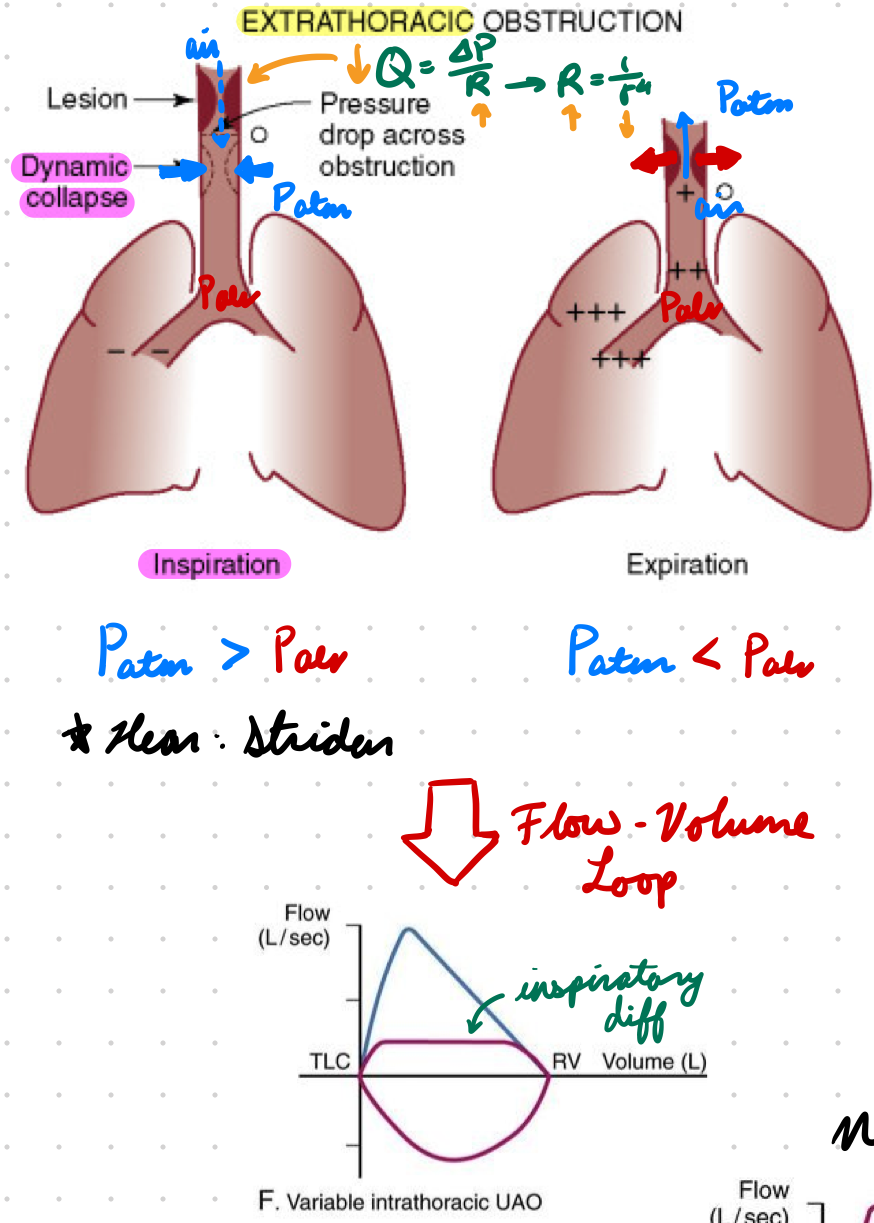
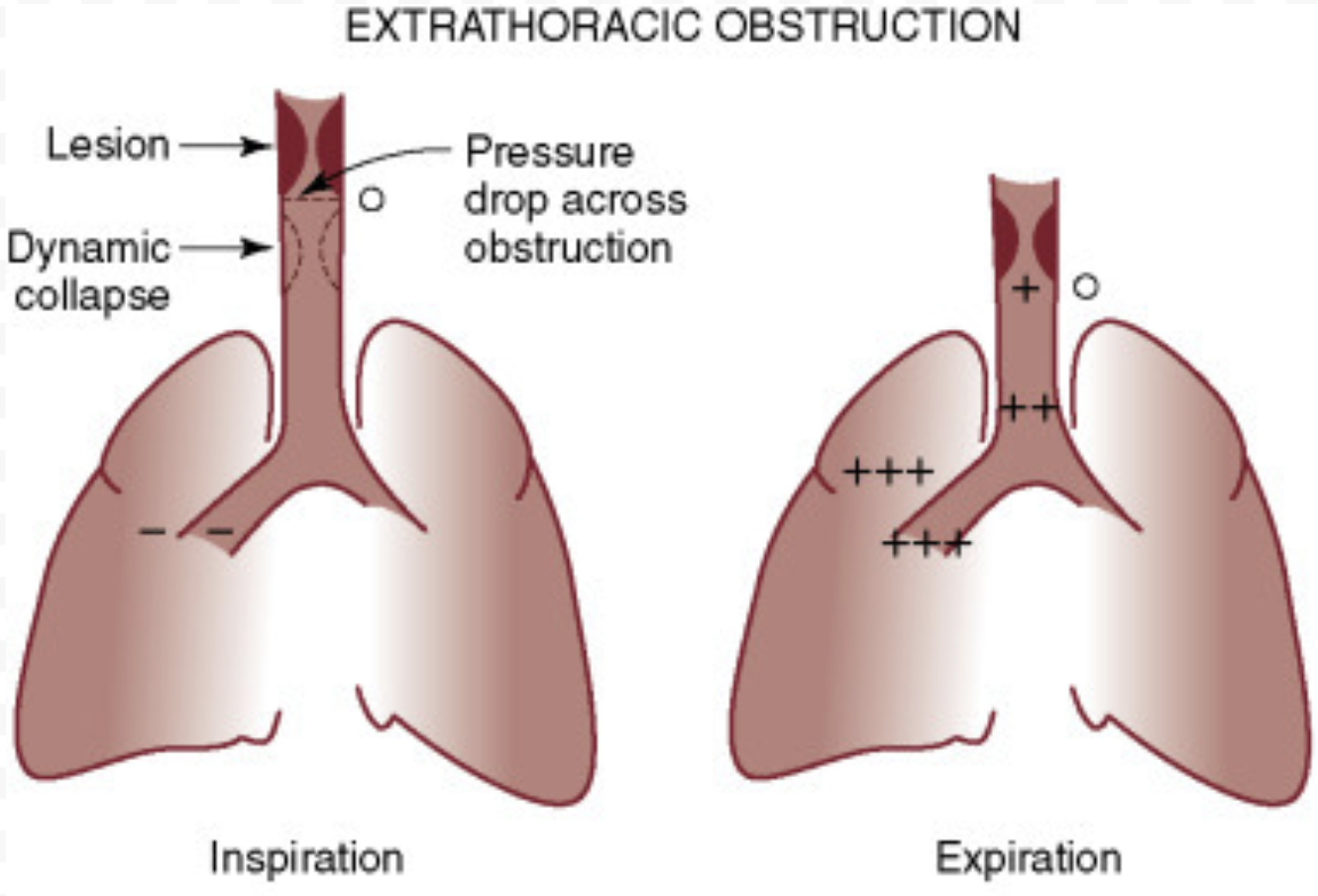
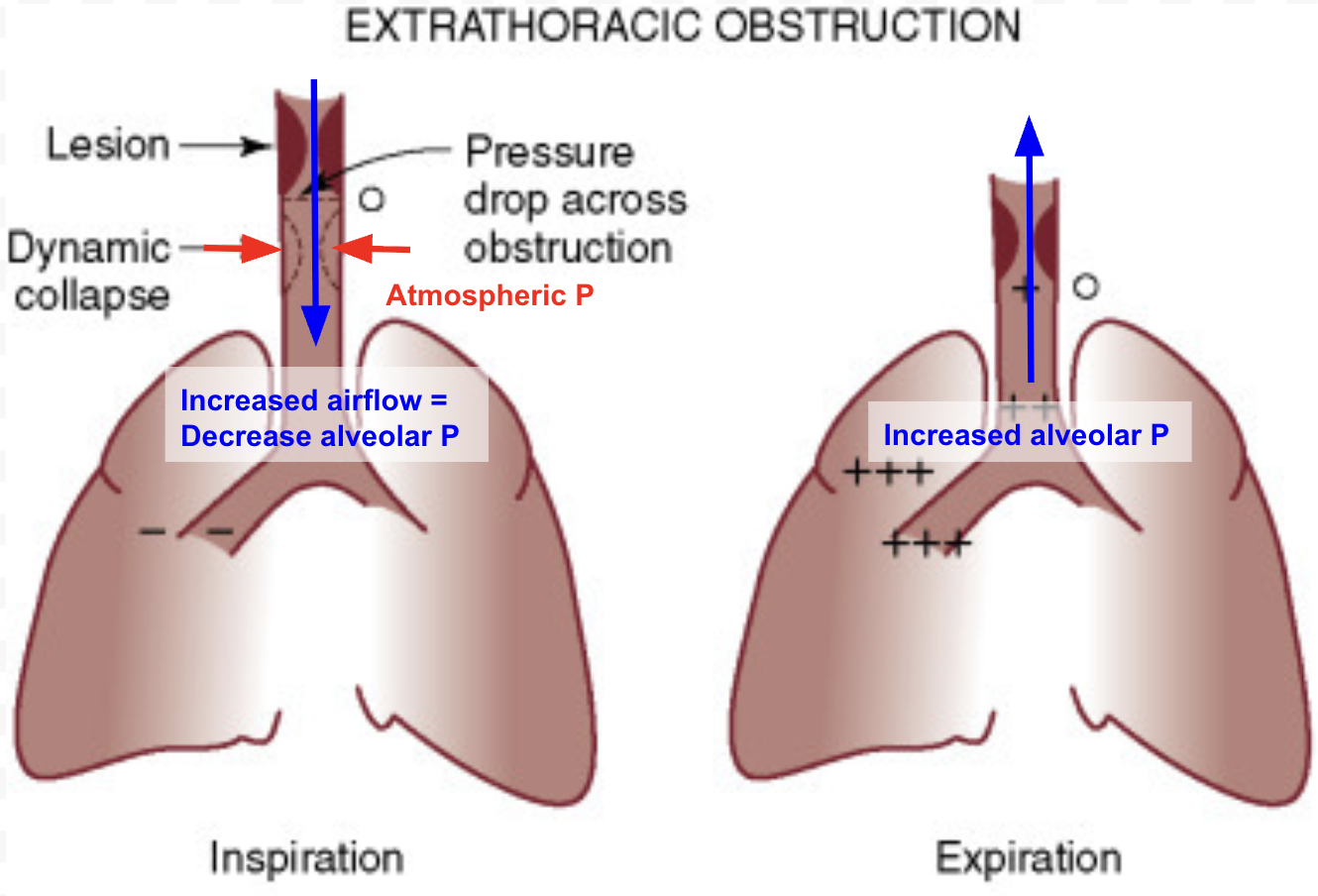
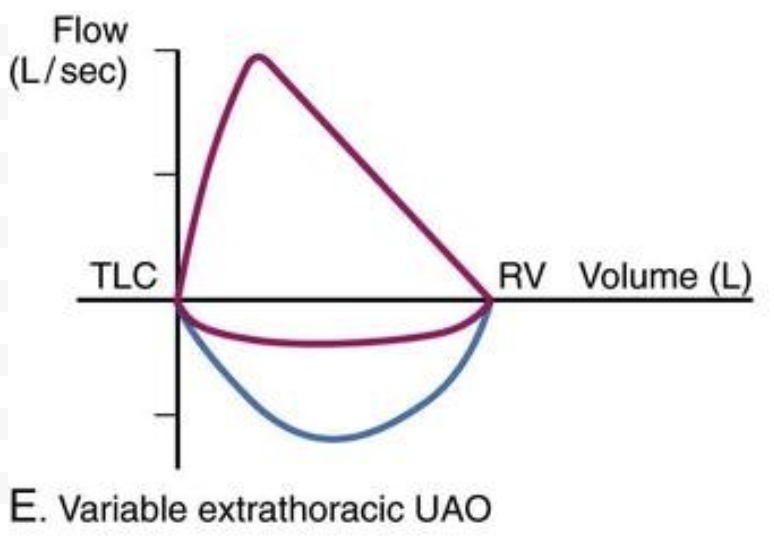
Extrathoracic Obstruction
Obstruction in URT
Extrathoracic Obstruction: Inspiration
Difficult
Obstruction = Narrow airway = Increase flow = Decrease pressure on airway wall
Atmospheric P > Alveolar P = Airway collapse inward = Worsen obstructive lesion
Hear: Stridor
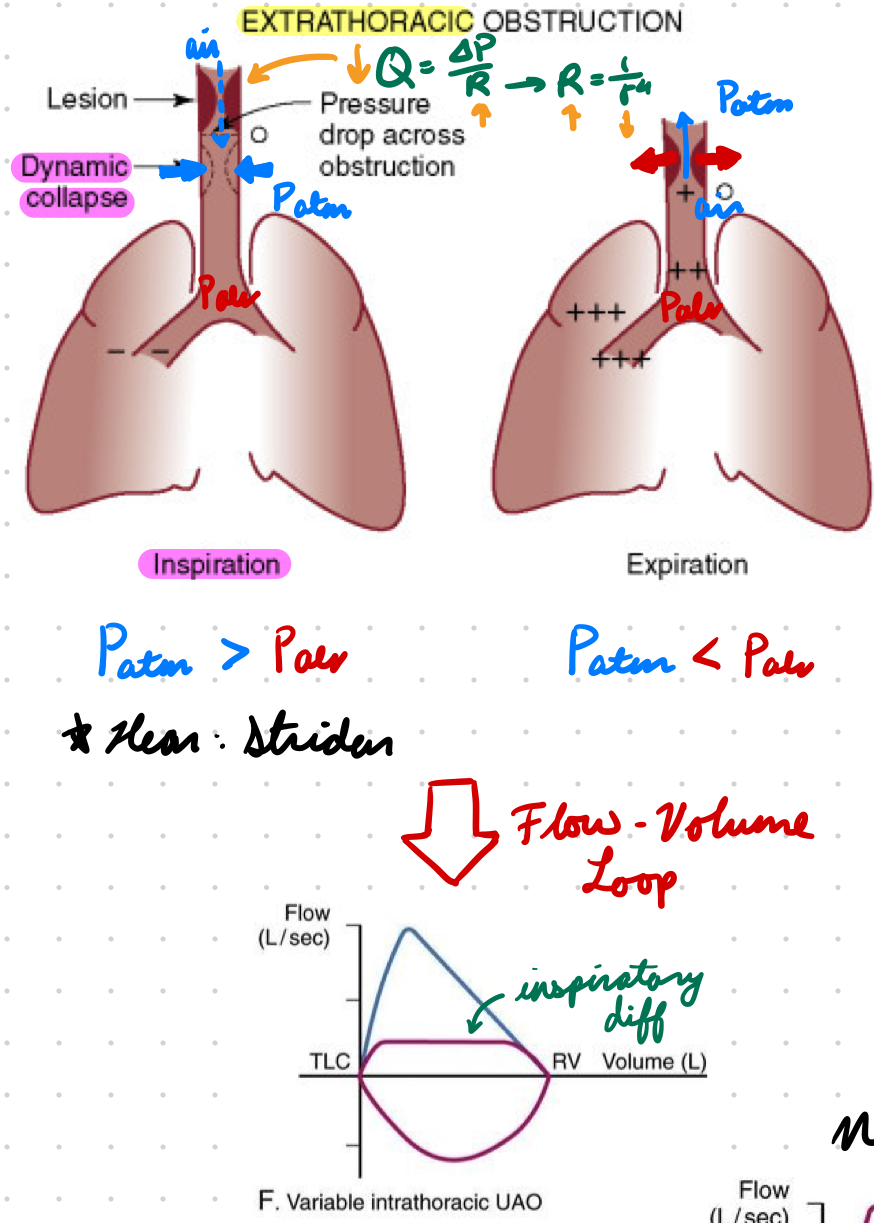
Extrathoracic Obstruction: Expiration
Alveolar P > Atmospheric P = Pressure opens airway
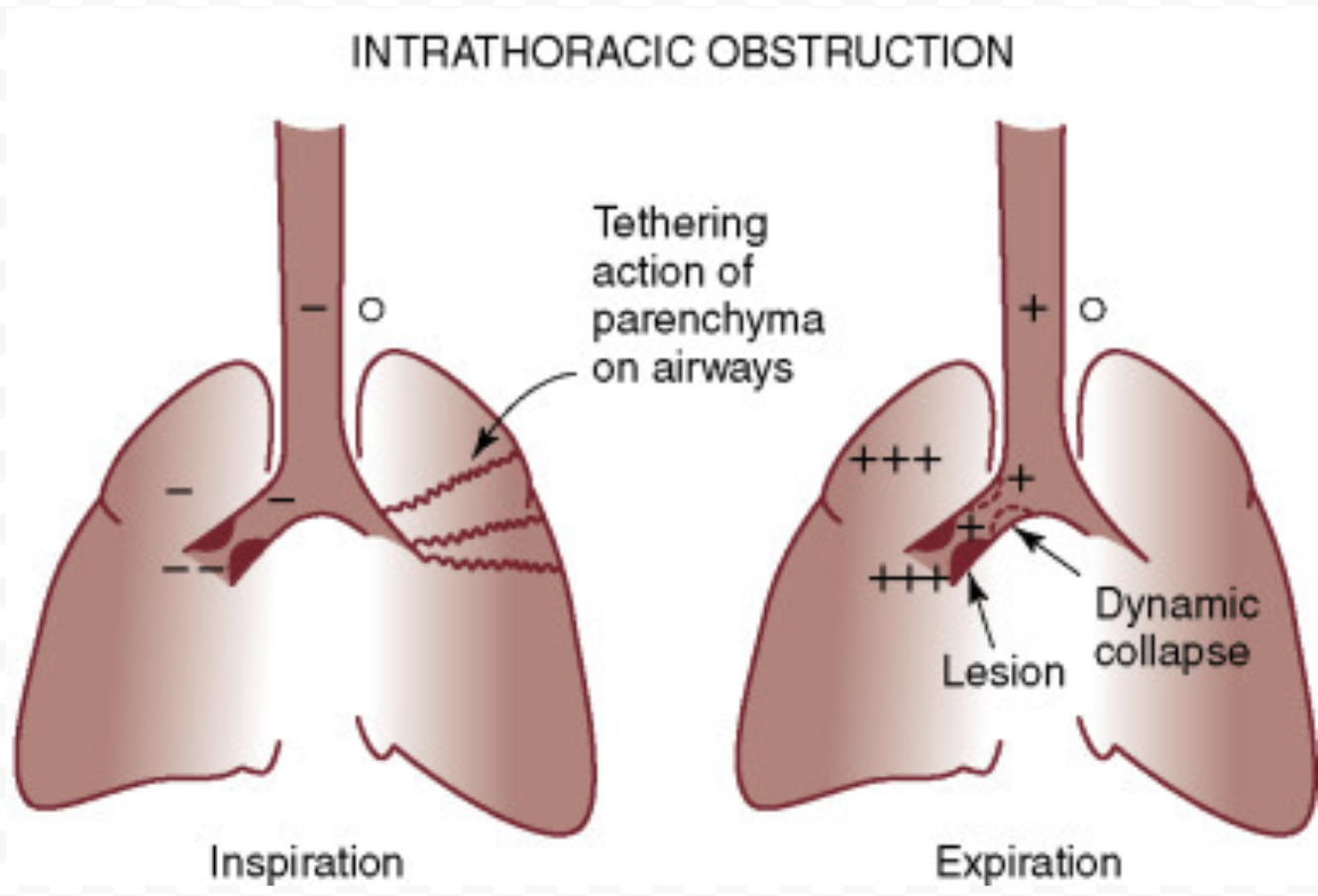
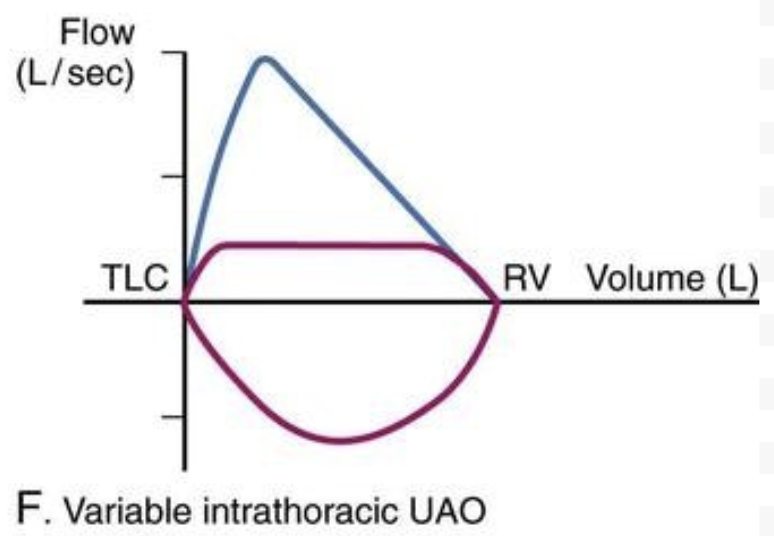
Intrathoracic Obstruction
Obstruction in LRT
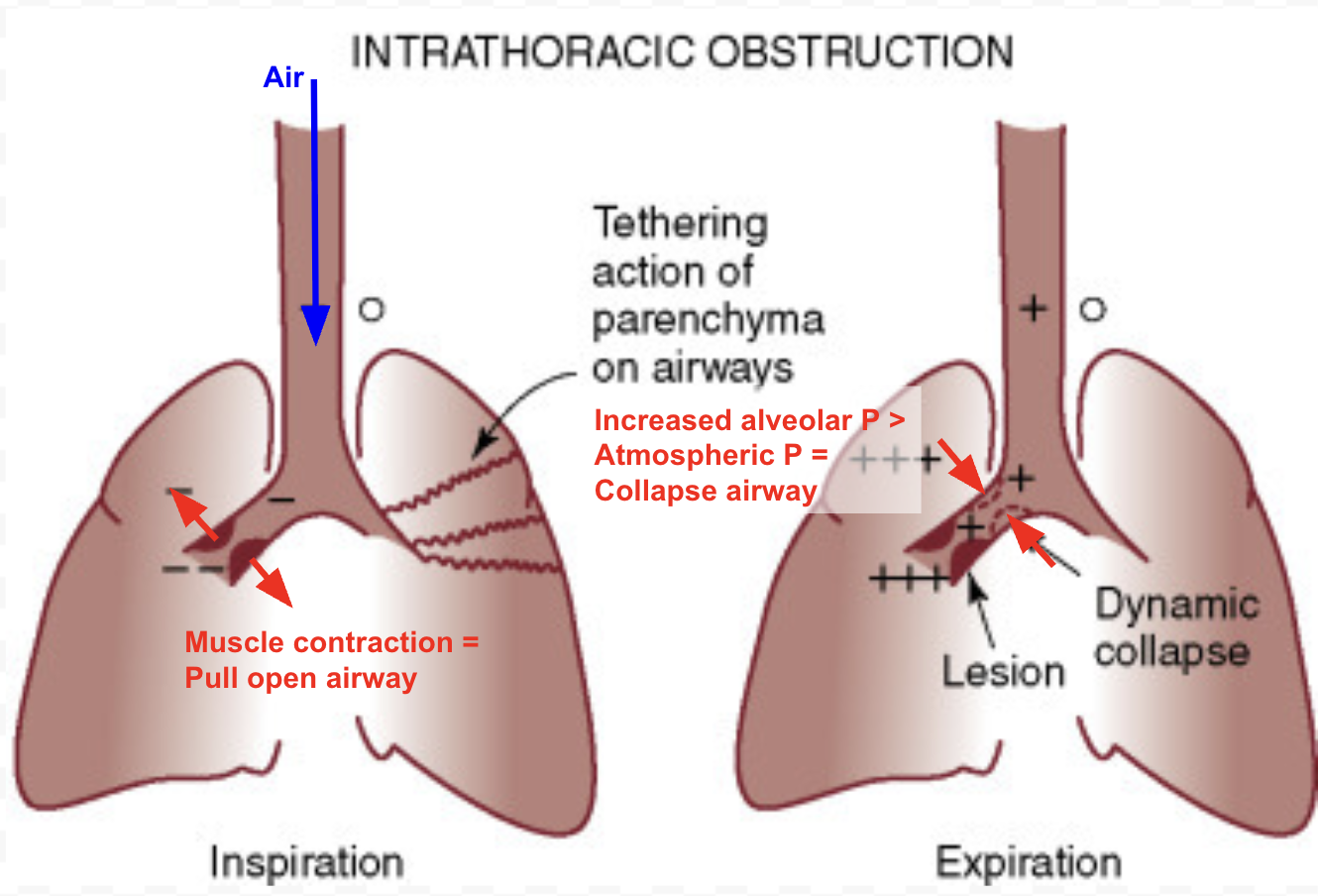
Intrathoracic Obstruction: Inspiration
Muscle contraction expands lungs = Open obstructed airway
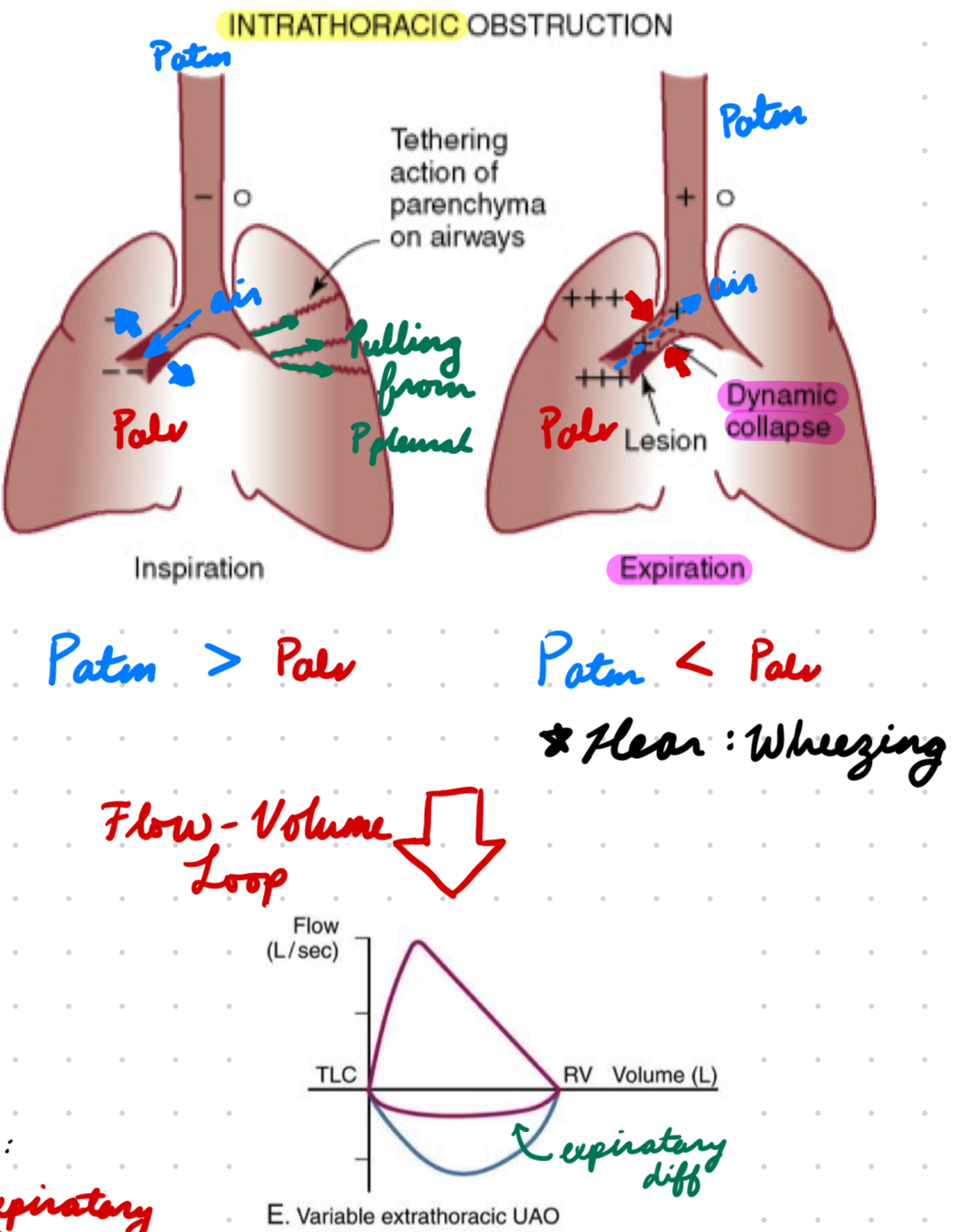
Intrathoracic Obstruction: Expiration
Difficult
Alveolar P > Atmospheric P = Collapse airway
Hear: Wheezing
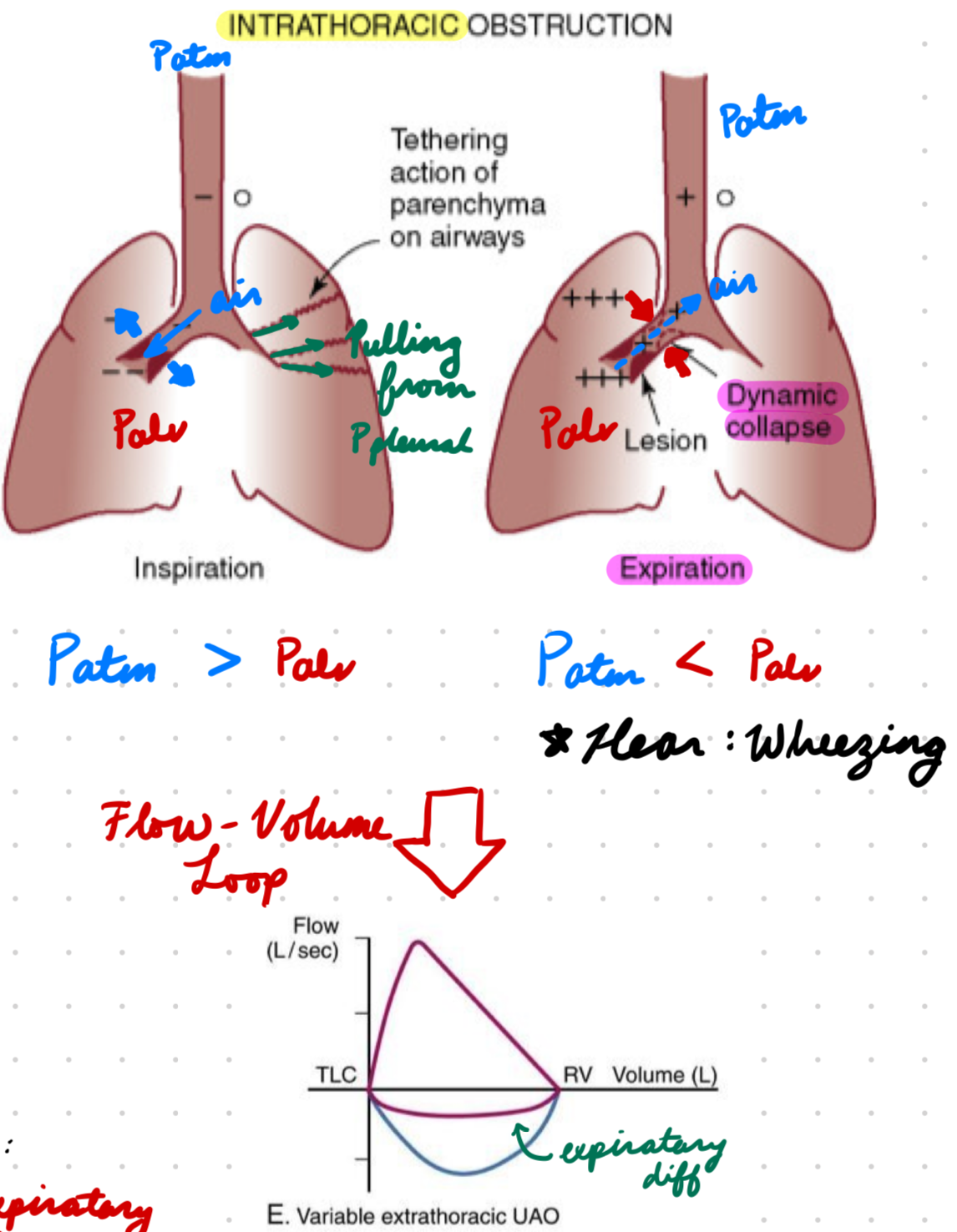
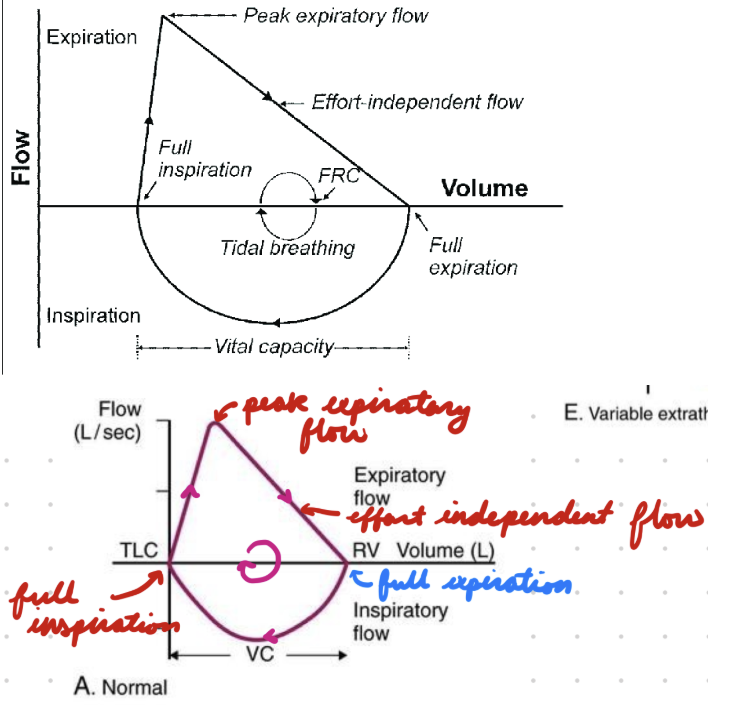
Flow-Volume Loop
From pulmonary function test
Read clockwise
Flow-Volume Loop: Extrathoracic Obstruction
Difficult inspiration = Depressed inspiration loop
Flow-Volume Loop: Intrathoracic Obstruction
Difficult expiration = Depressed expiration loop
Croup: Description
Respiratory illness affecting URT (larynx, trachea)
Croup: Epidemiology
Common in children <6 years (small airways)
Usually in fall and winter
Croup: Etiology
Viral infections (most common)
Mostly: Parainfluenza virus
Others: Adenovirus, resp syncytial virus, enterovirus, rhinovirus, coronavirus, echovirus
Bacterial infection (less common)
Airway abnormalities
Resp pathologies (allergies, asthma)
Croup: Pathogenesis
Inflammation and edema narrow upper airway
Subglottic larynx region and trachea
Decrease airflow
Cause:
Stridor
Increased resp rate, inspiratory volume, resp effort
Hypoxia, hypercapnia, resp failure
Croup: Investigations
No lab tests or imaging
Take history, physical, and response to treatment
Croup: Clinical Presentation
Stridor
Barky cough
Croup: Treatment
Usually self-contained
Steroids: Anti-inflammatory reduce edema + obstruction
Dexamethasone
Nebulized budesonide
Severe: Nebulized epinephrine
Epiglottitis: Description
Upper airway inflammation and obstruction
Life-threatening
Epiglottitis: Epidemiology
All ages
Vulnerable: < 12 months, > 85 years
Epiglottitis: Etiology
Bacterial infection
Staphylococcus and streptococcus
Viral and fungal infections
Epiglottitis: Pathogenesis
Edema in supraglottic structures (epiglottis surface and aryepiglottis folds)
Epiglottis shifts posteriorly
Obstruct airway
Inflammation narrow airway lumen = Decrease airflow
Epiglottitis: Investigation
Imaging after physical for confirmation
X-ray
Laryngoscopy
Ultrasound
Epiglottitis: Clinical Presentation
Fever
Sore throat
Painful swallowing (odynophagia) + drooling
Epiglottitis: Treatment
Antibiotics: Bacterial infection
3rd gen cephalosporin
Corticosteroids: Anti-inflammatory + reduce swelling
Dexamethasone
Budesonide
Children: Immediate intubation