Session 3: Clinical Effects of the Ageing Musculoskeletal System
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
Resorption
Osteoclasts break down bone tissue
Bone formation
Osteoblasts form a matrix to replace resorbed bone with new bone
Vertebral fracture
Curvature of the spine and loss of height
Pain, breathing difficulties, GI problems and difficulties in performing ADLs
Majority of vertebral fractures (50-70%) do not come to clinical attention.
Osteoporosis
Systemic skeletal disease characterised by low bone mass and microarchitectural deterioration of bone tissue leading to...
- Increased bone fragility
- Increased risk of fracture
Non-modifiable risk factors of osteoporosis
Age
Female sex
Ethnicity (caucasians)
Previous fractures
Family history
Late menarche (>16 years old), early menopause (<47 years old)
Modifiable risk factors of osteoporosis
Bone mineral density
Alcohol (>3.5 units/day).
Weight BMI <20
Smoking
Physical inactivity
Medication risk factors of osteoporosis
Long term antidepressants
Antiepileptics
Aromatase inhibitors
Long-term DMPA
GnRH agonists
PPIs
Oral glucocorticoids
Thiazolidindione for DM TZDs
Name some endocrine conditions which are associated with increased risk of osteoporosis
Diabetes mellitus
Hyperthyroidism
Hyperparathyroidism
Hyperprolactinaemia
Cushing's disease
Menopause
Hypogonadism
Androgen deprivation therapy
Treatment with aromatase inhibitors
Name some neurological conditions which are associated with increased risk of osteoporosis
Alzheimer's
Parkinson's
Multiple sclerosis
Stroke
Name some other conditions that are associated with an increased risk of osteoporosis
Rheumatoid arthritis
Systemic lupus erythematosus
Inflammatory bowel disease
Cystic fibrosis
Epilepsy
HIV
Depression
Asthma
Chronic kidney disease
Bone mineral density (BMD)
Expressed as T-score which is the number of SD below the mean BMD of young adults at their peak bone mass
Normal BMD
T-score of -1 SD or above
Osteopenia BMD
T-score of -1 to -2.5 SD
Osteoporosis BMD
T-score of -2.5 SD or less
Established severe osteoporosis
T-score of -2.5 SD or below with one or more associated features
How is osteoporosis diagnosed?
DEXA scan (dual energy x-ray absorptiometry)
Fragility fractures
Fractures that result from mechanical forces that would not ordinarily result in a fracture, known as low-level trauma e.g., fall from standing height or less
Risk factors for fragility fractures
Reduced bone density
Oral/systemic glucocorticoids
Age
Sex
Previous fractures
Family history of osteoporosis
Interventions (lifestyle) for osteoporosis
Static/dynamic weight bearing exercise (low and high force)
Muscle resistance training and balance
Interventions (diet) for osteoporosis
Supplementation with 10 micrograms/day of vitamin D (400 IU)
Dietary calcium
Vitamin B, Vitamin K
Reduce salt intake
Balanced diet
Osteoblast
Cells that form new bones and grow and heal existing bones
Osteoclast
Cells that degrade bone to initiate normal bone remodelling and mediate bone loss in pathological conditions by increasing their resorptive activity
Consequences of hip fractures
High mortality rate
High morbidity rate
PE/DVT/CVA/MI
Pressure sores
Chest infections/UTIs
Confusion
What is OA (NICE)
Osteoarthritis is defined by NICE as a disorder of synovial joints, that is characterised by...
- Focal areas of damage to the articular cartilage
- Remodeling of underlying bone at the formation of osteophytes - new bone at joint margins
- Mild synovitis
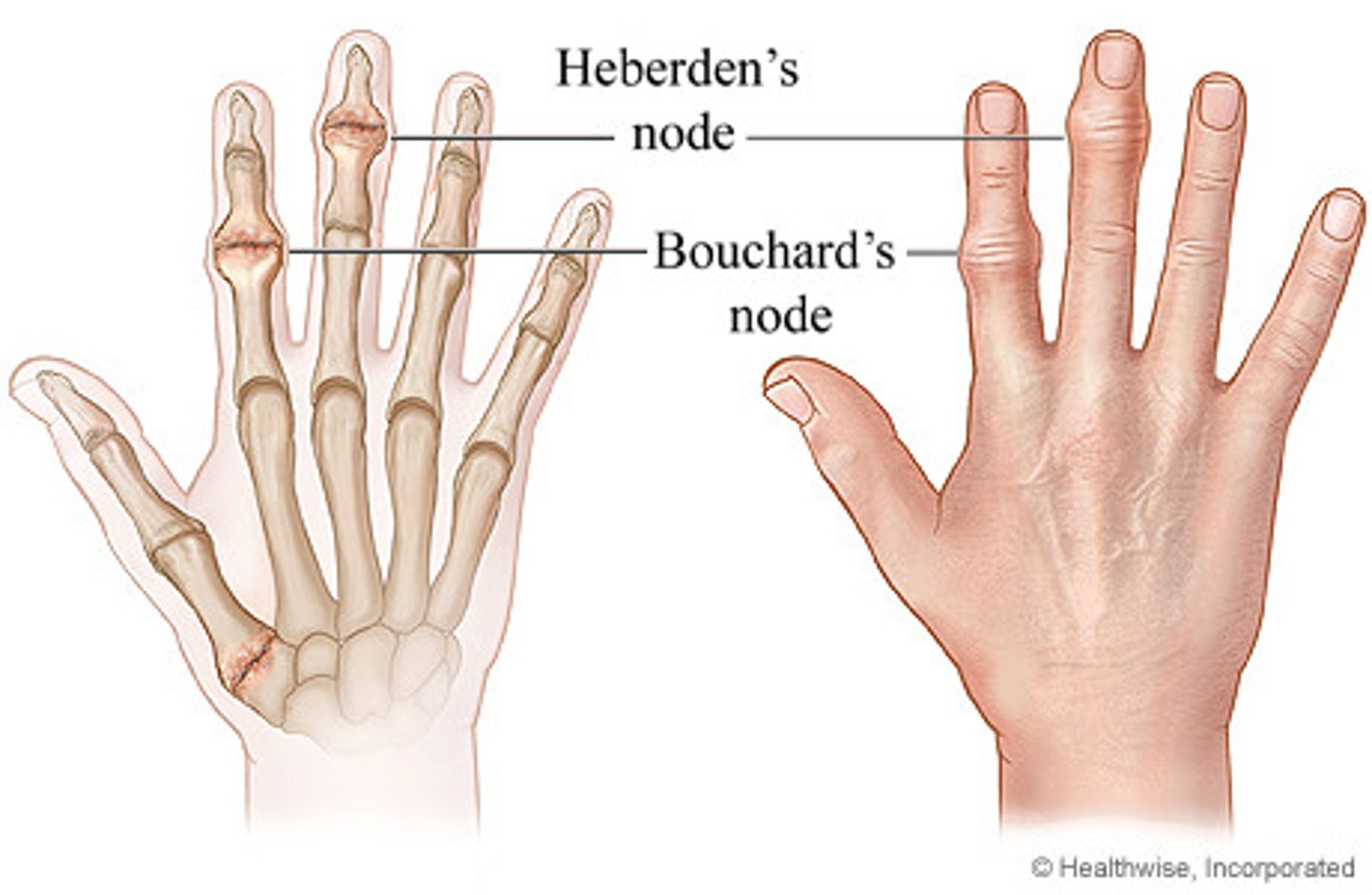
Clinical features of OA
Pain
Stiffness
Deformity
Joint swelling
Heberden's nodes
Bouchard's nodes
Radiological features of OA
Loss joint space
Osteophytes
Sclerosis
Subchondral cysts

Treatment of OA
NON-OPERATIVE
- Weight loss
- Exercise/physio
- Analgesia/NSAIDs
- Joint injection
OPERATIVE
LOCAL complications of a hip replacement
Leg length inequality
Dislocation
Infection
Loosening (after 10-15 years)
Neurovascular damage...
- Sciatic/femoral nerve damage
- Common peroneal nerve TKRs
- Other nerves: inferior/superior gluteal nerves
SYSTEMIC complications of a hip replacement
UTIs/chest infections
Clinical DVT
Non-fatal PE
Fatal PE
Mortality
Frailty in the musculoskeletal system is often correlated with two other major geriatric syndromes, what are they?
Sarcopenia
Cachexia
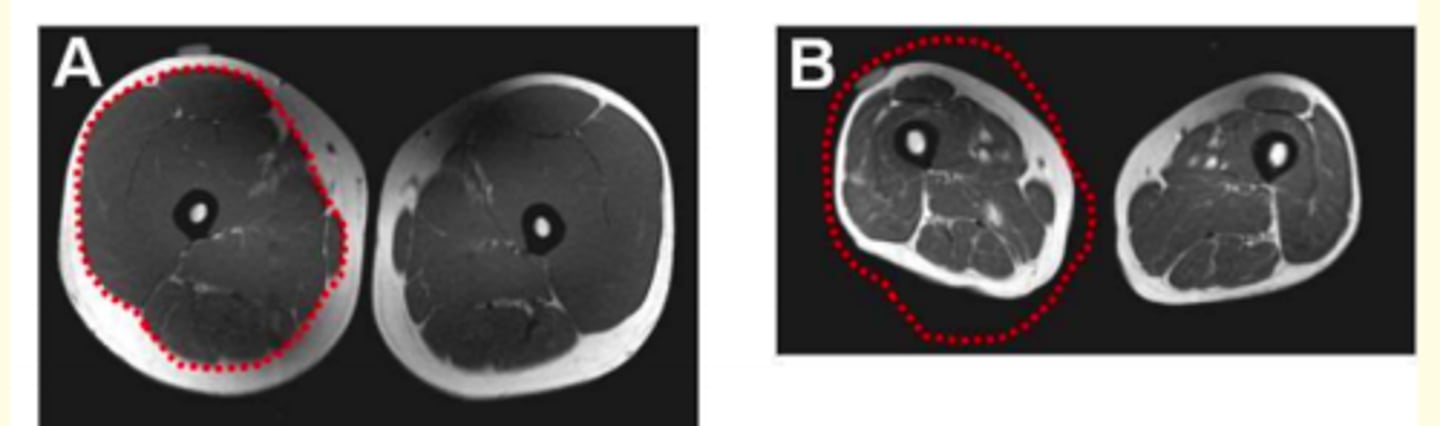
Sarcopenia
Syndrome characterised by progressive and generalised loss of skeletal muscle mass and strength, with a risk of adverse outcomes such as physical disability, poor quality of life and death
Diagnosis of sarcopenia
Diagnosis is based on documentation of criterion 1 plus (criterion 2 or criterion 3)
1) Low muscle mass
2) Low muscle strength
3) Low physical performance
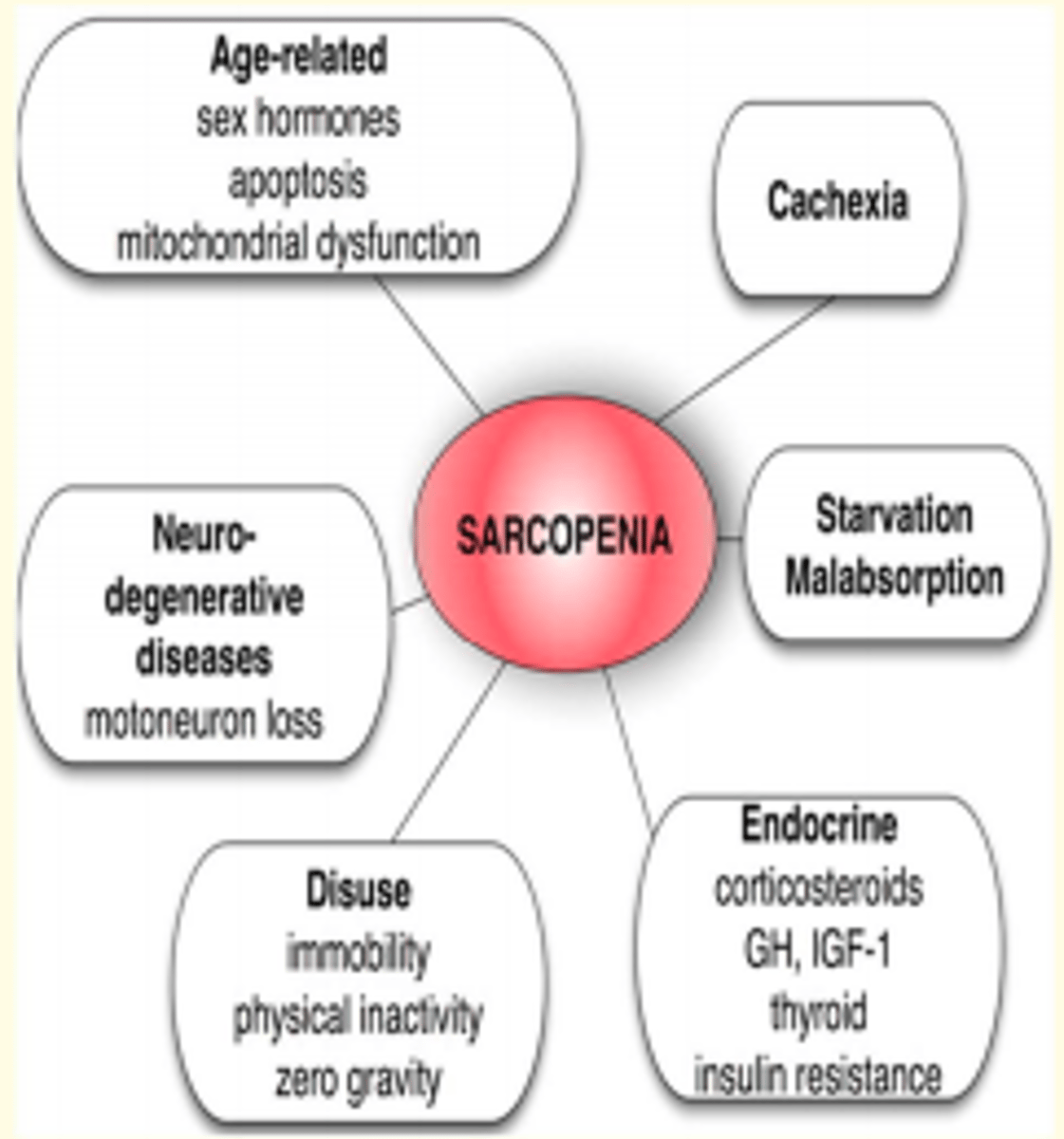
Pathogenesis of sarcopenia
- Muscle homeostasis is maintained in a delicate balance between new cell formation, hypertrophy and protein loss
- This balance is coordinated by the brain, endocrine system & immune system and is influenced by nutritional factors and levels of physical activity
- The adverse neurological, endocrine and immune components of frailty have the potential to upset this delicate homeostatic balance and accelerate the development of sarcopenia
Frailty
Frailty is a medical syndrome with multiple causes and contributors that is characterised by diminished strength, diminished endurance, reduced physiological function that increase individuals' vulnerability for developing increased dependency and/or death
What factors increase fall risk
- Decreased mobility
- MSK-related posture & gait changes
- Neuro-related gait & proprioception changes
- Environmental hazards
Potential interventions for frailty
1) Exercise = positive impact on MSK, endocrine and immune systems
2) Nutritional intervention = caloric and protein support and vitamin integration
3) Reduction of polypharmacy = STOPP and START criteria