Lec 21 - Prolactin and GH
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
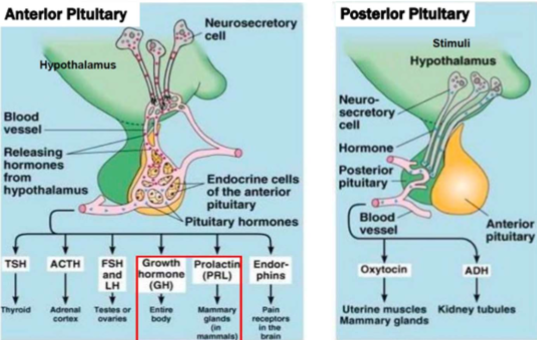
What parts of the pituitary gland does lactation require
Both anterior and posterior
- Anterior = prolactin
- Posterior = oxytocin
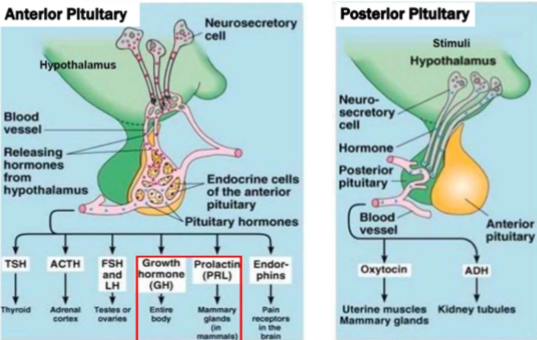
Where and what produces prolactin
Made by lactotrophs in anterior pituitary
Forms of prolactin in circulation
Monomer
Dimeric (big)
Macroprolactin -polymeric or immunoglobulin bound
Function of prolactin
- Pregnancy and lactation (breast milk production)
- uterine smooth muscle contractions
- Reproduction (sex hormone synthesis and fertility)
Specimen requirements and testing methods for prolactin
Serum or plasma (note TOC), tested via immunoassay
Gender variation of prolactin
Gender dependent - females secrete more than males
When are prolactin levels the highest
In the morning (pulsatile, diurnal variation)
Interferences of prolactin immunoassays
Non-specific immunoassays
Hook effect: high dose of antibody neutralizes ability for second Ab to do work = false neg (could be caused by MM)
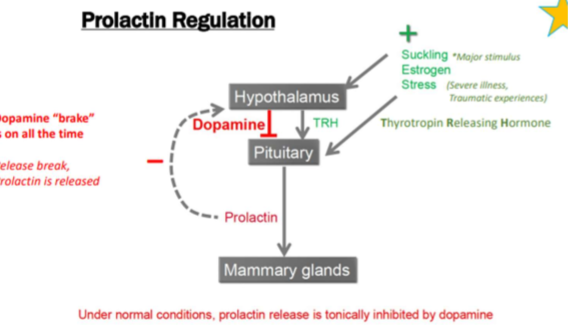
Effect of dopamine on prolactin
Inhibits prolactin released
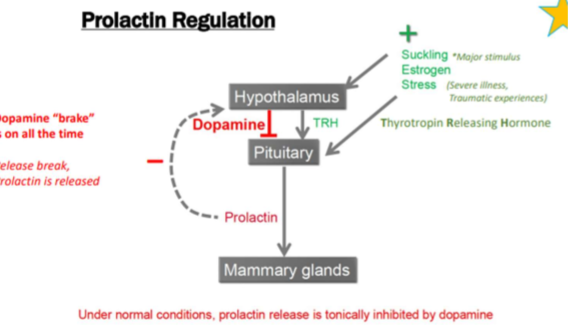
What causes increased secretion of prolactin
Suckling
Estrogen
Stress (severe illness, traumatic experience)
Thyrotropin releasing hormone (from the thalamus)
Physiological causes of hyperprolactinemia
Pregnancy, Breast feeding, stress, exercise, sleep
Non-physiological causes of hyperprolactinemia
- Prolactin secreting pituitary tumor
- Damage to hypothalamic pituitary dopamine path
- Medications
- Renal failure
- Liver disease
- Primary hypothyroidism (increased TRH)
- Macroprolactin
Clinical presentation
- Galactorrhea (breast discharge)
- Hypogonadism and infertility
- Low sex drive
- Headaches and visual problems
Hyperprolactinemia presentation in females
Menstrual dysfunction
Vaginal dryness
Hyperprolactinemia presentation in males
- ED
- Decreased body hair and muscle mass
- Delayed puberty
Diagnosis of hyperprolactinemia
Increased prolactin concentration in serum immnoassays
- if required, screen samples for macroprolactin (not bioavailable)
MRI - tumors
How to ID macroprolactin in samples
Gel filtration chromatography, PEG precipitation
Where is GH produced and secreted
Somatotrophic cells of anterior pituitary gland
What forms can be GH be found as
Monomer
Homodimer
Heterodimer
Multimer
GH distribution
50% Free, 50% bound to GH binding protein
Half life of Gh
20 mins - short
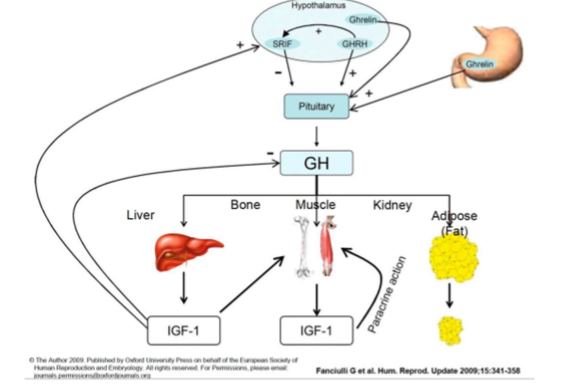
How is GH action mediated
Directly through growth hormone receptors on many tissues
Indirect action through hepatic insulin growth factor (IGF-1) release
Major functions of GH
- Tissue and bone growth
- Response to stress
- Modulates fat/carb/protein metabolism and body composition (decreases lipogenesis, increases lipolysis, amino acid uptake, glucose and protein synthesis)
- Raises glucose and FFA concentrations
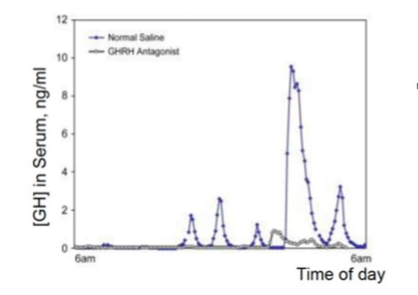
What impacts amount of GH secretion
- Pulsatile release with most release at night
- Circadian rhythm
- Influenced by age, sex, body composition
- Measured via immunoassay
Is GH testing common?
No - mostly use Insulin-like growth factor
What criteria is required for GH to be ran instead of IGF-1
1. Patients with acromegaly being monitored for therapy
2. Pre-approved endocrinologists
3. Pediatric patients less than 1 year old
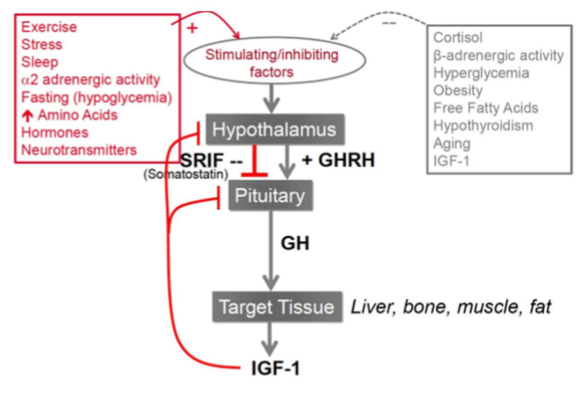
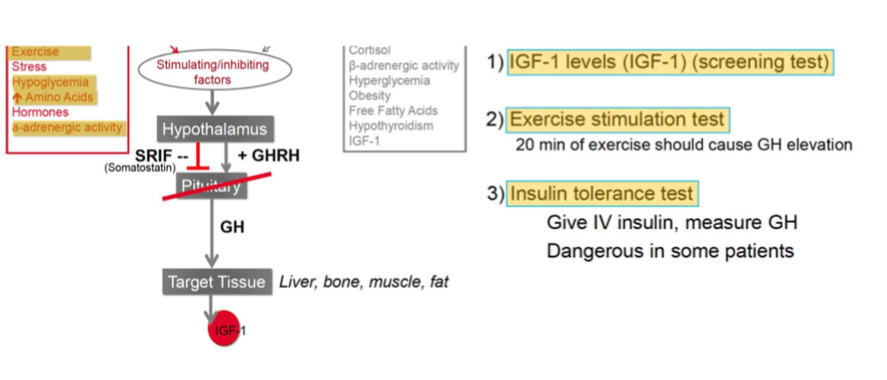
Positive influences on GH secretion
- Exercise
- Stress
- Sleep
- Fasting (hypoglycemia)
- AAs
- Hormones
- NTs
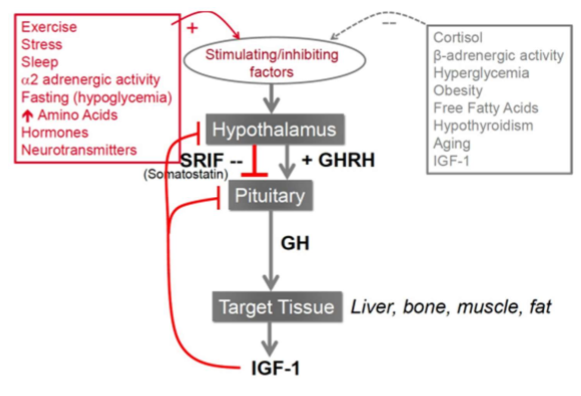
Negative influences on GH secretion
- Cortisol
- Hyperglycemia
- Obesity
- FFA
- Hypothyroidism
- Aging
- IGF-1: high amounts
Effect of GH on bone
Bone repair, stimulates osteoblasts

Effect of GH on Liver
Produces IGF-1
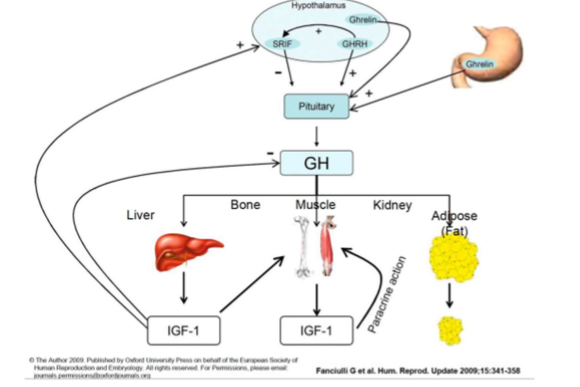
Effects of GH on fatty tissue
Promotes lipogenesis (FFAs for use)
Effect of GH on glycogen
Glycogenolysis - for sugar use
Where is IGF1 produced
Liver
Effect of IGF-1
Mediates indirect growth and fat metabolism effects of GH
Why is IGF a good marker for GH status
Fairly steady concentration throughout the day (good marker for GH status)
IGF reference ranges
Huge variation between and year
Causes of GH excess
Causes
- Pituitary tumors (adenoma)
- Hypothalamic lesions
- GnRH producing tumors
Effects of GH excess
Soft tissue, and bone overgrowth (gigantism in adults and acromegaly in adults)
Physicical features of kids with GH excess
Tall, long bones, large/coarse facial features
Physical features of adults with GH excess
- Large/coarse facial features
- Large organs
- Skin changes
- Osteoarthritis
- Hypertension
- Insulin resistance
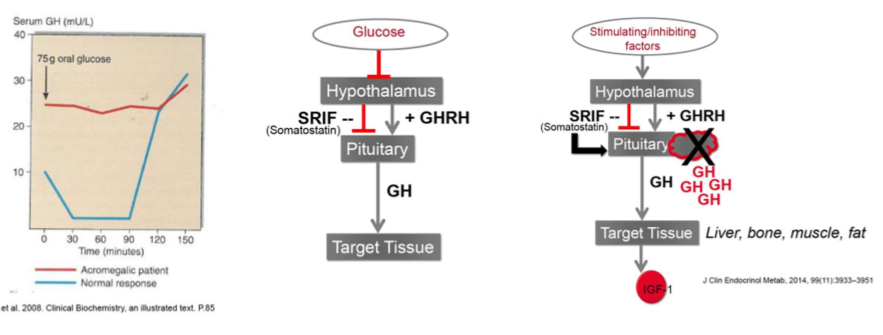
Lab testing of GH excess
1. Measure serum IGF-1 (screen)
2. Glucose supression test (give glucose, measure serum GH 2 hours post dose, should make GH undetectable)
3. MRI for tumor
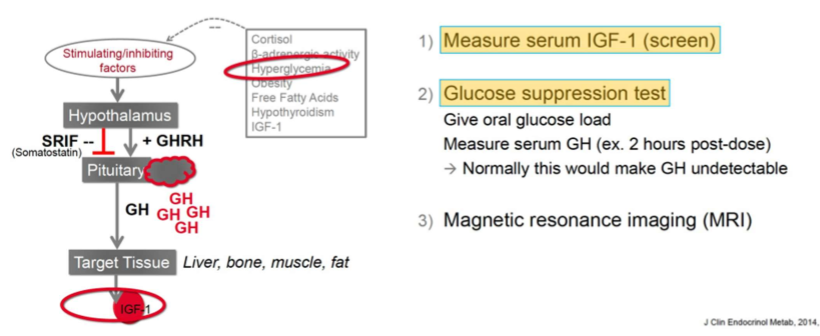
Should patients fast for glucose supression test
Yes
Causes of GH deficiency/resistance
Pituitary or hypothalamic abnormalities (deficiency)
GH insensitivity or resistance
Characteristic features in children with GH deficiency
- Low growth rate
- Short stature
- Central adiposity
- Susceptible to hypoglycemia
Characteristic features in adults with GH deficiency
- Decreased bone density
- Impaired serum lipids
- Abnormal body composition
- Premature mortality
Should you run glucose suppression test for GH deficiency?
No - only excess
GH deficiency lab testing
1. IGF-1 levels (screening)
2. Exercise stimulation test (20 min exercise should cause GH elevation)
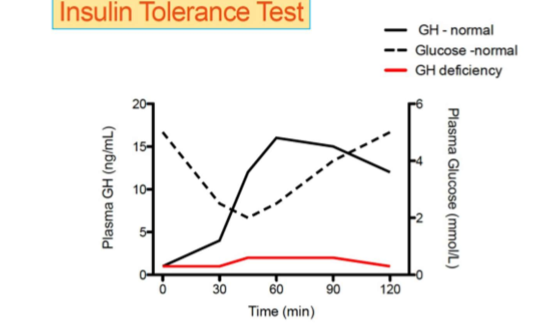
3. Insulin tolerance test (give IV insulin - can be dangerous in patients!)
Theory of Insulin tolerance test
Insulin makes someone hypglycemic - GH should increase to return glucose levels to normal
Theory of glucose suppression test
Giving glucose should suppress GH release in body. Failure to suppress GH release indicates acromegaly
How to treat GH deficiency
Treat with GH supplements (recombinant hGH)
hGH misuse
Athletes will take hGH to increase lipolysis, lean muscle mass, VO2 max.
Can also take EPO