lec 28 - sodium and water
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
17 Terms
important places for sodium reabsorption
PCT (66%) - SGLT (glucose), Na+/H+ exchanger (NHE), trans and paracellular
TAL (25%) - Na+/K+/2Cl- co-transporter (NKCC2), trans and paracellular
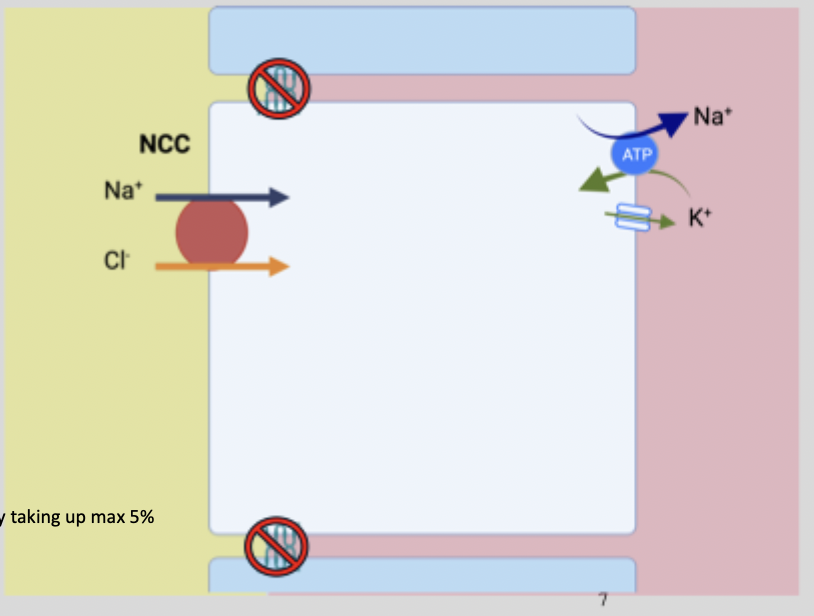
DCT (5%) - Na+/Cl- cotransporter, transcellular only
CCT (3%) - ENaC, transcellular only, hormonal control - aldosterone
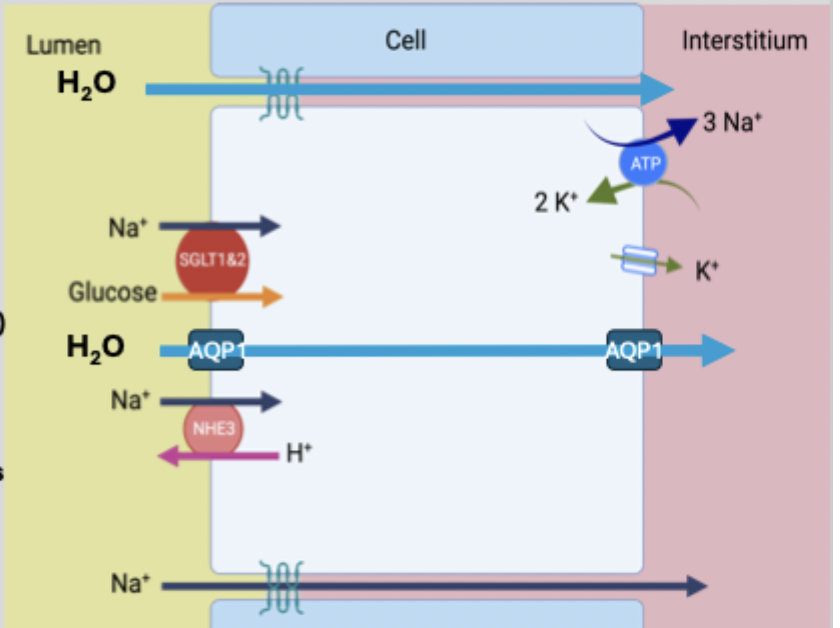
sodium re-absorption - PCT
66%
leaky epithelium - tight junction permeable to Na+ and water
trans- and para- cellular re-absorption of Na+
isotonic reabsorption (equal amounts of sodium and water)
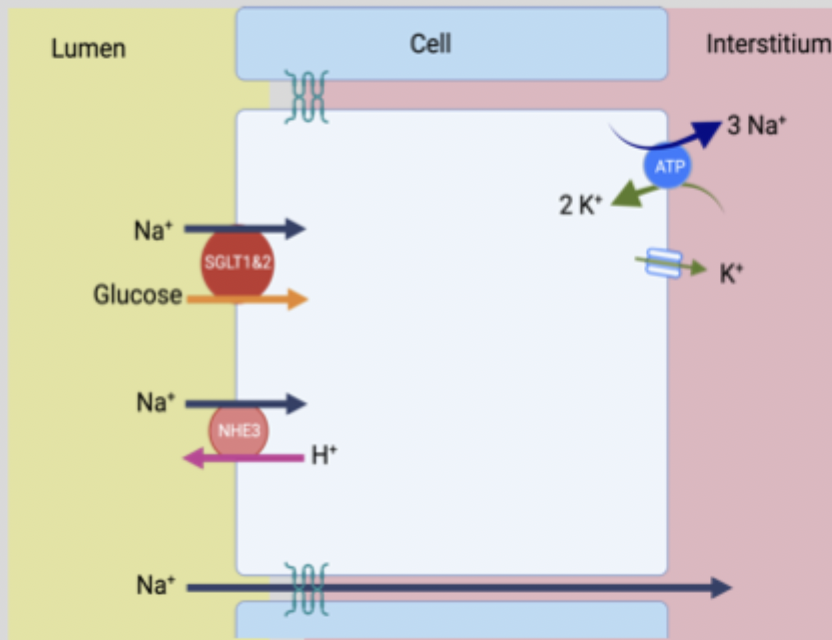
note that chloride will follow the sodium
sodium reabsorption in the TAL
25%
semi-tight epithelium - only permeable to Na+/not permeable to water
trans and para cellular reabsorption
loop diuretics (furosemide) inhibit NKCC2, increase diuresis
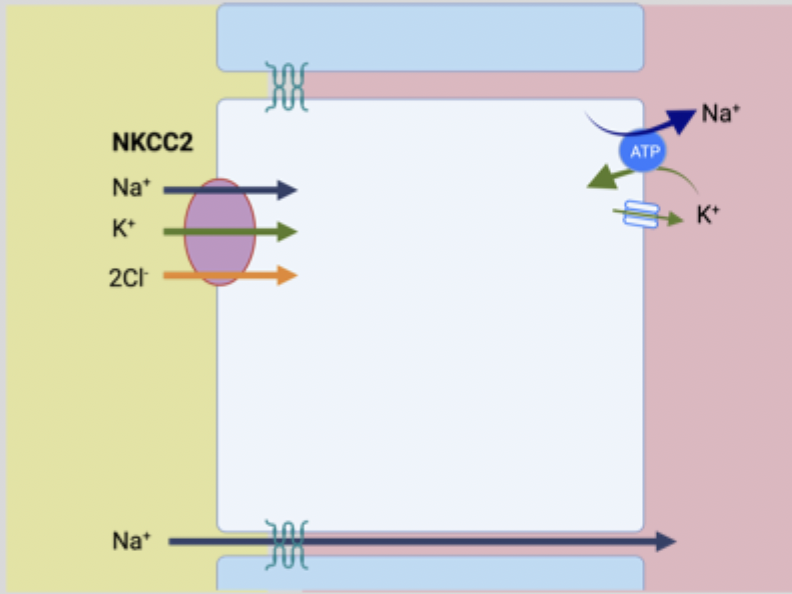
note there is also potassium channels at apical surface to make sure there is enough potassium for the transporter
sodium reabsorption in the DCT
5%
tight epithelium
transcellular re-absorption of Na+ (no paracellular transport)
diuretics (thiazides) inhibit NCC = mild diuresis
filtered sodium reabsorption in the CCD
3%
tight epithelium
transcellular reabsorption of Na+ (no paracellular transport)
regulated by aldosterone - increases ENaC expression and insertion into membrane
upregulates Na/K ATPase
diuretics (amiloride) inhibit ENaC, very mild diuresis
aldosterone
from the zona glomerulosa of the adrenal gland
binds to minerocorticoid receptor
alters gene expression
upregulation of ENaC and Na+/K+ATPase
de nvo synthesis of ENaC, Na+/K+ATPase and other proteins (genomic effects)
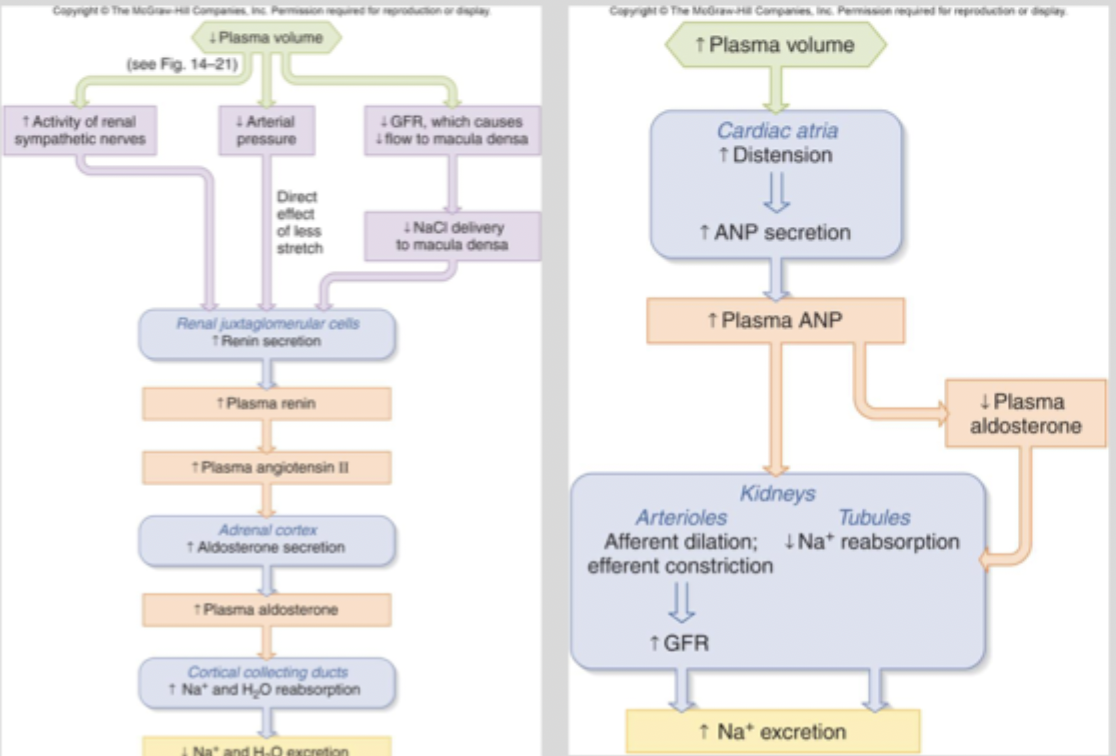
how does aldosterone get turned off
high plasma volume results in the release of ANP from cardiac atria
high plasma ANP levels reduce plasma aldoterone, increase GFR, reduce Na+ reabsorption, increase Na+ excretion
important places where water is reabsorbed
PCT - 66%
loop of henle - 25%
CD - ~2-8%
aquaporins throughout the nephron
AQP1 in PCT and descending thin limb - both apical and basolateral
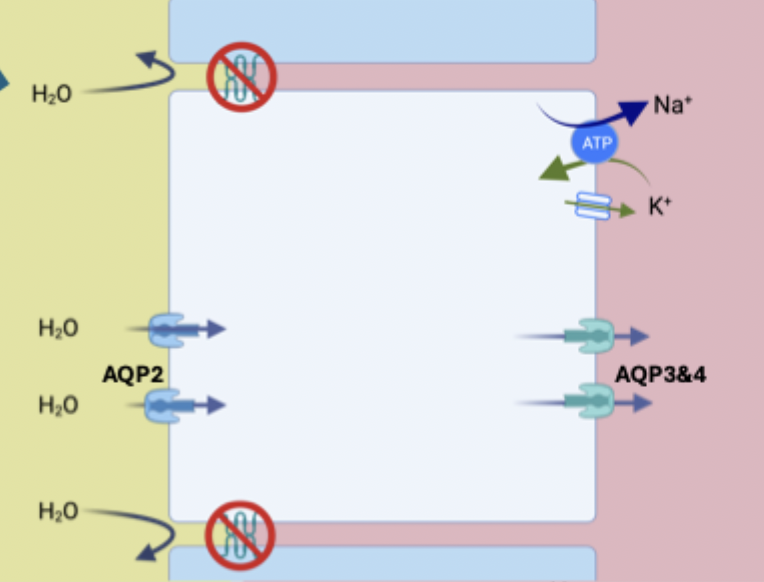
CCD - AQP2 in the principal cells of collecting duct - apical membrane, AQP3 in the prinicpal cells basolateral membrane
AQP4 - inner medullary collecting duct, basolateral membrane
water reabsorption - PCT
66% of filtered load
driven by Na+ reabsorption - isotonic
transcellular via AQP1, paracellular via leaky tight junctions
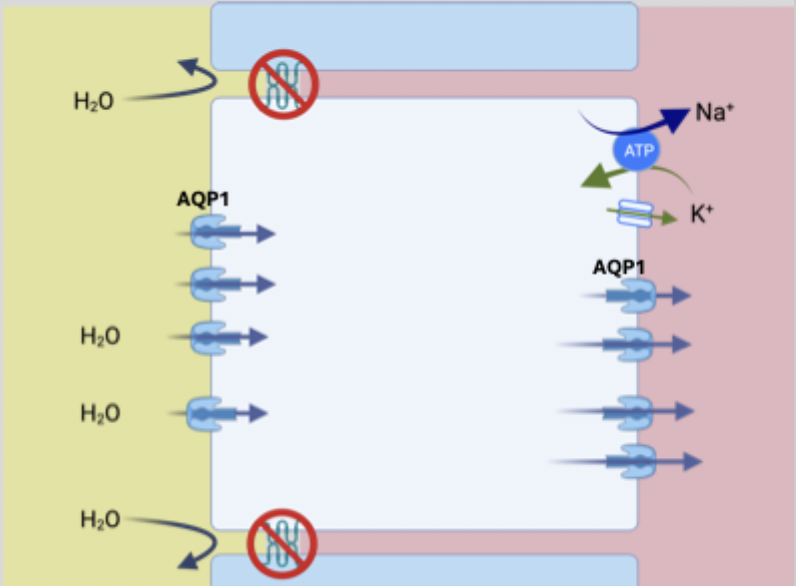
water reabsorption in th thin descending loop of Henle
transcellular re-absorption of H2O
high levels of AQP1
secondary bulk reabsorption, more regulated, AQP1, transcellular not paracellular
water reabsorption - collecting duct
tight epithelium - no paracellular transport, no unregulated transport
water reabsorption in the prinicipal cell of the CCT is regulated by ADH (vasopressin)
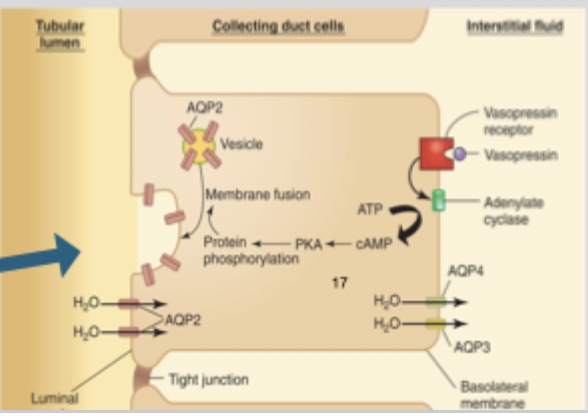
hormonal control of water reabsorption in the CCT
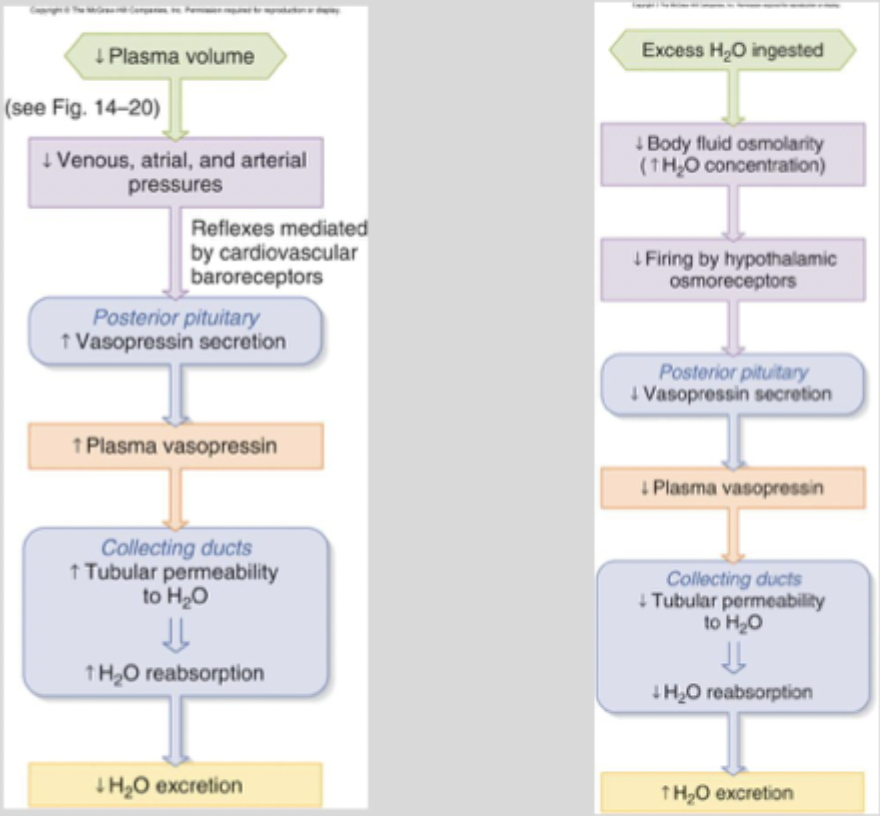
ADH released in response to low BP (baroreceptors), high blood osmolarity (osmoreceptors), increased ATII
circulating ADH binds to V2 receptor on basolateral membrane of CD cells
activated adenylyl cyclase, increased cAMP, activates PKA, phophorylation leads to sub-apical AQP2 vesicles moving to membrane via exocytosis
increased apical membrane water permeability
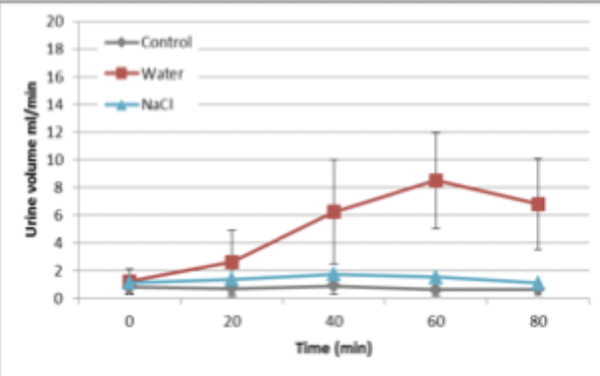
water homeostasis
we have a fast and slow system to regulate water homeostasis
fast: reacts to changes in osmolarity
slow: reacts to changes in volume
overall water and Na+ reabsorption diagram

water reabsorption and vasopressin diagram
renal sodium regulation summary
high plasma volume results in the release of ANP from cardiac atria
high plasma ANP levels reduce plasma aldosterone, increase GFR, reduce Na+ reabsorption, increase Na+ excretion