BPK 241 Lecture 8
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
Hip Bone
Femur
Pelvis
Innominate
Iluim (superiorly)
NB., ASIS, AIIS, crest
Ischium (inferior posterior)
Pubis (inferior anterior)
NB., ramus, symphysis
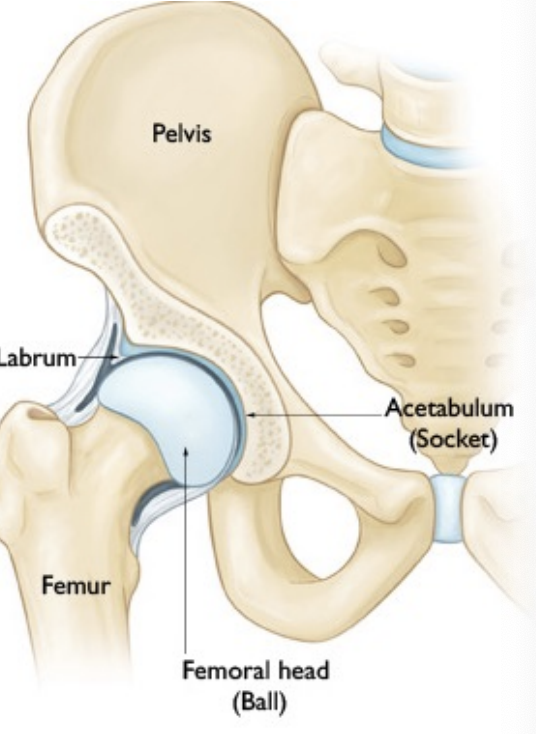
Hip Articulation
Head of femur with acetabulum
Socket deepened by acetabular labrum
Ball & socket joint
Synovial joint
Capsule

Labrum
Tough fibrous material (tough cartilage)
Hold on to head of femur
Distribute force

Avascular Necrosis
A condition that occurs when bone tissue dies due to lack of blood supply

Hip movement
Circumduction
Flexion & extension
Abduction & Adduction
Internal & external rotation
Flexion/ Extension
120º of flexion and 20º-30º of extension
Abduction/ Adduction
50º of abduction and 20º-30º of adduction
Internal/ External Rotation
45º external and 35º internal
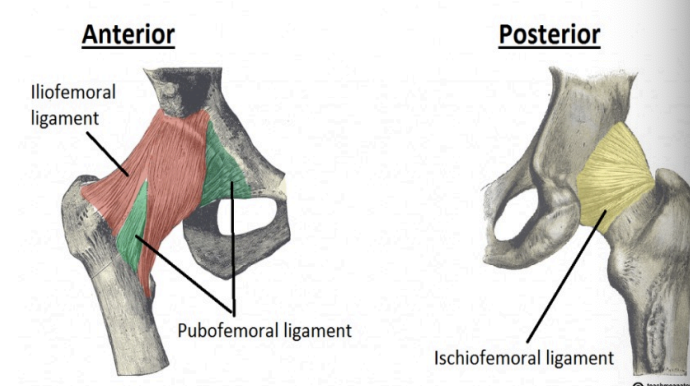
Capsule = ligaments
Iliofemoral
Ischiofemoral
Pubofemoral
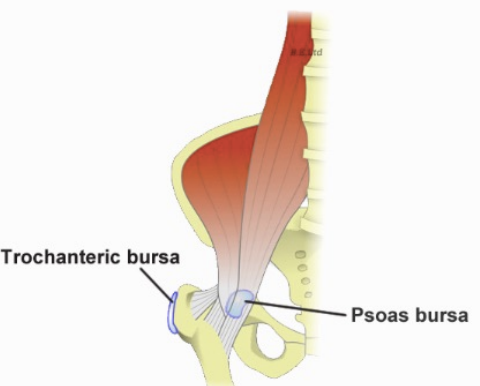
Bursae
Iliopsoas
Trochanteric
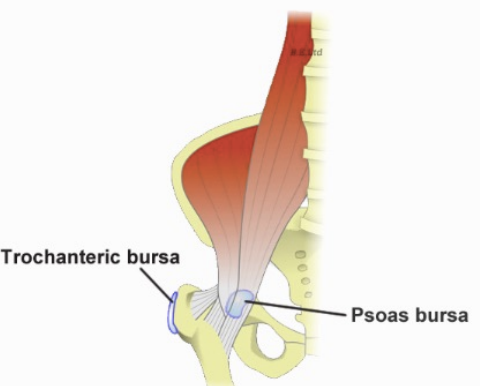
Iliopsoas bursae
Between iliopsoas muscle and anterior joint capsule
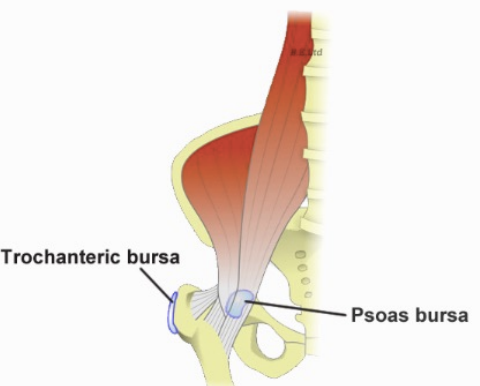
Trochanteric bursae
Between greater trochanter of femur and gluteus maximus muscle
Hip Sprain & Strains
Hx:
Violent torsion or extension
Hip flexion is resistant (iliopsoas strain)
SSx:
Deep pain, worse with movement
Tx:
Rest, NSAID, physiotherapy
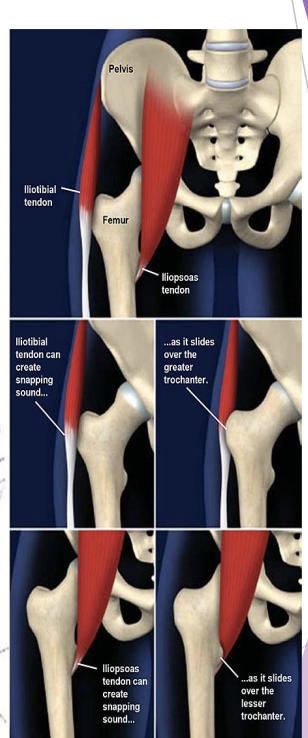
Subluxation vs Snapping Hip
Tendon sliding on a bump
Gymnastics, dancing, martial arts (shallow acetabulum?)
Often chronic; may lead to osteoarthritis
Tx=rest, exercises
Change activity
symptomatic?
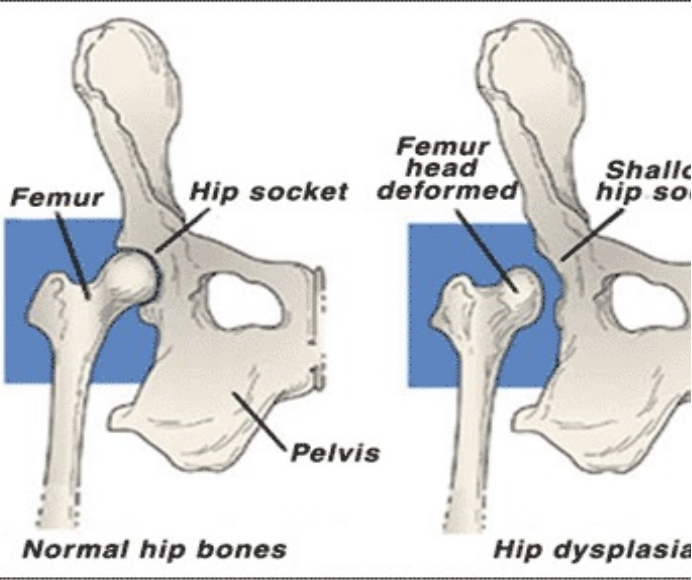
Hip Dysplasia
Checking for subluxation
Hip Bursitis
Hx: overuse or direct blow
SSx = tenderness, pain on movement
Tx = POLICE, NSAID, rest, physiotherapy

Labral Tear
Shearing, excessive forces at hip joint (internal rotation)
Hip Labrum pulls away from acetabulum
SSx: Deep groin/ buttock pain
Pain/stiffness moving hip in certain directions
Feeling clicking/locking when moving hip joint

3 Main causes of Labral Tear
Trauma (ie. MAVA)
Hip abnormalities (hip dysplasia, FAI)
Repetitive movements (most common)
Twisting (ie hockey/golf)
Extreme end range movements (ballet, gymnastics)
Repetitive joint loading (marathoners)
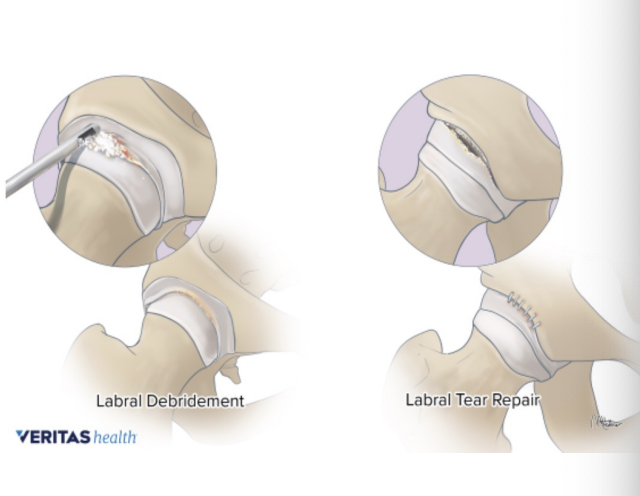
Labral Tear Treatment
Conservative
Rest, NSAIDs, injections, physiotherapy
Surgical
Arthroscopic labral debridement
Arthroscopic labral repair
Arthroscopic labral replacement
Labral tear predisposes athlete to articular cartilage degeneration, osteoarthritis
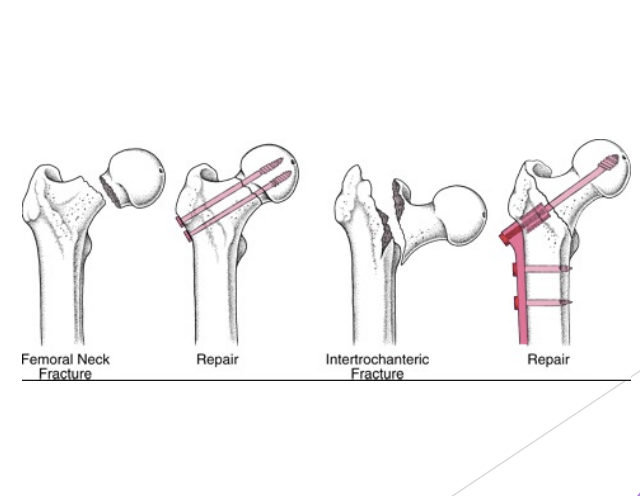
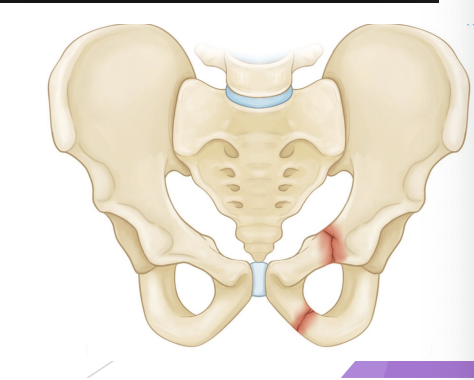
Fracture/ dislocation
Hx: severe trauma (MVA), or elderly person (neck or femur)
SSx: extreme pain, markedly reduced ROM, deformity (may not be present)
Tx: recognize, stabilize, transport (NPO)
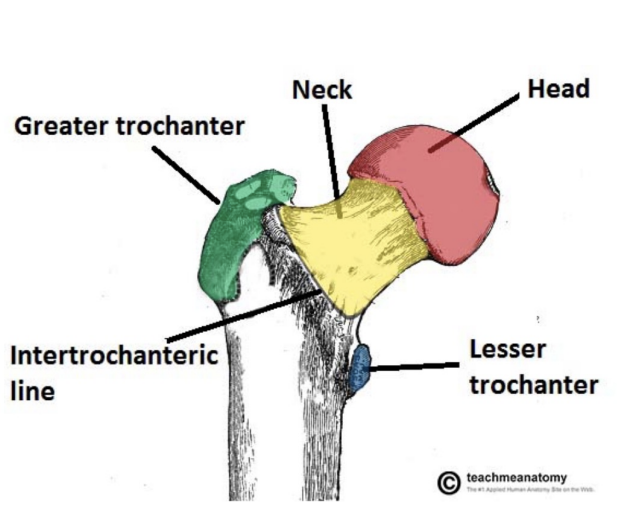
Thigh Bone
Femur
Head, neck, greater & lesser trochanters, shaft, condyles
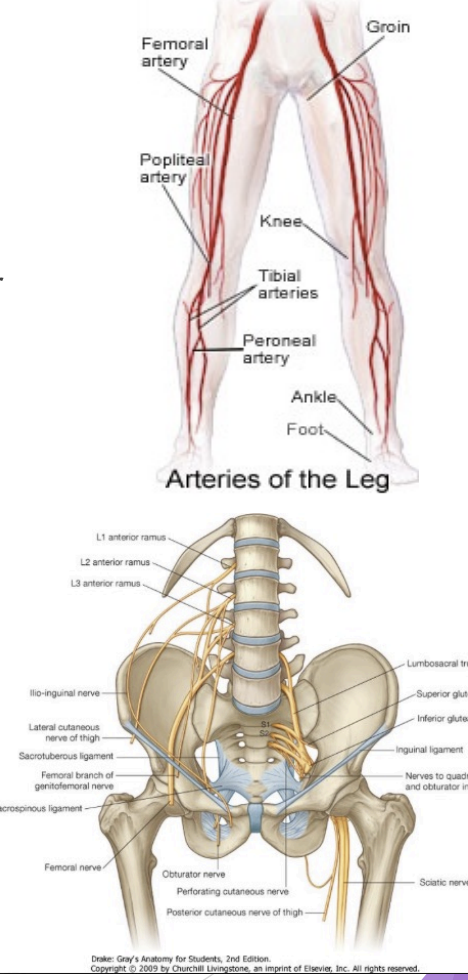
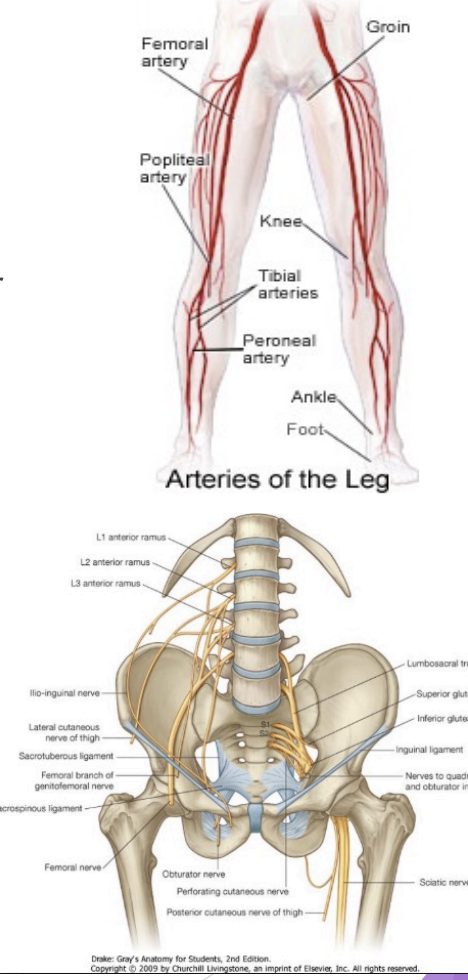
Thigh Artery
Femoral
Becomes popliteal artery
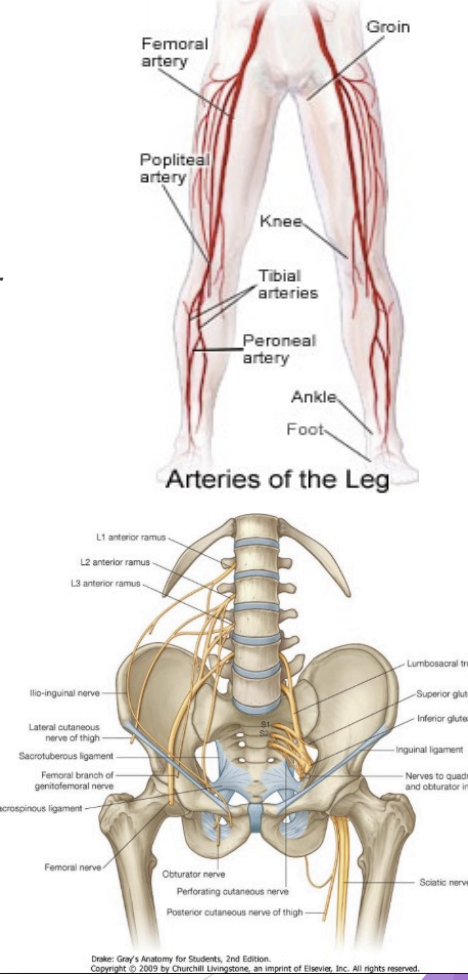
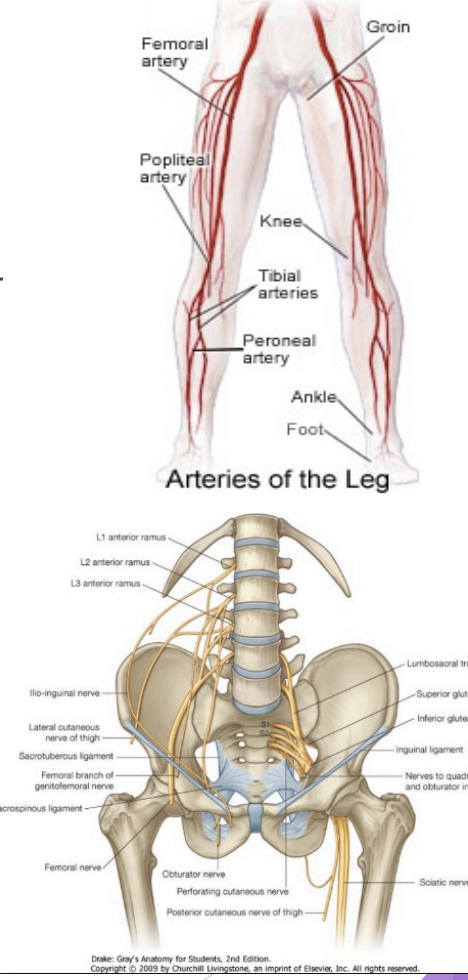
Thigh Nerves
Femoral (L2 - L4 nerve roots)
Sciatic (L4 - S3 nerve roots)
Thigh Muscles
Anterior
Quadriceps femoris
Posterior
Hamstring
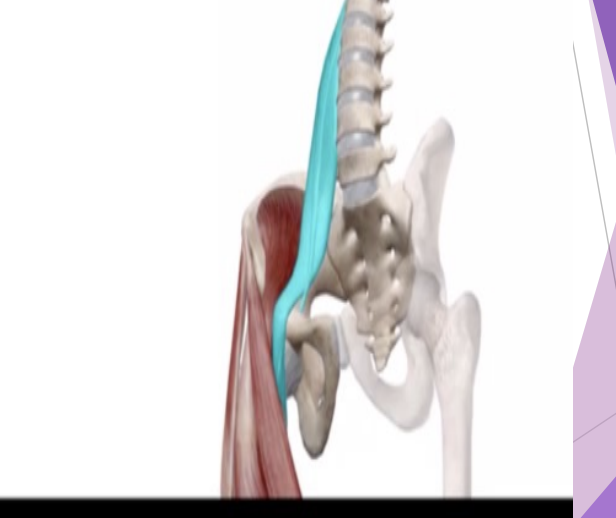
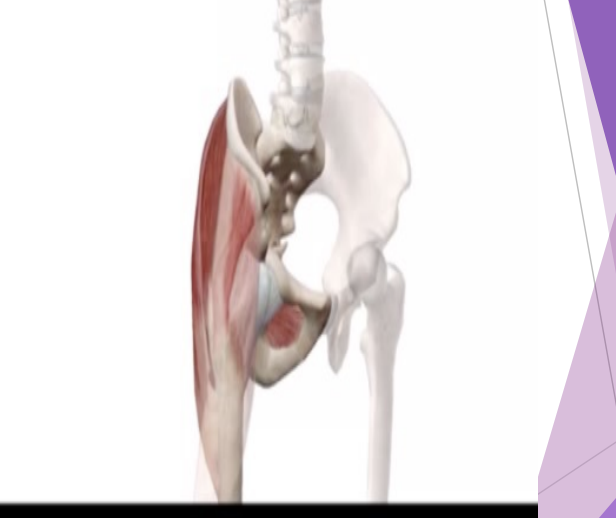
Hip/Thigh Flexors
Iliopsoas
Illiacus
Psoas (come off lumbar vertebrae)
Rectus femoris
Sartorius (largest in body)
Hip/Thigh Extensors
Gluteus Maximus
Hamstrings
Hip/Thigh Adductors
Adductor
Longus
Brevis
Magnus
Pectineus
Gracilis
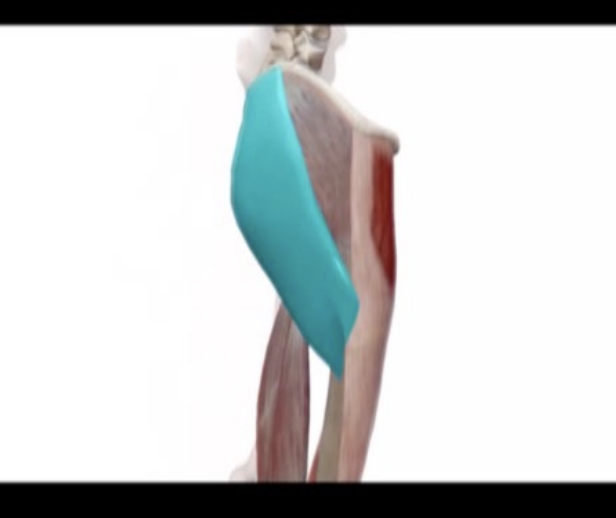
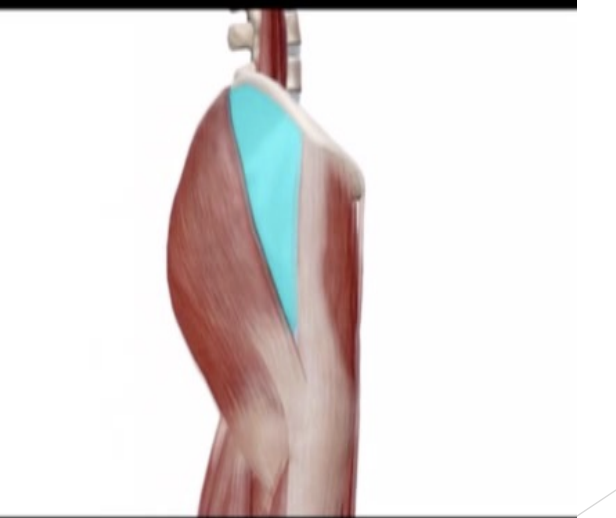
Hip/Thigh Abductors
Gluteus Medius
Gluteus Minimus
Tensor Fascia Latae (TFL)
Gluteus Maximus
Others: Hip rotators are intrapelvic
Hip External Rotators
Piriformis (sciatic nerve under it - if tight, it can pinch nerve)
Obturator externus and internus
Superior and inferior gemellus
Quadratus femoris
Hip Internal Rotators
TFL
Gluteus medius (anterior fibres)
Adductors
Pectineus
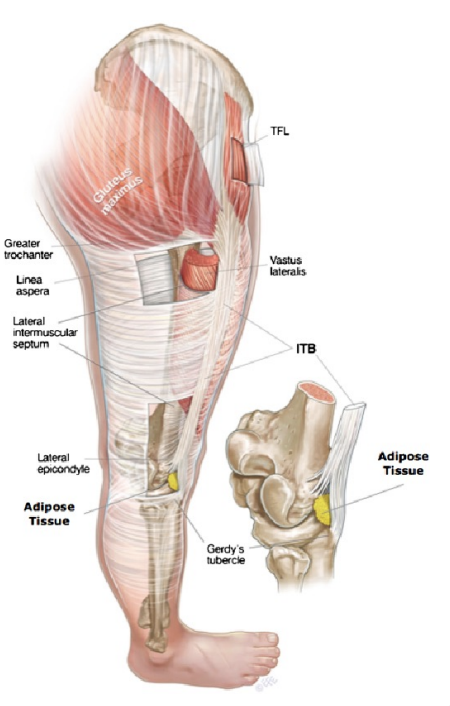
Iliotibial Band (ITB)
The ITB is not a single band but a lateral thickening of the fascia latae - similar to a stocking
The source of pain is from a richly innervated and vascularized layer of fat and connective tissue between ITB and lateral epicondyle
Hip Contusion
Hx: direct blow
SSx:
Pain, bruising
Tenderness/ firm on palpation
Swelling (circumscribed?)
Decreased ROM
Limp
Tx:
POLICE
NO heat NO massage directly over contusion
Padding
ROM exercises & physiotherapy
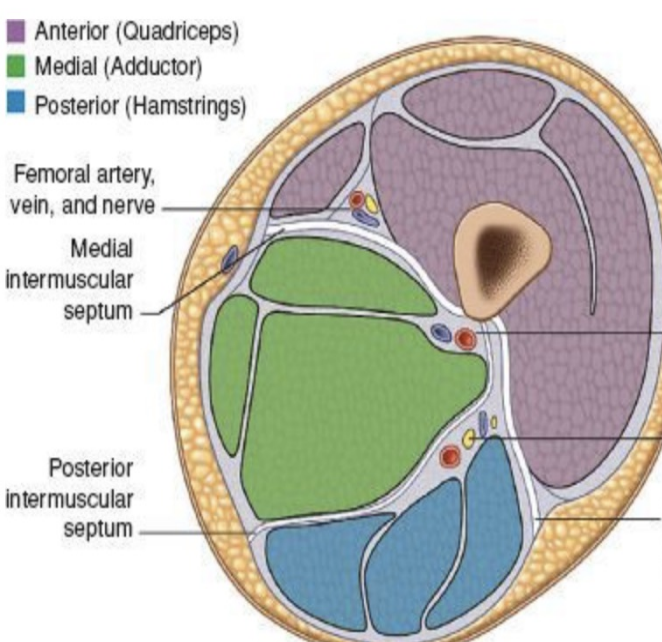
Thigh Compartments
Thigh divided into 3 compartments by intermuscular septa
Anterior (quadriceps)
Medial (adductors)
Posterior (Hamstrings)
Anterior Compartment:
Quadriceps muscle group
Primary knee extensors
Rectus femoris
Vastus lateralis
Vastus intermedius
Vastus medialis
Posterior Compartment:
Hamstring muscle group
Primarily knee flexors
Biceps femoris
Semitendinosus
Semimebranosus
Medial Compartment: Adductor Muscle Group
Adductor Muscle Group
Adductor magnus
Adductor longus
Adductor brevis
Pectineus
Gracilis

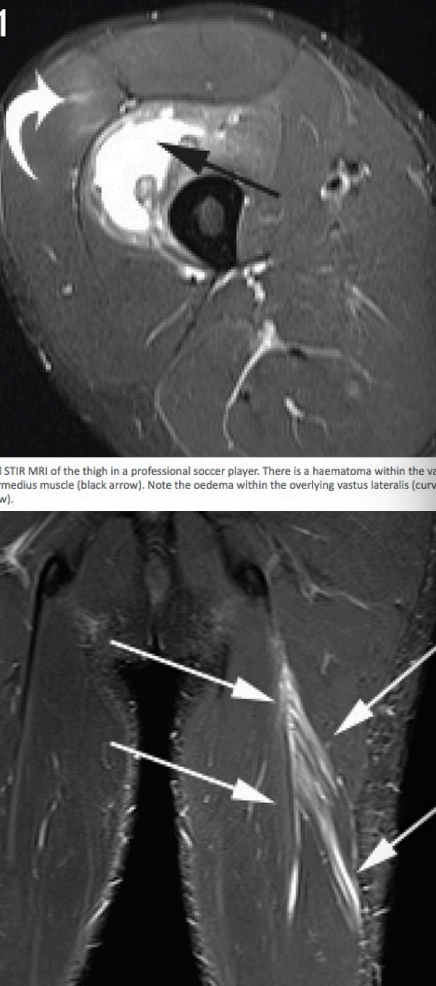
Myositis Ossificans
Several contusions or mishandling of severe contusion
ROM not returning after Quad contusion
Thigh firm on palpation several weeks to months later
Send for imaging
Thigh Strain
Hx:
Resisting a force, torsion, hyperextension, abduction
Predisposed by decreased strength or flexibility, previous strains
SSx:
1st degree
Pain (worse with resistance)
Tenderness
No limp, snap or pop
2nd degree
Pain & tenderness, bruising
Snap or pop felt/heard
Limp
3rd degree
As above, & gap in middle

Thigh Strains Treatment
1st degree
POLICE
ROM exercises, tape (compression wrap)
2nd degree
As above
Rest for 2 to 6 weeks
Physiotherapy & rehabilitation
3rd degree
NPO
Stablize
Transport to hospital (surgery)
Rest, physio, rehabilitation

Hamstring Strains
Causes
Inflexible
Improper warm up
Temperature
Fatigue
Violent contraction
Tx: POLICE, rest, stretching delayed, strengthening (eccentric), gradual return to activities, hamstring tensor wrap/core shorts

Iliotibial Band Friction Syndrome
Clinical features
Subjective: ache on lateral aspect of the knee - worse with cycling, downhill running
Objective:
TOP (tenderness on palpation) over lateral femoral epicondyle
+ve Ober’s
w or w/out burning sensation
Overdeveloped Vastus Lateralis
Overpronation - increased tibial rotation
Increased internal femoral rotation/ genu valgrum
ITBFS Treatment
Pathology is distal but often need to treat proximal
Exercise therapy similar to PFPS
strengthen hip abductors
Release GluteMax, TFL, vastus lateralis
Soft Tissue Release (Massage, Foam Rolling, Stretch)
Dry Needle
Thigh Fracture
Femoral fracture
Major trauma
SSx: severe pain, inability to weight bear
Tx: stabilize, NPO, get to hospital ASAP
Surgery, internal fixation with rod or plate
Rehab: gradual progression of ROM and strengthening/progressively weigh bearing over 4 to 6 months
Scrotal contusion
Pain subsides over five minutes
Tx = hip flexion, gentle breathing
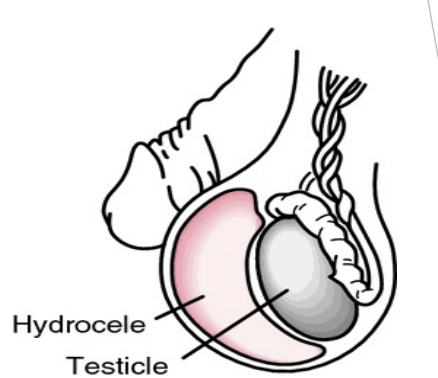
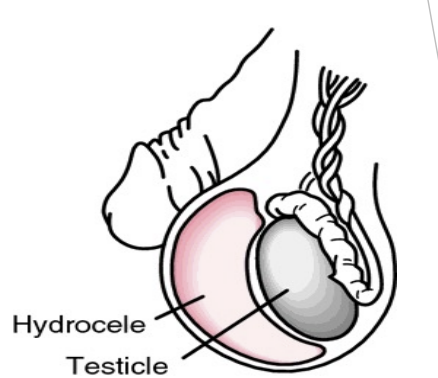
Traumatic Hydrocoele
Delayed complications of contusion (days, weeks, months)
Appearance of cluster of swollen veins
Tx = surgical, if warranted
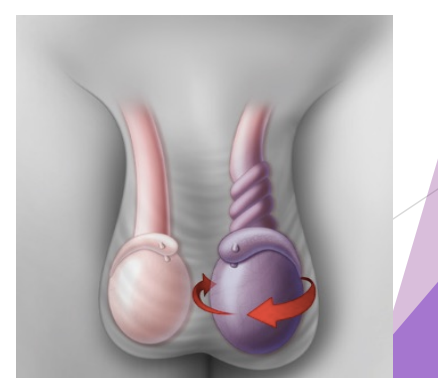
Torsion of spermatic cord
Pain increases over time
Nausea, vomiting
Shock (rapid HR & RR; clammy skin)
Swelling, extreme tenderness
Surgical emergency
NPO, transport ASAP
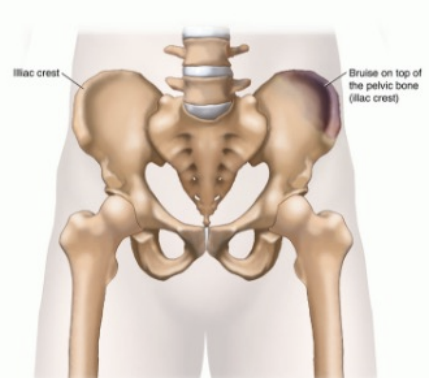
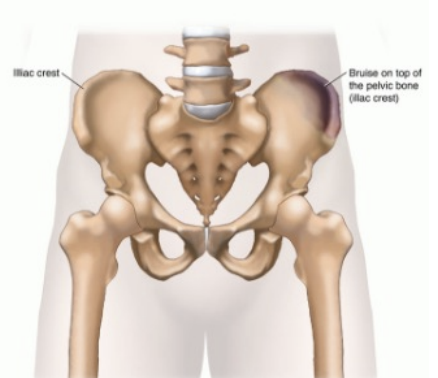
Hip pointer
Hx = contusion of iliac crest
SSx:
Pain, tenderness, bruising
Circumscribed swelling, limp
Difficulty with flexing thigh or rotating trunk
Tx:
Ice , rest, padding, physio
Coccygeal contusion
Hx = direct blow (fall,kick)
SSx:
Pain, bruising, tenderness
Tx:
Hospital for X-Ray
NSAID, warm baths
May need surgery