Speech Disorders Across the Lifespan Exam 2
1/65
Earn XP
Description and Tags
Exam 2
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
66 Terms
What should be included in a comprehensive speech-language pathology evaluation?
phonological assessment - assessment of voice quality, fluency, all areas of language, resonance, hearing, oral mechanism, and case history.
What are the goals of speech sound analysis?
1) determining if the speech sound system is “normal” or warrants intervention, 2) determining factors related to the disorder/ delay, 3) determining treatment direction and selecting targets, 4) making prognostic statements, and 5) monitoring progress.
What is the difference between relational and independent analysis?
Relational analysis refers to an analysis of speech sounds where they are compared to the adult or target form of sound productions. This is the most commonly used approach and the approach that is used within most standardized assessments.
Independent analysis refers to an analysis of speech sounds without comparison to the target sound or intended production. Independent analyses are most commonly used with individuals who are very young or who have limited phonological repertoires. When collecting a speech sample from a child who is unintelligible, it is helpful to transcribe the phonemes that the child is producing, without regard to whether they are used appropriately in target word(s).
What is the purpose of an oral mechanism exam?
to determine if there is a possible structural or functional basis to the speech sound disorder
Why is the GFTA-3 considered a standardized, norm referenced test?
because it gives you information about how the child performs compared to their peers
Why is the purpose of stimulability testing?
helps SLP understand how easily a child can learn to say a speech sound correctly, which is useful for determining how severe a speech sound disorder is, deciding which sound to target in therapy, and predict whether the child might improve without therapy (valuate how well a child can imitate a speech sound)
Why does stimulability matter?
High stimulability means the child might learn the sound quickly in therapy or even develop it on their own over time.
Low stimulability means the child may need more support and targeted therapy to learn the sound.
How does stimulability impact target selection (what SLPs would work on)?
Stimulability testing helps SLPs understand how easily a child can learn to say a speech sound correctly. It is useful for:
Determining how severe a speech sound disorder is.
Deciding which sounds to target in therapy.
Predicting whether the child might improve without therapy.
if a child can repeat a sound relatively easily that sound can be focused on first before moving onto the ones they are having a difficult time with
Define dose, frequency, and duration as it relates to treatment intensity.
dose- number of strategies per minute
Frequency- number of sessions per week
Duration- Length of each session
Why should SLPs include both speech sample analysis and standardized tests to assess speech sound production abilities?
some children may:
Be hesitant to talk, making it hard to gather enough data.
Avoid saying words that contain difficult sounds.
Have speech that is difficult to understand, making analysis challenging.
Not use all the speech sounds a clinician needs to assess.
AND
Captures natural, connected speech rather than isolated words.
Helps determine if errors are part of typical development, a phonological process, or a disorder.
Evaluates how well a child's speech is understood across different contexts.
Prevents misdiagnosis by considering dialects and bilingual language patterns.
Provides a starting point for treatment and allows SLPs to track improvement over time.
(Captures natural speech instead of just isolated words, allows clinician too hear speech in different contexts, and also with just speech analysis child may be more hesitant to speak and say difficult words
How might it affect a child if they only produce two sounds - all vowels but struggles with consonants
might be phonological if unable to make sounds
what is percent consonant correct mainly measure
how severe is disorder
phonological assessments must include these things (especially 2 for speech)
must have oral mech and hearing screening as well as voice quality, fluency all areas of language, resonance, and case history
minimal pair is only ______
is only stopping
phonological assessments are done as a part of comprehensive speech-language evaluation, which typically includes assessment of
voice quality, fluency, all areas of language, resonance hearing, oral mechanism, and case history
What are some goals of a speech sound assessment
determining if the speech sound system is “normal” or warrants intervention, determining factors related related to the disorder/delay, determining treatment direction and selecting targets, making prognostic statements, and monitoring progress
The Goldman-Fristoe Test of Articulation
standardizes assessment designed to evaluate a person ability to produce speech sounds in English. It assess articulation skills in child and young adults.
Purpose of GFTA- 3
Identify articulation errors in a child’s speech
Determine which sounds are misarticulated (substitution, omissions, distortion)
The GFTA consists of three sections:
sounds in words
sounds in sentence
stimulability testing
what is Sounds-in-Words (GFTA)
the main portion of the test
the child names picture while the clinician records and mispronunciations or errors in speech sounds
targets inital, medial, and final position sounds in words
What is Sounds-in-Sentences (GFTA)
assesses speech in connected speech
the child listens to a short story and then retells it using pictures for support
helps evaluate articulation in longer, more natural speech
what is Stimulability Testing (GFTA)
Stimulability testing helps SLPs understand how easily a child can learn to say speech sound correctly. it is is useful for
determining how severe a speech sound disorder is
deciding which sounds to target in therapy
predicting whether the child might improve without therapy
(GFTA) How is stimulability tested
The SLP asks the child to repeat a sound or word they previously mispronounced
if the child can say the sound correctly after hearing a model, they are stimulable for that sound
if the child cannot say the sound correctly, the SLP provides extra support (visual cues, slower speech)
The level of help the child needs shows how much scaffolding is required to learn the sound
why does stimulability matter
high stimulability means the child might learn the sound quickly in therapy or even develop it on their own time
low stimulability means the child may need more support and targeted therapy to learn the sound
Debate in research: What should SLPSs Work on
Some believe clinicians should work on only stimulable sound because these are sounds the child is already “ready” to learn
Others argue that targeting no-stimulable sound can help the child improve overall, as stimulable sounds might develop naturally
What is a standardized norm-referenced - types of scoring
an assessment that is administered and scored in a consistent manner across all individuals.
Raw Scores
Standard Scores
Percentile Ranks
Confidence Intervals
Severity rating based on standard scores
standardized norm-referenced - raw scores
the raw score is the initial score calculated based on correct and incorrect responses
it had no meaning on its own until it is converted into standardized values
standardized norm-referenced - Standard Scores
compare and individuals performance to the normative sample (group of same-age peers who took the test) Most tests have a mean of 100 and a standard deviation of 15.
85-115- average range
78-84 - mild delay or disorder
70-77 -Mild moderate delay or disorder
60-69 -moderate delay or disorder
below 60 - severe delay or disorder
standardized norm-referenced - percentile ranks
a percentile rank indicates the percentage of individuals in the normative sample who scored lower
a 50th percentile rank means the individual
a 7th percentile rank means they scored better than only 7% of peers, which is below average
standardized norm-referenced - confidence intervals
confidence intervals show the range of scores when a person’s true likely falls
Example: if a child scores 85 with a 90% confidence interval of 80-90, we can be fairly certain that their true ability lies in that range
standardized norm-referenced -severity ratings based on standard score
Standard Score | Severity Rating |
85 - 115 | Average |
78 - 84 | Mild Disorder |
70 - 77 | Mild-Moderate Disorder |
60 - 69 | Moderate Disorder |
Below 60 | Severe Disorder |
should standardized tests be the only measure of assessing communication skills
No , they should be used alongside observations of the client in the different settings, Parent/teacher/caregiver reports, Language samples and informal assessments
Strengths and limitations of standardizes tests
Reliable comparisons: Helps compare individuals to same-age peers.
· Objective and standardized: Ensures fair and consistent testing conditions.
· Provides benchmarks: Helps determine eligibility for services (e.g., a child scoring below the 10th percentile may qualify for therapy).
Limitations:
· May not reflect real-life communication: A child might score poorly but communicate well in everyday life.
· Cultural and linguistic bias: Many tests are normed on monolingual English speakers, which can disadvantage bilingual or dialectal speakers.
· Does not account for environmental factors: A child might struggle due to anxiety, inattention, or unfamiliarity with the test setting.
what does the Khan Lewis phonological analysis assess
evaluate phonological processes in children. designed to be used alongside the Goldman- Fristoe of articulation
the Khan Lewis (KPLA) analysis helps clinicians determine the presence of
phonological disorders, identify specific error pattern, guide intervention planning
what are the key features of the KPLA-3
Age range
administration time-
scoring-
analysis focus-
norm references-
connection to GFTA
Age range- 2;0 - 21;11 years
administration time- 10-20 minutes
scoring- manual or digital scoring
analysis focus- phonological processes, including substitutions, omissions, and distortions
norm references- compares a child’s performance to same-age peers
connection to GFTA - uses gfta-3 responses for analysis
standardized tools should be used concurrently with speech sample analysis because some children may -
be hesitant to talk, making it hard to gather data
avoid saying words that contain difficult sounds
have speech that is difficult to understand, making analysis challenging
not use all the speech sounds a clinician needs to assess
Speech sample analysis should be used concurrently with standardized tools because it:
Captures natural, connected speech rather than isolated words.
Helps determine if errors are part of typical development, a phonological process, or a disorder.
Evaluates how well a child's speech is understood across different contexts.
Prevents misdiagnosis by considering dialects and bilingual language patterns.
Provides a starting point for treatment and allows SLPs to track improvement over time.
what is one way to analyze a child speech sample
PCC Percent Consonant Correct.
What is PCC and what does it help clinicians determine
percentage consonant correct and is measure of how many consonant sounds a child correctly produces compared to the total number of consonants they attempt. - helps clinicians determine severity of a phonological disorder
how to find PCC
use a connected speech sample, identify all consonants the child attempts to say, count number of consonants correctly produces,
PCC = (correct consonants/total consonants) × 100
severity levels of PCC
85-100% = Mild
65-84% = Mild-Moderate
50-64% = Moderate-Severe
Below 50% = Severe
Why is PCC Important?
It provides an objective way to measure how much a child’s speech is impacted by phonological errors.
It helps determine the need for speech therapy and track progress over time.
It allows clinicians to set therapy goals based on the most frequently occurring errors.
stopping
child replaces fricatives/affricative (s,f,ch) with a stop sound (t,d,p)
glidding
child replaced liquid sounds (l or r) with glide sound (w y)
cluster reduction
/st/ - /t/
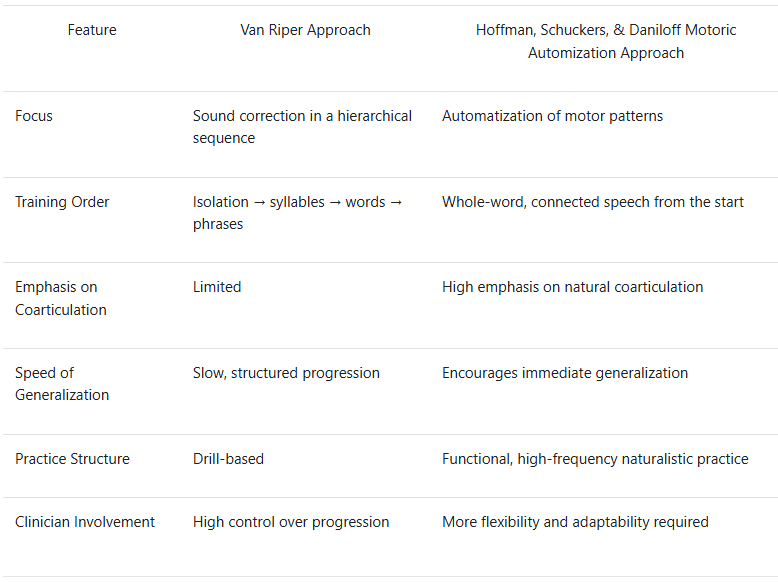
Van Riper Approach key principles
Based on a hierarchical sequence: isolation → syllables → words → phrases → sentences → conversation.
Uses a stimulus-response model, providing auditory discrimination training, followed by production tasks.
Emphasizes phonetic placement and shaping techniques to establish accurate articulatory placement.
Targets one sound at a time, working systematically toward mastery before moving to the next.
Focuses on error correction through drill-based practice, often with explicit feedback.
Gradual shift from structured to spontaneous speech.
ARTICUALTION
Van Riper Approach Therapy Progression:
Auditory Discrimination - The clinician presents minimal pairs (e.g., "sip" vs. "ship") and asks the client to identify the correct production.
Phonetic Placement Training - Using mirrors and tactile cues, the clinician teaches the correct tongue and lip placement for a target sound (e.g., /s/).
Isolation Practice - The client practices producing the sound in isolation with clinician feedback.
Syllable and Word-Level Practice - The client practices the sound in syllables (e.g., "sa, se, si") and words (e.g., "sun, sip, soap").
Sentence-Level Practice - The client constructs sentences using target words.
Conversational Practice - The clinician engages the client in structured conversation incorporating target sounds.
Van Riper Approach strengths and limitations
Strengths:
Well-structured and systematic approach.
Effective for children with phonetic-based articulation errors.
Provides clear, measurable steps for progress.
Limitations:
Can be slow-moving, as it requires mastery at each level before progressing.
Less emphasis on generalization to natural conversation.
Client is a passive recipient.
Hoffman, Schuckers, and Daniloff motoric automization approach key principles
focuses on speech motor control rather than isolated sound correction
emphasized automatization of motor pattern rather than traditional stepwise progression
encourages high- frequency practice in naturalistic contexts to build automaticity
involves coarticulation form the beginning rather than targeting sounds in isolation
uses functional task- oriented exercises rather than drills
focuses on generalization from outset, ensuring sounds are learned connected
Hoffman, Schuckers, and Daniloff motoric automization approach therapy example
warm up with movement- engage the client in rhythmic activities (clapping, tapping) to establish motor coordination.
whole-word practice- client practices whole words containing the target sound in functional phrases (Let’s go to the store” for the /s/ sound
high-frequency repetitions- the clinician encourages the client to produce words in rapid succession within meaningful dialogue
Coarticulation integration - the client practices the target sound in different word positions using natural speech patterns
Conversational Integration - clinician engages the clients in free speech activities, ensuring the target sound appears naturally in discussion
Reinforcement and Feedback - provide real- time feedback and adjust strategies based on performance
Hoffman, Schuckers, and Daniloff motoric automization approach strengths and limitations
Strengths:
Encourages rapid generalization into natural speech contexts.
More dynamic and adaptable to individual learning styles.
Client is an active participant.
Limitations:
Less structured compared to Van Riper’s method, which may make it harder to track small incremental progress.
May require more clinician expertise in understanding motor learning principles.
Less suited for children who need explicit, structured feedback and hierarchical learning.
comparison summary of Van Riper and Hoffman automization approach
Language and phonological disorders approach designs - key concepts
Strorybook - Based Intervention
Contrast Word Therapy Integration
Child initiated support
Language and phonological disorders - Storybook Based intervention
uses children’s books as a foundation for therapy sessions
storybooks provide contextualized and repetitive exposure to target sounds and words
encourages phonological awareness, semantic/narrative/morphosyntactic skills
Language and phonological disorders - Contrast Word Therapy Integration
embeds minimal, maximal, or multiple oppositions contrast words pairs into storybook reading activities
Helps children discriminate and produce target sounds within meaningful contexts
reinforced phonological contrast through structured play and interactive discussions
Language and phonological disorders- Child initiated support- language expansion and literacy development
children engage in auditory discrimination tasks (identifying words with correct vs incorrect sounds
encourages production of target sounds in structures and spontaneous speech tasks
uses corrective feedback and scaffolding to support speech production
builds comprehension by connecting phonological contrasts to story themes
encourages children to use contrast words in sentence-building and stoytelling
support early literacy skills by reinforcing phonemic awareness
Therapy session
tep 1: Select a Storybook with Phonological Targets
Choose a book rich in target sounds and contrast pairs.
Example: Sheep in a Jeep (for /ʃ/ vs. /s/ contrasts: "sheep" vs. "seep").
Step 2: Pre-Reading Explicit Activity
Introduce contrast words from the story (e.g., "jeep" vs. "deep," "sheep" vs. "seep").
Ask children to listen and identify differences between pairs.
Step 3: Interactive Story Reading
Read the book language and speech sound production.
Pause to engage children in contrast word production (e.g., "Did the sheep go in the seep or the jeep?").
Step 4: Post-Reading Activity
Phonological Practice: Use word sorting games to reinforce minimal/maximal contrasts.
Language Expansion: Have children retell the story using target words.
Generalization Activity: Incorporate story-based role-play using the contrast words in new sentences.
Contrastive therapy for phonological disorder
minimal pair therapy, maximal opposition therapy, and multiple opposition therapy
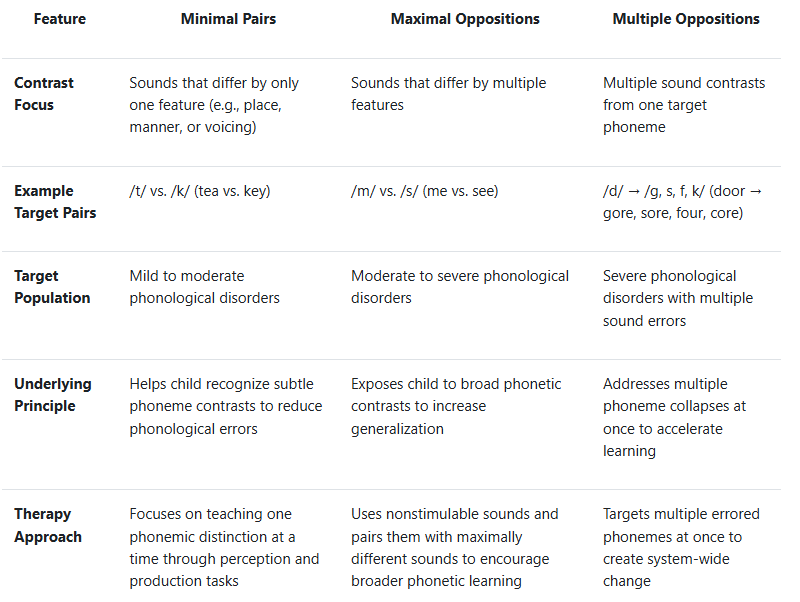
Minimal pairs, Maximal oppositions, multiple oppositions
Contrast Focus
Example Target pairs
Target Population
Underlying principle
Therapy approach
Advantage:
Minimal pairs
Maximal pair
Multiple
Minimal pairs: Effective for children with a small number of error patterns More effective for generalization
Maximal pair: Promotes widespread improvement across the phonemic system
Multiple: Efficient for children with severe phoneme collapses
minimal pair therapy
Goal: Help children distinguish between phonemes that differ by only one feature (place, manner, or voicing).
Target Population: Children with mild to moderate phonological disorders.
Activity: Picture Sorting Game
Steps:
Select minimal pairs based on the child’s phonological error (e.g., fronting: /t/ vs. /k/ → "tea" vs. "key").
Print or draw pictures representing each pair.
Have the child listen to the words and place them in the correct category (e.g., "Put 'tea' in the /t/ pile and 'key' in the /k/ pile").
Once the child consistently identifies the difference, encourage them to produce the words correctly.
Use a reward system (stickers, points) for correct responses.
Activity: "Guess the Word"
Maximal oppositions therapy activities
Goal: Help children generalize phonological learning by contrasting two sounds that are maximally different (i.e., differing in place, manner, and voicing).
Target Population: Children with moderate to severe phonological disorders.
Steps:
Choose word pairs with maximal contrasts (e.g., /m/ vs. /s/: "mat" vs. "sat").
Print or draw pictures of each word.
Have the child match the pictures and say the words aloud.
Exaggerate the differences in articulation to help the child understand the contrast.
Use a "silly voice" round where the child says the words in different tones to reinforce sound differences.
Activity: "Sound Jump"
Multiple Oppositions Therapy activities
Multiple Oppositions Therapy Activities
Goal: Address multiple phoneme collapses by contrasting several errored sounds at once.
Target Population: Children with severe phonological disorders who substitute one phoneme for many others.
Steps:
Identify a phoneme collapse (e.g., a child substitutes /d/ for /g, s, f, k/ → "door" for "gore," "sore," "four," "core").
Choose a set of four target words that contain the correct sounds.
Show the child pictures representing the words and name them.
Have the child repeat each word while touching the corresponding picture.
Use a game format/play (e.g., rolling dice and saying the word they land on).
Gradually increase complexity by using words in short phrases.