9) Benign vs. Malignant
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
33 Terms
What are PROTO-ONCOGENES?
genes that direct formation of normal proteins used in cell division
Ex. growth factors, GF receptors
“GO signals”
Mutations of PROTO-ONCOGENES lead to __
Oncogenes = uncontrolled cell growth
*might produce TOO MUCH protein
OR
produce ABNORMAL protein
What are TUMOR SUPRESSOR GENES?
A mutation in TSG leads to:
proteins INHIBIT cell growth
uninhibited cell growth (so starts proliferating)
(TSG becomes ineffective → you can’t STOP) → get neoplasia (uncontrolled/abnormal cell growth)
Any mutation is __ on its own.
The development of cancer is a __
not sufficient
complex process w/ multiple steps
1) What is this multistep process called?
2) What does it require?
1) Carcinogenesis
2) Initiation, Promotion, Progression
What is INITIATION?
Any carcinogens we mentioned (sunlight, smoke) that MODIFIES DNA
(still not cancer at this point; just mutated)
What is PROMOTION?
STIMULATES GROWTH of mutated cells
*Note: promoters could be initiators (also could NOT be)
ex. smoking → initiator and promoter
2nday chemical can also be a promoter
(still not cancer @ this point; just mutated)
What is PROGRESSION?
What’s a key word?
tumor cells COMpETE w/ each other
→ competition causes SMALLER mutations
→ cells become more AGGRESSIVE = malignant
keyword: survival of the fittest
*General:
Central property: tumor cells do not behave normally during cell division.
-mutation needs to pass onto the daughter cell
What are PROPERTIES of tumor cells?
1) PROLIFERATE to form new tissue
2) Evade body controls
- ignores signals to STOP dividing
- prolifates even though the body hasn’t said “we need more tissue”
3) Does not DIFFERENTIATE (no specific function)
4) # of cells NOT CONSTANT (apoptosis ignored)
5) Exhibits ANCHORAGE independence
→ metastasis follows
What are characteristics we might see of TUMOR CELLS?
What do we see during biopsy
1) increase in cell #
4) increase nuclear size / DNA
5) increase mitotic activity
2) loss of arrangement (disorganized)
3) varied morphology (cell shape/size)
Tumors are classified based on __
1) invasiveness (invasive, local;insitu, malignant)
2) tissue/cell type
oma = benign
carcinoma = malignant; epithelium
sarcoma = malignant, tissue
What are blastomas?
Neuroblastoma = adrenal medulla/neural
Hepatoblastoma = liver
Nephroblastoma = kidney
embyronic cells (cells really early during development)
aka: immature cells
What does dedifferentiation mean?
Mature/ well differentiated cell → dedifferentiates
→ BEHAVES like undifferentiated cells
→ can generate malignant tumors
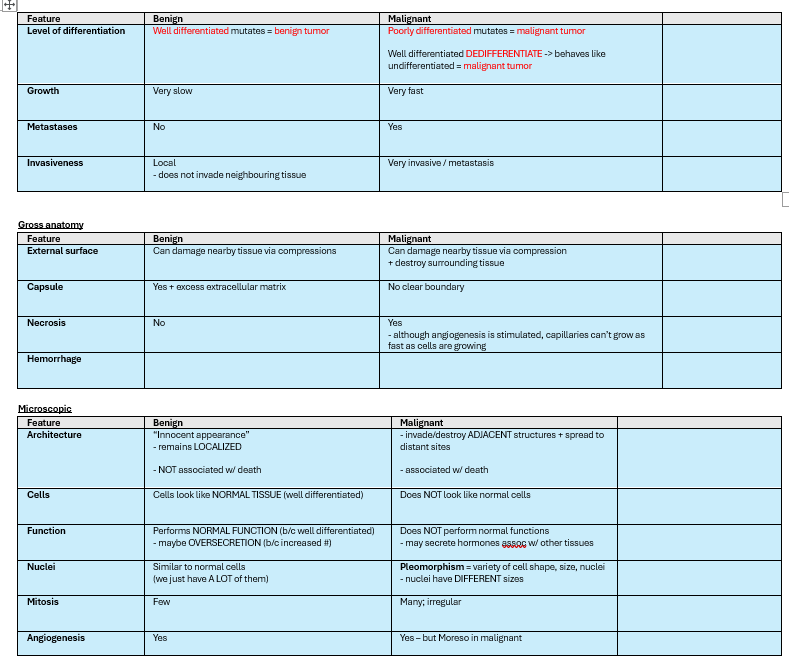
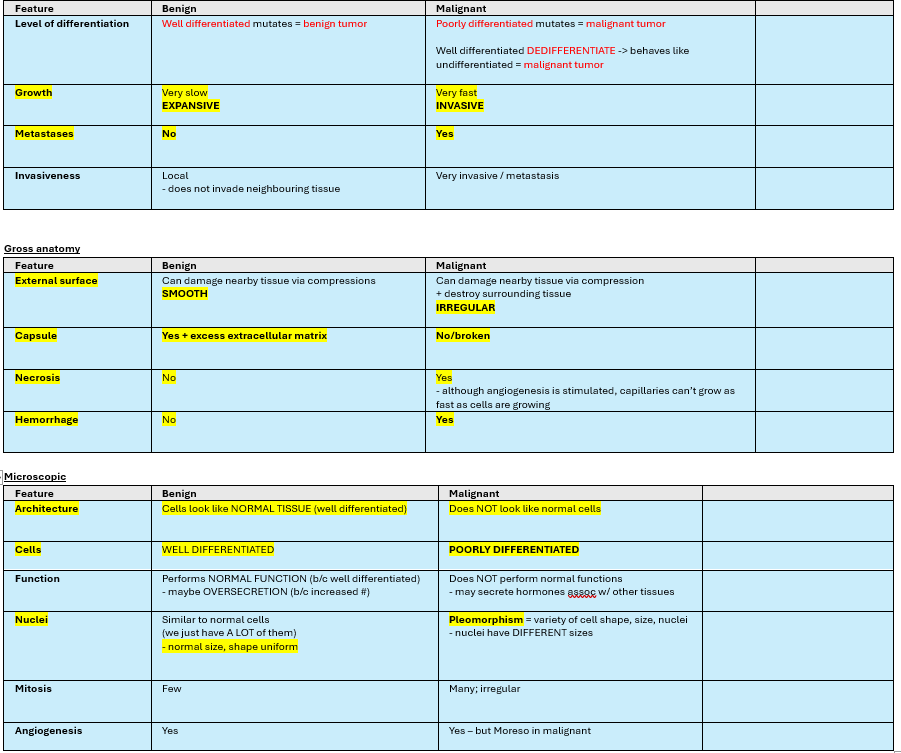
How do benign and malignant cells differ?
1) level of differentiation
2) rate of growth
3) metastasis
4) invasiveness
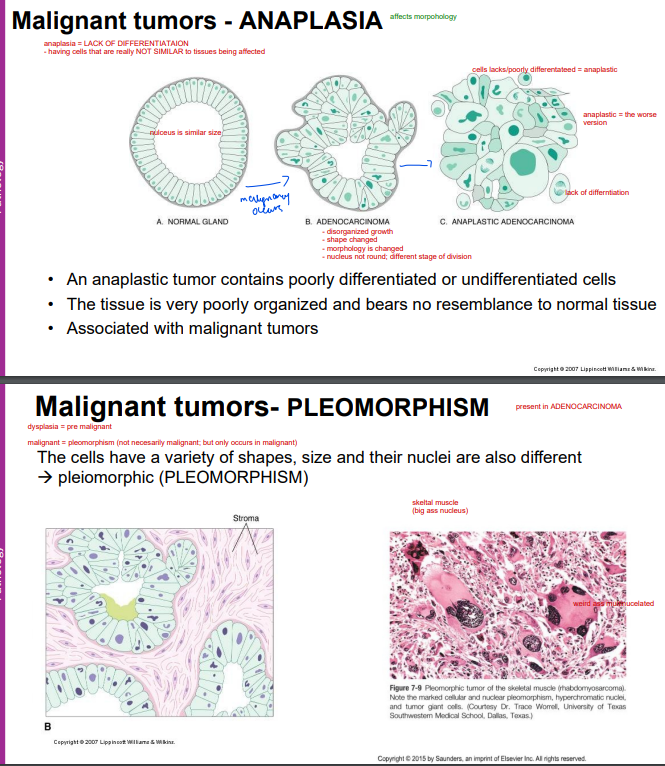
Malignant cells are known to have morphologic alterations.
What are they?
1) Anaplasia = poorly differentiated (no specific function)
- cells NOT SIMILAR to tissue being affected
2) Pleomorphism = variety of shapes, size, nuclei (different size)
A cancer cell that invades and metastasizes are __
Invasion and metastsis is the __
ALWAYS MALIGNANT.
major of cause of cancer related mortality/reduces chance of cure
(LO) Describe to MECHANISM involved in tumor metastasis.
INVASION/METASTASIS
1) Mutated cell loosen adhesion to original neighbours (anchorage independence)
2) Escapes original tissue
3) burrows through tissue to reach BV/lymph vessel
4) in BV/lymph circulating
5) exits circulation into another part of body
6) survives & proliferates in new environment
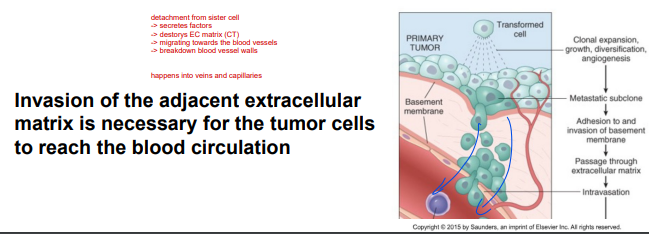
What is necessary for tumor/cancer cells to reach blood circulation?
invasion INTO adjacent extracellular matrix
*hall mark distinction b/w being benign and malignant
Tumor cells typically metastasize to a PREFERRED site. This is known as __
Why does this occur?
organ tropism
2)
- tissue-selective homing receptors
- prescence of hormones/GF in target tissues
Does metastasis only occur via blood?
NO
1) hematogenous spread (blood)
2) lymphatic spread
3) direct seeding via body cavities
1) What type of cells does hematogenous spread involve?
2) Where does it usually occur?
3) Where is the final location?
1) Sarcoma (typical) + sometimes carcinoma
2) via: venous drainage/capillaries
3) liver + lungs (b/c venous return)
1) What type of cells does DIRECT SEEDING involve?
2) Where does it usually occur?
3) Where is the final location?
1) ovarian carcinoma (epithelium)
2) tumor penetrates peritoneum (open fluid cavity)
3) tends to be on surface
1) What type of cells does lymphatic spread involve?
2) Where does it usually occur?
3) Where is the final location?
1) carcinoma (epithelium)
2) tumor cells invade lymph vessel → follows COURSE of lymph flow (one way)
→ cancer can get stuck (starts to grow)
What is NECESSARY for growth?
Angiogenesis
w/o blood, cancer doesn’t grow (needs nutrients)
What are clinical manifestations of cancer?
1) change in organ function
- organ failure
- oversecretion (benign)
- decreased production of normal secretion +overproduction of diff hormone = malignant
2) change in local effects
- bleeding
- compress BV = portal hypertension
- compress Lymphvessel = edema, ascites
- compress hollow organs = compress intestines constipation
- compress nerves
3) distant effects (hormonal production - paraneoplastic disorder)
4) non-specific signs of tissue breakdown (infarction/rupture)
- eli: ig just the nature of something big growing → things like compression
Give an example of a DISTANT EFFECT.
Paraneoplastic syndrome
ex. tumor/cancer produce hormones that is NOT usually produced there
systemic symptoms NOT b/c of local/metastatic spread,
→ OR expected hormones’ produced by the affected tissue
→ but due to it creating a different hormone
ex. lung carcinoma → produces parathyroid hormone → hypercalcemia
(usually only parathyroid creates parathyroid hormone)
What is cancer cachexia syndrome?
“generalized effect of cancer”
ex. of paraneoplastic syndrome
-weightloss
- muscle wasting
- anorexia
- weakness
- anemia
*not b/c of loss of appetite, but caused by cancers”
Why is tumor grading and staging importnat?
quantifies aggressiveness of tumor + know what kinda tx we will use
also helps us monitor as we go
What’s the difference b/w GRADING & STAGING?
1) Grading = how well differentiated
- tf does it look like; do they look similar to the cells around it
- high grade = poorly differentiate
- low grade = well differentiated
2) Staging = how does it behave
Takes into account TNM:
- tumor size
- lymph node metastasis
- distance metastasis
__ is highly important for prognosis and treatment
Tumor staging
Why are TUMOR MARKERS beneficial?
What are their limitations?
biochemical assays can detect molecules → indication of presence of tumor
Ex. prostate specific antigen (PSA) = high levels = potential for prostate cancer
Limitations = when you exercise, there are physiological effects. You may have HIGH levels of PSA after exercise.