W10: Paediatrics prescribing
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
18 Terms
WATCH LECTURE
Discuss different prescribing strategies based on the age, modality and refractive error of paediatric patients.
Discuss the “Glasses in Classes” initiative.
What considerations should be made when prescribing for children (Leat, 2011)?
Is the refractive error within the normal range for the child’s age?
Will this child’s refractive error emmetropise?
Will this level of refractive error disrupt normal visual development or functional vision?
Will prescribing spectacles improve visual function or functional vision?
Will prescribing glasses interfere with the normal process of emmetropisation?
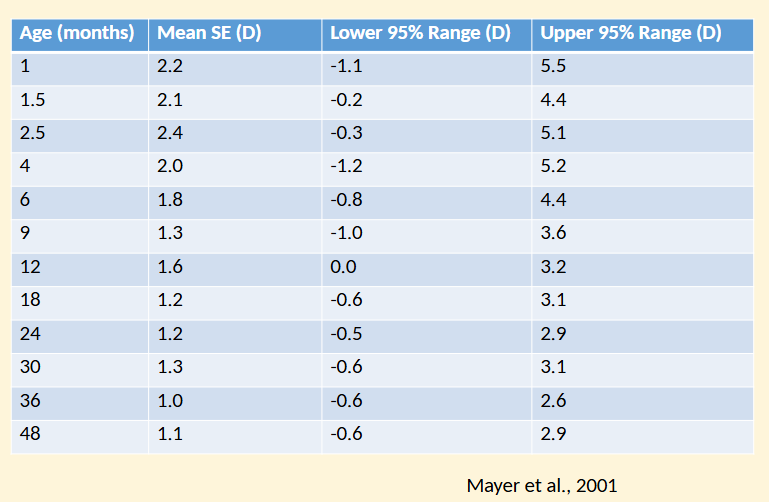
What is the normal range of refractive error in infancy and early childhood?
Most infants tend to be hyperopic.
Range of refractive error is much wider in the first year than later in childhood.
Astigmatism is high at birth: 69% have >1.00 DC (Varghese et al., 2009).
What is the normal range of refractive error according to Mayer et al (2001)?
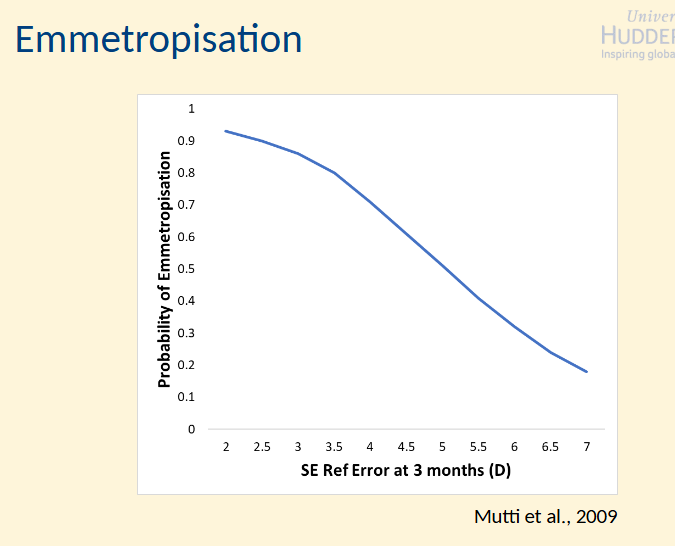
What factors affect emmetropisation in early childhood?
Most children will emmetropise.
Those with high refractive errors in the first 3 months are at risk of not emmetropising.
High hyperopia
High astigmatism
High anisometropia
Emmetropisation
Mutti et al ,2009
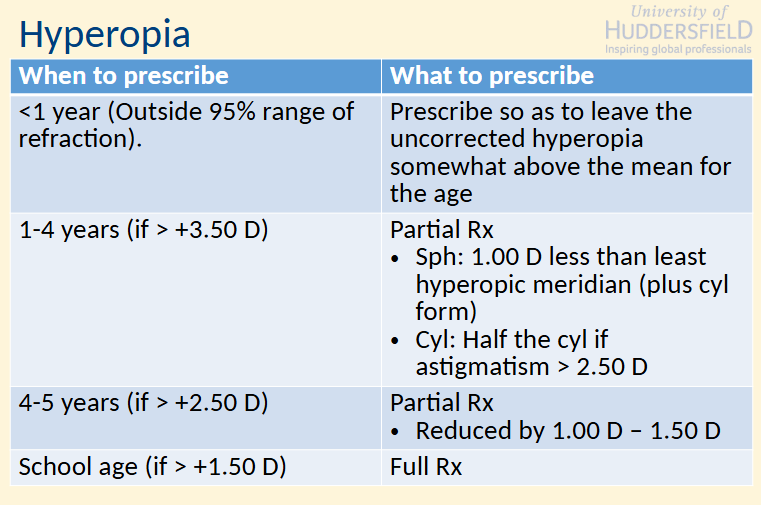
Hyperopia
When/What to prescribe
Accommodative SOTs should receive the full Rx.
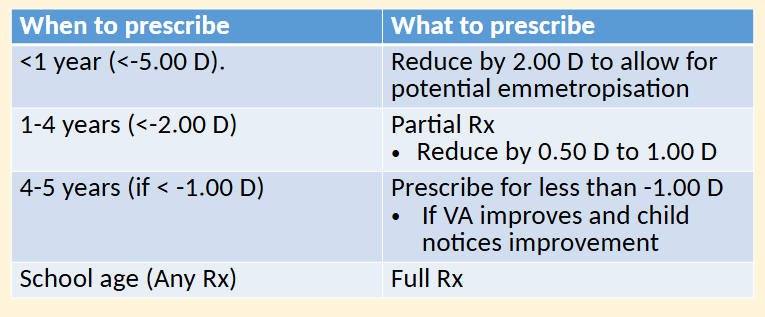
Myopia
When/What to prescribe
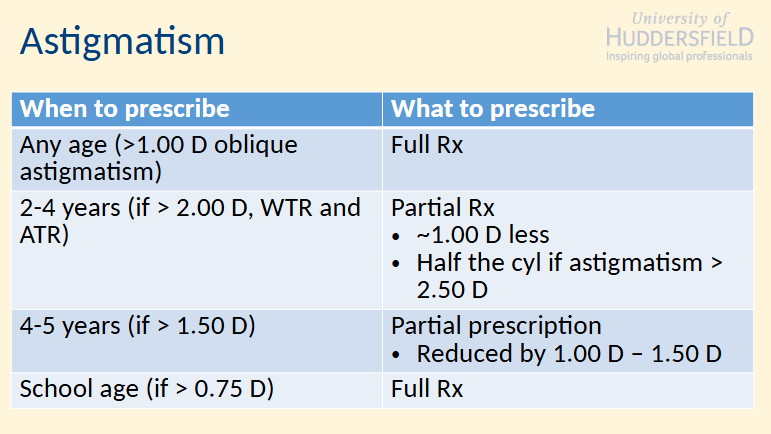
Astigmatism
When/What to prescribe
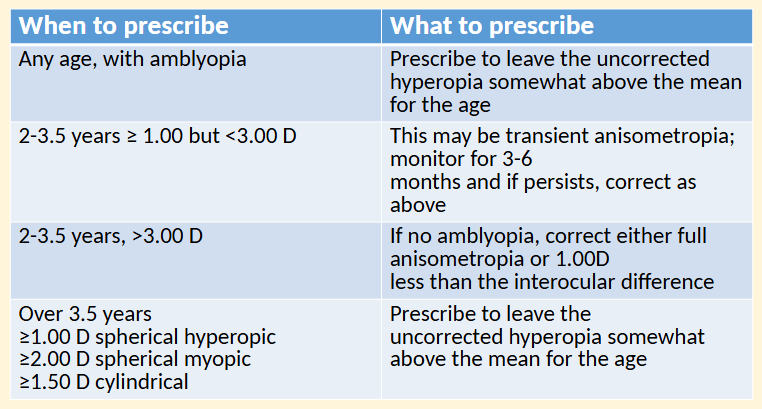
Anisometropia
When/What to prescribe
What factors should be considered when deciding a child’s spectacle-wearing schedule?
Must be tailored to the patient’s individual needs.
Also depends on severity of refractive error.
Need to use clinical judgement
Consider what tasks require glasses:
Close work
Board / TV
Sports
What is the relationship between early literacy, visual acuity, and spectacle adherence?
Research suggests early literacy is assoc’d w/ VA
Failure to adhere to spectacle wear can negatively impact a child’s vision + education.
(Bruce et al., 2018)
What is the aim of the “Glasses in Classes” project?
To find out if schools can support children in wearing their glasses.
Part of the Born in Bradford programme.
What is the difference between control and intervention schools in the Glasses in Classes project?
Control Schools:
No change to vision screening process.
Children w/ reduced vision are referred to hospital or community optometry for full assessment.
Intervention Schools:
Screening results (pass/fail) are shared w/ the school.
A designated vision co-ordinator follows up children who fail to check if parents need help arranging appts
How are glasses provided and managed in intervention schools within the project?
Children who need glasses rec two pairs:
1 personal pair to be worn as directed by the optometrist.
1 extra pair kept in school.
School pair only used if child forgets their own glasses, returned to the vision co-ordinator at the end of the school day.
Project results have been affected by the Covid pandemic + protocol has been adapted, expanding the project to 500 schools.
What areas were included in the 2021 expansion of the scheme?
As of September 2021, the scheme was expanded (Dept of Education, 2021).
New areas: Doncaster, Derby, Durham, Norwich and Breckland, and North Yorkshire Coast.