Growth Hormone
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
18 Terms
What cells synthesize/release GH?
What are the Effects of GH?
Somatotrophs in the AP produce growth hormone (somatotropin)
Effects:
Increased size/# of cells/ mitosis
Specific differentiation
Describe the Difference between GHRH and Somatotropin
Hypothalamus stimulates GH secretion from somatotroph via growth hormone releasing hormone (GHRH)
Hypothalamus inhibits GH synthesis and release from somatotroph via somatostatin
Draw out the pathway of GH and SomatoStatin
Starting From the hypothalamus and ending at the effector organs
(Adipose, Muscle, Hepatocyte, and other effectors)
Include the Physical Conditions in which GH will be stimulated to release
Include the Negative Feedback Mechanisms
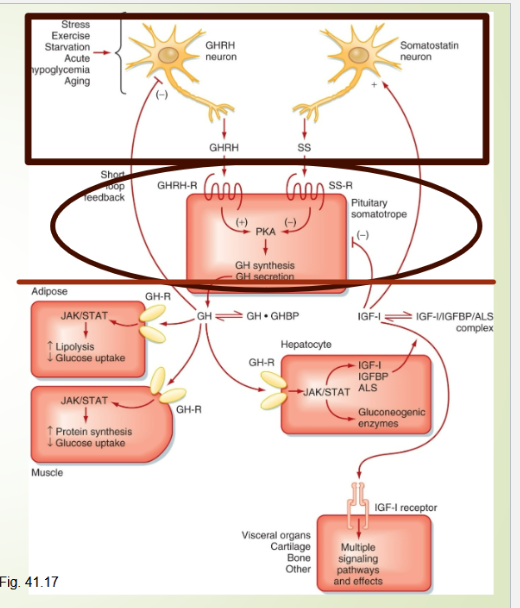
Describe the Negative Feedback in the GH pathway
Negative Feedback on GH pathway
Long Loop (IGF-1):
Inhibits GH production from Somatotrophs
Inhibits GHRH release from arcuate nucleus in hypothalamus
Stimulates secretion of Somatostatin from periventricular nuclei
Short Loop (GH):
inhibits GH release from Somatotrophs
When is GH released throughout the day?
Why is IGF-1 a better indicator of GH Secretion?
Draw out a graph depicting Bursts of GH throughout the Day
GH is released primarily during slow wave sleep
IGF-1 is a better indicator because:
regulated by GH
Longer Circulating Half-Life

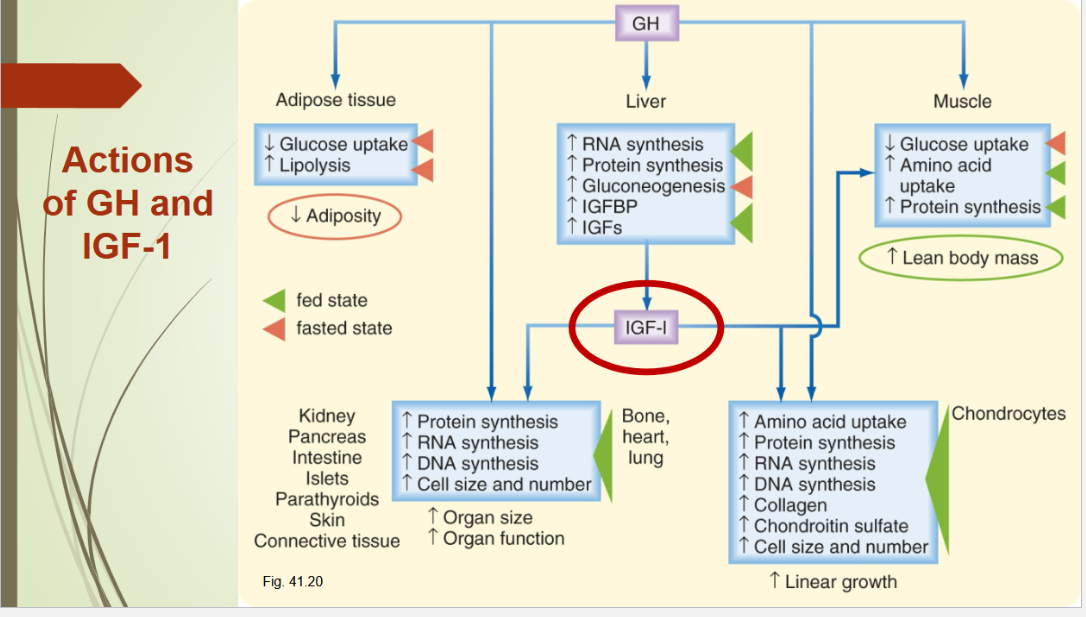
What is the main target of GH and what is GH’s Action?
What happen to 50% of GH? Why is this beneficial?
Liver:
GH’s main target = Liver → stimulates production of insulin-like growth factor (IGF-1)
GHBP:
50% of GH is bound to GH-binding protein (GHBP)
Increases Half-Life of GH
Make it less available for degradation by Liver/Kidney
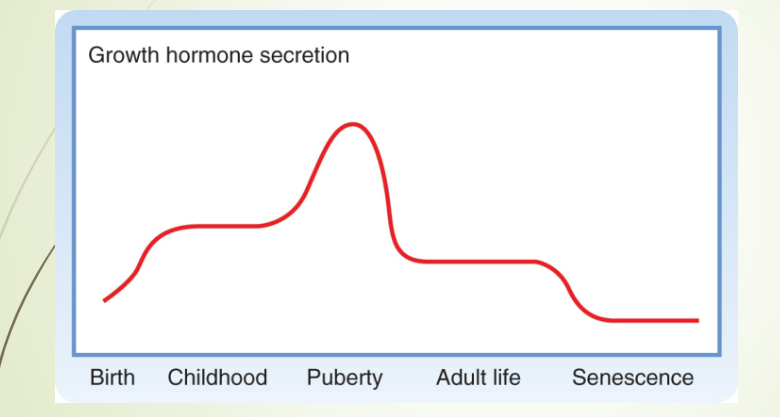
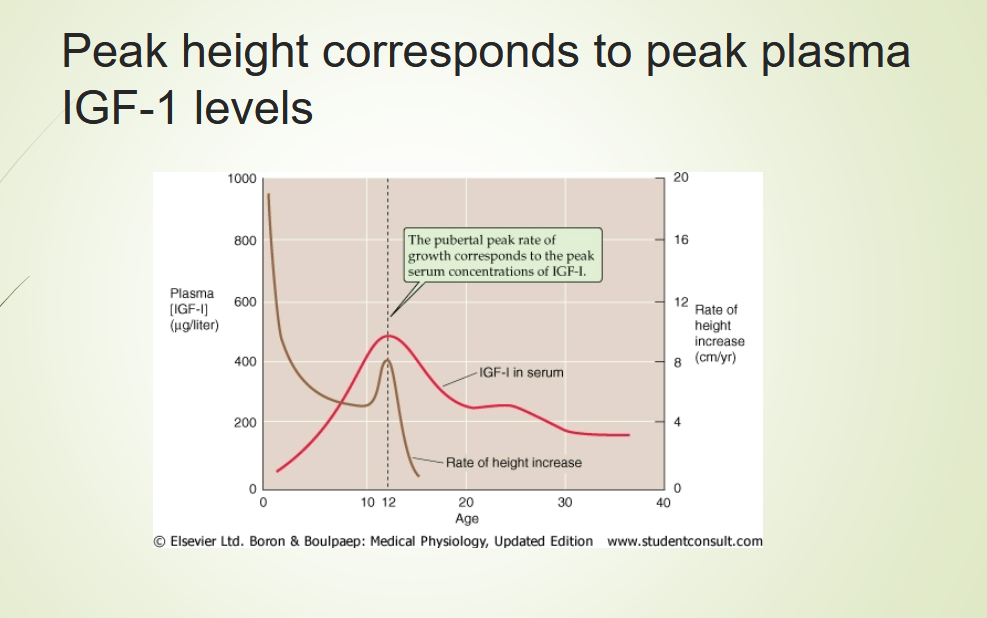
Draw out the graph of GH Secretion during lifespan
What does Peak Height Correspond with?
What is the most biologically active somatomedin?
Where is this molecule Secreted from?
What is its general function?
What are the effects of this molecules?
IGF-1:
most biologically active somatomedin is IGF-1 or Somatomedin C
mainly secreted from the liver after stimulation by GH
Has Insulin-Like Effects → promotes fuel storage in various tissues
Inhibits GH and GHRH secretion
Effects:
Stimulates the growth of bones, cartilage, and soft tissue
stimulates osteoblast replication and collagen/bone matrix synthesis
Regulates metabolism of chondrocytes
mitogenic (stimulates DNA, RNA, and protein synthesis)
Describe the the Effect of GH and IGF-1 on Bone Growth
How does GH fail?
Bone Growth:
Increases growth of skeletal frame:
Increases deposition of protein by chondrocytic and osteogenic cells
Increases rate of reproduction of these cells
Increases rate chondrocytes → osteogenic cells
Long bones grow in length at the epiphyseal cartilages
stimulates osteoblasts
Osteoblasts in bone periosteum deposit new bone on the surfaces of older bone
Osteoclasts remove old bone
Failure:
GH Fails w/o insulin and carbohydrates
needed for energy and enhanced AA and glucose transport
What type of hormone is GH? What does it activates?
What are its general Metabolic Effects?
How can GH cause diabetes?
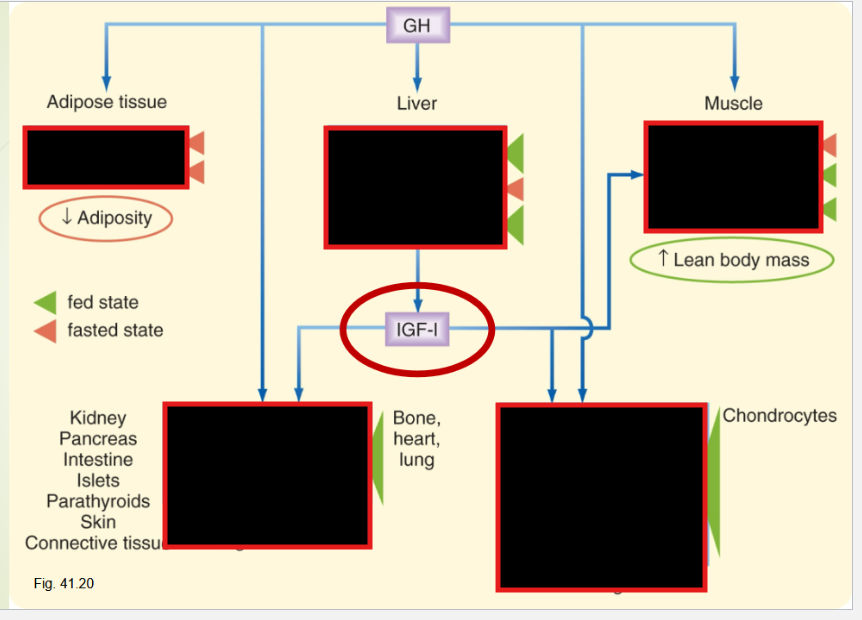
Describe the Specific Metabolic Actions that GH has on:
Adipose Tissue
Skeletal Muscles
Liver
GH = Anabolic/Lipolytic Hormone
activates hormone sensitive lipase and mobilizes fats from adipose.
General Metabolic Effects:
counteracts the action of insulin on lipid and glucose metabolism
decreases skeletal muscle glucose utilization
Stimulates Lipolysis/ hepatic glucose production
GH can cause DIabetes b/c it:
Decreases carbohydrate utilization
Hyperglycemic effects b/c:
decreased glucose uptake
increased glucose production (by liver)
Increases FFA oxidation = stimulate GNG
This increases Insulin Levels (in order to maintain normal glucose levels) → Insulin resistance
Adipose:
Stimulates Release and Oxidation of FFA
mediated by regulating the activity of
lipoprotein lipase
Skeletal Muscles:
decreases skeletal muscle glucose utilization
stimulates amino acid uptake and incorporation into protein
suppression of protein degradation
cell proliferation
Liver:
stimulates hepatic IGF-1 production and release
promotes GNG and reduces glucose uptake
Net result = stimulating hepatic glucose output
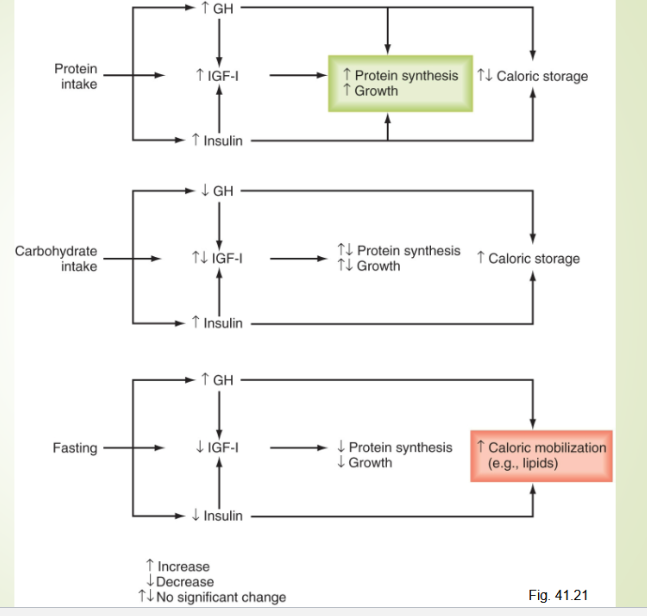
Describe the interaction of nutrient, GH, and IGF-1 when the pt has:
ample nutrient?
High Calories, low AA
Fasting (or low nutrient availble)
Ample nutrients:
Amino acids increase GH and insulin
High serum glu increases insulin secretion
High GH, insulin and nutrients promote growth
High calories, low amino acids:
High carbs increases insulin secretion
But low amino acid inhibits GH and IGF production
Dietary carbs and fats used for energy but not good conditions for growth
Fasting, overall low nutrient availability:
Low carbs and fats increase GH levels and lower insulin levels, however IGF levels are low, conditions do not favor growth.
GH is beneficial because it promotes fat mobilization while attempting to minimize tissue protein loss.
With less insulin, peripheral tissue glucose use is decreased, sparring glucose for essential tissues such as brain
List out the Stimulating and Inhibiting Factors of GH Secretion

How can Dwarfism occur?
Describe the etiology of Laron Dwarfism
What happens if there’s a deficiet in GH secretion after growth plate
Dwarfism:
If GH Deficiency developed before puberty
Many cases derived from panhypopituitarism
All Anterior Pit. Hormones deficient
not mature sexually and infertile
Laron Dwarfism:
GH secretion is normal or high
Receptor defective so liver does not produce IGF-1
If GH Deficiency At Adulthood:
At this point, Growthplate (epiphyses) has close
Causes Hypoglycemia
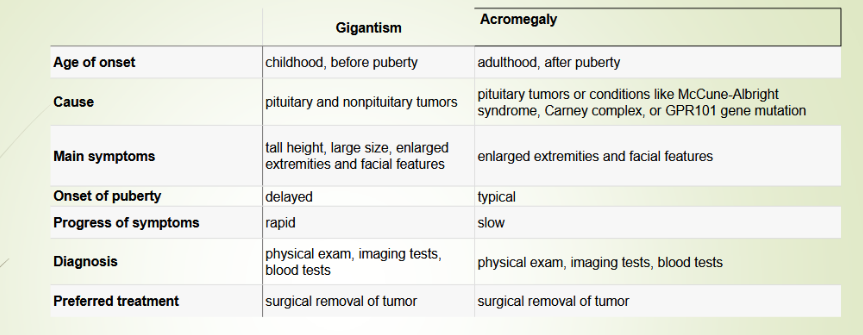
Differentiate between Gigantism and Acromegaly
Gigantism:
Hypersecretion of GH in children and adolescents
Increased bone length/thickness
Acromegaly:
Hypersecretion of GH during adulthood
enlargement of the hands and feet, coarsening of
facial features, insulin resistance, and diabetes
Describe how hyper GH can cause pituitary diaabetes
Pituitary Diabetes:
lipolysis and decreased glucose uptake → high blood glucose → high Insulin Secretion (Type II) → Burn out of B-cells (Type 1)