April 11 Notes
1/92
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
93 Terms
Disorders of Amount of Movement
Movement disorders related to the basal ganglia
Movement disorders related to the basal ganglia
Hypokinesia and hyperkinesia
Hypokinesia
Decreased/lack of movement without weakness or spasticity
Hyperkinesia
Excess/Abnormal movements
Hypokinesia disorders
akinesia, bradykinesia, muscle rigidity
Hyperkinesia disorders
tremors, dystonia, chorea and tics
Hyperkinetic Dysarthria
Basal ganglia damage
Perceptual features vary based on types of movements and degree of movements interacting with speech
Respiration
Sudden, forced inspiration or expiration
Phonation
Harsh voice quality
Strained-strangled voice quality
Transient breathiness
Voice tremor
Articulation
Imprecise articulation
Prosody
Excess and equal stress
What type of damage results in hyperkinetic dysarthria?
basal ganglia
Why do perceptual features in hyperkinetic dysarthria vary?
based on types of movements and degree of movements interacting with speech
Hyperkinetic dysarthria respiration features
sudden, forced inspiration or expiration
Hyperkinetic dysarthria phonation features
harsh voice quality, strained-strangled voice quality, transient breathiness and voice tremor
Hyperkinetic dysarthria articulation features
imprecision
Hyperkinetic dysarthria prosody features
excess and equal stress
Possible Principles and Features of Treatment for Dysarthria
Considers any and all relevant subsystems of speech
Considering differences in prognosis for specific conditions
Restorative treatments (if appropriate)
Compensatory strategies
Exploring multimodal communication/AAC
Conversational strategies
(CHECK YOUR WORD DISCUSSION DOCUMENT AND ADD THAT STUFF TO THIS SET)
What is the difference between disorders of speech (like apraxia of speech and dysarthria) and disorders of language (like aphasia)?
i completely zoned out but you can figure it out
acquired apraxia of speech
NOT a type of dysarthria
Damage typically occurs in the premotor cortex
Speech errors are irregular
Perceptual characteristics include:
Consonant and vowel distortions
Distorted substitution of phonemes
Slowed rate
Unusual stress patterns
What is NOT a type of dysarthria?
acquired apraxia of speech
Acquired apraxia of speech damage typically occurs in the ___
premotor cortex
In acquired apraxia of speech, speech errors are ___
irregular
Acquired apraxia of speech perceptual characteristics include
Consonant and vowel distortions
Distorted substitution of phonemes
Slowed rate
Unusual stress patterns
Possible Principles and Features of Treatment for Acquired Apraxia of Speech
Intensive speech therapy to optimize motor learning
Compensatory strategies
Exploring multimodal communication/AAC
Conversational strategies
Potential for therapies that build on more intact functions like Melodic Intonation Therapy
language vs. speech question
Other Speech Disorders
Neurological underpinnings of fluency disorders
Developmental stuttering
Not damage, but structural and functional differences present
Findings suggest that for people who stutter, differences include (shown):
Increased brain activity during speech in the right hemisphere
Reduced auditory activations
Neurogenic stuttering
Language: What is it really?
Language is:
A set of arbitrary symbols
Agreed upon by a community or society
Which can be combined to communicate an infinite number of concepts between community members
Language is also about knowing how to put strings of sounds, symbols, or handshapes together into phrases, sentences and narratives, to express our thoughts and beliefs, opinions and preferences
Aphasia
Acquired neurogenic language disorders
Varying degrees of difficulty across:
Language expression, comprehension, and naming
Different modalities
Most commonly associated with strokes
Aphasia
Acquired neurogenic language disorder
Varying degrees of difficulty across:
Language expression, comprehension, and naming
Different modalities
Most commonly associated with strokes
____ is an acquired neurogenic language disorder
aphasia
In aphasia, there are varying degrees of difficulty across
Language expression, comprehension, naming and different modalities
Types of Aphasia
Global, Mixed Transcortical, Broca’s, Transcortical Motor, Wernicke’s, Transcortical Sensory, Conduction and Anomic
Aphasia Classification
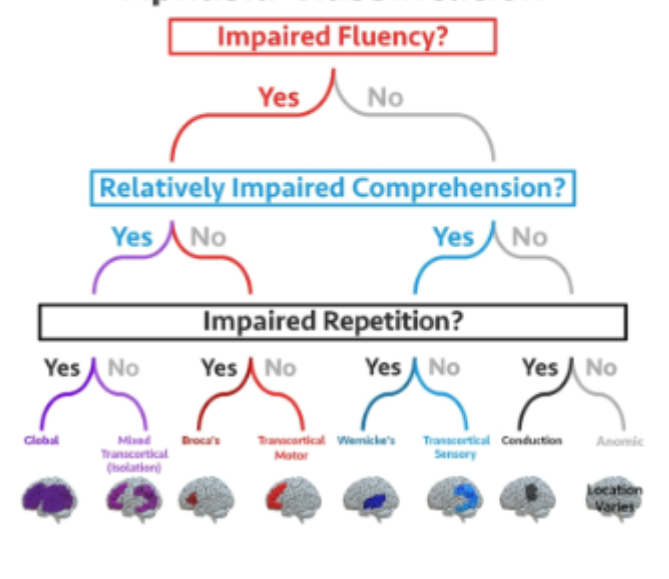
Broca’s-like Aphasia
Damage to anterior areas of the left frontal lobe
Language production is typically telegraphic, agrammatic, and effortful
Comprehension is relatively intact
Produces paraphasia
Repetition is affected due to overall expressive difficulties
Broca’s-like Aphasia is caused by damage to which areas?
anterior areas of the left frontal lobe
What is language production like in Broca’s-like Aphasia?
typically telegraphic, agrammatic, and effortful
What is comprehension in Broca’s-like Aphasia like?
relatively intact
What does Broca’s-like aphasia produce?
paraphasias
Repetition in Broca’s-like Aphasia
affected due to overall expressive difficulties
Wernicke’s-like Aphasia
Damage to the left posterior temporal lobe
Language production is typically grammatically and syntactically correct, but may be defined as “lacking meaning” (jargon)
Comprehension is impaired
Presence of paraphasias and neologisms
Repetition is affected due to comprehension difficulties
Wernicke’s-like Aphasia is caused by damage to these areas
left posterior temporal lobe
Language production in Wernicke’s-like Aphasia
typically grammatically and syntactically correct, but may be defined as “lacking meaning” (jargon)
Comprehension in Wernicke’s-like Aphasia
impaired
These are present in Wernicke’s-like Aphasia
paraphasias and neologisms
Repetition in Wernicke’s-like Aphasia
affected due to comprehension difficulties
A note on paraphasias
not a surprising phenomenon when you consider the language activation process in the brain
Anomic Aphasia
Mostly fluent, somewhat hard to categorize. Predominant difficulty in word-finding/naming
Fluency in anomic aphasia
mostly fluent, somewhat hard to categorize
Transcortical Forms of Aphasia
When repetition is fairly preserved
Transcortical motor (more expressive and Broca’s-like)
Damage is around Broca’s area, but not the area itself
Transcortical Sensory (more receptive and Wernicke’s-like)
Damage is around Wernicke’s area, but not the area itself
Mixed Transcortical
Relatively rare
Global Aphasia
expressive and receptive difficulties
most severe form of aphasia
may produce very few words
what is present is often paraphasias and/or verbal stereotypes
Neural Substrate of Language Recovery Following Stroke
Natural recovery of language:
Activation of brain areas immediately surrounding the damaged brain
Increased activation in undamaged speech and language association areas in the language dominant hemisphere
Activation of homologous areas in the non-dominant hemisphere
Varying levels of recoveryHa
Harnessing the ability of the brain to change
attempting to capitalize on neuroplasticity
Requires:
repetitive training of the system or behavior being targeted
challenging tasks
neural system or behavior in which change is desired must be engaged in training
repetitive engagement of brain networks
Neurogenic Cognitive-Communicative Disorders
visual processing, processing speed, working memory, attention, auditory processing, long term memory, logic and reasons
Dementia
progressive disorder with multiple subtypes
memory and at least one other cognitive function must be impaired
language difficulties are often semantic in nature
Types of dementia
Alzheimer’s, Vascular, Lowy body, Frontotemporal
Other, including Huntington’s, Mixed dementia: Dementia from more than one cause
Frontotemporal Dementia (FTD)
Progressive nerve cell loss specifically in the frontal and temporal lobes
Typically diagnosed earlier than Alzheimer’s
Includes multiple subtypes:
Behavioral variant frontotemporal dementia (bv FTD)
Primary progressive aphasia
FTD that mainly affects movement
Traumatic Brain Injury
Not strokes
strokes and TBIs are both acquired brain injuries
However, strokes are not traumatic (i.e., caused by an external force)
Typically more diffuse, unless it’s a penetrating head injury
Primary Progressive Aphasia
a type of frontotemporal dementia
a very unique dementia
doesn’t fit in neatly to our classification of aphasia
main concern is language, rather than cognition
Traumatic Brain Injury difficulties and impacts
difficulty is less likely to impact language directly
More likely to impact:
attention
memory
social communication
executive functioning
TBI Physical Symptoms
Headaches
Neck pain
Dizziness
Easily fatigued
Numbness or tingling
TBI Sensory symptoms
Sensitivity to light
Sensitivity to sound
Blurred or double vision
Lost sense of taste or smell
Ringing in ears (tinnitus)
TBI cognitive symptoms
memory problems
difficulty concentrating
difficulty making decisions
difficulty finding words
difficulty sequencing info
TBI emotional symptoms
easily agitated
mood swings
persistent anxiety
feelings of shame or guilt
feeling inept or worthless
behavioral symptoms
impulsive behavior
verbal outbursts
physical outbursts
getting lost easily
changed sleep patterns
TBI Symptoms
Physical: headaches, neck pain, dizziness, easily fatigued, numbness and/or tingling
Sensory: sensitivity to light, sensitivity to sound, blurred or double vision, lost sense of taste or smell, ringing in ears (tinnitus)
Cognitive: memory problems, difficulty concentrating, difficulty making decisions, difficulty finding words, difficulty sequencing info
Emotional: easily agitated, mood swings, persistent anxiety, feelings of shame or guilt, feeling inept or worthless
Behavioral: impulsive behavior, verbal outbursts, physical outbursts, getting lost easily, changed sleep patterns
Right Hemisphere Language Deficits
Include communication difficulties, attention deficits, and cognitive effects
Most interestingly, left neglect
Right hemisphere communication deficits may include, but are not limited to:
difficulty processing emotion
impaired prosodic abilities
disrupted content and organization of connected speech
impaired comprehension of connected speech
difficulty with abstract language
Left neglect is a ___ deficit
right hemisphere
Right hemisphere language deficits include
communication difficulties, attention deficits and cognitive effects
Neuroscience of Autism Spectrum Disorder
findings are mixed and complex, but some differences in autistic individuals/people with ASD include (Ha et al. 2015):
increased gray matter in frontal and temporal lobes
Differences in the cerebellum and limbic system
Differences in activation for executive functioning (shown)
Swallowing (deglutition)
Complex activity incorporating motor, sensory, and cognitive skills
Includes multiple phases based around movement of a bolus
oral (buccal) preparatory phase
oral phase
pharyngeal phase
esophageal phase
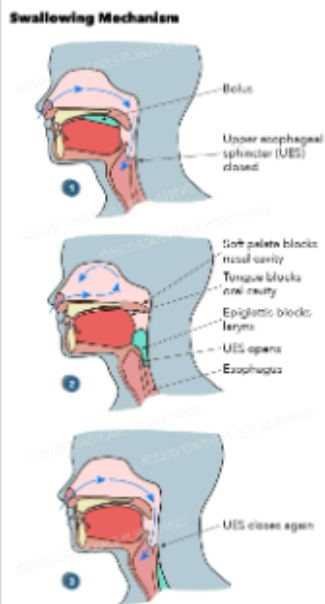
Oral (buccal)
the voluntary part of swallowing, the food is moistened with saliva and chewed, food bolus is formed and the tongue pushes it to the back of the throat (the pharynx). This process is under neural control of several areas of the cerebral cortex including the motor cortex
Pharyngeal phase
Starts with the stimulation of tactile receptors in the oropharynx by the food bolus. The swallow reflex is initiated and is under involuntary neuromuscular control. The following actions are taken to ensure the passage of food or drink into the esophagus:
The tongue blocks the oral cavity to prevent going back to the mouth
The soft palate blocks entry to the nasal cavity
The vocal folds close to protect the airway to the lungs. The larynx is pulled up with the epiglottis flipping over covering the entry to the trachea. This is the most important step since entry of food or drink into the lungs may potentially be life threatening
The upper esophageal sphincter opens to allow passage to the esophagus
Esophageal phase
Food bolus is propelled down the esophagus by peristalsis- a wave of muscular contraction that pushes the bolus ahead of it. The larynx moves down back to original position
Swallowing Disorders and the Cranial nerves
Includes cranial nerves more likely to be associated with:
Oral phase of swallowing
Pharyngeal phase of swallowing
Damage to specific cranial nerves or widespread damage
Cortical Areas Associated with Swallowing Disorders
Especially relevant to strokes
Primary motor cortex
difficulty swallowing in correct and precise manner
potential one-sided paralysis or weakness
Primary somatosensory cortex, along with temporal areas
Damage can be associated with oropharyngeal residue
Potential one-sided decrease in sensation
Insula
Hub for swallowing function
Basal ganglia
related to strokes or degenerative conditions
affecting the efficiency of swallowing
Parkinson’s Swallowing
Thalamus
Associated with difficulties in sensory-motor integration
Affecting hyoid/laryngeal movement; how much someone can consume at a time
Cognition and Swallowing
Difficulties with memory, attention, executive functioning, etc. that impact swallowing
Includes issues like:
Distractibility
Forgetting to eat/drink
Forgetting that one is in the process of eating/drinking
Dementia and Swallowing
Neuromuscular Electrical Stimulation (NMES)
Electrical stimulation of the affected peripheral nerve
Provided by trained professionals
Variable effects and variable recommendations
hearing and the Nervous system
Involves one critical cranial nerve and the remainder of the central auditory pathway
Series of brainstem structures interconnected via nerve pathways
Causes: Brain Injuries
potential for a variety of hearing and/or balance
May not be identified initially
Of a particular concern for blast injuries
Blast injuries can lead to
hearing loss
Auditory Processing Disorders
Normal pure-tone hearing, difficulty recognizing patterns of complex sounds or speech in noise
Can be developmental or acquired
Several viewpoints exist on types and associations with language disorders
Cortical Deafness
Also referred to as cerebral deafness
Extremely rare (~12 reported cases_
Inability to process speech and nonspeech sounds in the presence of normal or near-normal objective peripheral auditory function up to the level of the brainstem
Typically associated with bilateral temporal lobe damage