ANTH2250 exam notes
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
culture concept
a cognitive and emotional concept that permeates all human activity
people’s values are based in their ideas about the world- ideas shape how people think and react
why do people think and act the way they do?
always changing and being disputed, boundaries not so distinguishable
different cultural ideas of pain: anglo-saxon is to get the pain out, while in south east asie one should keep it in
can also impact the practices/treatment of a disease, and how it is spread
bioculturalism
significant interactions that take place between biology and culture in health and illness
Means health is shaped by
• Cultural conceptions
• Social connections (including global, political and economic)
• Human biology
medical anthropology
tries to understand health and illness processes
considers the biological, psychological, socio-political, economic and structural influences on health and disease
what is sickness
how it is understood, experienced and acted on by sufferers, their social networks, and healers
how health-related beliefs and practices fit within and are shaped by social and cultural systems and environmental contexts
researched through field methods, holistic and ethnogrpahy
historical origins of medical anthropology
1950’s, evolved out of wwII concerns and treatment of indigenous healing and global health initiaives
emic vs etic
emic = insiders view —> local, cultural reality, what does it mean to the person
etic = outsiders view —> outsiders interpretation, applying theories and perspectives that originated from outside the culture being studied
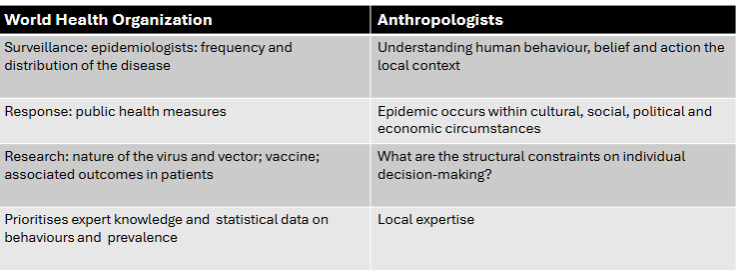
WHO vs anthropology definition of health
“not merely the absence of disease or infirmity but
complete physical, mental and social well-being” WHO
not enough mention of the spiritual aspect,
who based in epidemologists while anthropolgy is based in human behaviour and beliefs,
who believes in standard public health measures, while A thinks epidemics occur within a cultural factor
nature revolves around the virus, while for A it is based around why individuals make a decision
WHO priotritises expert biomedical knowledge while A believes on local expertise
3 theoretical approaches
ecological (aspects of the environment), interpretive (what people mean), critical (power and equality)
ecological approach
how the environment impacts how people react to an illness
biocultural perspective that views health and disease within an elaborate ecosystem, one that includes phsysical, biological and cultural componants
ecosystem persepctive: physical (climate, energy, materials), biotic (plants and animals, food, shelter), cultural (technology, social organisation, ideology)
how do people survive in this environment?
What resources help people cope?
Are ethnic boundaries restricting resources?
interpretive approach
how are illnesses and sickness culturally constructed?
what impacts how someone responds to or experiences an illness?
benefits: reduces one size fits all data, reduces assumptions, easier to interpret interactions, insider knowledge, critiques ethnocentrist views
limits: lose sight of the general, reduces ability to question, doesnt consider external factors
adaptation, resilience, resources
critical medical anthropology
what are the effects of social inequality on human health?
social inequalities = health inequalities
origins in marxism and critiques of capitalism/colonialism
focus on:
origins of dominant cultural constructions in health
how do health ideas and practices reinforce inequality?
social origins of disease: how do poverty, discrimination, and fear of violence contribute to ill health
who gets sick?
who gets treatment?
whos favoured?
can be effected by VISA status, gender, ethnicity, age, health insurance
causes health disparity (life expectancy), created by structural causes
structural causes= capitalism, racism, gender, colonialism
causes social suffering= not an individual experience, but rather connected to broader changes and conditions
ethnocentrism
the tendency to judge others using a personal criteria, can only be overcome through tolerance
idioms of distress
socially and culturally mediated ways of experiencing and expressing distress. for example in western medicine it may be demaning and relying on medication, while for someone else it may be using the spirits to explain
disease theory
disease theory = ideas about the nature of health, ideas about the cause of disease
personalistic system: results from action of supernatural being, non human being or a human being (deity, ghost, witch)
naturalistic system: imbalance of elements in the body (e.g. ying and yang)
disease vs illness
disease= naturally occuring, the pathogen, biomedical definition of lack of health, body loses a battle with the environment and succumbs to the pathogens, reaction to outside forces like microorganisms, shocks and pathogens
illness= the reaction to the disease, framed by cultural construction, expression of human mind and body, emotional state and social context, always culturally/socially/psychologically open to interpretation, subjective (thoughts, feelings, intentions, desires, self image), charged through metaphor, words have different meanings for different langauges
HIV Film
differing views between younger and older generations
money spoiling the minds of the community
little education in how HIV works and what it is, big belief in the way of life changing is causing this e.g. spending less time with parents
higher cost of living and little access to healthcare
people are too busy trying to live and survive, they aren’t worried about a disease
everyone seems to know someone who has it, seems desensitised, women would rather have money and a good conversation
importance of hausman
ethnomedicine
medical systems embedded in a socio-cultural system, includes biomedicine, contains a disease theory and a health care system
changing concept over time
all healers are ethnohealers
shaped by culture: how bodies work, what are the risks, who has expertise, how do bodies interact with the envrionment
medical pluralism
array of medical traditions at both conception and practice level
physicans, dentists, dieticians, healers, social workers, yoga teachers, chinese herbalists
health seeking process is a creative process, healers mix techniques
Complementary and Alternative Medicine (CAM)
from the biomedical perspective to refer to medical subsystems that are distinct alternatives and may function alongside biomedicine, Australians use the term complementary medicine quite broadly
includes biological, body based therapies, energy therapies, alternative medicine, mind body interventions, some debate about if new medications qualify
when do therapies become mainstream? debate about if one takes away from the other, increasing medicalisation, competitiveness
Sharmanism (ayahuasca)
Shamans are mediators between the spirit and the human worlds,need ayahuasca in order to move freely between the two and negotiate and restore relations between them (Fotiou 2016)
Ayahuasca was used in communal rituals of men, singing and dancing, for locating game animals, divination, in warfare and conflict, to see faraway places, and for healing by communicating with spirits, in native art, cosmology and ethnoastronomy (Fotiou 2016, p. 152)
debates around how it is used, whether the cultrual background should be removed by others, healer vs user perspective
Aboriginal understanding of ‘heart sickness’
effected by langauge barriers and lack of cultural understanding
anglo habbit of ‘dumbing down’, dont have an understanding of what they have
dont get told treatment plans and what it means, only what they have to do
gender
male dominated discipline, women were often the wives of and directed to particular topics, contributions of women were often discreditied
early perceptions of gender anthropology: own asumptions and binary, mens work, debates over womens status and power, 1960’s sisterhood, cultural diversity,
feminisms
1st 1850-1920: including women in ethnography
2nd 1920-1980: academia, removed sex from gender
3rd: acknowlege different experiences between women based on class, race, sexual identity like in critical race theory
what differences mean and how they interact with everyday life
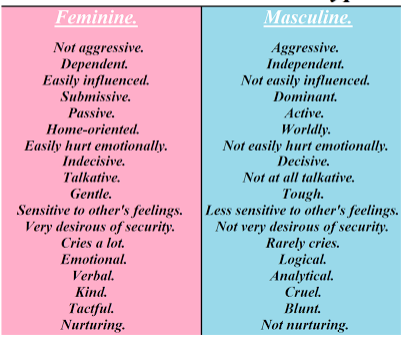
traditional gender stereotypes
more commonly articulated openly and can imply acceptance, a matter of conforming to rules
roles also focus more on actions (who looks after children, who speaks for family in public)
changing nature of gender roles and how it relates to health
changed in the 1930’s as a part of war effort, 1950’s housewife, modern business woman, modern day trad wife?
these inidvidual choices, such as in the tradwife movement, shows how domestic vs paid labour intersect with wellbeing and systemic issues
more independence given to women to make their own choices but decisions may be made more along the lines of how will this impact their role as a capitalist worker
increased emotional and physical labour of both working and having children (both expectations and not just 1)
universal body
how medicine conceives of, or
constructs, the body and what the
implications areUnexamined assumptions that the
body is universally the same (Lock &
Nguyen, 2018)The prevalence of the prototypical
male body within biomedicine-
imposes pathology onto female
states such as pregnancy and
childbirth where bodily changes are
viewed as ‘symptoms’ (Murphy-
Lawless, 1998).
medicalisation and intersex
giving a bodily condition or behaviour a medical label, defining the problem in medical terms, and using a medical
intervention to treat it
refers to medicine as a form of social control, has been used in lifecycle transitions, making a medical problem out of a normal human experience, can also be used to evaluate risk
example: anger issues
• intersex people have innate sex characteristics that don’t fit medical and social norms for female or male bodies
• Medical interventions have often been imposed
• Transgender is a term used to describe people whose gender identity differs from the sex they were assigned at birth
• Some transgender people may desire medical interventions (surgery, hormones) This has been challenged in recent times particularly in relation to affirmation in childhood vs issues related to gender dysphoria.
cultural competence
the ability of systems to provide care to patients with diverse
values, beliefs and behaviours, including tailoring delivery of care to meet patients’ social, cultural and linguistic needs
asks how systems and professionals can respond to diversity
structural violence
the influence of social structures on health, considers issues beyond people’s control that effect health, embedded in the poltical and economic organisation of the world, drawing attention to them aims to address them
health disparities
unequal distribution of health and disease; differences in health across groups, disproportionate/excess morbidity/life expectancy for one group in particular
unequal access to healthcare/health support in disadvantaged groups
examples include the african american population having a life expectancy of almost 10 years less than white americans
can be explained by social gradient: People who are less advantaged in terms of socioeconomic position have worse health (and shorter lives) than those who are more
advantaged
social determinants of health
social determinates also matter for health disparity, such as living conditions, lifestyle choices, housing, healthcare, discrimination, education etc.
Concept of Social Determinants of Health =broader, intersecting aspects of society, social relations, and social structures have a strong influence on health
impactful in the 19thC with measles outbreaks for example, vaccines helped but hygiene did significantly as well

Marshallese film
causes of TB rates
crowding, poverty-induced immune system, stress, malnutrition, colonisation, remenants of nuclear fallout, bad sanitation, bad facilities such as waste systems, displacement
what kinds of intervention are needed
better housing and facilities, education as to the disease and how the treatment works, more farming land and better nutrition, better quarantine measures
local biologies
how bodies are effected by culture, history and environment
example is the paper on menopause: symptoms are experienced differently in different counties e.g. hot flashes vs pain
impacted by biosocial differentiation: human bodies are not the same everywhere, continual bio-social interactions that differentiate people across time and space
Passing film
identity is not a choice but choosing to transition is
concept of masculinity, and having to change personality to fit in with new gender
role of power, men have higher expectations and duties
difficulties with unspoken rules
more effort to fit in and be accepted
needing to prove yourself
doctors questioning
gender vs sexuality health differentiation
masculine vs feminine actions being perceived differently e.g. aggression
intersectionality
Term coined by American feminist legal scholar, critical
race theorist, and civil rights advocate Kimberlé Williams
Crenshaw
describes overlapping or intersecting social identities
and related systems of oppression, domination,
or discrimination. Began with a focus on gender and
race.considers how multiple overlapping categories of
identity, difference, and disadvantage, including gender
and class, interact to produce outcomes (Hyde 2014).examples include transgender and gender diverse individuals being more likely to experience mental health issues, gp diagnoses also differentiate
biopower (Faucalt)
Michel Foucault’s idea of biopower describes how modern nation states attempt to regulate through "an
explosion of numerous and diverse techniques for achieving the subjugations of bodies and the control
of populations".
Biopower can include the application and impacts of political
power on all aspects of human life.
biopower = technologies and techniques
which govern human social and biological
processes
How governance takes place in the absence
of force
has been used in the case of aboriginal australians to sustain the labour force and claim to look out for them
also argues that we can learn from the past, not just in their mistakes, but what they did right
clinical gaze
• Foucault argued that doctors’ new powers of diagnosis relied on their ‘gaze’ - a new type of medical perception and
experience
• Physicians who observed bodies carefully could potentially
penetrate the illusions of outdated theories and see the
hidden ‘truth’ of disease
• In the process, practitioners gained much power and status, because no-one could challenge their stories of illness
evidence based medicine (EBM)
• Anthropology of Biomedicine: A critical perspective
• Randomised Control Trials (RCT’s):
-highly selective recruitment and enrolment process for trial participants
(“The problem of generalizability” (Lock & Nguyen, 2010, p. 251).
Issues:
-Volunteers tend to me more motivated and therefor unrepresentative of real patients.
-follow up, tracking better than in ordinary busy clinics
-based on the idea of ‘Biological equivalence’
-not neutral or context-free technology of knowledge creation
-devalues the clinical experience
-only collects quantitative data, ignores differentiation and local biologies
enlightenment thinking
began in Newton era, body as a machine metaphor, universal, progressive narrative, the body is an easy thing to diagnose and treat unlike the mind, removed from cultural scrutiny, becomes a domain of medicine, medicine become rational and objective
Rosenhan experiment through CMA perspective
gives doctors the power even with defiance from the person
once someone is labelled in a box do they stay there?
stereotyping of mental health issues
objectivity in what mental health is?
are doctors more likely to symptomise with a certain background?
robots for autism
an example of technology that continues debate about if this is about the individual or society, symptom of biomedicine
Can robots-human relationships equal human-human relationships?
What kinds of ideas about relationships are reflected in robots? Do they
advance inequalities or ameliorate inequalities?
questions:
the social, moral or ethical implications
• unintended consequences
• Who decides what is normal, who programs it
• Why is this preferable to other, low or no-tech options?
• Does it work in practice or only in a lab setting?
• What are the experiences of users?
• What might the invention of social robots to improve health tell us
about medical values and beliefs in Australia
reproductive justice
• Term coined in 1994 by 12 Black and African American women called Women of African Descent for Reproductive Justice (WADR).
social movement strategy that essentially deals with issues surrounding who can have children, who can keep them, who can afford them and who can afford to have healthcare both before and pre natal. prolife and prochoice do not deal with all of these aspects and is also not nuanced enough to deal with different groups of women
3 policies:
The right to have children (fertility access,
combatting sterilisation abuse, birth justice and doula
support)The right to not have children (access to birth control
and abortion)The right to care for families in safe environments, to
care for families with safety and dignity (adoption
justice, childcare support, environmental racism,
family policing such as foster care, education
systems, prisons and policing.
reproductive governance
attempts to govern reproduction through state and non state factors, and concerns what reproductive choices are available to people
australia’s 1960’s breed out the colour campaign
post wwII baby boomer labour contracts
removal of indigenous children from families in the stolen generation
treatment of women in refugee camps
“one for mum, one for dad, and one for the country” peter costello
‘…the mechanisms through which different historical configurations of actors – such as state,
religious, and international financial institutions, NGOs, and social movements – use legislative
controls, economic inducements, moral injunctions, direct coercion, and ethical incitements to
produce, monitor, and control reproductive behaviours and population practices’
bare branches and china’s one child policy
one child policy
reduces innovation from the younger generation, can cause labour and blue collar work shortages, less support for family and more economic and emotional labour for the child, gene diversity decreases,
bare branches
involuntary bachelor villages, marriage becomes even more important and pressurised, women leave the country to find work in the city and child rates decrease, women become commercialised, less money given to the country
ART (Assisted Reproductive Technologies)
assisted reproductive technology (ART) has brought increased freedom and
opportunity for some peopleYet advances in reproductive technology have promoted and maintained
certain power relations, notions of gender, and particular constructions of
the familymany IVF clinics accept only heterosexual married couples as clients, and
many physicians have been unwilling to assist single women, gay or lesbian
couples, welfare recipients, and other women they do not consider to be
good potential mothers (more screening and expectations, also more expensive and eliminatting based on economic factors)moral issues surrounding who donates eggs and how they are organised
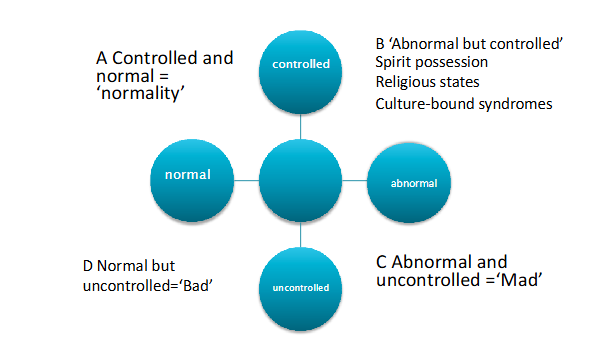
normality and difference
normality
A social or cultural definition is based on
shared beliefsProvide guidelines
Is multidimensional: depends on behaviour,
demeanour, dress, emotional state,
language, etc.The appropriateness to context of the
aboveSocial definition may vary within a culture
4 stages of Helman’s frame work
uncontrolled normality- anti-social behaviours that are considered to be within the norm, but still punishable, crime, people who recognise but break the rules
controlled abnormality- ways to be different that are socially accepted and culturally defined like mardi gras, individually may be attributed to spirits
uncontrolled abnormality- behaviours regarded as social problems, erratic and uncontrolled behaviour and violence, can be madness'
normality
mental health and illness
occur in all countries and are on the rise, 13% increase in the last decade of mental health and substance abuse issues, increasing in children
different cultures have their own systems for diagnosing and curing mental illness, not everything can be under the biomedical label like depression
anthropology vs psychiatry different definitions, A believes it is due to someone being defined as ill based on the perception that their wellbeing is different while P sees it as changes in thinking and emotion
“culture bound syndrome”- mental illnesses that were seen as unusual because of the influence of culture e.g. fear of embarrasing others in japan
cultural psychiatry
mind/body dichotomy, psychotherapy and medication to treat, study and comparrison of mental illness, and its treatment, in different social and cultural groups
diagnoses 3 things:
1. Diagnosis and treatment of mental illness where
the practitioner and the patient are from different
cultural backgrounds
2. The effects on mental health of migration,
urbanisation and social change and disruption
3. Social and health inequalities that contribute to
mental illness (poverty, deprivation)
Kereta film
Experience of mental illness in bali
• Medical pluralism-searching out multiple healing modalities
• Supernatural attrition/acceptance of spirits vs hallucinatory ideas about
his experience
• Idioms of distress-jacket ‘agreed with him’
• Trauma-Western perspective and schizophrenia
• Trauma-war, stillborn (life events)
• Haunted by spirits that reflect the life events
• Social estrangement/social withdrawal
structural/external influences impacting this
• Psychiatry-Western model. Not a not a lot of talk therapy
• State violence/communism/violence and culture of silence imposed
• Pesticides and multi-national companies-Capitalism
• Gender roles-stoicism/grief restricted
concept of social suffering (how bodies remember)
global health and medical humanitarianism
global health
health problems transcend borders and are best adressed through cooperative actions, there are however countries/areas with notable health disparities
idea of health as a global common good and the right to health
improving health for all people by reducing avoidable disease, disabilities and deaths'
the causes or consequences of ill-health circumvent, undermine, or are
oblivious to the territorial boundaries of states, and thus beyond the capacity
of states to address effectively through state institutions aloneIncreasing involvement of the private sector, NGOs, philanthropic agencies,
pharmaceutical industriesis being expored through non state actors such as the gates foundation, and through humantiarian programs such as the WHO and sustainable development goals
anthropologists aim to understand expose and reduce global inequalities (social processes, power relations, development sector), we also consider cultural diversity and assumptions
also involves power over other states and peoples
burden of disease= how a group of people’s health is effected
film about Haiyan in the Phillippines
• “techie aid workers” were treated as second-class citizens in their
own country, where key decisions were imposed by international staff
rather than co-designed with local aid workers
• Resettlement sites lack basic services like water and infrastructure
and also opportunities to make a living. Concrete homes do not feed
empty stomachs. Post-disaster rehabilitation requires a holistic
approach that focuses on the well-being of communities
• the process of rehabilitation is often mediated by the state and
professional NGOs, at the expense of hearing the demands of the
most precarious communities
Reading: ecological approach in Mongolia
What are some of the different ideas about parasites in animal species in Mongolia?
Animals, nature and humans are all on the same equal footing, so treatment of animals is similar to the treatment of humans, relies on mutualism\
Animals can self medicate with the use of certain plants to expel them, using the animal dung as a healing salve , we learn from the animals behaviours
Parasites are given agency, if you make a noise when approach medicine the parasite will hear and react, also humanised, described as boiling when spicy flowers are eaten
What kinds of adaptive human behaviours and relationships with the surrounding ecology form part of the herders' existence ?
The blossoming of the yargui flower is a symbol that a plentiful goat herd is around the corner, part of the observation that they have for life
The lifeblood from animals can flow to humans as all species are interconnected, especially if the hunter knows that they have been consuming healing plants
Health relies on the health of the animals and the surrounding nature
What is threatening the balance between animal and human interaction
The removal of habitat and climate change meaning that mountainside climates are becoming warmer, which reduces the harvest of these medicinal plants
Overgrazing
Increasing demand for supplies such as cashmere
Increased introduction of biomedicine and antibiotics, reduction in the belief of ancient systems
Danger from using bulk and unreliable cheap medicine as a form of experiment
Drugs can effect the quality of dung for example and the microorganisms around, so dung for example takes longer to decompose and effects the landscape and surrounding people's health
Reading: rheumatic fever in australia
What are some of the cultural perception of rheumatic fever and rheumatic heart disease of Aboriginal people in the Northern Territory?
Rheumatic as a phrase isn't used and holds no meaning, so the clinical presentation of the disease immediately poses a problem as they may not know what that means in western biomedical terms
"heart sickness" is something that happens, cause is rarely understood, a lot of connection to nature such as rain or smoke causing coughing, some also believe it is genetics. There is not a connection being made between symptoms and disease.
Often physically manifested as a bug for instance as the cause.
What problems were encountered between Aboriginal people and clinicians?
Aboriginal languages are often just seen as a form of communication not a culture so it can be difficult to communicate that there are different perceptions and values had by them
English is not spoken in the home, only with outsiders and white people, so there is a language barrier. If the detail and prescriptions for example are described in english, how is one meant to understand when that’s not their language? The words used in english do not have a counterpart, so they cannot be understood. The people who understand are more likely to understand the seriousness of their disease.
Clinicians do not understand that their not being understood, so they skip straight past the pronunciation.
There is no communication about whats actually happening and as a result autonomy is being lost. People who had been given injections for 10 years were still asking what it did. Also didn't know how long it would go for, and clinicians responded that they didn’t want to frighten them (a problem in itself!)
Different understanding of the word of sickness for example, to them it means something that comes from the earth so there is translation issues even with a translator
There is still also uncertainty about whether treatment is for their benefit or the clinicians, there is a level of distrust.
Can you describe the link between communicative competency and Aboriginal health?
You can’t just name the conditon, you have to try to describe it, also some cultural understanding would be beneficial.
Reading: endometriosis in Australia
it took years for women to get a diagnosis and even longer to get treatment
women in rural areas were more likely to not receive adequate healthcare and treatment
expectation that period pain is normal and to just ‘suck it up’, associated with what it means to be a woman, pain rarely discussed, often self managed
there was a catalyst that caused the woman to seek treatment (professional recommendation, social disruption, impacts self, ‘gut feeling’)
2 cycles: the first is pain with self management and the second involved gp referral
Reading: masculinites in denmark
health issues and problems are taken on the shoulder and treated as normal
keep things that are private in the home and dont discuss them because no one wants to hear them
strong and independent
capable of handling and problem and dont need help
beer or something masculine has to be involved to socialise
non-biomedical healthcare is frowned upon, women are allowed to be ‘free’ and ‘crazy’ but men have to be the logical ones
this is a theraputic landscape as it describes all aspects of the health from the non biomedical therapies to the chemical treatment to the emotions and the timescale behind it
Reading: roundhouse in west timor
male and female quaters seperated in the house, the mother sits in the rear near the kitchen utensils, female domains more protected from eyes of guests
women have been sacrificed to provide food to the earth, so when you enter you must bow to pay respect to the food at the door
the two poles representing the mother and the father of the two married people are united with gods pole in the centre
father seen as the leader of the family, single leadership
reading: local biologies
menopause is mainly based around experiences from northern american or european women, from this we can learn different experiences are common, for example japanese women didnt report hot flashes as often as canadian women
with kuru and the fore population, some individuals are at increased risk due to polymorphisms in their dna, the kuru was also acting as a natural selecting factor that was eliminating a certain amino acid
social processes can entangle with the physical
reading: egg donation and racialised eggs
The ways in which race lives on in these
vital substances reproduce old ideas of
race and hold important implications for
notions of justice, inheritance, and
identity
• Couples prefer certain donors on the basis of ‘race’, education,
appearance, cultural assumptions
• These often are a mismatch with the majority of donors who
are socio-economically disadvantaged, ‘undesirable’ minorities
donating for income (in the US context)
• ‘Selling’ eggs leads to assumptions and myths about the
biology of race and inheritance
• human eggs are thus racialized in various ways in order to
convert them into key commodities of the fertility industry
• what does this mean for racial and reproductive justice?
• the demand for better options for “under-represented
ethnicities” in gamete [egg cell] donation reflect calls for
increased equity and representation in health care
• Yet, such calls seem to overlap with – indeed, rely on – the
acceptance of race as biological, as it is configured through
phenotype, appearance, blood, gene pools, and individual
genetics
reading: reproductive justice (US)
includes the effects of colonialism and people of colour into the conversation, adds historical reasoning
deals with the question of legitimacy- who gets to be a legitimate mother? what do race and class have to do with this? who is denied this? underwrites that motherhood is a class privillege
impact of politicians and politics on healthcare
attack on vulnerability, issues surrounding who is defined as a women and intersections with gender spectrum
reading: birthing on country (australia)
loss of bush midwives
inner city setting had changed the landscape of the birthing process
lack of access to traditional sites had reduced the mental health and connection to ancestors
it was easier to include your child in a particular aboriginal group if they were born on country, this made the beurocratic system easier for families
reading: migrant workers in china
social stratification: the poors experience with health is worse, which in turn makes the disease worse
more stress created as they cant afford to not work, effects income
chronic illness is chronic, making it hard to work and get employment, not just them but also their families
they either have to pick treatment or labour; they dont have the time and money to do both, unlike the rich, disease isn’t something you can get fixed/treated, theres a process that is long and difficult but there’s less support for it
reading: disability worlds
the exposure and integration of disabled people into society has grown recently as in the past they were hidden from view or institutionalised, left parents unprepared with how to raise disabled children
discusses the process of disability awareness, then the study of disabilities in the academic fields and then the limiting factors of it
60’s and 70’s saw a range of changes including more education and funding for legislation and hospitals
disability is socially constructed, and they aren’t broken or to the side, its just a new normal, also how social factors describe what counts as a disability
reading: theraputic citizens in tanzania
theraputic citizenship is building an identity not based on nationality but on health and conditions. But in this, governments use this to decide who lives and who dies . theraputic privilage in this article is the process of triaging people, who gets priority? and how do we treat refugees who dont have the privillege of freedom? which diseases require treatment more than others?
refugee camps do not have the resources or referals for complex diagnoses and treatment
staffing issues, medical professionals can diagnose the issue but cannot stay to monitor the situation or communicate their expertise
refugees are customers/represent nonstate organisations and relations, if something goes wrong it may sour founding and representations of these organisation
referals make this decision, if they get denied they dont have a choice, prognosis was quite important “they’re going to die anyway”
very subjective system
reading: slow research- local as method
• Too much emphasis on RCTs and quantitative evidence as if it is
objective
• Too many ‘roll outs’ of universal policies
• Too much political investment in global scale interventions can often
mean an unwillingness to adjust to specific local circumstances
Ways to assert a "slow research" agenda (Adams et al 2014):
1. Assume that the facts about health are found in an “often
incalculable mosaic of evidence”
2. Resist the pull of universal new policies; be wary of “roll-
outs” (shifting to the new goals of a global effort does not
always mean that local communities are being served)
3. Have a keen eye for “the tyranny of the global”: political
investments in global scale interventions and an unwillingness to
adjust to specific local circumstances that might actually improve
outcomes
4. Value what is already working, even if that means rejecting the
prestige and fiscal opportunities of the new (p.185)
5. See local as not just a condition of time or place, but a method
6. Develop not just a deep understanding of local culture, but of local
politics, history and histories of medical intervention
reading: singer on biocultural approach
What is meant by bioculturalism or the biosociocultural approach?
Includes the perspectives of society and human emotions into the approach of health, such as with the AIDS crisis, questions would also be asked about behaviours leading to its contraction , and which groups are more vulnerable as well as how the virus destroys the immune system
Three key behaviours: the intersection between the cultural, the social and the biological and how they effect a health condition. All are equally important to the health of an individual. They're all different and they all interact with each other
What is meant by medicalization?
Role of medicine in social control, giving behaviour to a medical label. For example if someone says you're "overreacting", if you make it medicalised, there is now less stigma and emotion around it because hormones and physical reasons have been assigned to it, from badness to sickness
Can you think of an example?
Mental health would be a large example of this, instead of saying to someone that they're depressed so they should just cheer up, if you assign physical traits to it such as a medical lack of dopamine, it suddenly seems uncontrollable
What are some ways that anthropology has been used to understand and improve human health?
Recognises how people around the diseased person are effected, studies human relationships and emotions and how they change with health. Bluebond-Langer used research on CF to show how to conflict manage families with CF, and also reduce the impact on siblings mental health
Used in association with communities to remove factors that contribute to the disease, such as removing rubbish and cleaning water supplies in the dengue outbreak
Can you think of another health problem that could be better resolved using anthropological ideas or methods?
COVID-19 would have been an interesting medical situation to investigate, how the isolation effected the recovery and mental health of the afflicted, maybe creating management plans so that isolation isn't a barrier to recovery
disease causation
supernatural causation
mystical
animalistic
magical
natural causation
humoral system imbalance
infection
accident
deterioration
placebo effect, can also cause biological reductionism
qualitive research
seeks meaning and understanding, does not use statistics, who what when where why, flexible, seeks more depth than breadth, useful when research is not well understood, helps understanding and builds theory
interviews (casual, structured, individual), observations, diaries, focus groups
biopolitics
Biopolitics are the strategies through which biological aspects of citizens/subjects become the target of political strategies
• Examples: fertility control; immunisations; healthy living
campaigns; health screening/medical certificates; social
payments drug testing
• Governing the life of the population
disability
• Social conditions exclude full participation in society
• Who’s allowed to be human? (Goodley 2021)
• Western philosophy of ‘humanism’ problematically centred particular kinds of
humans only
idea of what is a disability changes and develops with time e.g. the perception of autism