2) High power lens
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
What are the best lens and frame choices for high prescriptions (high plus or high minus)?
Both
↓ eye size frame (to cut off excess ET in (-) & overall weight in (+))
↓ vertex distance
frame PD = patient's PD.
↑ n (for thinner, lighter lens)
AR coating to ↓ reflections
.
High (-) lenses
use hide-a-bevel to ↓ myopic rings
.
High (+) lenses
aspheric lenses (↓ lens thickness)
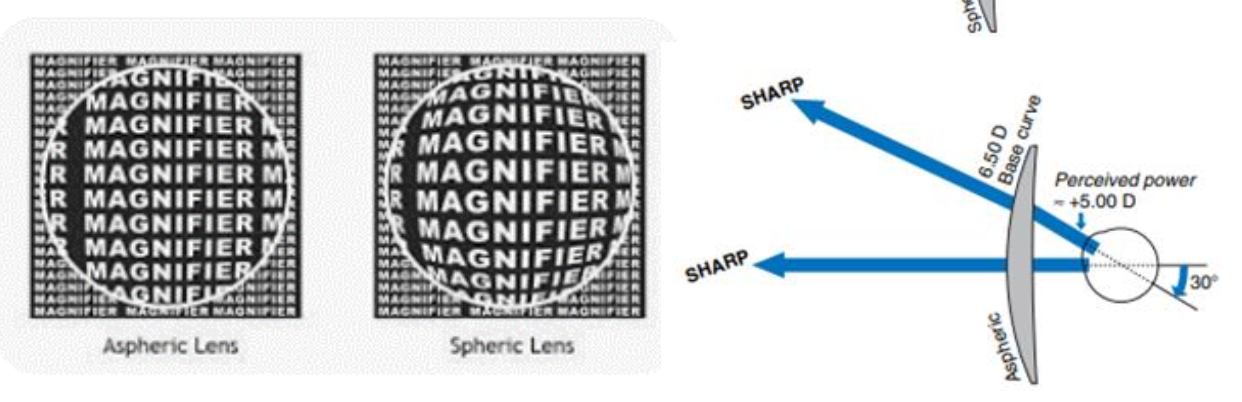
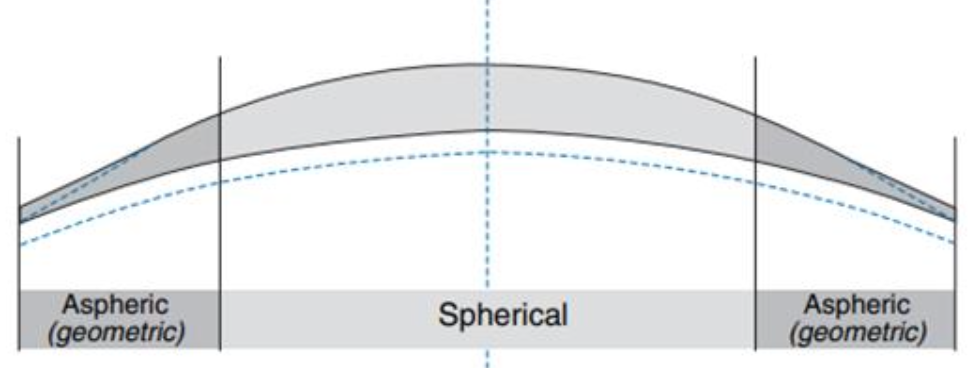
How does an aspheric design affect high (+) lenses?
periphery is flattened → ↑ ET (thickens)
flatter front surface allows a plano slab to be removed → ↓CT (thinner)
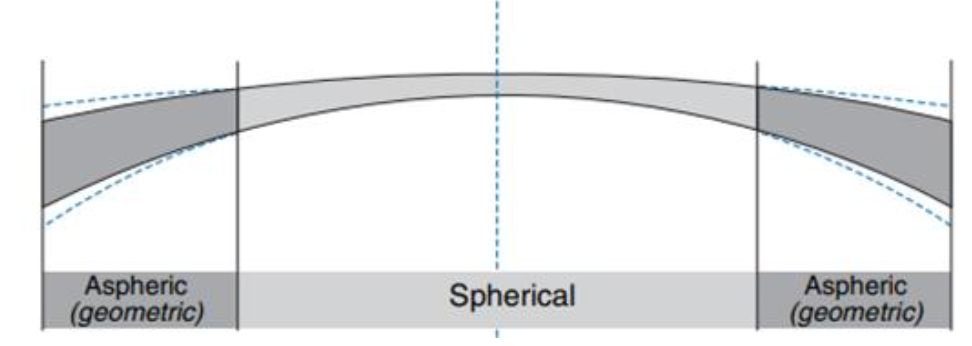
How does an aspheric design affect high (-) lenses?
↓ ET by:
Steepening the front periphery
Flattening the back periphery
True or False - Both aspheric and atoric lenses can be single vision, multifocal, or progressive.
True
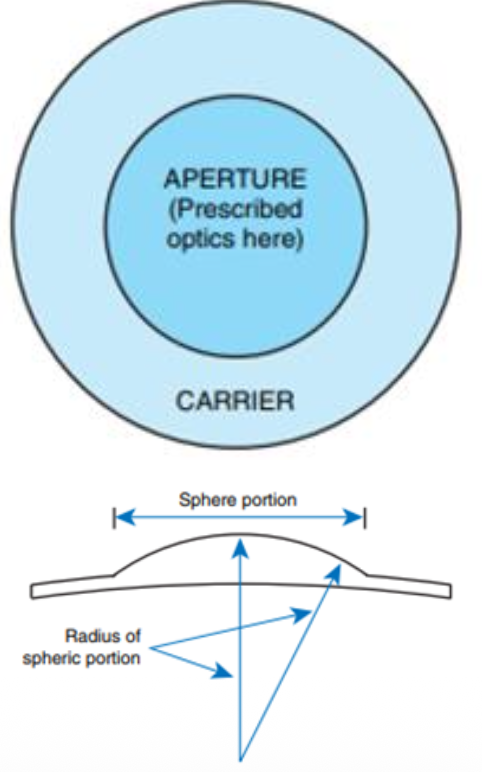
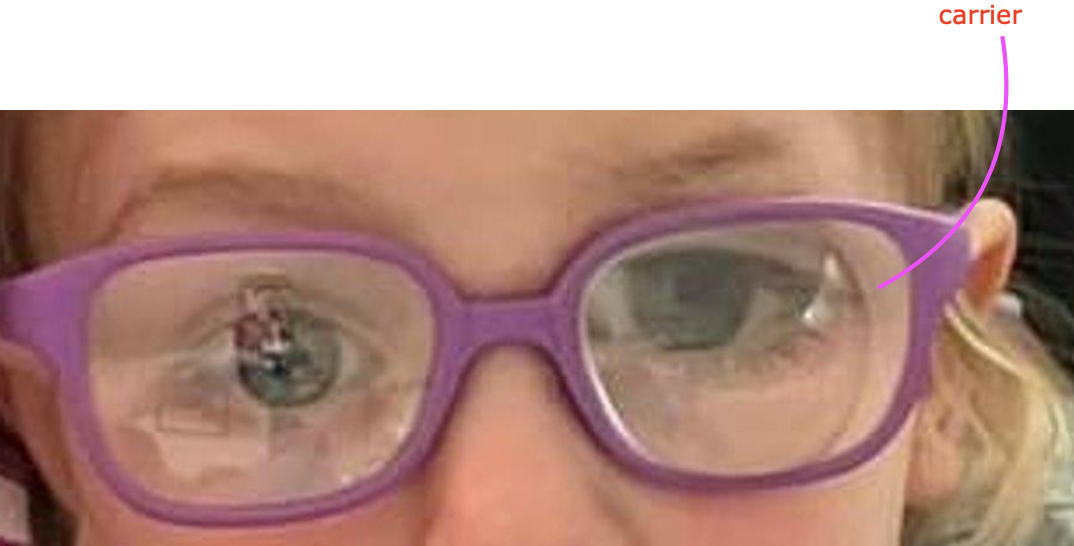
What are Lenticular Lenses?
→ central area with the proper rx (aperture) + outer skirt is plano/near plano (carrier)
useful for high powered (+) or (-) lenses
carrier size is adjusted to fit the frame
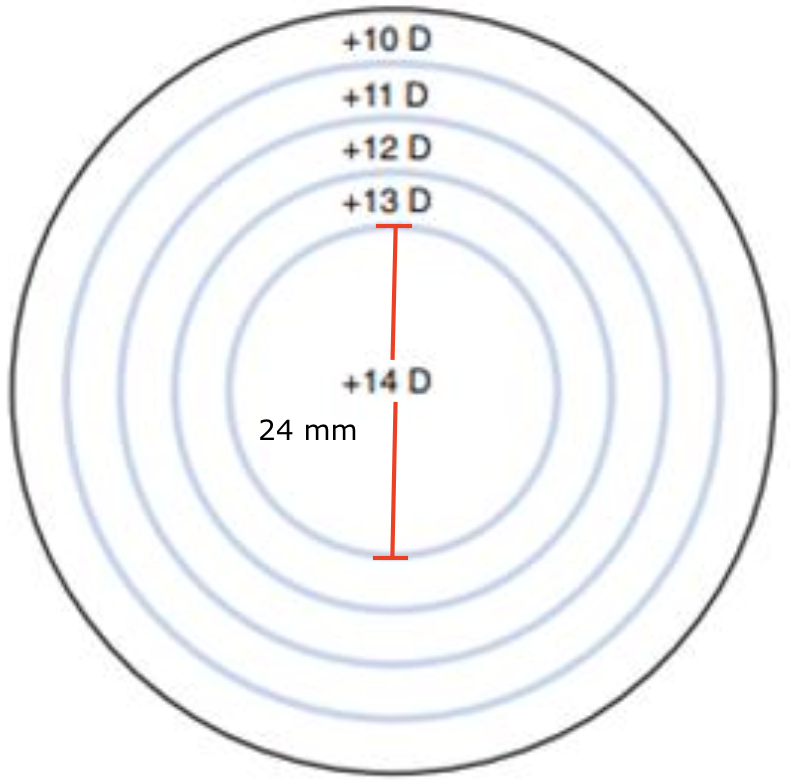
What is the Welsh 4-Drop?
→ 24 mm central area surrounded by 4 concentric rings where each drops by 1.00 D in power
type of lenticular lenses
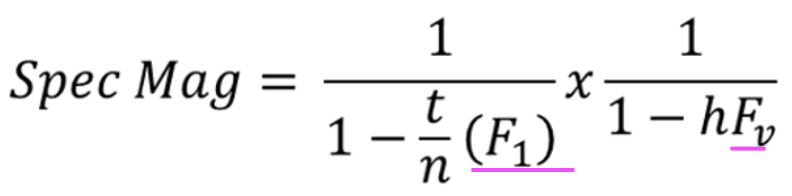
How does shape mag and power mag change for (+) lens?
↑ shape mag
↑ power mag
How can (-) lenticulars be made?
very flat BC
(-) BC → minus "bowl" in the lens center
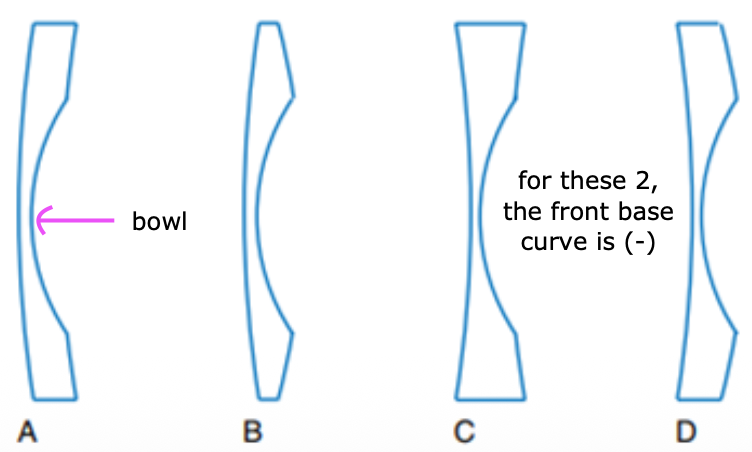
What is myodisc?
→ trade name for high (-) power lens, where only in the center (the bowl), and the rest of the lens is thin and plano(the carrier)
BC = flat

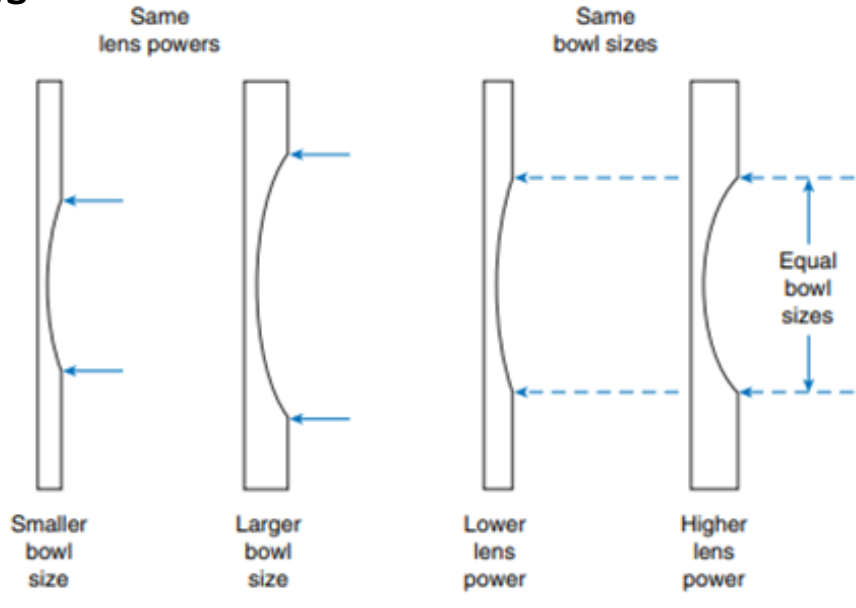
True or False - Bowl sizes and power are dependent on each other.
No
For what lens powers does vertex distance and it’s role on Feffective come into play?
greater than +/-4.00
How does changing vertex distance affect the effective power of a lens and the prescription?
Move lens farther from the eye → lens become effectively more (+)
prescribe more (-)
Move lens closer to the eye → lens becomes effectively more (-)
prescribe more (+)
this is why CL Rx is more plus than glasses
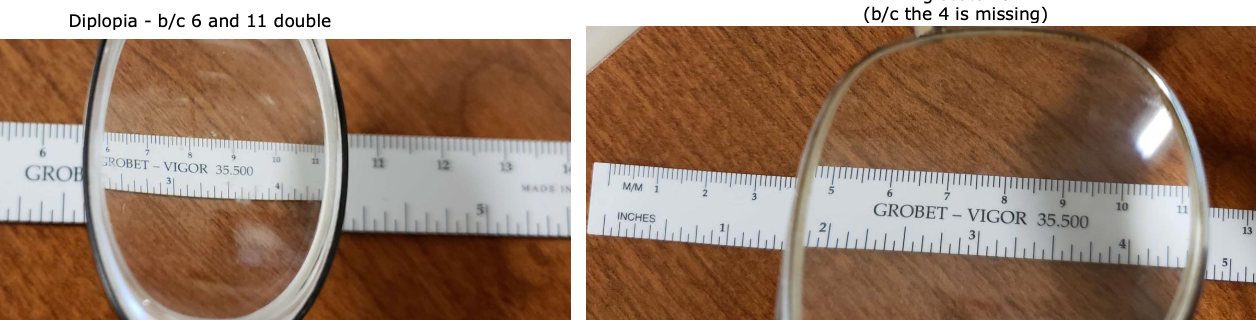
What prismatic effects are induced in a high (-) vs high (+) lens?
High (-) = diplopia
High (+) = ring scotoma — "Jack in the box" phenomenon
What is Aphakia? What refractive error does it create?
→ crystalline lens is absent from the eye
large amount of uncorrected hyperopia (b/c eye becomes more minus → hyperopia)
if aphakic in 1 eye, the anisometropia created with the aphakia → aniseikonia
What is Pseudophakia? How can the patient can aniseikonia?
→ crystalline lens has been replaced by an artificial lens
if pt has substantial Rx before cataract surgery and pseudophakia brought them to plano in one eye, the anisometropia → aniseikonia
What is the best way to correct for Aphakia?
→ via CL
CL is worn close to the entrance pupil → dramatically ↓ mag
since CL moves with eye, it ↓ aberrations
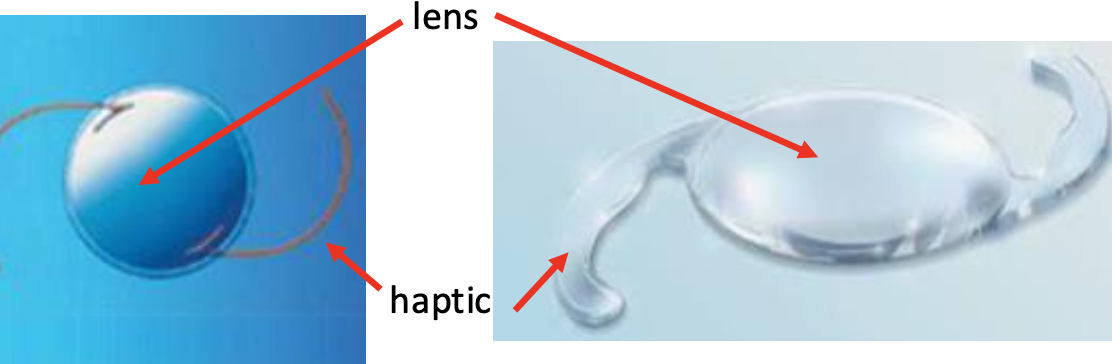
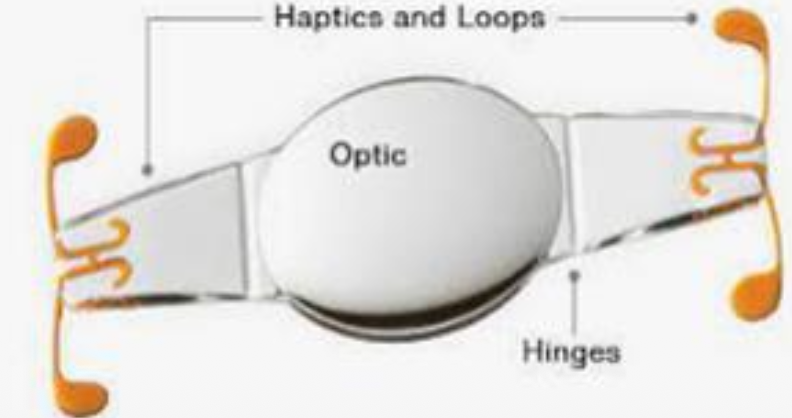
What is an IOL?
→ artificial lens implanted inside the eye at or near the location of the natural lens
gives plano rx (but residual astigmatism or ametropia, it can be fixed with "normal" glasses)
1 piece or 3 piece
haptic holds the lens in place
aim for distance, near, or monovision
What are the different locations/types of intraocular lenses (IOLs) and why did placement change over time?
Early IOLs: Placed in the anterior chamber with haptics resting in the angle → high risk of GLC due to damage/interference with aq drainage, so iridectomy was commonly performed to prevent pupillary block
Iris clip IOL: Attached directly to the iris for support
Sutured AC IOL: Anterior chamber IOL secured sutured to the iris
Modern IOLs: Usually placed in the posterior chamber within the capsular bag
List the 3 potential problems you can run into with IOLs. Name the respective visual problem associated with it.
Tilted → astigmatism
Mis-placed → prismatic effect
Displaced/dislocated → diplopia
caused by trauma or weak zonules

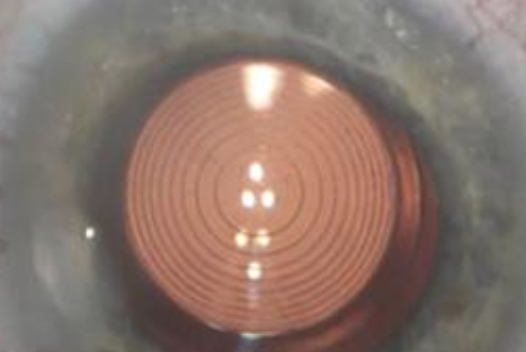
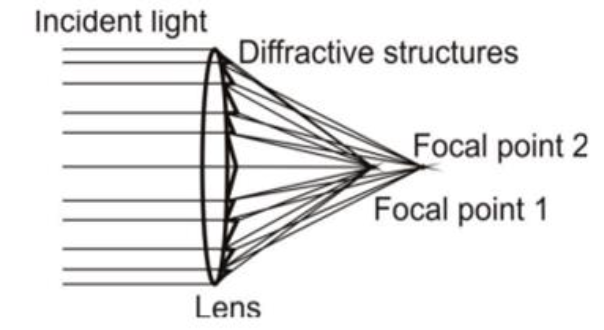
How can multifocal IOL account for distance and near vision?
via concentric zones
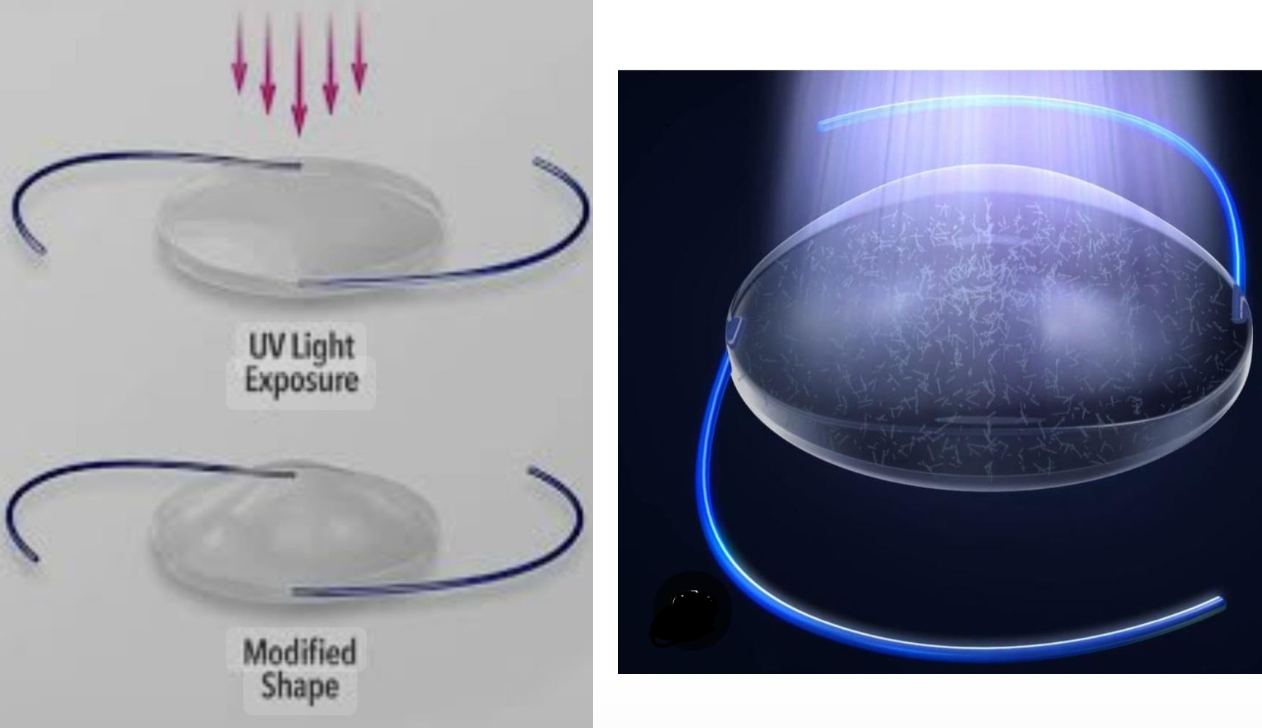
How are accommodative IOLs placed?
→ placed in the capsule
have hinges that bend when the ciliary muscle moves (to allow for accommodation)
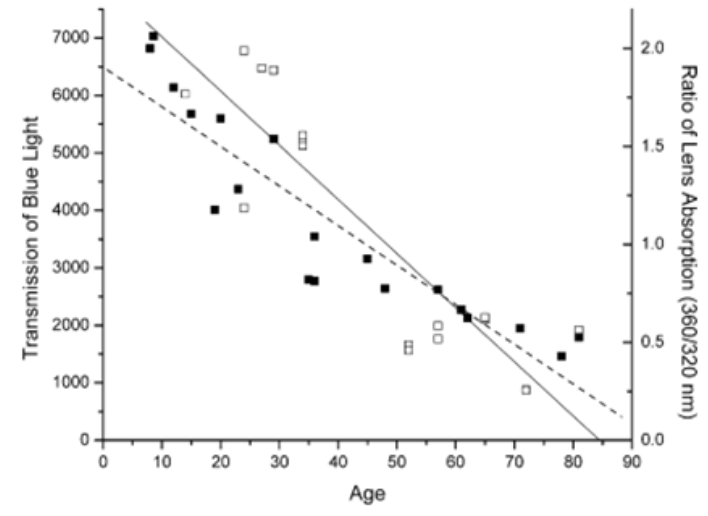
Why are UV-blocking IOLs important after cataract surgery?
→ natural lens normally absorbs UV light, protecting the retina
retina can be exposed to harmful wavelengths after lens removal surgery
Modern IOLs block UV light and ↓ short-wavelength transmission to mimic the protective function of the natural lens
How does age affect blue light transmissions?
↑ Age = ↓ blue light transmitted (↑ absorbed)