Lecture 10: Suture Materials and Patterns
1/110
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
111 Terms
choosing suture material
size and chemical make-up
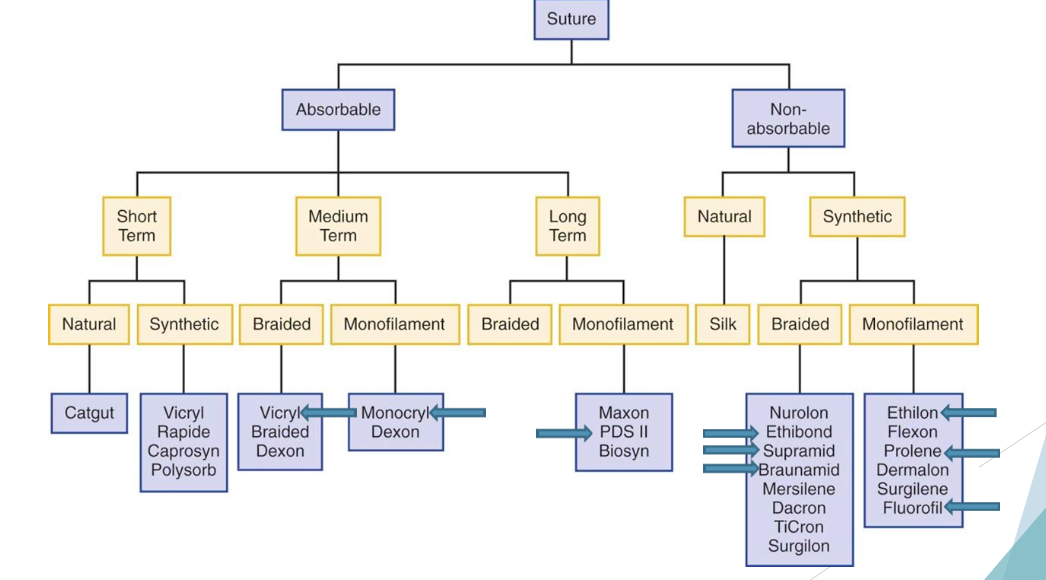
natural vs synthetic
think:
strength of closure —> how long does it need to last?
choosing suture material
absorbable vs nonabsorbable
think:
inside or outside of body?
inflammatory response?
choosing suture material
monofilament vs multifilament
think:
wound contamination
how to choose suture material for LA:
same options as SA, only BIGGER!
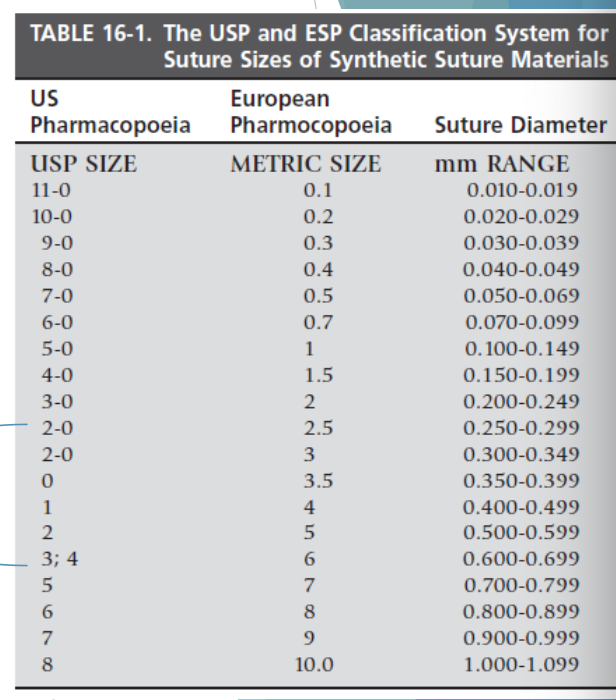
Typitcally use 2-0 for SQ and 2 or 3 for linea alba!
suture selection principles:
suture should be as strong as the normal tissue through which it is placed
tensile strength reduction over time should correspond to healing of the affected tissue
suture is not needed after the wound is healed
the strength of the wound is more dependent on the tissue’s ability to hold the suture than the suture material itself
suture with elasticity is ideal for?
skin closure (adapts to wound edema)
suture with high stiffness is chosen for what?
abdominal closure, herniorraphy, prosthesis, etc
what will oversize suture do to your closure?
it will WEAKEN it! due to excessive tissue rxn
bigger is not always better!
what to do with wounds under tension
increasing the number of sutures (or using a tension relieveing suture pattern) is better than increasing suture size
suture strength needs to do what?
last to support healing tissueand withstand physiological forces during recovery
how long do internal organs and subQ take to heal?
relatively fast
few days
full strength in a couple of weeks
how long does fascia take to heal?
slowly
couple weeks
full strength in a couple months
linea alba: baseline strength at 8 weeks
how long does skin take to heal?
seals within 1 day
primary incision heals in 10 - 14 days
full strength < 30 daysb
better apposition —>
decreased healing time
commonly used suture in large animals
if you can’t remove it, what suture do you use - absorbable or nonabsorbable?
use absorbable
SubQ, organs, ligatures
if you can remove it, what suture do you use?
non-absorbable
skin
ideally should be inert —> reduces inflammation = speeds healing
what is needed for suture absorption in absorbable suture?
inflammation
increase suture size = increase volume of knot which is important to know why?
this is more important than number of throws on knot when it comes inflammation
increased volume of knots =
increased inflammation
increased inflammation =
weaken closure
use the smallest suture possible!!!
which needle is the most commonly used in vet med?
3/8 or ½ circle
more ergonomic to use
¼ circle = opthalmologic surgery
5/8 circle: confined or deep locations
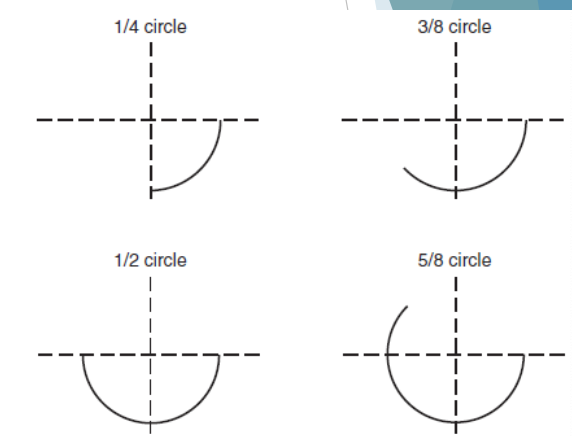
needle sizes
determinent for picking a needle for a wound:
want to be able to reaach across both sides of the wound with the needle
taper point needle
round needle shaft does not enlarge hole as it passes through
good for delicate tissue
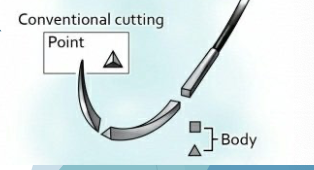
reverse cutting needle
cutting edge on the convex (outer) side
makes needle stronger than conventional cutting
less risk of tissue cut out
skin, fibrous tissue
conventional cutting
uncommon
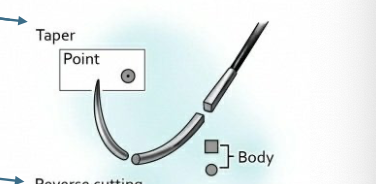
taper point needle

reverse cutting needle
conventional cutting needle
Buhner needle
special needle in LA sx
used to purse string prolapses

buhner needle
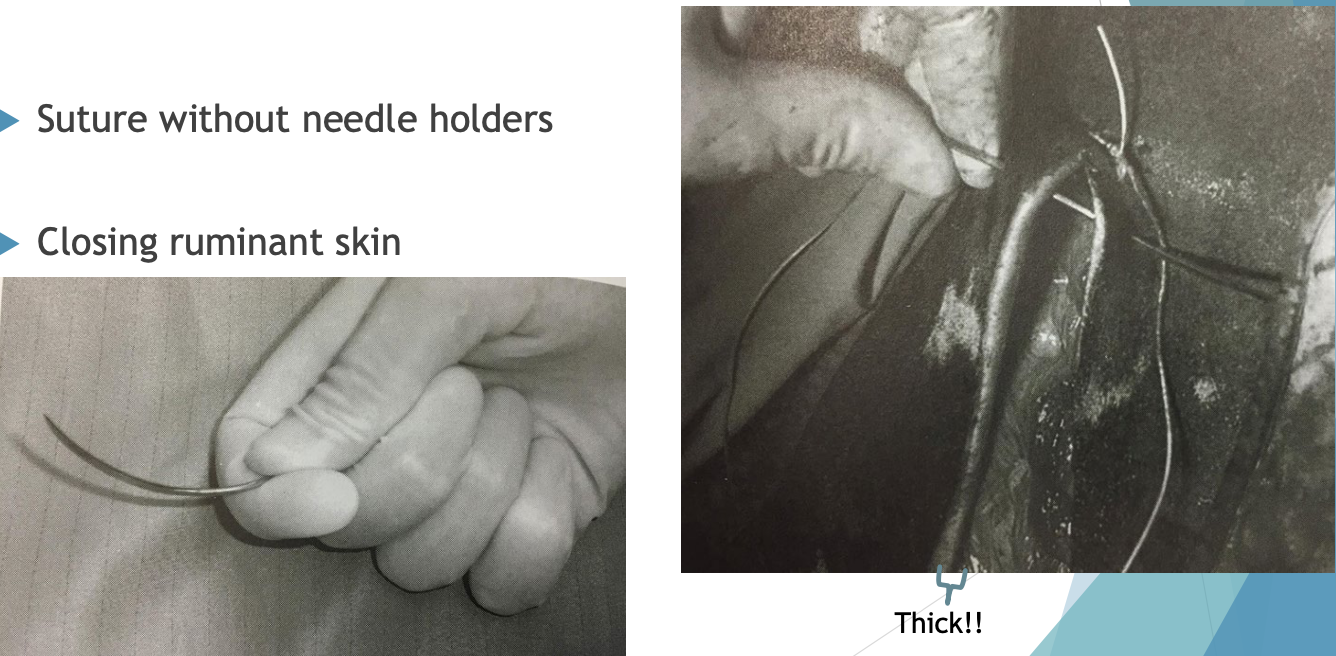
S needle
special needle in LA sx
used to close cow skin
negates need for needle drivers
easier to punch through thick skin
use suture on a reel

S needle
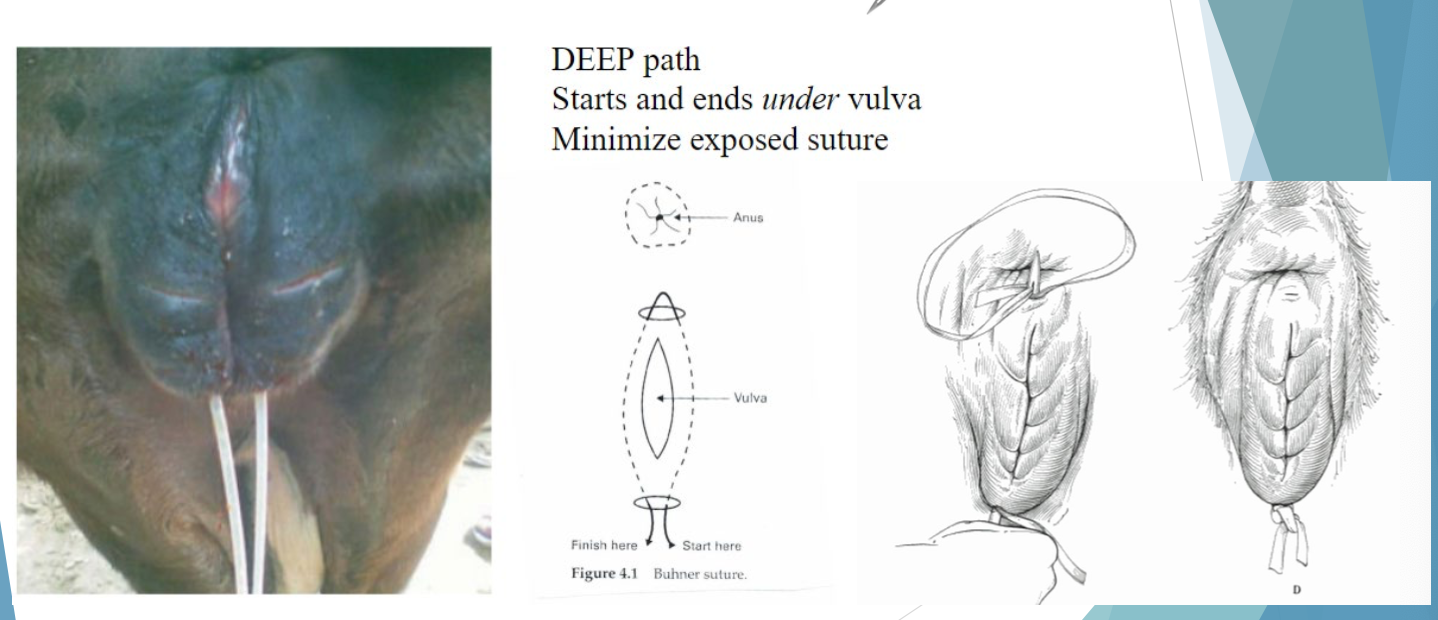
Buehner needle and suture vaginal prolapse
DEEP path
starts and ends under the vulva
minimize exposed suture
S needle usage
suture without needle holders
closing ruminant skin
good for thick skin!!
knot tying techniques
knot = weakest point in the suture pattern
even if its perfect!!
important to do this correctly to prevent dehiscence of incision

wound dehiscence. Ouchie
simple throw
half a knot
square knot
2 simple throws that are reversed
surgeon’s throw
placed when a square throw is slipping
more friction
more suture material left in the wound
granny knot: 2 throws, NOT reversed
NOT secure, do NOT do this
half hitch
pulling up on the suture end instead of across
NOT secure
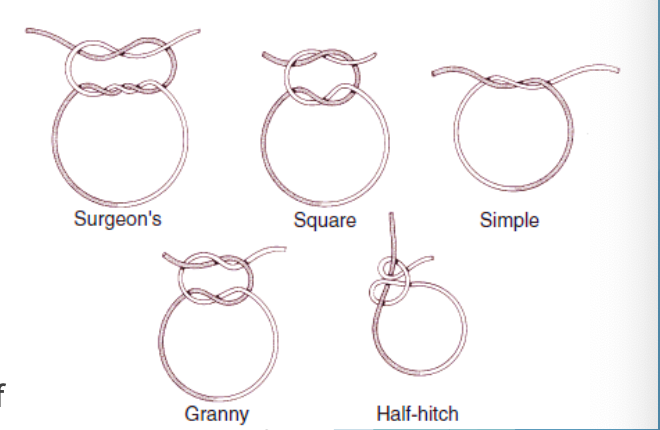
types of knots
knot security
suture type:
memory and coefficient of friction
body fluids contact suture and can change the frictional behavior of suture
knot security
number of throws:
2-0 PDS (polydiaxanone) or nylon: 4 throws are needed for a secure ligature
larger suture = needs 5 throws!
#2 or #3 Vicryl (polyglactin 910) or #2 PDS (polydioxanone)
for knot security, how long should the tag length be?
at least 3mm in length
when tying loops, how can you create knot security?
need knot security!
increasing suture size =
decreasing knot security!
monofilament for skin suturing =
decrease bacterial transport into deeper tissues
nonabsorbable suture we like to use in the skin:
polypropylene (Prolene)
nylon
common suture pattern for skin:
simple interrupted with no tension (USP 2-0)
± tension relieving patterns (;arger suture: 0, 1 or 2)
specifics on how to suture skin:
apposition of tissues edges or slight eversion
bites about 5mm from skin edge
collagenase activity within 5mm of wound —> sutures may pull through
wounds may require suture to be further away
sutures for fascia
most common in LA - linea alba!
species difference: bites 15mm away from cut edge
extra suture needed to combat potential abdominal distension
suture to close fascia:
polyglactin 910 (Vicryl), Polydioxanone (PDS)
size: #2-7 (#2 or #3 most common)
what type of suture do we commonly use in cattle to close fascia?
catgut! It’s cheap!
don’t use in horses, too much inflammation
suture specific for delicate tissue like subcutaneous, GI organs:
PDS (polydioxanone), Vicryl (polyglactin 910), Monocryl (poliglecaprone)
typically use USP 2-0
Suture pattern for GI tract:
inverting suture patterns
Lembert
Simple continuous oversewn with a Cushings
suture for contaminated wounds:
monofilament only!
nonabsorbable suture - inert
elastic - allows for tissue swelling
all wounds in horses are contaminated!!!
suture to use in farm animals
ideally same suture as other animals ——>
to reduce cost:
chromic cat gut
suture on a reel
supramid
braided nylon
braunamid
braided polyamide

when to remove sutures
10 - 14 days
what is staging removal for wounds under tension?
take out every other suture or every 1/3 initially
most common absorbable suture:
polydiaxanone - PDO/PDS
polyglactin 910 - Vicryl
poliglecarpone 25 - Monocryl
polyglyconate - PGA/Dexon
most common non-absorbable suture:
polypropylene - Prolene
polybutester - Novafil
coated polyster - Ethibond Excel
nylon - Ethilon
skin staplers facts
stainless steel
inert
fast to put in
stable remover or hemostat to remove
patient recheck opportunity
wounds with NO tension
appose wound edges

skin staplers
stable removal can be:
tough!
NOT for mini colics
foals are really tough too!!!

large animal suture patterns are:
the same as small animal (:
few that are more common in large animal though.
inverting tissue pattern
more common in LA
invert the tissue edges to help make a seal
uses: uterus, GI tract, urinary bladder
suture does NOT come out the tissue edge
adjacent to the edge to fold in some tissue
examples: Utrecht, Cushing, Lembert

inverting suture pattern
Utrecht is commonly used on which organ?
uterus!
Utrecht suture pattern
Cushing pattern is commonly used on which organ?
GI, urinary bladder
often combined with a simple continuous first
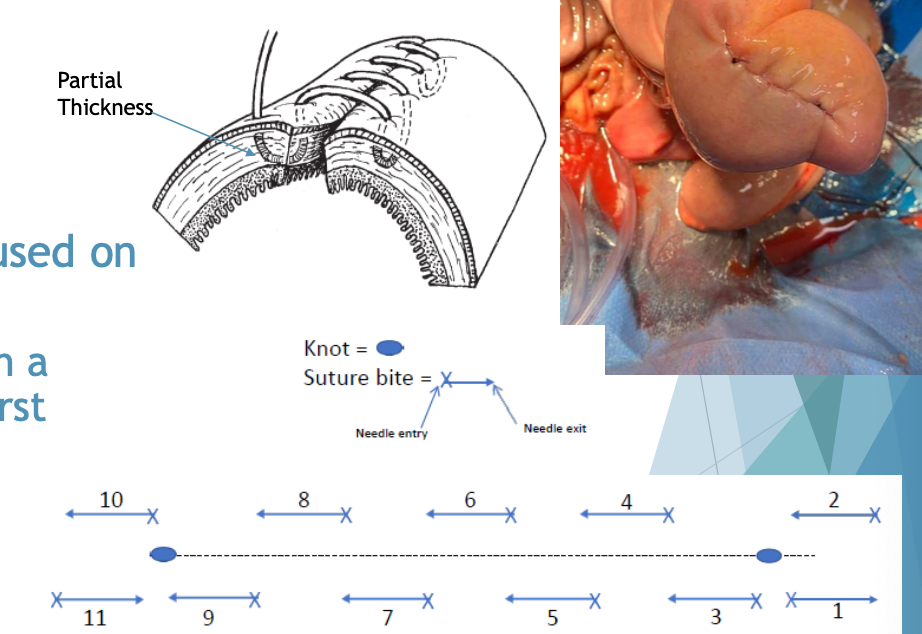
Cushing suture pattern
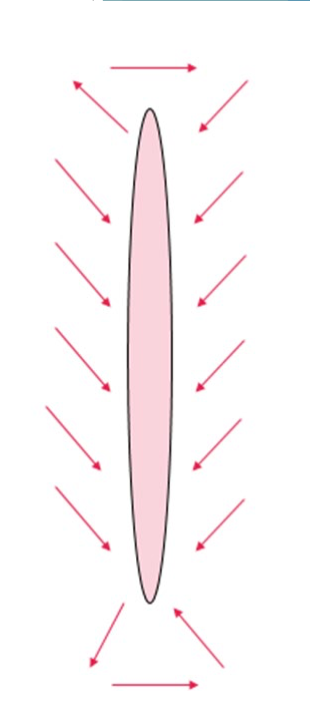
Lembert suture pattern is commonly used on:
GI or urinary bladder
be careful not to make a “cuff” of tissue deep to your suture line
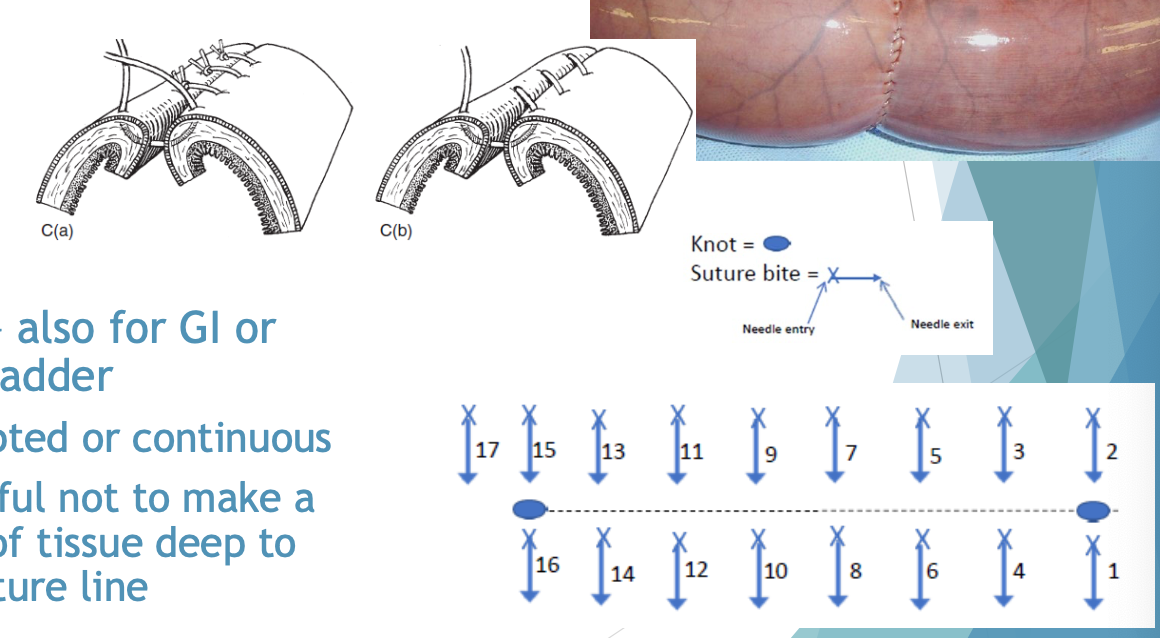
Lembert suture pattern
suturing wound under tension
tension impedes healing
impairs blood supply
prevents perfect apposition
shear stress on wound

Langer’s lines:
relaxed skin tension lines
incision parallel = least tension
incision perpendicular = most tension
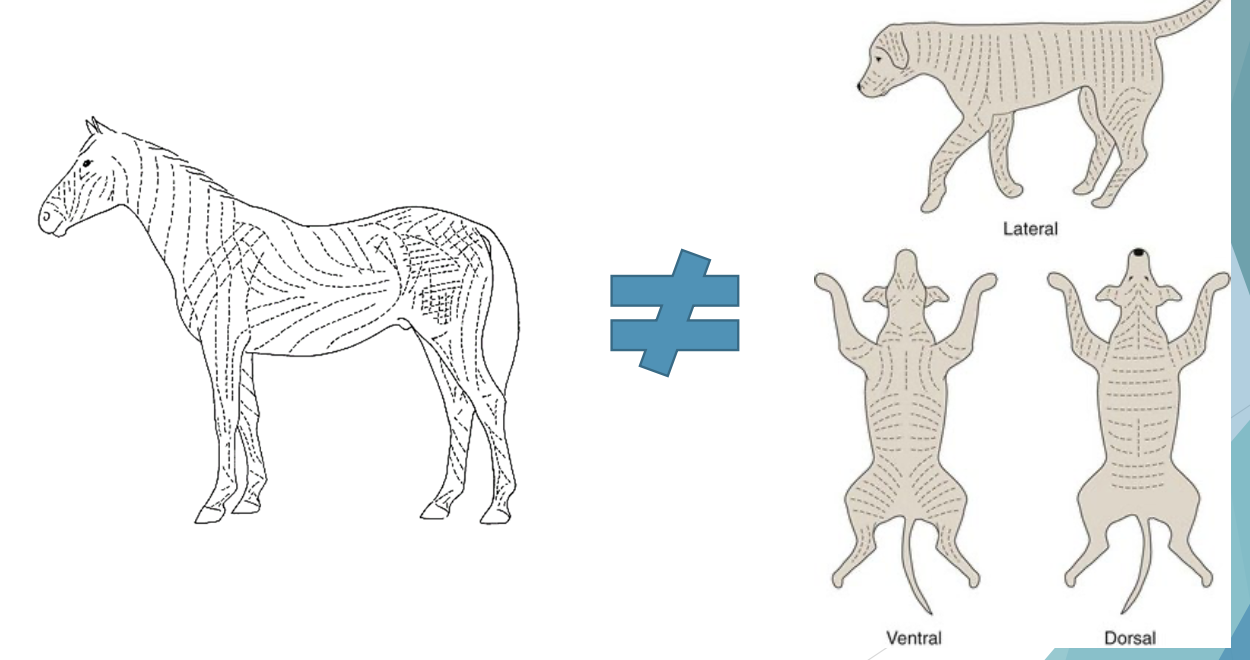
LA and SA langer’s lines are:
different!
preferable why to suture wounds under tension:
use limb immobilization
add more sutures
use tension-relieving techniques
what is not preferable when suturing wounds under tension?
using bigger suture
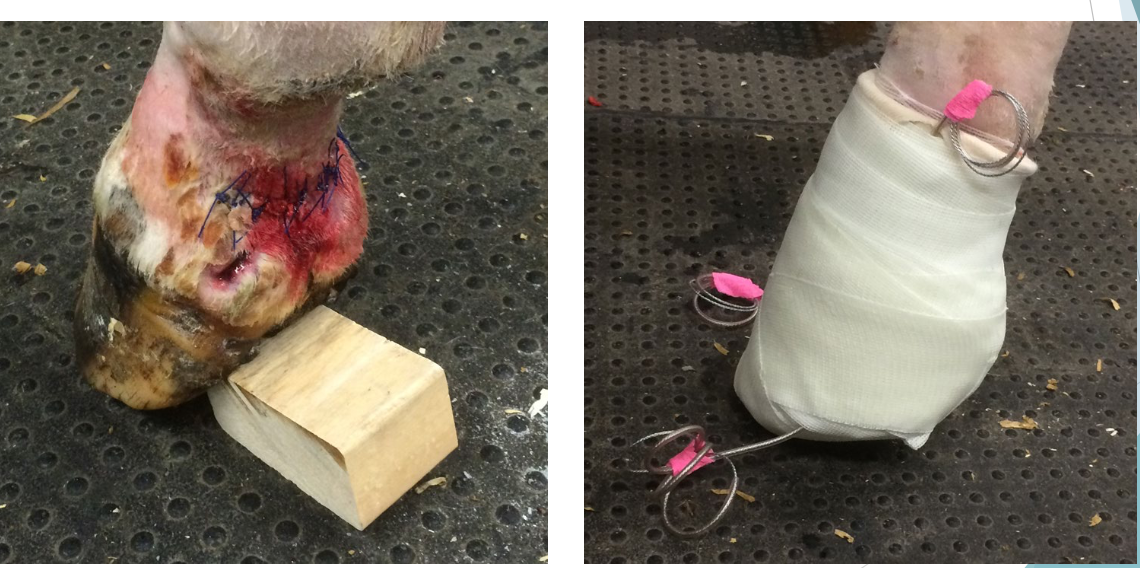
wound/limb immobilization

splint/bandaging as wound/limb immobilization
tension relieving techniques
release incisions
walking sutures
tension relieving suture patterns
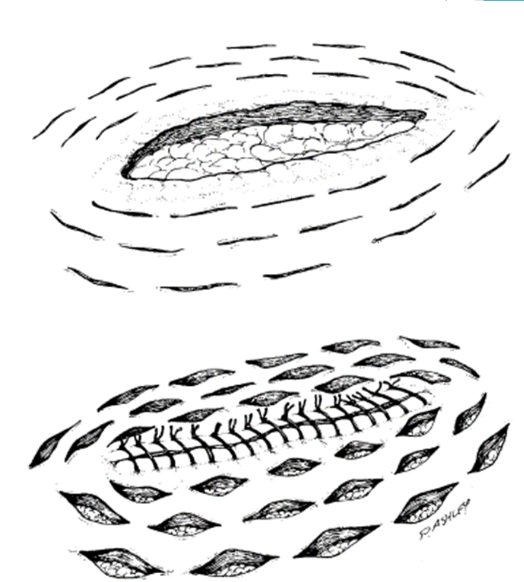
± use of stent
± combo patterns
skin tension lines

relief incisions
close the primary wound and leave the relief incisions to heal by second intention
tension relieving pattern
walking sutures
using your suture to “pull” the skin over the top of the defect
even out tension
obliterate dead space
no closer than 2-3 cm apart
can increase inflammatory response with extra suture

tension relieving pattern
stents
distribute tension more evnely along suture to prevent pull-through
staged removal if needed
avoid using a stented closure on its own
always a combo of stents and other suture patterns
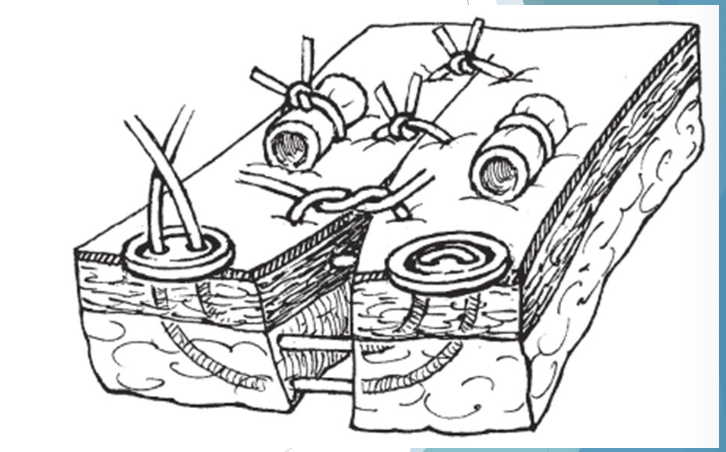
stents

walking sutures
tension relieving pattern
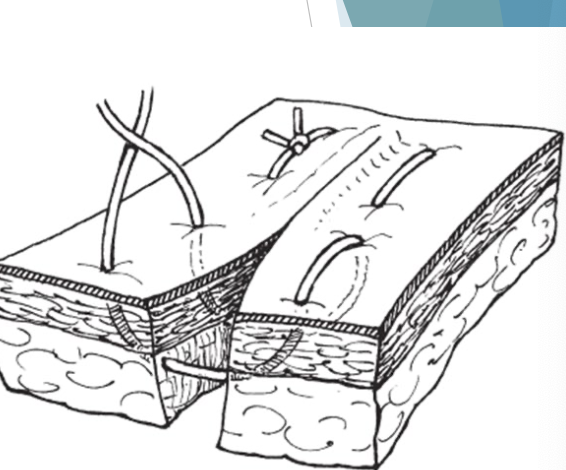
vertical mattress
less impingement of blood supply compared to horizontal mattress
good apposition, but some eversion
interrupted only
bites are perpendicular to cut edge
vertical mattress
tension relieving pattern
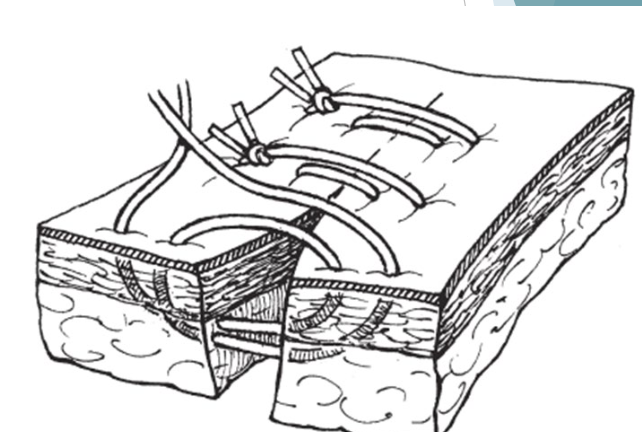
horiztonal mattress
strong tension relieving - will not tear through tissue
but tends to impede blood supply
RARELY use without stents
most eversion possible
can apply in continuous pattern
visible bites are parallel to cut edge
horizontal mattress
tension relieving pattern
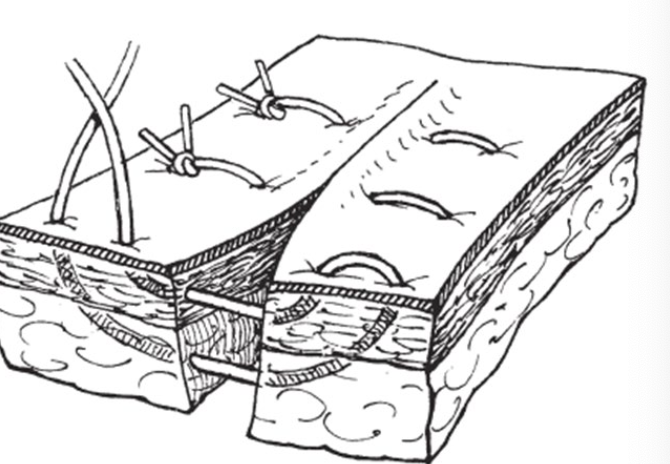
near-far-far-near
excellent apposition and tension relief
interrupted only
most suture in wound
near-far-far-near
special suture pattern
ford interlocking
mild tension relieving continous pattern
reduces suture disruption if one part breaks
good apposition
commonly used to close skin on cow flank incision
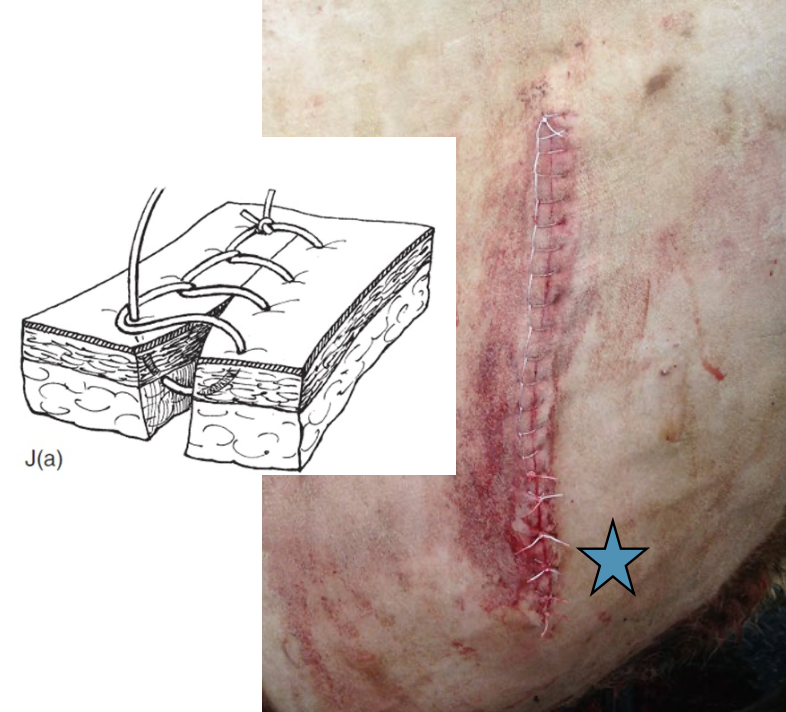
Ford Interlocking Pattern
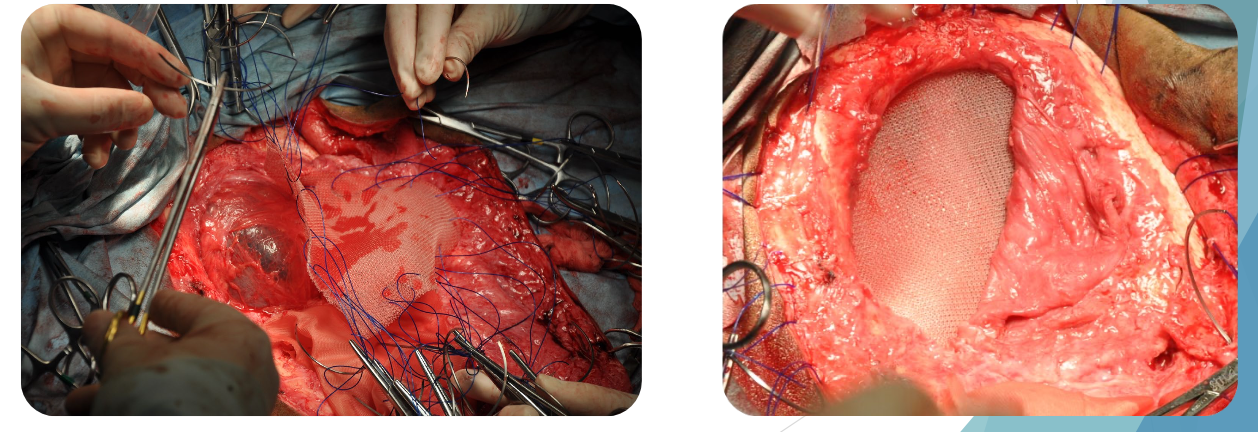
mesh for large defects
polyglactin 910 - Vicryl
Polypropylene - Prolene
differences from small animals
punching through skin - much thicker
practice!
tightness on skin sutures
snug!
more frquently use surgeon’s throws
PDS II NOT preferred for closing linea alba
RARELY use intradermal patterns