4. Anorexia Nervosa
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
40 Terms
What are the main symptoms associated with Anorexia Nervosa?
low body weight
restriction
What are the main symptoms associated with Bulimia Nervosa?
binge episodes
compensatory action: purging or restriction
What are the main symptoms associated with binge eating disorder?
binge episodes
no compensatory actions
What are the 3 key links between interoceptive bodily signals and eating disorders?
intuitive link through the gastrointestinal system
failure to detect hunger leading to restriction
failure to detect fullness leading to binge eating
What are the key links between interoception, emotions and eating disorders?
patients confuse body sensations with emotions
find it difficult differentiating between emotions and emotional regulation
Axlexithymia is quite prevalent with EDs, particularly Anorexia: not being able to match up body feelings and emotions.
What are three 3 behavioural patterns in Anorexia Nervosa?
extreme overvaluation of shape and weight
disturbed eating, resulting in clinically significant impairments in health and psychosocial function due to self-starvation
resistance to treatment, poor prognosis, high mortality
What are the DSM criteria for Anorexia Nervosa?
restriction of energy intake to be less than what the body needs - leading to significantly low body weight
intense fear of gaining weight
disturbance in the way in which one’s body weight or shape is experienced; inaccurate estimation of their own body size
reduced capacity to soothe oneself or empathise with others
emotionally inhibited (flattening of affect)
depression, negative self evaluation
alexithymia - inability to describe or recognise emotions
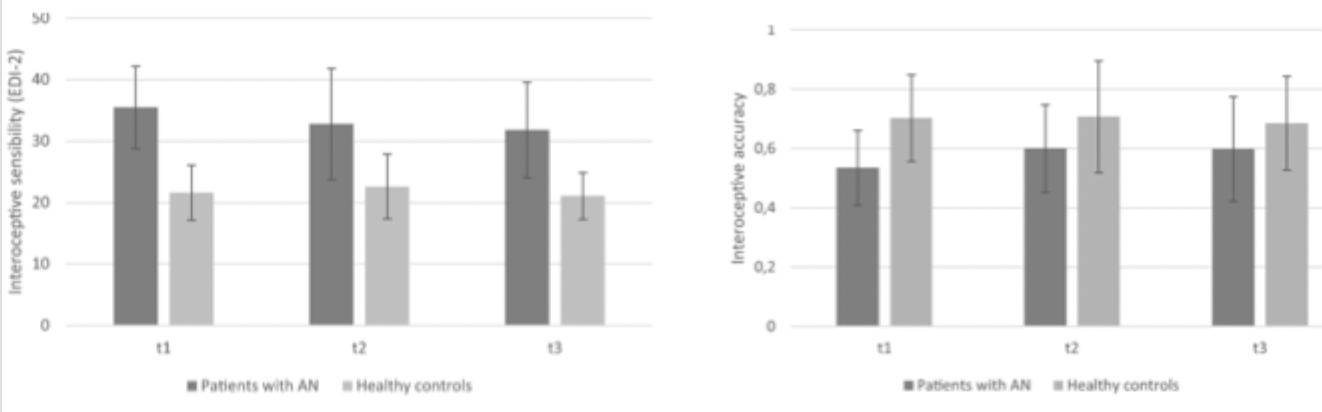
What does the Interoceptive Deficits subscale aim to identify with in the eating disorder inventory questionnaire?
a lack of confidence in recognising and accurately identifying emotions and sensations of hunger or satiety
confusion and mistrust related to affective and bodily functioning are characteristic of eating disorders

What does the research as a whole suggest about the different types of interoceptions and their role in Anorexia?
research does not dissociate between different types of interoception that may be impacted
interoceptive sensibility and interoceptive accuracy were not correlated in patients with AN
but instead → dysfunctional thoughts and feelings impacting the interpretation of visceral signals
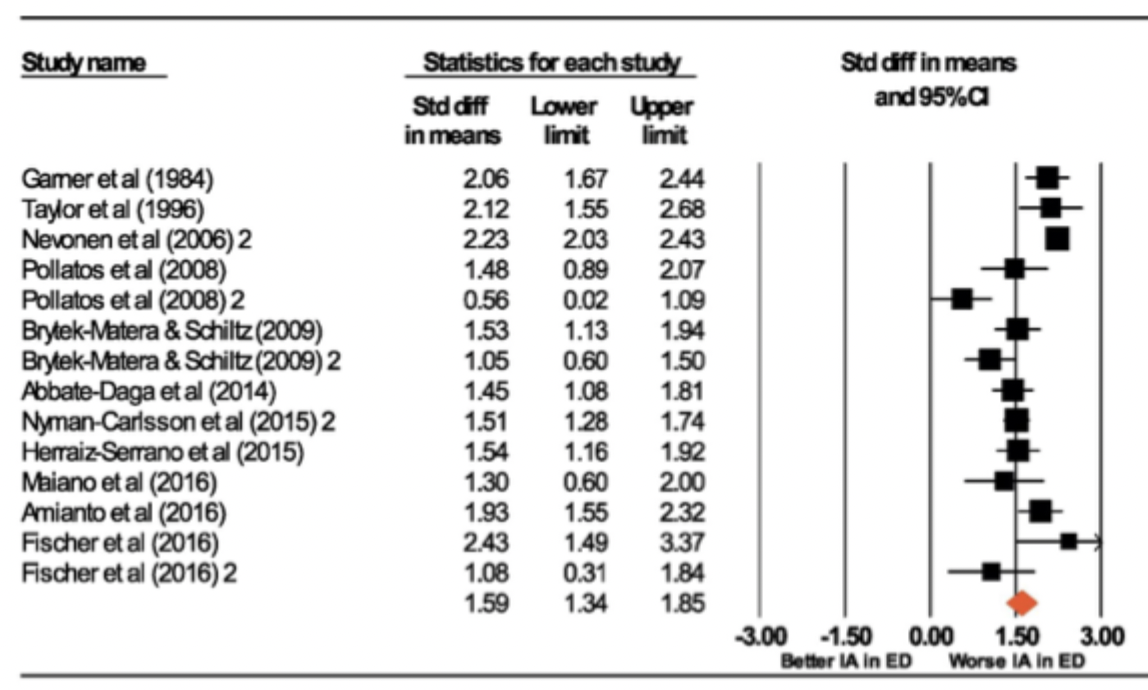
What did Jenkinson et al’s meta analysis across all EDs, using EDI interoceptive scale find regarding AN patients?
significantly lower scores
systematic overall effect → AN patients significantly different score lower on interoceptive scales compared to people who don’t have a diagnosis
What did Jenkinson et al’s meta analysis across all EDs, using EDI interoceptive scale find regarding patients with EDs other than AN?
Bulimia Nervosa had equivalent effects to AN
Binge earing disorder had a smaller effect size, but still significant and present
lower interoception in those with higher alexithymia
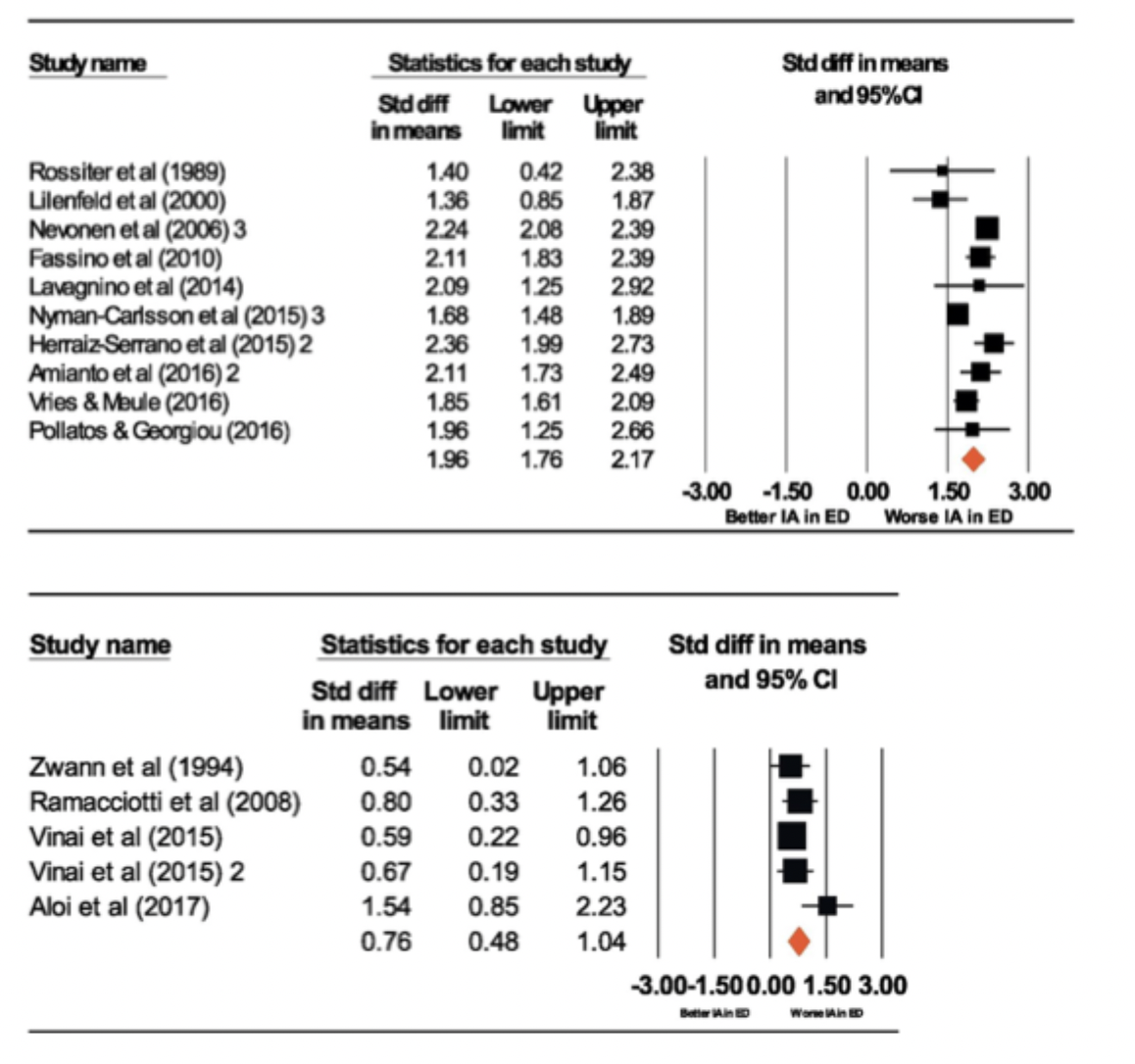
What might be the conclusions of Jenkinson et al’s meta analysis across all EDs, using EDI interoceptive scale?
interoceptive sensibility may be a transdiagnostic characteristic of EDs
it varies across diagnosis
may be a heritable risk factor and/or important for maintenance and development
interoceptive sensibility could be a target for therapeutic intervention
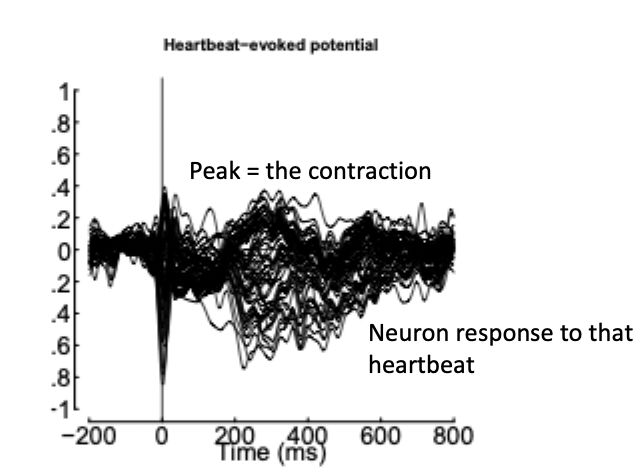
What did Pollatos et al (2008) find conducting an interoceptive accuracy task with AN patients?
heartbeat perception task was performed using four intervals of 25s, 35s, 45s and 100s
during all trials, ppts were asked to silently count their own heartbeats
patients with AN exhibit a generally reduced capacity to accurately perceive bodily signals
have less intense emotional experiences in many everyday situations
therefore indicating the potential importance of interoception in the pathogenesis of AN
In contrast to the findings of Pollatos et al what do eshkevari and Kinnaird show regarding interoceptive accuracy in AN patients?
findings are mixed using interoceptive accuracy task
Eshkevari et al (2014) → no difference between ED and controls (both at chance)
Kinnaird et al (2020) → no difference between AN and HC in accuracy but confidence was different (interoceptive awareness)
What did Lernia et al (2018) find in a case study of AN vs Healthy controls using:
heart beat counting task (interoceptive accuracy)
confidence measure (interoceptive awareness - when compared to accuracy score)
MAIA (interoceptive sensibility)
found a trend towards lower interoceptive accuracy but enhanced confidence of interoception (interoceptive awareness)
patient less able to regulate distress and distract from bodily signals → reduced body trust (interoceptive sensibility)
patients demonstrated detachment between the ability to perceive the body and the awareness → object reality and experience of the body become detached
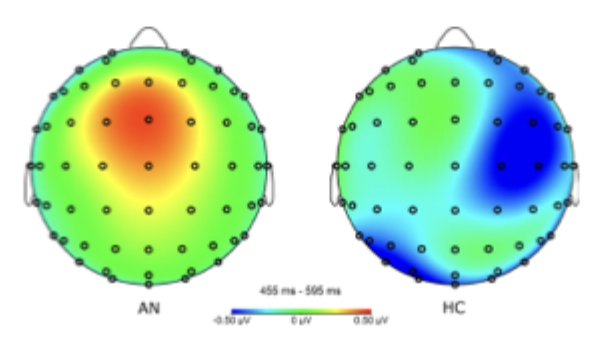
What did Lutz et al (2019) find comparing using a heartbeat counting task during EEG-HEP, comparing AN and HC?
no significant difference in interoceptive accuracy
but significant differences in interoceptive neural processing
disturbance of interoceptive signal processing found at the level of cortical representation → difference in the way the brain is processing the heartbeats in AN patients
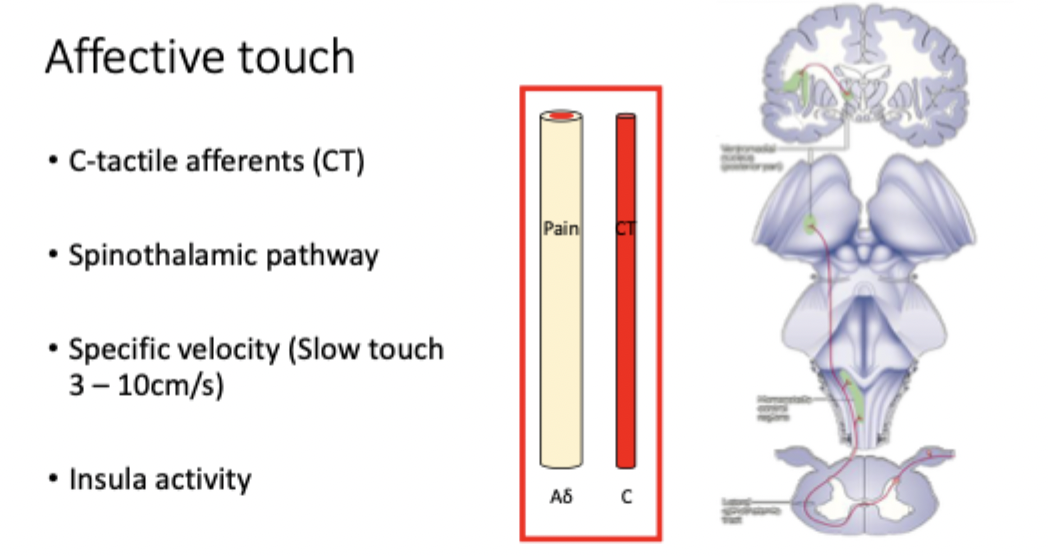
Affective touch definition
touch specifically associated with pleasantness sensations
informs about physiological body state
some evidence that affective touch can modulate pain (similar mechanism to scratch and itch)
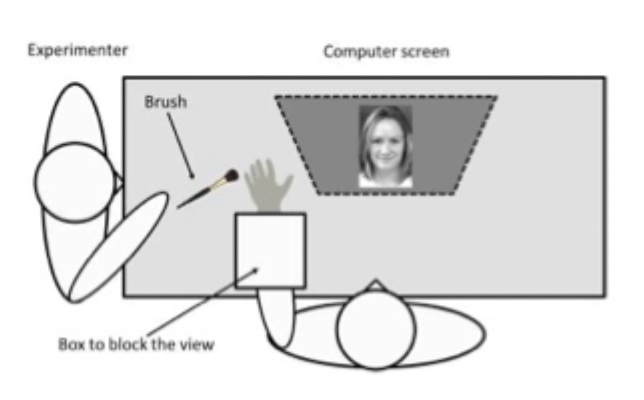
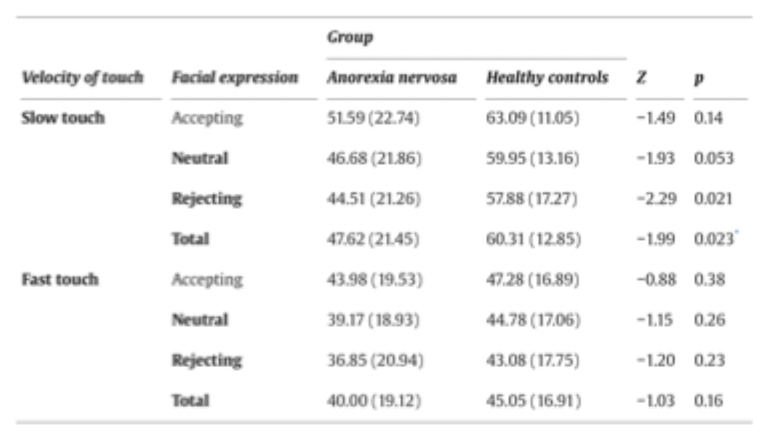
What did Crucianelli et al (2016) find when AN patients were given affective and neutral touch when looking at images of faces with different facial expressions?
smiling, rejecting and neutral
measured judgements of pleasantness and anhedonia
pleasantness of affective touch was lower in AN
moderated by social context in both groups
difference more likely to be bottom-up than top-down → the CT pathway

What did Murialdo et al (2007) find investigating regulatory control of heart rate variability in EDs using the tilt table test?
lie on a table that adjusts your body position from horizontal to vertical to simulate standing up
monitored changes in heart rate and blood pressure
patients had lower blood pressure
sympathetic cardiac activity did not increase in patients after lying to standing as occurs in healthy control
cardiac abnormalities similar in AN and bulemia even though only AN are emaciated (not linked to BMI)
illustrates more widespread difficulties → exhibit differences in both heart rate detection/interpretation and regulation, consistent with insular cortex involvement
What did Fischer et al (2016) find conducting CBT with 15 AN patients - paying special attention to maladaptive emotional processes?
aim of the intervention is a normalisation of the eating behaviour and to reach an adequate body weight - but also targeting aetiology
tested at the beginning, after 4-6 weeks, and at the end of therapy
found significant improvements of BMI and depression
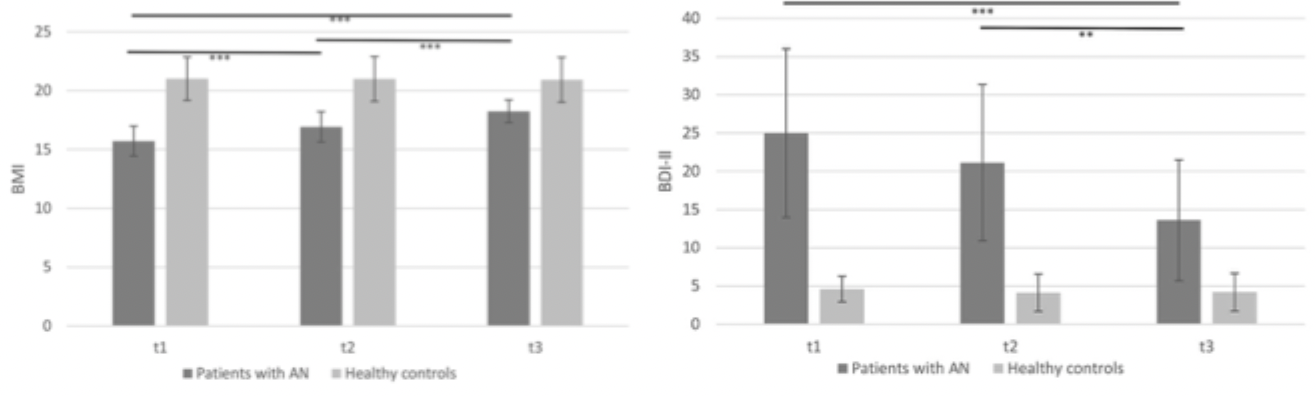
interoceptive accuracy and sensibility - any recovery was small and inconsistent
What do the results of Fischer et al CBT study in which depressive symptoms of AN patients improves but interoceptive accuracy and sensibility did not lead us to conclude?
interoception processed differently in AN
does not improve with other symptomology (weight and depression)
a potential mechanism for development, maintenance and relapse of AN
Most interoceptive differences seem focused on the gastric system → are heartbeat monitoring tasks indicative of all interoception? Should other tasks be used in relation to AN?
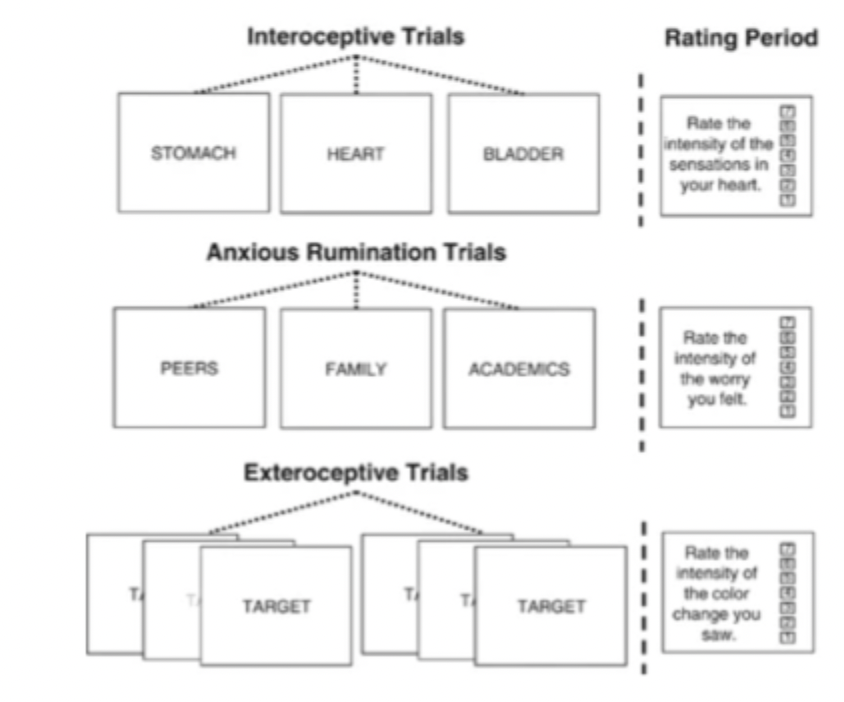
What did Kerr et al (2016) find in weight restored (recovered) AN patients who completed an interoceptive attention task which focused on sensations in their heart, stomach and bladder. Followed by anxious rumination phase and exteroceptive trial?
activity in the dorsal mid-insula was reduced in AN patients during stomach interoception
activity in the anterior insula was relatively higher in AN patients during heart interoception.
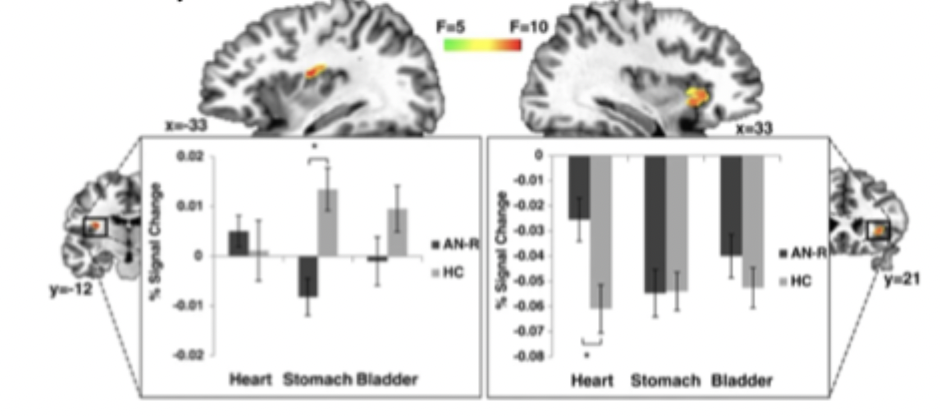
AN displayed increase activation during anxious rumination in the dorsal mid-insula
activity in this region during stomach interoception also correlated with measures of anxiety and psychopathology
different functional activity in the dorsal mid-insula during gastric interoception → contributes to the symptomatology of AN - includes anxiety
What occured in Kerr et al (2016) study when patients were asked to change their attention to stomach?
little signal change/ facilitation effect
we can infer that there was higher activity at baseline
hypervigilance → attending all the time, so don’t see effect when shifting to it
What is involved in the vicious cycle with stomach interoception which might exacerbate gastrointestinal symptoms during weight restoration and inhibit recovery?
gastric discomfort leading to increased anxiety that then leads to greater gastric discomfort
How might interoceptive processing in gastric and cardiac domains influence AN symptomology?
many AN patients difficulty detecting hunger and satiety
hypervigilance of gastric symptoms may lead to anxiety over eating and distorted exteroceptive bodily experience (feeling fat)
reduced ability to detect heart beats → flattening of affect
How might the somatic error hypothesis and other prediction theories relate to AN?
these theories suggest inaccurate interoceptive predictions in psychiatric disorders
difference in gastric processing may not be sensory input but interpretation
unclear mechanisms for how interoception underlies a complex disorder such as AN
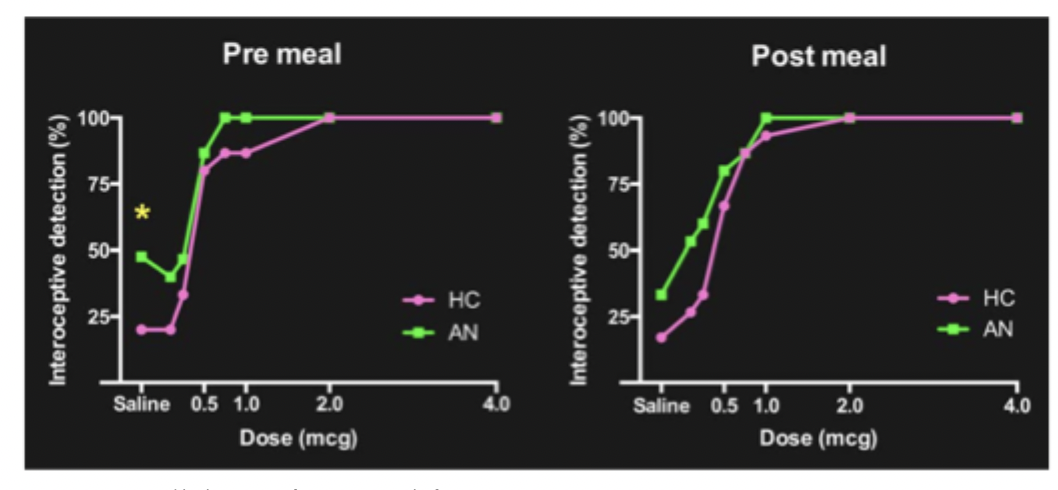
What did Khalsa et al (2015) find regarding interoception and eating?
ppts given drug to make heart rate increase or saline
measured pre and post meal intensity of heartrate and breathing
interoceptive detection thresholds and interoceptive accuracy
patient group reported higher rates of interoception before eating
AN experienced more intense cardiorespiratory sensations before consuming a meal
AN more likely to report interoceptive experiences in all conditions, particularly in low arousal conditions
AN could be anticipating general increases in interoception during a meal
anticipating food intake (and/or gastric discomfort) could lead to anxiety
How is interoception not an all or nothing measure?
dependent on modality and environment
the insular cortex integrates information across modalities with visceral/interoceptive sensation
supports a prediction error rather than a general issue
What prevents intuitive eating in AN?
inaccurate mapping of interoceptive signals in AN results in prediction errors about the internal bodily state
intuitive link between difficulty perceiving hunger and satiety and dysfunctional eating habits
How might interoception underlie restrictive symptoms of AN?
impaired interoceptive experiences means that AN patients cannot use internal signals to perceive physical changes of weight loss
also do not recognise satiety or hunger
AN patients continue to restrict food intake despite emaciation
How might interoception underlie the emotional symptoms of AN?
AN is associated with high rates of alexitheymia
AN linked to decreased ability to self-regulate emotions - regaining homeostasis - autonomic control of the insula
inaccurate perception and interpretation of interoceptive signals → intense fear of gaining weight
What factors might influence AN patient’s disturbance in the way in which one’s body weight or shape is experienced?
overevaluation of weight and shape
self-objectification
inaccurate (overestimation) experience of body size
What is the definition of body image?
How you experience and feel about your body
mental representation of body in brain
What is involved in Objectification Theory?
bodies are viewed and evaluated based on appearance
the body as an object (sexual)
the body and sexuality are separate from the person
objectifying others and objectifying the self → the more you self objectify, the more important body appearance and deviations from social ideas is important for self worth
How does the allocation of attention influence interoception and lead to self-objectification?
competition of cues hypothesis suggests their are finite attentional resources available
emphasis on body appearance detracts from internal signals and vice versa
less attention paid to ‘unreliable’ bodily signals - down regulated
poor interoception in AN → self objectification, only way to learn about body is through vision
How does interoception underlie body image and lead to disturbance in the way in which one’s body weight or shape is experienced?
failure to update external perception of the body through direct sensory input - don’t realise they have lost weight and continue to feel dissatisfied with their body
an over-reliance on exteroception (vision) leads to enhanced self objectification and symptoms such as body checking
Insular cortex is a neural hub connecting interoceptive signals with other modalities including exteroception, cognition and emotions
potential mechanism in AN of interoception underpinning many of the key symptomology in AN
What might the failure to address it in treatments lead to?
a high chance of relapse
Interocepetive prediction errors may lead to further errors and negative affect that if unresolved may lead to…
risk of relapse particularly with certain triggers
both exteroceptive and interoceptive bodily symptoms continue following weight restoration
Weight restored AN patients show differences in insula activity when…
anticipating food
decreased response to the taste of food stimuli
What is the current state of AN treatment and what might guide future inventions for treatment?
interoception abnormalities seems resistant to current treatments
plasticity of the insula suggests such issues can be targets for treatment
potential interoceptive treatments need to be tested e.g. interoceptive exposure to increase tolerance to the physical symptoms of anxiety through repeated provocation triggers, and mindfulness