Positioning Notes: L-Spine
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
Routine Views for L-spine pediatrics- less than 8
AP & Lateral
AP L-spine technique
90 kVp, 10 mAs
AP L-spine centering
Center @ iliac crest (L4) & down MSP
AP L-spine breathing
Suspended expiration
AP L-spine evaluation criteria
area from T12 to superior sacrum should be included
intervertebral joints open
no rotation
sacroiliac joints should be equidistant from vertebral column
symmetric vertebrae, with the spinous processes centered to the bodies
AP L-spine merrill’s SID recommendation
48” (to reduce distortion & open intervertebral disk spaces more)
AP L-spine merrill’s collimation recommendation
8×14 or 8×17
AP L-spine merrill’s recommendation
recommend PA position
this would place intervertebral disk spaces at an angle more closely parallel to the divergence of the beam
patient dose is also reduced due to decrease abdominal thickness when prone
RPO/LPO L-spine technique
90 kVp, 18 mAs
RPO/LPO L-spine centering
Center @ L3 (1-1.5” above iliac crest), entering about 2” medial to ASIS
RPO/LPO L-spine - purpose
articular processes & z-joints of side closest to IR are seen
RPO/LPO L-spine- breathing
suspended expiration
RPO/LPO L-spine- evaluation criteria
T12- sacrum included, down to SI joint
z-joints closest to IR seen
vertebral column parallel w/ tabletop so that the T12-L1 & L1-L2 joint spaces remain open
RPO/LPO L-spine- OVER ROTATION
Z-joint is not well visualized & pedicle is POSTERIOR on vertebral body (Pedicles are oval/smushed)
RPO/LPO L-spine UNDER ROTATION
Z-joint not well visualized & pedicle is ANTERIOR on vertebral body
RPO/LPO L-spine- Merrills obliquity
60 degrees (to show L5-S1 z-joints)
Lateral L-spine technique
96 kVp @28 mAs
Lateral l-spine centering
@ level of L2/L3
Lateral L-spine breathing
suspended expiration
Lateral L-spine evaluation criteria
T12- L5/S1
open intervertebral disk spaces & foramina of L1-L4
no rotation
posterior margins of each vertebral body should be superimposed
the crests of the ilium should nearly superimpose each other
vertebrae should be aligned down the middle
spinous processes in profile
Lateral L Spine rotation
If one crest is bigger it is more AWAY from the IR (magnified)
Lateral L-spine: merrills SID recommendation
48” (to reduce magnification of the spine)
Lateral L-spine: Merrills recommendation if the long axis of the vertebral column is not horizontal
elevate the lower thoracic region w/ a radiolucent support (preferred method)
if not using a support,
angle tube 8 degree caudad for females
5 degree caudad for males
RH- when a patient arrives for AP & Lateral (only) L-spine imaging, obtain___
all l-spine vertebrae on lateral image (there is no need for an L5-S1 conedown image)
Lateral L5/S1 L-spine technique
96 kVp, @ 45 mAs
Lateral L5/S1 L-spine
10×12 LW collimation
Caudal angle 2” posterior to elevated ASIS & 1.5” inferior to iliac crest
females= 8 degree caudad
males= 5 degree caudad
left marker anterior
Lateral L5/S1 L-spine breathing
suspended expiration
Lateral L5/S1 L-spine Evaluation criteria
lumbosacral joint should be clearly seen & open
all of the 5th lumbar vertebra should be included as well as the upper portion of the sacrum
lumbosacral joint centered
no rotation (crests of ilia are nearly superimposing each other)
A larger waist on Lateral L5/S1 L-spine may require a slight__
cephalic tube angle
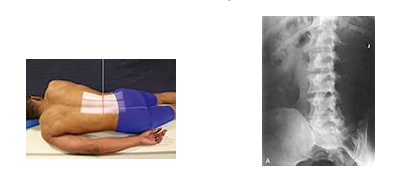
Special Views: L-spine- Anterior Oblique (RAO/LAO)- purpose
articular processes & z-joints of side furthest from IR (scotty dog seen)
Special Views: L-spine- Anterior Oblique (RAO/LAO)- patient position
prone, turn away from side of interest 45 degrees
An oblique position of 60 degrees from the plane of the IR may be needed to show L5/S1 Zygapophyseal joints
Adjust body so long axis of patient is parallel to table.
In this position the lumbar spine lies in the longitudinal plane that passes 2” lateral to the spinous processes.
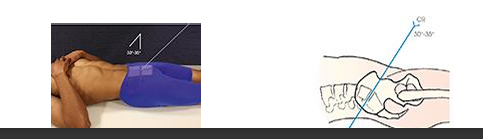
Special Views: L-spine: L5/S1 AP axial (ferguson method) purpose
lumbosacral joint & a symmetric image of both sacroiliac joints free of superimposition
(30 degree cephalad for males, 35 degrees for females)
Special Views: Lumbar Spine: AP right & left bending (spinal fusion)- purpose
Used to evaluate the integrity of a spinal fusion. Also used for early scoliosis to determine presence of structural change when bending to right and left. May be used to localize a herniated disk as shown by limitation of motion at the site of the lesion.
when are AP right & left bending (spinal fusions) performed after fusion procedure?
6 months
Special Views: Lumbar Spine: LATERAL FLEXION & EXTENSION (spinal fusion) purpose
Used to determine whether motion is present in the area of a spinal fusion, indicating nonunion, or to localize a herniated disk as shown by limitation of motion at the site of the lesion.
what special view of the L-spine is this?
Anterior obliques (RAO/LAO)
what special view of the L-spine is this?
L5/S1 AP axial (ferguson)

what special view of the L-spine is this?
AP right & left bending (spinal fusion)