Biomechanical Analysis Midterm
1/157
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
158 Terms
what are the phases of gait in order?
Closed chain: muscles are working to stabalize
Initial contact
Loading response
Mid stance
Terminal stance
Open chain: muscles are working to swing the leg forward
Pre Swing
Initial Swing
Mid Swing
Terminal Swing
what is the initial contact phase of gait?
the instant the foot contacts the ground
what is the loading response phase of gait?
begins with foot contact and ends with contralateral limb toe off
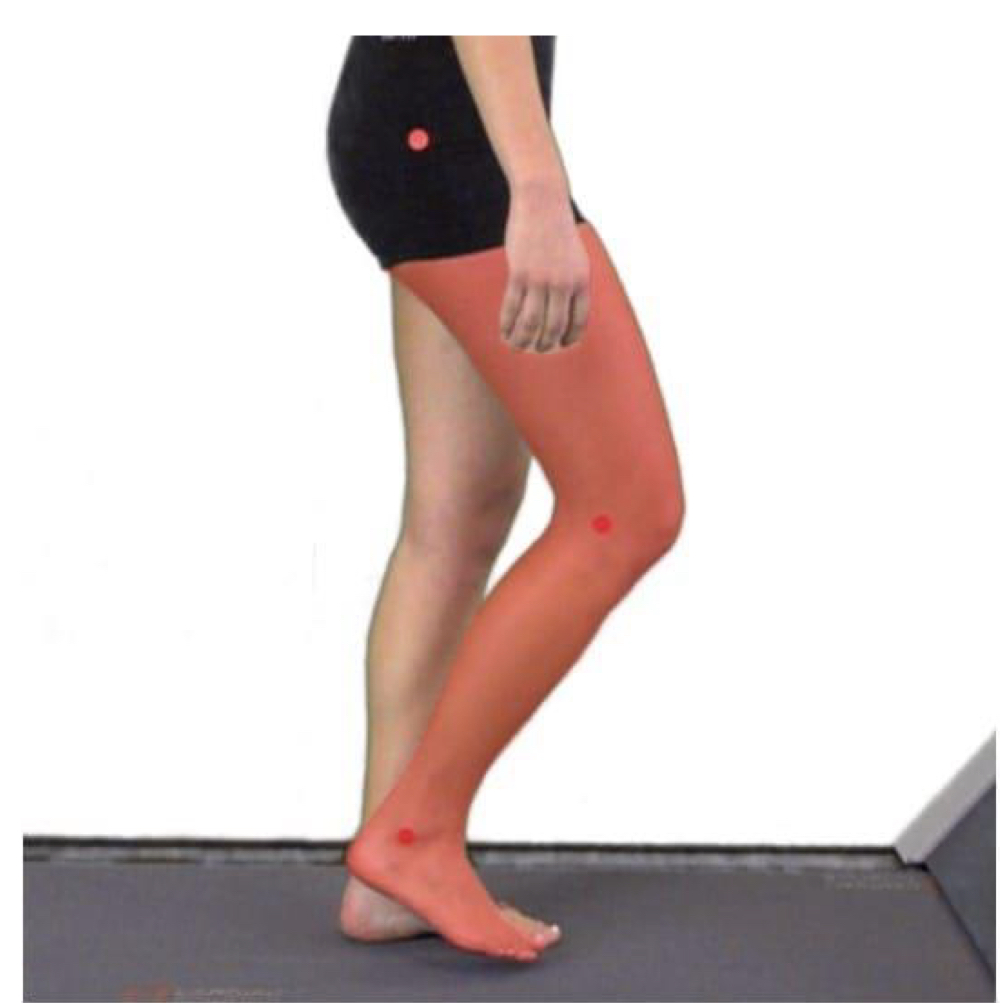
what is the mid stance phase of gait?
begins with contralateral limb toe off and ends with ipsilateral heel rise

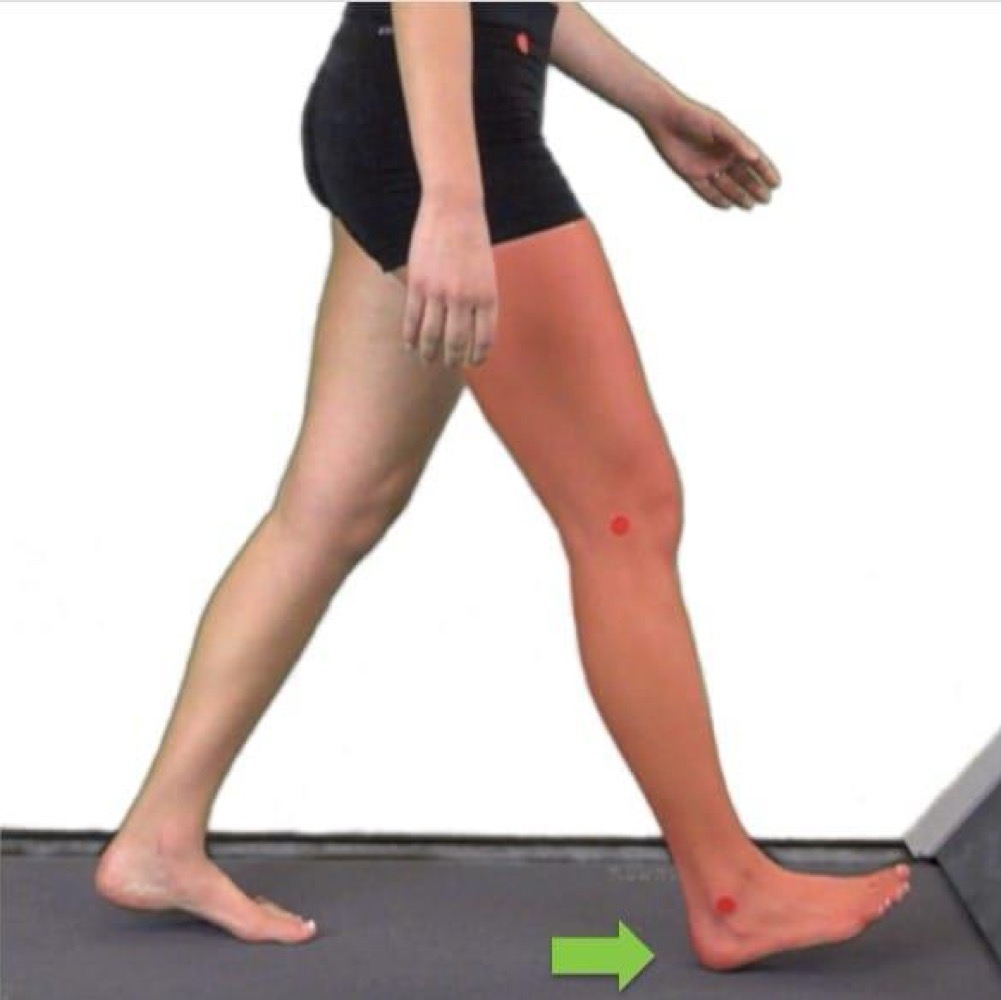
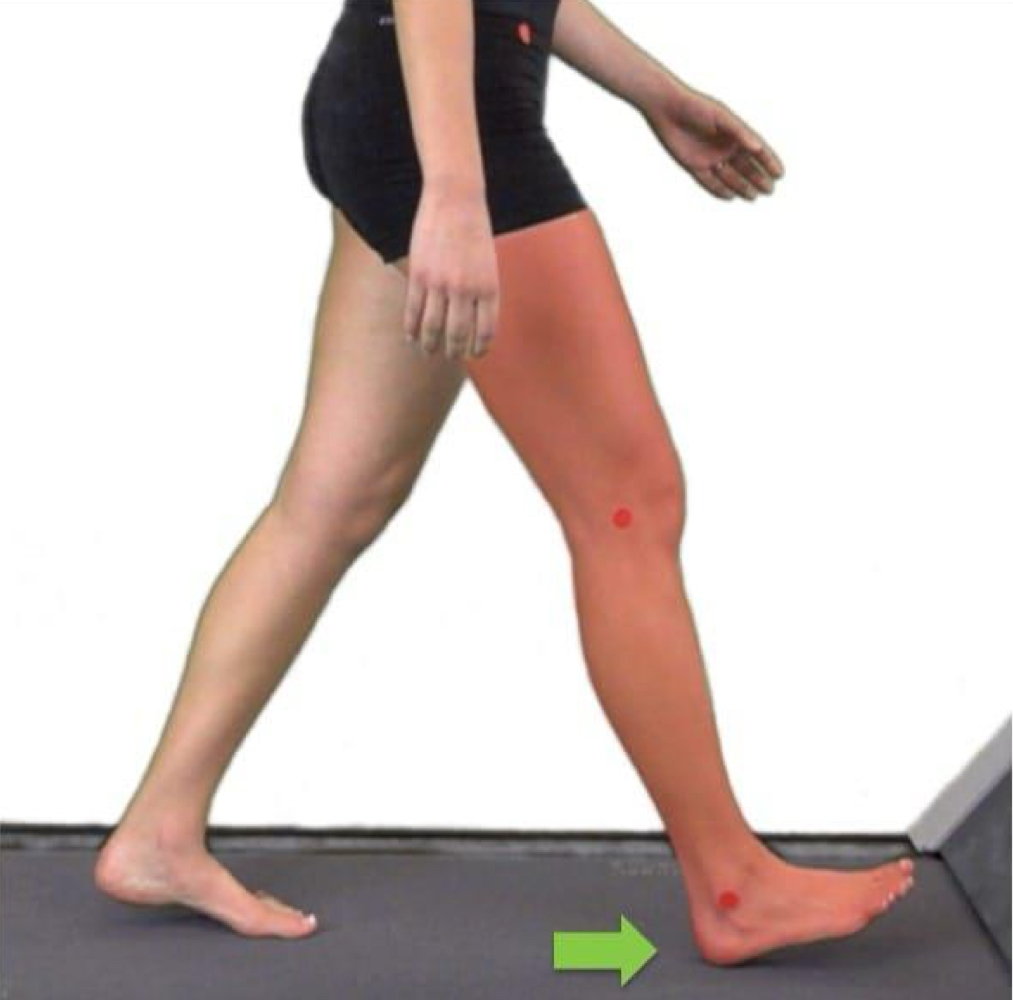
what is the terminal stance phase of gait?
begins with ipsilateral heel rise and ends with contralateral limb foot contact

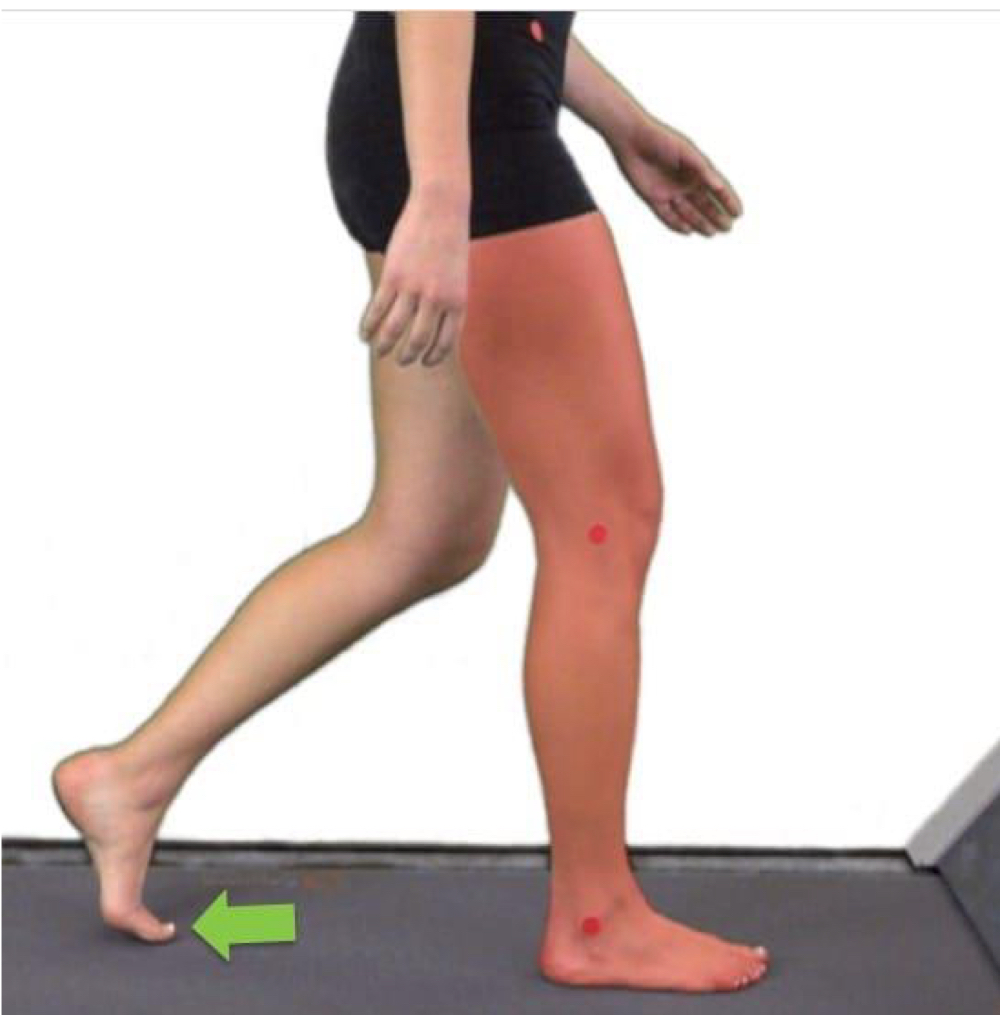
what is the pre swing phase of gait?
begins with contralateral limb foot contact and ends with ipsilateral toe off

what is the initial swing phase of gait?
begins with ipsilateral toe off and ends when the medial malleoli are aligned
what is the mid swing phase of gait?
begins when the medial malleoli are aligned and ends when the ipsilateral tibia is perpendicular to the ground

what is the terminal swing phase of gait?
begins when the ipsilateral tibia is perpendicular to the ground and ends when the ipsilateral foot strikes the ground
what is the cyclical process of observational gait analysis?
Identify deviations
Develop hypotheses for probable causes that are informed by the patient (ICF)
Plan and perform the examination
Examination findings plus patient and family context informs treatment
Reevaluate—measure effectiveness of treatment
how can we identify deviations when observing gait?
watch the individual in both the sagittal and frontal planes to have a more complete picture of the patient. movement in the transverse plane is inferred based on what you see in other planes
use technology to help support what you observe and provide data that can’t be seen
what are primary deviations?
a deviation due to an impairment local to the area in question
ex: decreased DF during the swing phase due to stiff plantar flexors
what are secondary deviations?
due to an impairment that is at adjacent joint or further away
ex: excessive hip flexion during the swing phase to compensate for lack of DF
how can we develop a hypothesis using primary and secondary deviations?
we would want to assess/examine the areas where we see deviations. for ex, if we see decreased DF during the swing phase, we would assess the ankle and hip. if the hip has no impairments then we can assume it is a primary deviation like stiff plantar flexors.
how do we plan our examination of gait?
we have our examination priorities made up of red flags and SINNS, identifying deviations, and patient context
what are our objective and subjective gait measurements we can use to reevaluate gait?
subjective: observations— keep in mind there is bias in this
objective:
walking speed
10 meter walk test (10MWT)
timed up and go test (TUG)
6 minute walk test (6MWT)
functional gait assessment (FGA)
what are the components that make up walking speed?
walking speed/velocity is the distance travelled during a specific period of time (m/sec or m/min). the components that make it up are…
cadence: the number of steps taken during a specific time period (steps/min)
stride length: the linear distance between 2 successive events on the same limb. so basically the distance between initial contact on the R limb until initial contact again on the R
the larger the stride length, the faster the gait speed
how do we calculate walking speed?
velocity= distance/time
cadence= steps/time
stride length= walking speed/ ½ cadence
what are the noermative values for the 10 meter walk test in individuals ages 20-59?
velocity: W 1.32 m/sec (79.3 m/min); M 1.36 m/sec (82.1 m/min)
cadence: W 121 steps/min; M 111 steps/min
stride length: W 1.32 m; M 1.48 m
what are the components of the 10 meter walk test?
instruct patient to walk at their normal walking speed begining at a point 2 meters before the intended start time
record the length of time it takes for the lead foot to cross the start line and finish line
repeat for a total of 3 times and average them up
what are the components of the timed up and go test?
patient is given one chance
patient may use any assistive device they normally use
on the word go patient stands up and walks 3 meters, turns around the cone, and walks back to the chair and sits back down
timer stops when the patients back is resting against the back of the chair
what are the components of the 6 minute walk test?
test should be done in an enclosed 30 meter walkway
give encouragment in standardized intervals like 30 sec or two minutes and record to maintain retest quality
participant should be told to walk at a comfortable pace
in patient with pulmonary or cardiac dysfunction, vital signs should be monitored at regular intervals to seem how the body responds
if they cannot walk 6 minutes, use the distance they ended at. they can also take breaks but the timer does not stop.
what is instrumented gait analysis?
the objective, quantitative measurement of human walking using specialized technology
what are the differences between instrumental gait analysis (IGA) and observational gait analysis (OGA)?
IGA
quanitative
objective
reliant on technology
high cost
takes time to set up
only in research or specialty clinics
IGA
qualitative
subjective
may use technology to support such as filming someone
low cost
can be done quickly
can be used in almost any clinic setting
what 3 categories of data collected make up instramental gait analysis?
temporal spatial, kinetics, kinematics
stance accounts for how much of the gait cycle?
just over half
swing accounts for how much of the gait cycle?
swing
the majority of the gait cycle is spend in what?
single leg support
what spatial characteristics can IGA tell us?
stride and step length
step width— wider in someone with impaired balance which leads to more frontal plane side to side movement
foot progression angle— when heel strikes the ground, do toes go out to the side, the middle, or stay with the angle of the heel
what are the main kinematic movements we could see using IGA?
translational movements (linear displacement)— COM
rotationanl movements (angular displacement)— joint angles
why is limiting COM displacement important?
more vertical and lateral displacement leads to less efficiencly, taking away the energy needed to move forward
discuss vertical displacement
normal is around 5cm
highest during mid-stance
lowest during loading response and pre-swing
discuss lateral displacement
normal lateral displacement is around 3.5cm
maximum excursion during mid-stance
what are the types of rockers during gait?
heel rocker: occurs during initial contact through loading response
ankle rocker: occurs during stance phase when the body pivots over the talocrural joint
forefoot rocker: occurs during terminal stance when the body pivots over the MTP joints
toe rocker: fulcrum off great toe MTP joint
what are ground reaction forces?
the effect forces from the ground have on our body. they can predict an external moment which are the effect of the GRFs on our joint
what are external moments?
calculated based on the position of the joints in space relative to the forces of ground reaction forces and acceleration of hte body limbs
if our muscles did nothing, this is where our body would want to go
what are therapists habits of mind?
ways of knowing—how we learn, think, and reason
what are therapists habits of hand?
ways of doing— what skills we do, how we improve them and utilize them. how we carry ourselves, biomechanics, assessments and intervention techniques
what are therapists habits of heart?
ways of being— our theraeutic alliance. how we present ourselves to the patient and others. how we interact, communicatae and build theraputic alliance with the patient.
what is clinical reasoning?
a process of reflective inquiry in collaboration with a patient which seeks to promote a deep and contextually relevant understanding of the clinical problem, in order to provide a sound basis for clinical intervention
what is the clinical reasoning universe?
patients are always at the center. every decision we makes should include them
therapist: we don’t have to ignore us but we have to be able to self regulate and be self aware of our strengths and weaknesses
context
what is bayesian reasoning?
it apples probability theory to deductive and inductive reasoning
one reasons through data/observations to create raise of lower the probability of things that are true
it allows for multiple hypothesis to be considered and helps us to rank or prioritize them
what is type 1 processing?
it is an automatic, subconscious way of thinking through things. it allows us to recognize and instantly react without having to go through steps
pros are that it is faster, and more efficient and therefore less cognitively demanding
cons are that it relies heavily on pattern recognition but when something doesn’t fit a pattern, it can be easy to miss or overlook possibly important things.
it is often our default setting with more cognitive load/stress
what is type 2 processing?
it is a systematic, conscious way of thinking through things. relies more on steps and analysis
it should be used more often however, it is less efficient and increases cognitive load
what does expert clinical reasoning look like?
use type 1 processing
can recognize need for type 2 processing
reasoning is individualized to the patient and includes the contextual element related to the patient clinician interaction
rational: using logic and will get to an answer that you get to
reflection IN action: reflecting in the moment and able to pivot and make correction in real time
what does novice clinical reasoning look like?
rely on type 2 processing
default to type 1 processing when under cognitive load, this increases probability of clinical reasoning errors
do not recognize that clinical reasoning is a collaborative process between the clinician and the patient
rationalize: have an answer in mind and come up with resions to get to that answer
reflection ON action: reflecting back on past experience
what are clinical reasoning erros?
inadequate knowledge: you are only able to reason through what you know so you should fill knowledge deficits
faulty data gathering: poor or incomplete performance of assessments in both our physical examination skills and communication and questioning skills will lead to less important information gathered
faulty data processing: inappropriate application of knowledge or use of cognitive biases and faulty reasoning can lead to incomplete or innacurate conclusions
faulty metacognition: this is the most important aspect and yet when we don’t do it well, it leads to the inability to recognize logical fallacies and cognitive biases
what are the logical fallacies?
appeal to authority, bandwagon, red herring
what is appeal to authority and an example?
when an individual will state or trust something is true becuase someone in power has said it is true
ex: treating the patient based on their referred diagnosis vs performing your own evaluation
what is bandwagon fallacy and what is an example?
doing something because everone else is doing it that way
ex: at the clinic your at, no one performs observational gait analysis. as a new member of the this clinical practice you dont either because no one else does
what is red herring fallacy and an example?
information that misleads the clinician or distracts them from what is important. putting a lot of emphasis on something that actually isn’t relevant
ex: assuming a meniscal tear is the cause of someones gait impairments even though this is a common finding in the older asymptomatic healthy opulation and may not acutally play a part in their gait impairment
what are the cognitive biases?
confirmation bias, anchoring bias, recall bias, recency bias, outcome bias
what is confirmation bias and an example?
when a clinician only uses or seeks evidence that supports their point of view and disregards or avoid evidence that does not support it.
ex: shaping your examination to help support a diagnosis you really like while ignoring other potential sources of symptoms or contributing factors
what is anchoring bias and an example?
when a clinician is overly influenced by the first evidence they collect and the hypothesis it generates.
ex: you are examining a pt with LBP and the first thing you observe is limited trunk rotation during gait. therefore, you hypothesize the cause of their LBP is a lack of trunk rotation despite other data that conflicts with this later in the exam
what is recall bias and an example?
the tendency of a clinician to remember their favorable results and not remember the less than spectacular outcomes. this causes you to overestimate the effectiveness of an intervention.
ex: when performing an intervention, we tend to focus ont he patients that this intervention has helped opposed to all those it was not helpful for
what is recency bias and an example?
the tendency to place too much emphasis on experiences that are freshest in your memory even if they are not the most relevant or reliable.
ex: after attending a dry needling course, you begins to reason that all of your patients need dry needling in the coming weeks
what is outcome bias?
believing that a patients positive outcome is directly related to the intervention that you performed. in reality, patients will naturally get better over the course of time if they are healthy in spite of what we do.
ex: My patient met all of their therapy goals and is pain free after 6 weeks of therapy twice a week after an acute ankle sprain. During their treatment I performed ultrasound at every visit. Therefore 6 weeks of ultrasound is helpful for ankle sprains and I should do this with every new ankle sprain I treat.
what are the two phases that occur during closed chain gait?
weight acceptance: absorving force and using those forces to move forward
single leg support: balancing on one limb while keeping momentum moving forward
what is the phase that occurs during open chain gait?
swing limb advancement
what are the phases that are part of weight acceptance?
initial contact and loading response
what are the key events of weight acceptance
heel strike
heel rocker
shock absorption
stable base for weight acceptance
what is the importance of heel strike during weight acceptance?
it sets the stage for everything else to happen
required for initiation of heel rocker
it is the initial contact to the ground
what is the importance of heel rocker during weight acceptance?
allows for the advancement of the forefoot and tibia
minimizes vertical center of mass displacement— this reduces unnecessary energy use so more energy can be used to move forward
what is the importance of shock absorption during weight acceptance?
controlled plantar flexion and knee extension help decelerate body weigh and keep the body moving forward
minimizes vertical center of mass displacement
what is the importance of a stable base for weight acceptance during weight acceptance?
our legs need to be 100% ready to accept weight
is vital for weight shift from one foot to the other
minimizes lateral center of mass displacement
what are the problems we could see with heel strike during weight acceptance?
with no heel strike…
we will land on our forefoot or a flat foot which shifts ground reaction forces anterior to the ankle. this increases load on the PFs and changes GRF and external moments up the kinetic chain
it does not allow for the initiation of a heel rocker
what are the problems we could see with heel strike and shock absorption during weight acceptance?
excessive deceleration leads to loss of forward momentum. this increases compressive forces on joint surfaces and the mensicus in the kinetic chain, increases load on passive stabalizers of the sagittal pland, and puts increased demand on muscles in the kinetic chain in order to push you forward
increase in vertical COM displacement increases demands of muscles in the kinetic chain and causes excessive extension at the hip and knee
increase in lateral COM displacement as a compensatory method to move forward. this increases load on passive stabalizers of the frontal plane (MCL or LCL), increases shear forces on joint surfaces and menisci in the kinetic chain, and puts increased demands on muscles in the kinetic chain
what are problems we could see with a stable base for weight accpetance during weight acceptance?
inadequate deceleration causing excessive forward momentum. this increases load on passive stabalizers of the sagittal plane and puts increased demand on muscles in the kinetic chain
increase in vertical COM displacement, usually falling closer to the ground. this puts increased demand on muscles in the kinetic chain as well as excessive flexion at the hip and knee in the sagittal plane
increase in lateral COM displacement increases load on passive stabalizers of the frontal plane, increases shear forces on joint surfaces and the menisci in the kinetic chain, and puts increased demand on muscles in the kinetic chain.
what allows for us to have efficient gait?
our trunk and pelvis, hip, knee, and foot and ankle need to all work together in every moment. if something is not working well, there is a lack of efficiency.
the main theme of not being efficient is moving either too much or not enough
what are the kinematics of an efficient trunk and pelvis during weight acceptance?
minimal displacement in the sagital and front planes
sublte movement within the transverse plane
what are the kinetics of an efficient trunk and pelvis during weight acceptance?
deep postural muscle activity in order to provide stabalization and fine correction
isometric contraction of the contralateral QL and ipsilateral glute med to keep the pelvis and trunk together and upright
what does an inefficient trunk and pelvis look like during weight acceptance?
sagittal plane: excessive trunk extension or flexion and excessive anterior or posterior pelvic tilt
front: excessive lateral flexion or contarlateral pelvic drop (trendelenburg)
transverse: excessive or limited trunk or pelvis rotation (runway walk)
what are the kinematics of an efficient hip during weight acceptance?
25 degress of flexion
minimal adduction
minimal IR
what are the kinetics of an efficient hip during weight acceptance?
isometric contraction of hip extensors
eccentric to isometric contraction of hip abductors
eccentric to isometric contraction of hip ERs— eccentrics allows for little give to absorb shock and then isometrics provides stability
what does an inefficient hip look like during weight acceptance?
sagittal: excessive or limited hip extension or flexion
frontal: excessive or limited hip adduction
transverse: excessive or limited hip IR or ER
what are the kinematics of an efficient knee during weight acceptance?
0-5 degrees of knee flextion at initial contact
15 degrees of knee flextion at loading response
slight tibial IR to allow for “unlocking” of the screw home mechanicsm
what are the kinetics of an efficient knee during weight acceptance?
eccentric contraction of knee extensors
concentric contraction of popliteus
what does an inefficient knee look like in weight acceptance?
sagittal: excessive or limited knee extension or flexion
frontal: excessive knee valgus or varus moment
transverse: excessive or limited tibial IR or ER
what are the kinematics of an efficient foot and ankle during weight acceptance?
0 degress at initial contact to 5 degrees of PF at loading response
0 to 15 degrees of toe extension
supinated foot at initial contact to slight pronation at loading response
what are the kinetics of an efficient foot and ankle during weight acceptance?
eccentric contraction of DFs
eccentric contraction of toe extensors
eccentric contraction of arch support muscles to prevent it from falling
what does an inefficient foot and ankle look like during weight acceptance?
sagital: excessive or limited ankle DF or PF. excessive or limited toe extension or flexion
frontal/transverse: excesive or limited supination (more rigid foot so decreased shock absoprtion) or pronation (less rigid foot so less stable base)
what is forefoot contact ?
initial contact is made with the forefoot, usually due to excessive PF
what is flatfoot contact?
initial contact is made with the entire foot, usually due to excessive PF or a balance impairment
what is foot slap?
rapid PF at initial contact
what is high arch or Pes Cavus?
excessive supination
what is flatfoot or Pes Planus?
excessive pronation
what is too many toes?
excessive tibial or hip ER
what is extension thrust?
rapid movement into knee extension
what is valgus thrust?
rapid valgus moment
what is knock kneed?
valgus position of the knee
what is varus thrust?
rapid varus moment
what is bow legged?
varus position of the knee
what is trendelenburg gait?
excessive contralateral hip drop
what are the phases within single limb support?
mid stance and terminal stance
what are the key events of single limb support?
ankle rocker
forefoot rocker
stance limb stability
trunk stability
what is the importance of the ankle rocker during single limb support?
it is required for the initiation of forefoot rocker
it begins storing elastic energy in the achilles as our PF’s stretch
it minimizes COM displacement
what is the importance of forefoot rocker during single limb support?
it is required for initiation of toe rocker
helps store elastic energy in the achilles tendon
it minimzes COM displacement
what is the importance of stance limb stability during single limb support?
provides a stable base for the trunk to continue forward movement
minimizes lateral COM displacement
what is the importance of trunk stability during single limb support?
provides a stable base for efficient swing of the contralateral limb so that muscles can pull the swing limb forward
minimizes lateral COM displacement
what are problems during ankle and forefoot rocker in single limb stance?
if we don’t move enought into DF, the achilles will not be stretched enought to store energy or if we have decreased PF tone, they won’t store energy. Therefore there would be inadequate ankle and forefoot rocker. This minimizes elastic energy store which increases demand of muscles in the kinetic chain and increases COM displacement.
theres an increase in vertical COM displacement which increases demand of muscles in the kinetic chain and increases load on joints and passive stabalizers of the foot and ankle (if center of mass drops)
theres an increase in lateral COM displacement which increases load on passive stabalizers of the frontal plane, increases shear forces on joint surfaces and meniscus in the kinetic chain, and increases demand of muscles in the kinetic chain