Extended Treatment Fields
1/8
Earn XP
Description and Tags
ONCOL 355 - Planning and Dosimetry I. University of Alberta
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
9 Terms
why do we need extended treatment fields?
when we need a big field to treat entire volumes of interest
even when the collimators jaw size on LINACs is full, we still need more
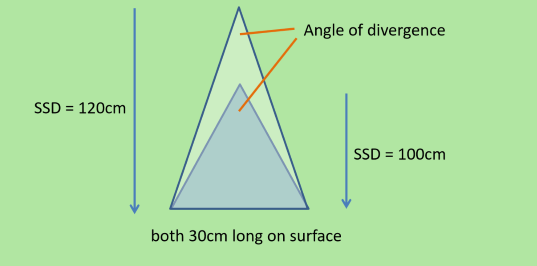
What do we have to use to treat extended treatment fields
beam divergence
need to move the patient greater than 100 cm SSD
can be done by lowering couch

What two plans can extended fields be used for
single field plans (SSD setup)
SSD > 100 cm, field size defined at surface
full leg/abdomen for example
POP plan —> SSD set up
SSD >100 cm, field size defined at surface at each beam entry point
essentially like doing 2 single fields however with compensate dose distribution like POP

How does the dosimetry change from a 40 cm field vs two 20 cm fields
there is decreased scatter at the field edges because the RT is so divergent that the scattered particles are less likely to be deflected back and contribute dose to the field edges
we may choose to have 2 20 cm abutting fields
How does dose rate change at extended distances
dose rate will decrease the further away we treat
meaning longer treatment times (more MU to get dose to depth)

If SSD increases, what happens to PDD?
The percentage depth dose (PDD) increases due to less divergence so there is more scatter back to the calc point
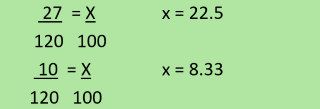
If we have a field size of 27 × 10 cm (LxW) at 120 cm SSD, what does the collimator setting need to be at 100 cm to get the same field size
L = 22.5 cm
W = 8.33 cm
We need a field length of 37 cm, and the max jaw size is 35×35 cm. What SSD should we plan for the patient?
105.7 cm
we usually will just round up to 110 cm
using the same previous question, if the SSD of this patient plan is 110 cm, what is the collimator setting for the jaw?
33.6 cm