week 38 - ovarian cancer
0.0(0)
Studied by 1 personCard Sorting
1/16
There's no tags or description
Looks like no tags are added yet.
Last updated 4:05 PM on 7/8/26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
1
New cards
ovarian cancer introduction
* lifetime risk of 1:75
* 70% occur in >55 (risk increases with increasing age)
* ‘silent killer’ because it typically has no symptoms until it reaches an advanced stage → bloating, pelvic or abdominal discomfort or pain, difficulty eating a meal or early satiety and urinary symptoms
* may cause ascited, omental and/or peritoneal metastases all of which are signs of advanced stage disease
* may lead to acute symptoms caused by pleural effusion, bowel obstruction or venous thromboembolism etc
* most are diagnosed at an advanced stage
* stage I disease has <10% chance of a recurrence, whereas stage IV disease has >90% chance recurrence after treatment of the primary disease
* overall the 5 year survival is 30-40%
* the best overall survival and progression-free survival outcomes were seen in patients with no residual macroscopically visible tumour after surgery (‘complete cytoreduction’)
this may increase 5 year survival from 30 to 60%
* epithelial malignancies (carcinomas) comprise around 90% of malignant tumours found in the ovaries
* the rest are non epithelial → germ cell tumours (mainly diagnosed in the first 2 decades) and sex cord stromal tumours (more common in adult women)
ovarian metastases of other tumours are also non epithelial
* 70% occur in >55 (risk increases with increasing age)
* ‘silent killer’ because it typically has no symptoms until it reaches an advanced stage → bloating, pelvic or abdominal discomfort or pain, difficulty eating a meal or early satiety and urinary symptoms
* may cause ascited, omental and/or peritoneal metastases all of which are signs of advanced stage disease
* may lead to acute symptoms caused by pleural effusion, bowel obstruction or venous thromboembolism etc
* most are diagnosed at an advanced stage
* stage I disease has <10% chance of a recurrence, whereas stage IV disease has >90% chance recurrence after treatment of the primary disease
* overall the 5 year survival is 30-40%
* the best overall survival and progression-free survival outcomes were seen in patients with no residual macroscopically visible tumour after surgery (‘complete cytoreduction’)
this may increase 5 year survival from 30 to 60%
* epithelial malignancies (carcinomas) comprise around 90% of malignant tumours found in the ovaries
* the rest are non epithelial → germ cell tumours (mainly diagnosed in the first 2 decades) and sex cord stromal tumours (more common in adult women)
ovarian metastases of other tumours are also non epithelial
2
New cards
physiology of ovarian cancer
1. site of origin and carcinogenesis:
* originally, the ovary was considered the primary site of almost all ovarian tumours
* but various subtypes of ovarian cancer (serous, endometrioid, mucinous and clear cell) resemble the epithelium of the fallopian tube, endometrium, endocervix and GI tract, respectively
*subsequently, close examination of the fallopian tube led to the frequent identification of* ==__*preinvasive and early invasive high-grade serous cancers in the fallopian tube*__==
* it is currently assumed that the majority, if not all, high-grade serous cancers originate from the epithelium of the distal fallopian tube
* a clonal relationship between STICs (serous tubal intraepithelial carcinomas) and high-grade serous cancer lesions was found → ==__high grade serous cancer presenting as an ovarian tumour should probably designated as tubal carcinoma__==
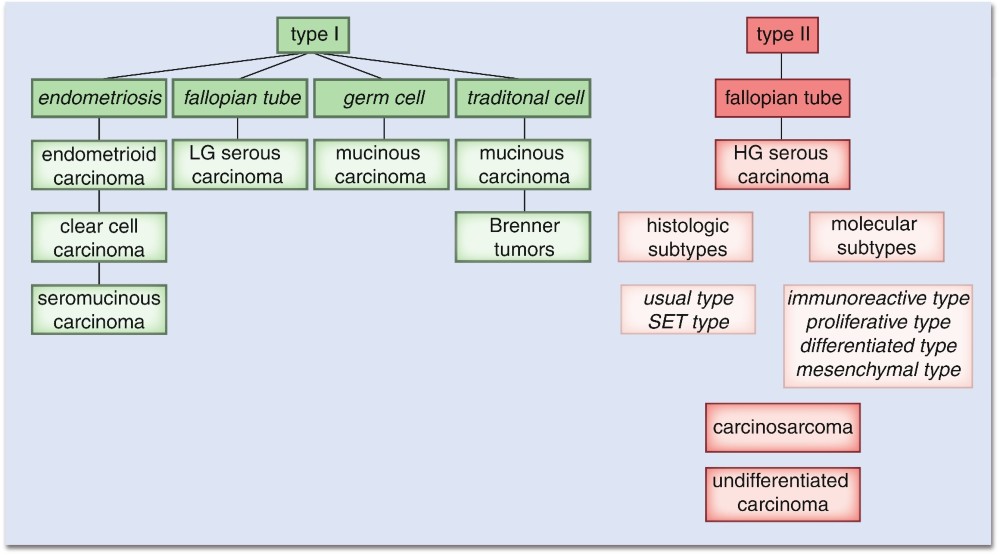
* ovarian cancers are split into type I and II and then further subdivided into histological categories
* ==__endometrioid and clear cell carcinomas do not have a direct relationship with the fallopian tube, but their origin is likely related to endometriosis__==
due to chronic inflammation → chronic imbalance of inflammatory mediators → can act as growth mediators
also PTEN and KRAS mutations have been described in endometriosis
* *for primary ovarian mucinous tumours the cell of origin remains unclear, but might be related to teratoma, which is in fact a germ cell tumour, and/or endometriosis. Often, mucinous carcinomas located in the ovary turn out to be metastatic disease of gastrointestinal malignancies*
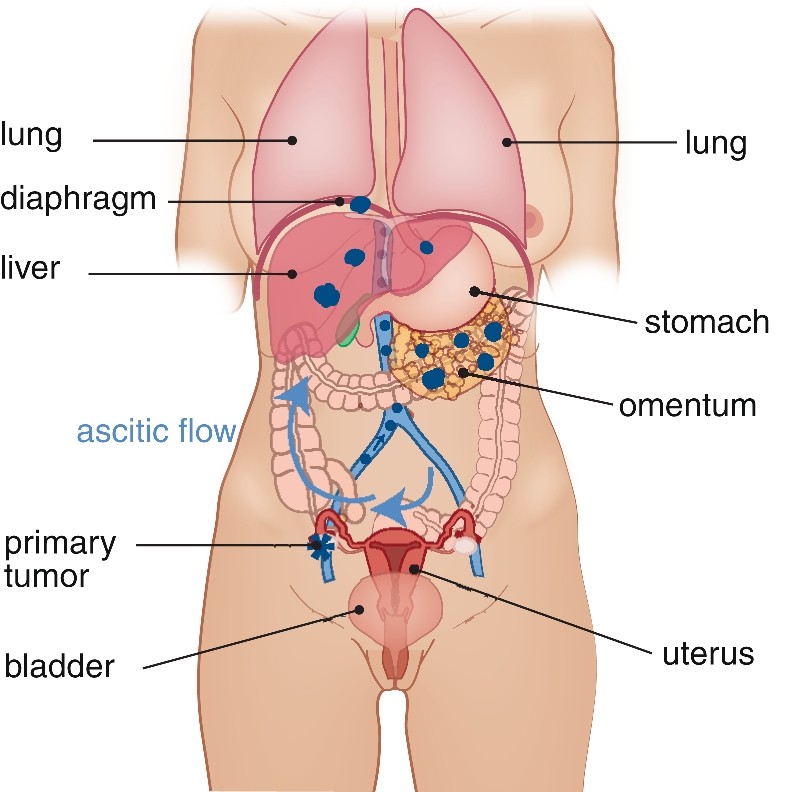
2. pattern of disease spread:
* spread to the peritoneum and intra-abdominal organs through ==__exfoliation__== (process of spontaneous or induced complete detachment of single epithelial (tumour) cells)
* transported throughout the peritoneal cavity by the natural circulation of peritoneal fluid, from the pericolic gutters (???) (especially on the right side), along the intestinal mesentery to the right hemidiaphragm
* advanced stage → excessive shedding of tumour cells into the peritoneal cavity → ascites → facilitates spread of tumour cells throughout the peritoneal cavity
* can also spread lymphatically (most common through the pelvic and para-aortic lymph nodes) and haematogenously
* may reach the pleural cavity and supraclavicular lymph nodes in advanced stage
* distant metastases are most commonly found in liver, lung and pleura
3
New cards
types I and II ovarian cancers
4
New cards
what is the most common type of ovarian cancer in lynch syndrome
endometrioid
5
New cards
spread of ovarian cancer
6
New cards
pathophysiology of epithelial ovarian tumours
1. serous:
1. benign serous:
* 60% of serous tumours, bilateral 7-20%, 1 to > 30 cm
* serous cystadenomas → unilocular or multilocular cysts + thin wall, smooth outer surface + inner lining with smooth single layered serous epithelium, resembling tubal epithelium
* serous adenofibromas → share features with ^ but the wall is solid and fibrous
2. borderline serous:
* 10-15% of serous tumours, bilateral 25-40%, usually > 5cm
* unilocular or multilocular cystic tumours, smooth outer surface but can contain polypoid excrescences
* inner surface comprises serous epithelium, with pseudostratification of the nuclei, nuclear enlargement and increased mitosis, this epithelium lines flat surfaces, with arborizing papillary structures (???)
* survival of stage I SBTs is not different from the general population
3. malignant serous → low and high grade serous carcinomas
1. low grade serous carcinoma:
* < 10% of serous carcinomas, mean age of 46, >90% have stage II or higher but stage IV is rare
* KRAS or BRAF mutations are found in 50-60% (but targted therapy rarely works)
* often mixed with serous borderline tumours
* macroscopically → multilocular cysts with papillary formations
* microscopically → papillary or micropapillary fronds, consisting of tumour cells with small, uniform nuclei and a low mitotic count
2. high grade serous carcinoma:
* 30% of serous tumours, ==__> 80% of ovarian carcinomas__==, mean age 56, bilateral in 65% if highstage but 25% if stage I
* > 80% have p53 mutations (5-15% have BRCA1/2)
* vary in size
* macroscopically → can be solid, cystic, papillary or a mixture
* microscopically → solid and papillary are the most common patterns, but cribriform and microcystic patterns may also occur
* large centrally placed nuclei with prominent nucleoli and high mitosis
2. mucinous:
1. benign mucinous (mucinous cystadenomas):
* 80% of primary ovarian mucinous tumours, mean age of 50, 95% are unilateral
* macroscopically → large unilocular cysts
* microscopically → thin-walled fibrous cysts lined by mucinous epithelium (resembles mucinous epithelium of the GI tract (can vary which part of the GI))
* sometimes these cysts are associated with a teratoma (dermoid cyst) or Brenner tumour
2. borderline mucinous:
* 2nd most common borderline ovarian tumour (30-50%), mean age 40-49, mostly unilateral, if bilateral it should raise suspicion of metastasis
* macroscopically → cystic unilocular or multilocular cystic tumours, with a high variation in size (diameter up to 50 cm), weighing several kilograms
* outer surface is smooth + cysts are filled with mucinous material
* microscopically → lined by intestinal type mucinous epithelium + villiform papillae with pseudostratification of the nuclei, nuclei enlargement and increased mitosis
* ==__*sometimes transitions to small proliferative foci and even intra-epithelial carcinoma are found but if they don’t exceed 5 mm, they do not negatively influence the prognosis and therefore, unless in the presence of intra-epithelial carcinoma, they are classified as borderline mucinous tumours*__==
3. mucinous carcinoma:
* 3-4% of all primary ovarian carcinomas, mean age of 45, unilateral
* macroscopically → complex solid and cystic tumours, variable sizes
* microscopically → complex structures of glands, arborizing slender papillae, cribriform and solid areas of mucinous cells
* the mucinous cells often show loss of mucin production, nuclear enlargement, hyperchromasia and increased mitotic activity (??? but theyre mucinous lol)
* 2 types of invasion:
1. expansile pattern of invasion → dilating cysts with little or no stromal reaction (may be difficult to differentiate from a borderline tumour except for complexity of the tumour)
2. infilitrative pattern → smaller or larger infiltrating clusters of mucinous cells, with hyper-maturation, severe atypia and induction of desmoplastic stroma
* *A transition between benign and borderline to malignant features is often seen in primary ovarian mucinous carcinomas. This feature can be of great value to differentiate between metastatic mucinous tumours involving the ovary, as metastatic tumours often show the same or even less malignant cellular and architectural features. Immunohistochemistry is only useful in a minority of cases to distinguish primary mucinous ovarian carcinoma from a metastasis from the gastrointestinal tract*
3. endometrioid:
1. bening endometrioid:
* endometriotic cysts = cystic forms of endometriosis in the ovary, with or without pelvic or intra-abdominal endometriosis
* endometriotic cystadenomas in general show the same features, but lack the endometriotic stroma
2. borderline → rare
3. malignant endometrioid (endometrioid carcinoma):
* 10-15% of ovarian carcinomas, mean age of 58, bilateral in 15-20%, mean diameter of 15 cm
* macroscopically → smooth outer surface and a cut surface with solid and cystic areas, often containing blood or haemorrhagic fluid
* microscopically → complex cribriform formations and closely packed glandular structures of endometrioid epithelium
* tumour cells show nuclear enlargement, mitotic activity and frequently signs of apoptosis
* squamous morular metaplasia is frequently seen
\
clear cell carcinoma is often associated with endometriosis, treated the same as high grade serous carcinoma
the Brenner tumour (epithelial tumours (seem to be of mullerian origin, ==__wtf does that mean???__==) resembling transitional epithelium) may be benign or malignant and may be associated to mucinous tumours
7
New cards
stromal reaction
stromal reaction in cancer is similar to the stromal reaction induced by injury or wound repair: increased ECM and growth factor production and secretion, which consequently cause growth of the tissue
8
New cards
adenoma vs adenocarcinoma
Some tumors found in glandular cells are not cancerous. These are called adenomas. However, some tumors that form in the glandular cells are cancerous. These are called adenocarcinomas
9
New cards
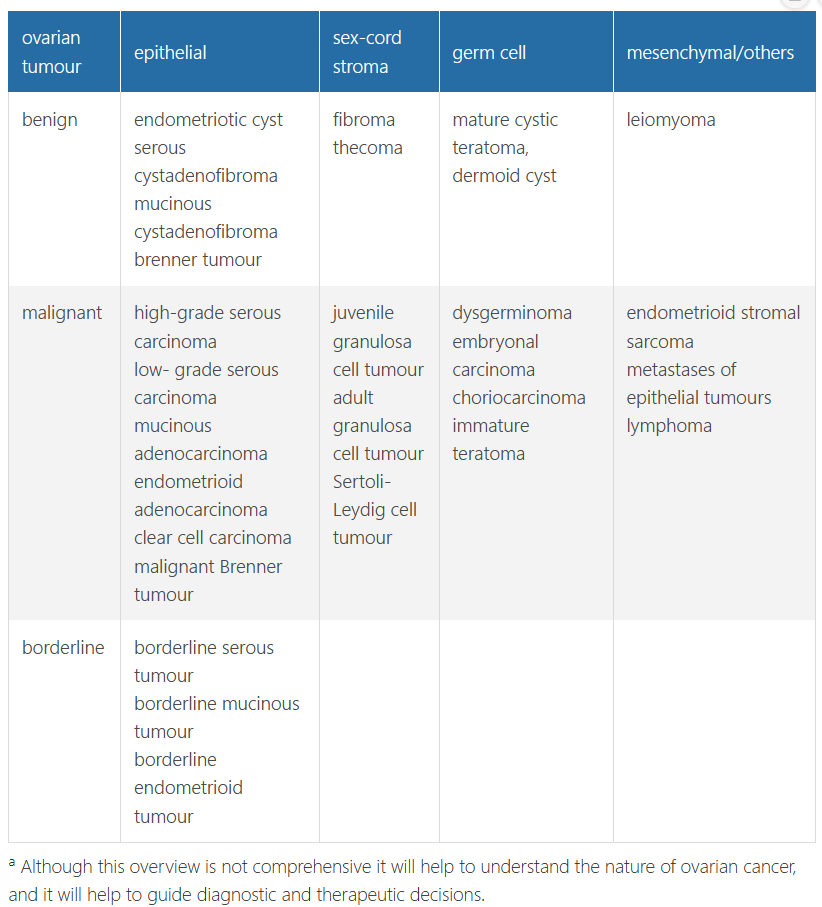
overview of the most commonly diagnosed ovarian tumours
Based on histological criteria the majority of these tumours fall within three major categories: serous, mucinous, and endometrioid tumours. Clear cell and Brenner tumours are less frequently found
10
New cards
pathophysiology of non epithelial ovarian tumours
(these are main 2, there are more)
\
1. sex cord stromal tumours
1. pure stromal tumours → ovarian fibroma and ovarian thecoma (or a combo = fibrothecoma)
* both are benign
* fibromas → 4% of ovarian neoplasms, mean age of 48
* presents as a pelvic mass, almost always unilateral
* macroscopically → smooth outer surface and on cut surface they show a grey-white solid aspect, sometimes with oedema and cystic degeneration
* hard to elastic consistency
* microscopically → composed of intersecting bundles of spindle cells with bland nuclei
often rich in collagen
* thecomas → 1% of ovarian neoplasms, mean age of 59, unilateral
* frequently present with oestrogenic symptoms, although androgenic symptoms are also described (go over this\*\*\*)
* macroscopically → smooth outer surface and a yellow cut surface, due to the presence of steroid hormone producing cells
* microscopically → composed of sheets of ovoid uniform tumour cells, without nuclear atypia
2. pure sex cord tumours → granulosa cell tumours
* best known form is adult granulosa cell tumour (juvenile is rare)
* 1% of all ovarian tumours, mean age of 53 (but wide range)
* present in postmenopausal women with vaginal blood loss
* present in younger patients with bleeding disorders such as menorrhagia or amenorrhoea, sometimes presents with virilisation (in both ages or?)
* normally unilateral, 10 cm but can vary
* macroscopically → outer surface is smooth, cut surface shows a mixture of solid and cystic areas with weak consistency and tan to yellow colour
* microscopically → different growth patterns
→ often trabeculae, sheets and cords of cell with palte cytoplasm and a centrally located round to slightly irregular nucleus, with a bland appearance and classically a nuclear groove
* clinical course is that of a low-grade malignant tumour
* intraperitoneal recurrences or lymph node metastases can be found after long intervals, sometimes exceeding 5 years or more
2. germ cell tumours:
1. benign germ cell tumours:
* consist of mature teratomas derived from 1 germ layer (monodermal teratomas) and those derived from 2 or 3 germ layers (mature cystic teratomas, formerly known as dermoid cysts)
* mature cystic teratomas are frequently seen, accounting for 20 % of the ovarian tumours
* can occur at any age but are mostly seen during reproductive ages
* macroscopically → cysts, often filled sebaceous material, frequently combined with hair
* cyst wall may contain a solid elevation, in which the presence of nearly all tissue types is described
* may occur with primary ovarian mucinous tumours
2. malignant germ cell tumours:
* immature teratomas can present as a mature cystic teratoma, in which a microscopic proportion of immature tissue is present
* otherwise the tumour consists almost entirely of immature tissue which usually has primitive neuro-ectodermal tissue
* although CT may be needed, prognosis is good
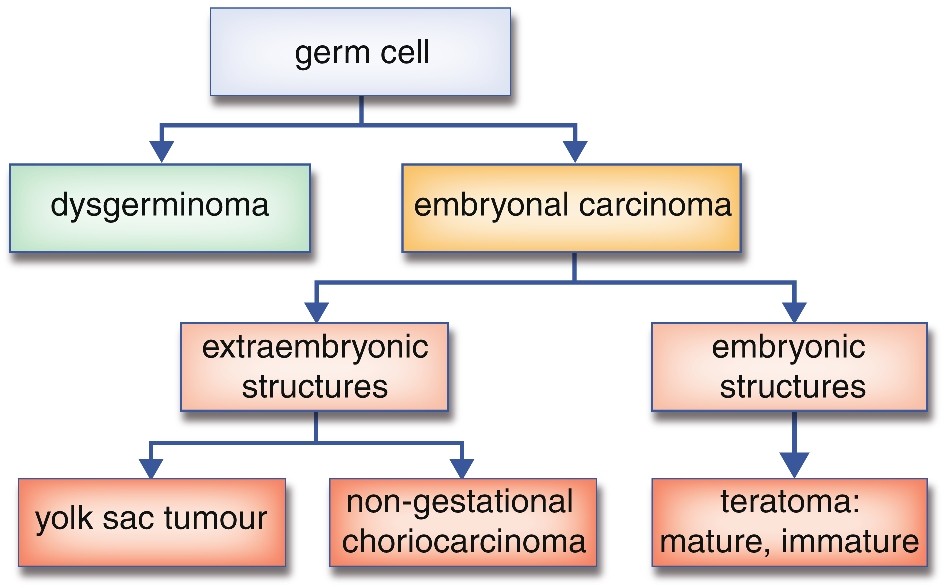
* dysgerminoma:
* most common ovarian germ cell tumours
* = a primitive germ cell tumour consisting of tumour cells without features of differentiation
* mean age of 22
* macroscopically → >10 cm, consist of a solid mass with a soft and tan appearance
* haemorrhage and necrosis or degeneration is frequently present
* microscopically → consists of sheet and solid areas of undifferentiated large tumour cells, with large nuclei and a high mitotic count
* often also contains lymphocytes
* male counterpart = seminoma
* most present with a fast growing abdominal mass, often accompanied by abdominal pain due to haemorrhage or necrosis
* extremely sensitive to CT
\
1. sex cord stromal tumours
1. pure stromal tumours → ovarian fibroma and ovarian thecoma (or a combo = fibrothecoma)
* both are benign
* fibromas → 4% of ovarian neoplasms, mean age of 48
* presents as a pelvic mass, almost always unilateral
* macroscopically → smooth outer surface and on cut surface they show a grey-white solid aspect, sometimes with oedema and cystic degeneration
* hard to elastic consistency
* microscopically → composed of intersecting bundles of spindle cells with bland nuclei
often rich in collagen
* thecomas → 1% of ovarian neoplasms, mean age of 59, unilateral
* frequently present with oestrogenic symptoms, although androgenic symptoms are also described (go over this\*\*\*)
* macroscopically → smooth outer surface and a yellow cut surface, due to the presence of steroid hormone producing cells
* microscopically → composed of sheets of ovoid uniform tumour cells, without nuclear atypia
2. pure sex cord tumours → granulosa cell tumours
* best known form is adult granulosa cell tumour (juvenile is rare)
* 1% of all ovarian tumours, mean age of 53 (but wide range)
* present in postmenopausal women with vaginal blood loss
* present in younger patients with bleeding disorders such as menorrhagia or amenorrhoea, sometimes presents with virilisation (in both ages or?)
* normally unilateral, 10 cm but can vary
* macroscopically → outer surface is smooth, cut surface shows a mixture of solid and cystic areas with weak consistency and tan to yellow colour
* microscopically → different growth patterns
→ often trabeculae, sheets and cords of cell with palte cytoplasm and a centrally located round to slightly irregular nucleus, with a bland appearance and classically a nuclear groove
* clinical course is that of a low-grade malignant tumour
* intraperitoneal recurrences or lymph node metastases can be found after long intervals, sometimes exceeding 5 years or more
2. germ cell tumours:
1. benign germ cell tumours:
* consist of mature teratomas derived from 1 germ layer (monodermal teratomas) and those derived from 2 or 3 germ layers (mature cystic teratomas, formerly known as dermoid cysts)
* mature cystic teratomas are frequently seen, accounting for 20 % of the ovarian tumours
* can occur at any age but are mostly seen during reproductive ages
* macroscopically → cysts, often filled sebaceous material, frequently combined with hair
* cyst wall may contain a solid elevation, in which the presence of nearly all tissue types is described
* may occur with primary ovarian mucinous tumours
2. malignant germ cell tumours:
* immature teratomas can present as a mature cystic teratoma, in which a microscopic proportion of immature tissue is present
* otherwise the tumour consists almost entirely of immature tissue which usually has primitive neuro-ectodermal tissue
* although CT may be needed, prognosis is good
* dysgerminoma:
* most common ovarian germ cell tumours
* = a primitive germ cell tumour consisting of tumour cells without features of differentiation
* mean age of 22
* macroscopically → >10 cm, consist of a solid mass with a soft and tan appearance
* haemorrhage and necrosis or degeneration is frequently present
* microscopically → consists of sheet and solid areas of undifferentiated large tumour cells, with large nuclei and a high mitotic count
* often also contains lymphocytes
* male counterpart = seminoma
* most present with a fast growing abdominal mass, often accompanied by abdominal pain due to haemorrhage or necrosis
* extremely sensitive to CT
11
New cards
social determinants of ovarian cancer
* risk factors of epithelial ovarian cancer → early menarche, nulliparity, late menopause and increasing age
* risk decreases with → more pregnancies, breast feeding and tubal ligation
oral contraceptive use is associated with a 30-50% reduction in risk of ovarian cancer, depending on duration
* the associations between oral contraceptive use and parity with reduced risk have also been confirmed for women who carry a *BRCA1* or *BRCA2* mutation
* 18-24% of all cases of ovarian cancer are due to an inherited mutation of BRCA1/2
other mutations (moderate to low penetrance genes) → lynch syndrome (MMR genes) and peutz jeghers (STK11 gene)
* familial ovarian cancer also obviously increases the risk
*women with one first-degree relative (FDR) have a hazard risk (HR) for developing ovarian cancer of approximately 2, however with two or more relatives (of which one FDR) the life-time risk increases to more than 10%*
* it is recommended to undergo genetic counselling in all women diagnosed with ovarian cancer regardless of the type or staging
* risk decreases with → more pregnancies, breast feeding and tubal ligation
oral contraceptive use is associated with a 30-50% reduction in risk of ovarian cancer, depending on duration
* the associations between oral contraceptive use and parity with reduced risk have also been confirmed for women who carry a *BRCA1* or *BRCA2* mutation
* 18-24% of all cases of ovarian cancer are due to an inherited mutation of BRCA1/2
other mutations (moderate to low penetrance genes) → lynch syndrome (MMR genes) and peutz jeghers (STK11 gene)
* familial ovarian cancer also obviously increases the risk
*women with one first-degree relative (FDR) have a hazard risk (HR) for developing ovarian cancer of approximately 2, however with two or more relatives (of which one FDR) the life-time risk increases to more than 10%*
* it is recommended to undergo genetic counselling in all women diagnosed with ovarian cancer regardless of the type or staging
12
New cards
prevention of ovarian cancer
1. ovarian cancer screening:
* possible transvaginal US and CA125 levels yearly but they dont seem to increase rate of diagnosis or a reduction in morbidity sooooo no effective screening tools
2. risk reducing salpingo oophorectomy:
* since no effective screening tools for early detection of ovarian cancer are currently available, risk-reducing salpingo-oophorectomy (RRSO) is the only effective strategy to reduce ovarian cancer incidence and mortality in high-risk women = life time risk of ovarian cancer of at least 10% which includes all **BRCA1**
* prophylactic surgery is recommended before the age at which the incidence rises, which is 35-40 for *BRCA1* carriers and 40-45 for *BRCA2* carriers
* RRSO has an effectivenes of 96% in preventing BRCA associated ovarian cancers
* women with an estimated ovarian cancer risk of 10 % or more due to familial ovarian cancer or another mutation can also apply for RRSO, although there is no recommended age for RRSO in these women so theyre usually done around menopause
* RRSO would cause an acute hypo oestrogenic status → short term side effects such as hot flushes, sleeping problems, reduced sexual interest and vaginal dryness
long term have not been studied yet
13
New cards
diagnosis of ovarian cancer
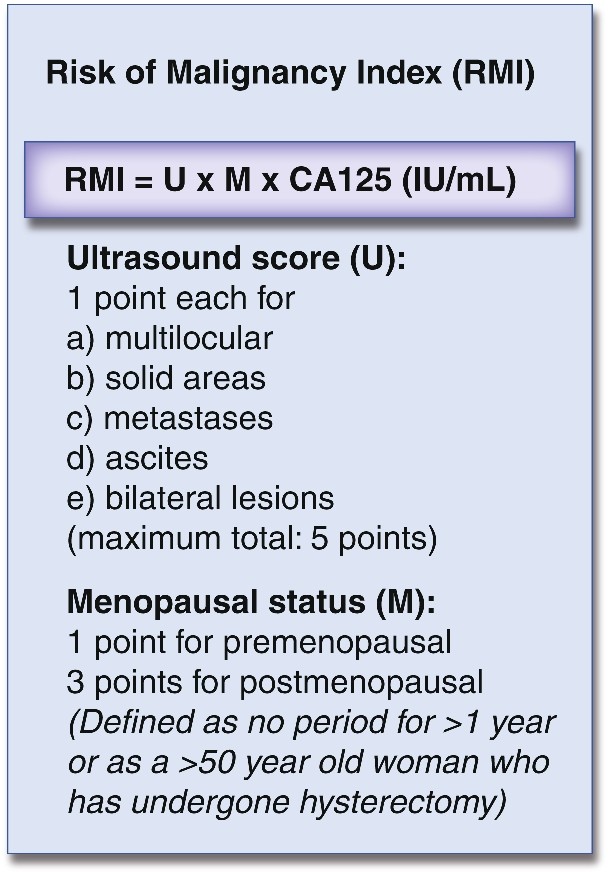
* adnexal mass? → verify the clinical suspicion of malignancy → use the Risk of Malignancy Index (RMI) → combines CA124, pelvic US and menopausal status
* RMI > 200 = high risk of malignancy → should be discussed and or referred
* CT scans of the chest and abdomen may be performed to determine the extent of disease
* diagnosis is only confirmed after surgical removal of the ovary, fallopian tube or biopsy of the omentum or on tissue or fluid obtained preoperatively since it is a histololgical diagnosis
* !! when non-epithelial origin is suspected serum human chorionic gonadotropin and ==__α-fetoprotein__== titres should be determined in addition to CA125. ==__Inhibin__== is secreted by granulosa cell tumours and is a useful tumour marker for this disease
* RMI > 200 = high risk of malignancy → should be discussed and or referred
* CT scans of the chest and abdomen may be performed to determine the extent of disease
* diagnosis is only confirmed after surgical removal of the ovary, fallopian tube or biopsy of the omentum or on tissue or fluid obtained preoperatively since it is a histololgical diagnosis
* !! when non-epithelial origin is suspected serum human chorionic gonadotropin and ==__α-fetoprotein__== titres should be determined in addition to CA125. ==__Inhibin__== is secreted by granulosa cell tumours and is a useful tumour marker for this disease
14
New cards
therapy for epithelial ovarian cancer
1. early stage:
* surgical staging is indicated in patients with apparent early stage epithelial ovarian cancer
→ entails surgical removal of ovaries, fallopian tubes and uterus, omentum, as well as surgical sampling of abdominal and pelvic areas, pelvic and para-aortic lymph nodes and peritoneal washings
==__wait??? EVERYTHING is removed?????__==
* adjuvant CT seems to help in high risk early stage disease (= stage IB/C grade 2/3, any stage grade 3 or clear-cell histology)
2. late stage:
* cytoreductive surgery → removal of all visible tumour tissue, also including removal of ovaries, fallopian tubes, uterus and omentum
* sometimes a bowel resection needs to be performed (then a stoma may be necessary, perm or temp)
* surgery is combined with CT when cytoreduction seems feasible with acceptable morbidity
* if surgery is not feasible or if unacceptable morbidity is expected then delay → neo adjuvant CT
→ *if complete or optimal cytoreduction seems feasible after 3 cycles of neo-adjuvant CT ‘interval cytoreductive surgery’ may be done → followed by at least 3 more cycles of adjuvant CT*
* the CT is platinum-based chemotherapy, generally carboplatin due to reduced toxicity compared with cisplatin, in combination with paclitaxel CT
* CT is administered through IV or through intra peritoneal delivery
* other possible treatment:
* targeted therapies with monoclonal antibodies
→ eg. bevacizumab targets the angiogenic factors VEGF (angiogenesis appears to be an important component driving the growth of ovarian cancer)
3. recurrent disease:
* around 70% of those with high stage ovarian cancer will replace within 3 years
* cytoreductive surgery may be considered in patients with a complete response following primary therapy, a disease free interval of at least 6 months and in patients with limited recurrent disease = surgery seems feasible
* the most important factor in determining the chance of response to 2nd line CT is the duration of the disease free interval since the last dose
→ platinum-sensitive disease when patients progress > 6 months after the CT
* platinum based CT is the treatment of choice (do we need to know specifics?)
→ platinum-resistance disease when patients progress 1–6 months CT
* they have a poor prognosis with a median life expectancy of < 12 months → palliatvive
* bevacizumab is being investigated
combination with CT is recommended for bevacizumab-naïve patients with a platinum-sensitive recurrence
* single agent PARP inhibitor therapy is approved as maintenance treatment for patients with somatic or germline BRCA mutations after response to CT
* *at time of recurrent disease there are, in general, no curative treatment options and certainly not if 2nd line CT fails*
4. palliative treatment:
* advanced epithelial ovarian cancer is ultimately fatal in the majority of cases, despite optimal management with surgery and CT
* the cancer causes symptoms, but the treatment can also cause adverse effects including neuropathy, nausea and fatigue
* CT can be used for palliative care (so then whats causing the symptoms???)
* other options → intermittent ascitic drains or a permanent tunnelled ascitic drain, blood transfusion in case of anaemia and pain management
15
New cards
evaluating response to treatment and follow up\*\*\*
*CA125 is elevated in most patients with advanced disease and serial measurement is a useful marker to assess the response to chemotherapy. If the CA125 value does not reach the normal range or when there is residual disease on CT, front-line treatment is considered to have achieved only a ‘partial response’.*
*There is little evidence guiding the type of follow-up after completion of primary treatment. Clinical evaluation with or without pelvic examination is often carried out every 3 months for 2 years, after which the frequency of follow-up is reduced. In a randomized phase III trial, monitoring of CA125 after completion of primary treatment was shown to increase amount of chemotherapy given, due to earlier detection of recurrence. This reduced quality of life without improving overall survival and should therefore not be performed during follow-up. However, CA125 monitoring may have value in the detection of recurrence in chemotherapy-naïve patients after early stage disease, and in the detection of surgically resectable recurrence. Trials aiming to answer this question are ongoing.*
*There is little evidence guiding the type of follow-up after completion of primary treatment. Clinical evaluation with or without pelvic examination is often carried out every 3 months for 2 years, after which the frequency of follow-up is reduced. In a randomized phase III trial, monitoring of CA125 after completion of primary treatment was shown to increase amount of chemotherapy given, due to earlier detection of recurrence. This reduced quality of life without improving overall survival and should therefore not be performed during follow-up. However, CA125 monitoring may have value in the detection of recurrence in chemotherapy-naïve patients after early stage disease, and in the detection of surgically resectable recurrence. Trials aiming to answer this question are ongoing.*
16
New cards
treatment for non epithelial ovarian cancer
* most frequent non-epithelial ovarian tumours are GCTs (diagnosed mainly in the first 2 decades) and SCSTs (especially granulosa cell tumours) (most commonly in adult women)
* GCTs are extremelty sensitive to CT so primary surgery should be conservative
*depending on the tumour stage, primary surgery is followed by watchful waiting or multimodality chemotherapy. Fertility can be preserved in most cases*
* adult-type granulosa cell tumour → resection of all visible tumour is considered adequate surgical treatment
* long term (> 10-20 y) disease free intervals can be achieved by surgery alone
* endometrial sampling should be performed to rule out the presence of concomitant endometrial cancer due to incessant oestrogenic stimulation
* *when surgery is no longer possible, chemotherapy or endocrine therapy is an option in symptomatic patients*
* GCTs are extremelty sensitive to CT so primary surgery should be conservative
*depending on the tumour stage, primary surgery is followed by watchful waiting or multimodality chemotherapy. Fertility can be preserved in most cases*
* adult-type granulosa cell tumour → resection of all visible tumour is considered adequate surgical treatment
* long term (> 10-20 y) disease free intervals can be achieved by surgery alone
* endometrial sampling should be performed to rule out the presence of concomitant endometrial cancer due to incessant oestrogenic stimulation
* *when surgery is no longer possible, chemotherapy or endocrine therapy is an option in symptomatic patients*
17
New cards
when should a non epithelial tumour always be suspected
all women < 30 years of age with an abdominal mass
→ measure not only CA125 but also alpha fetoprotein and inhibin
→ measure not only CA125 but also alpha fetoprotein and inhibin