PSYC 301 MT2 - Attention
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
visuospatial attention
selectively focus on a location in space while ignoring others
*different from attention in attention-deficit/hyperactivity disorder → executive function (planning, monitoring performance, concentrating)
classic test of visuospatial attention: posner cueing task
measures reaction time differences
two trial types:
1. congruent: cue predicts target location
2. incongruent: cue misleads
posner cueing task - results
early after cue presented → faster responses (facilitation)
later after cue presented → slower responses (inhibition of return, attention suppresses going back to the same spot)
posner cueing task - purpose
allows researchers to study visuospatial attention independent of gaze
posner cueing task - elements
can change elements of task depending on research question
- amount of time cue is up
- location of cue
- appearance of cues
contralateral neglect/hemispatial or unilateral neglect
failure to notice or respond to objects on the side opposite the brain lesion
spatial bias: eyes and movements are drawn toward the same side as the lesion (ipsilesional side)
neglect - causes
not caused by basic vision or motor problems—rather, attention to the opposite side (contralesional space) is reduced
causes: most often stroke, but also trauma or alzheimer's disease
neglect - features
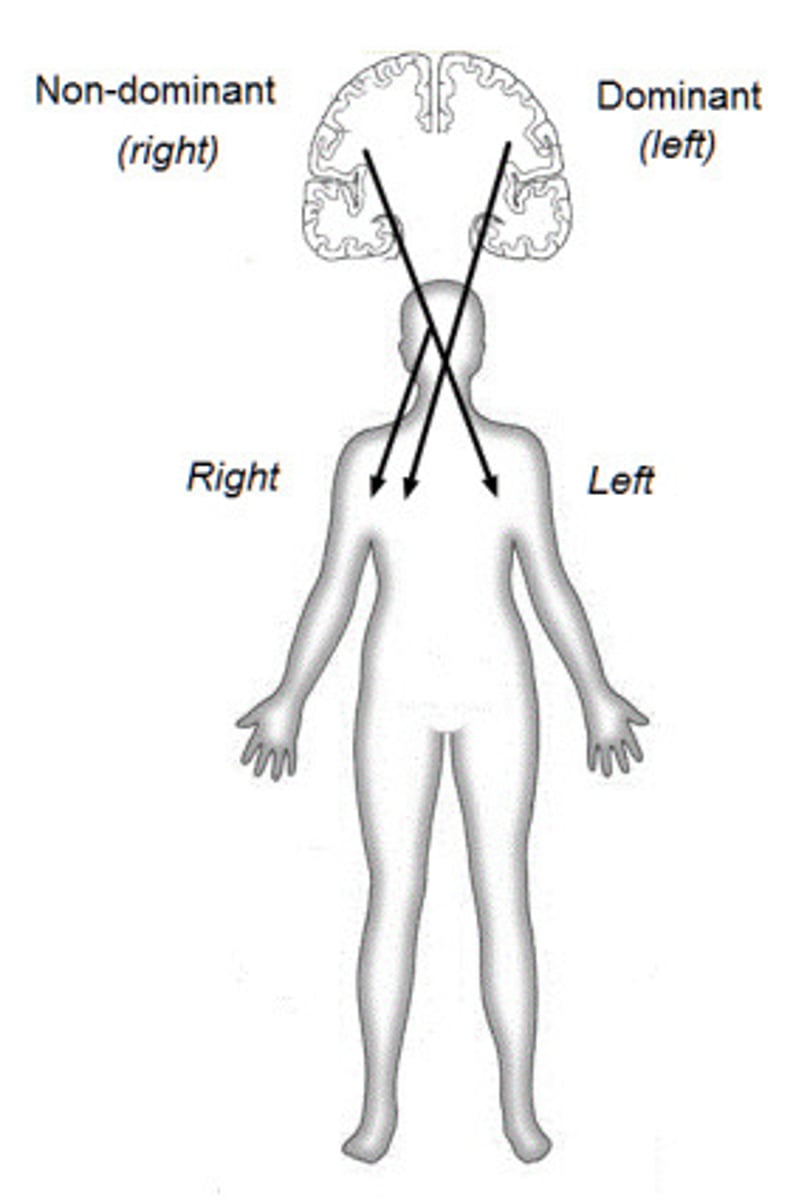
typical pattern: right hemisphere damage → left-side neglect
affects 25-30% of stroke patients, 3-5 million a year worldwide
even body parts on neglected (contralesional) side can be ignored
neglect - tests
1. clock drawing
2. line cancellation: given a piece of paper with black lines and asked to cross out all lines
3. drawing: may only draw on right side
4. eye movements: eyes movements mostly on right side
5. imagination: neglects left side of space, only described all landmarks on the right
6. visual judgement: fail to notice abnormalities occurring on the neglected (usually left) side. when asked which image they prefer, they often choose the "normal" one and more likely to notice dramatic oddities, even though they can't identify what's wrong with the other
7. line bisection: asked to mark middle of the line; if neglect is severe might mark very far right
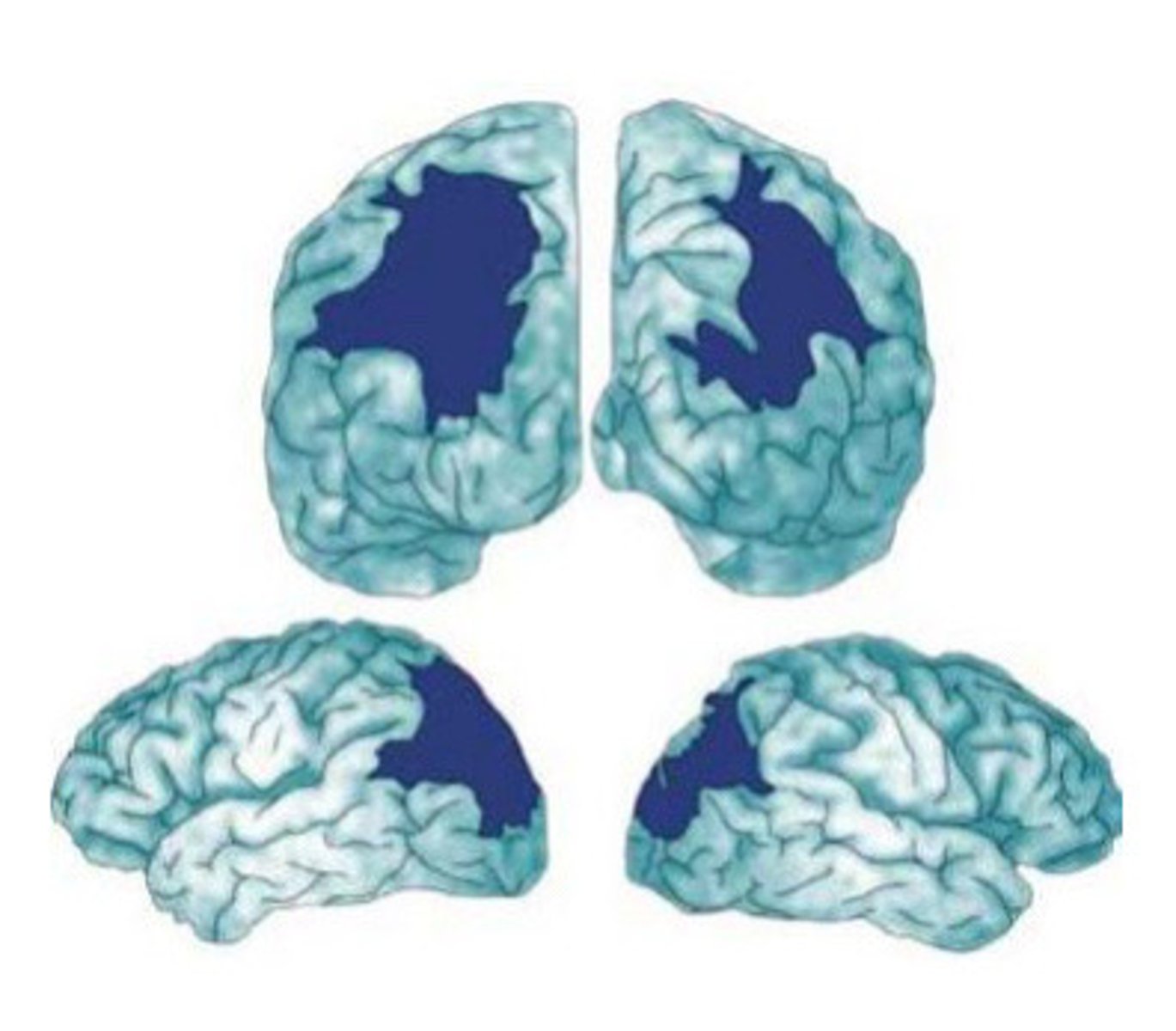
neglect - brain structures
all in right hemisphere, 3 major cortical areas
1. inferior parietal lobe and temporo-parietal junction
2. superior temporal gyrus
3. ventral frontal cortex
*damage to white-matter tracts connecting the 3 areas can also lead to neglect
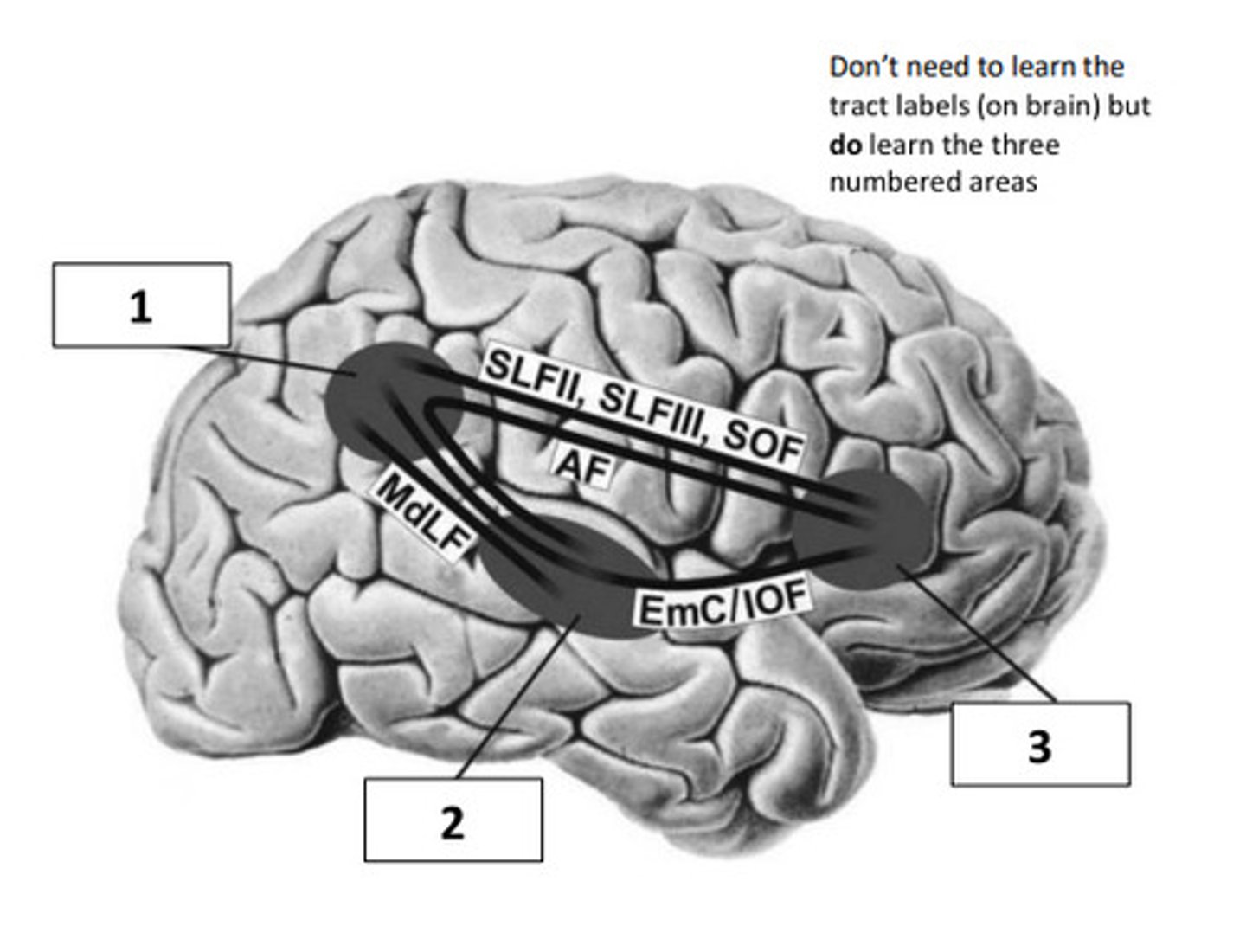
neglect - brain structures - function
spatial orienting, transforms signals from eyes and body into spatial representations
why is neglect so lateralized?
right parietal cortex monitors both sides of space while left parietal cortex monitors only right
pseudoneglect
asymmetry in brain lateralization can be seen in healthy adults too
tested via line bisection → non-brain damaged individuals show slight bias to the left (pseudoneglect) because the right hemisphere is so dominant in processing space (i.e. perceiving left side to be bigger than it is)
when do subcortical injuries lead to neglect?
DWI (diffusion-weighted imaging) show cortical injury
PWI (perfusion-weighted imaging) show areas of delayed blood flow
subcortical injuries lead to neglect only if there’s right-hemisphere cortical hypoperfusion (reduced blood flow to cortex), not subcortical damage alone
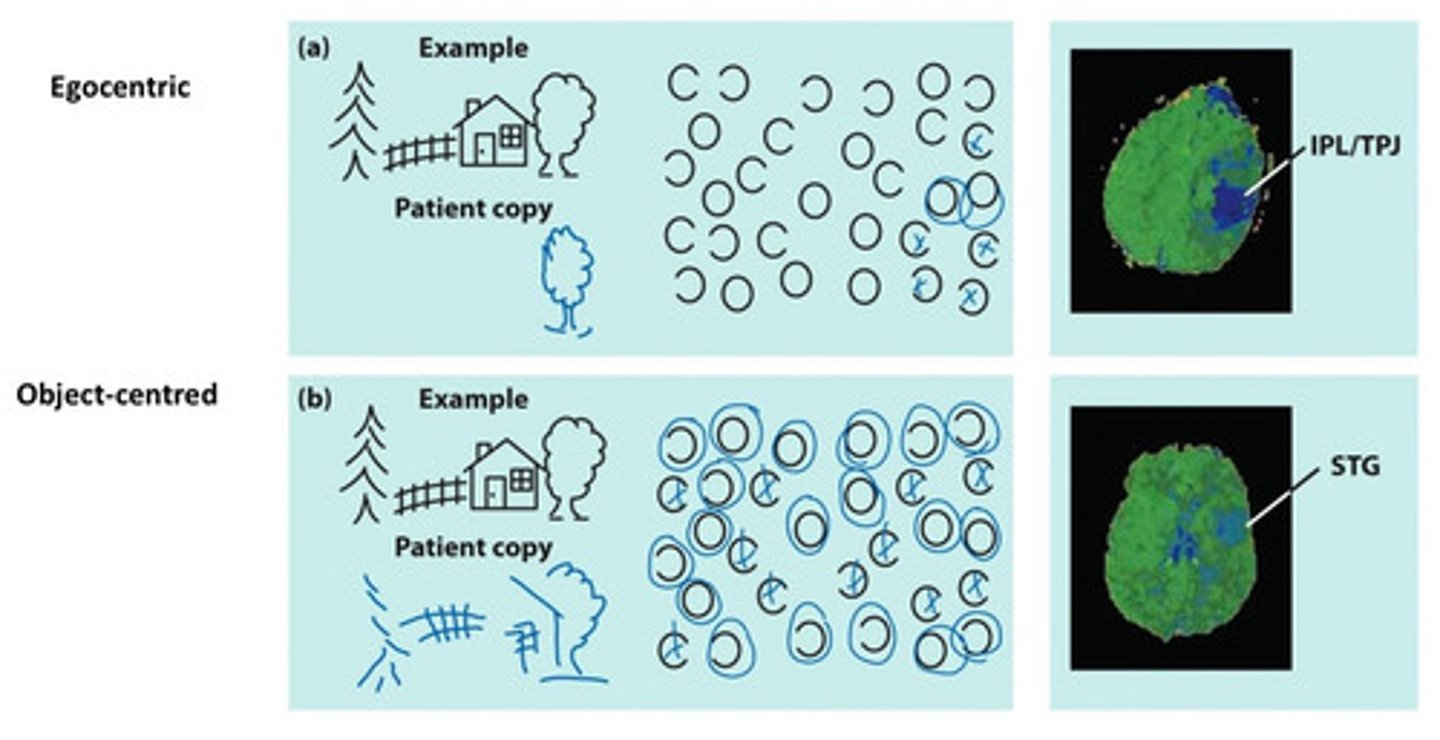
neglect - types
1. egocentric: neglects the left side of space relative to their own body
2. object-centred: neglects the left side of individual objects, no matter where the object is in space
neglect - recovery signs
1. allesthesia: mislocating stimuli from neglected side to non-neglected side
2. simultaneous extinction: detects stimulus on neglected side alone, but not when stimulated ipsilaterally (both sides together) because easily detected stimulus “cancels out” detection of other stimulus
neglect - spectrum of recovery
recovery ranges from temporary mild neglect → permanent denial of contralateral space
neglect - treatment
1. prismatic adaptation: shifting visual field can temporarily correct bias
2. VR reaching training: improves visual scanning and cancellation tasks
3. rTMS (inhibitory, low-freq) over left PPC: can lessen neglect for 15 days
balint’s syndrome
severe disruption of attention and explicit spatial awareness based on large region of brain damage
characterized by:
1. oculomotor apraxia
2. optic ataxia
3. simultanagnosia
e.g. cannot locate items they see and can’t tell when item is moved toward or away from them
oculomotor apraxia
can’t shift gaze (“sticky fixation” or “psychic paralysis of gaze”)
due to damage to saccade-planning areas in parietal cortex
optic ataxia
misreaching under visual guidance (especially with contralesional hand)
damage to superior parietal lobe
simultanagnosia
can only perceive one object at a time (can't see simultaneous objects/events)
balint's syndrome - functions that are impaired
sensory + language intact, but spatial attention severely impaired
balint's syndrome - causes
bilateral parieto-occipital damage (stroke, dementia, trauma)
balint's syndrome - recovery
only small case studies, no standard treatment program
coping strategies can help (e.g. practice dialing a phone) but neurological change is almost impossible because of the distribution of brain damage
peripersonal space (PPS) and other traits
attention system prioritizes space near the body
inside PPS → bisection performance left bias; outside → bisection performance right bias
large PPS: correlated to anxiety and claustrophobia
small PPS: correlated to autism and schizophrenia