Lecture 4 - Physical, Sensory, and Perceptual Development in Infancy
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Physical changes
Second-busiest period of physical change
First year: 25cm-30cm growth &triple body weight
Age 2 for girls and 2.5 for boys: half adult height
Heads are proportionately much larger – have nearly full-sized brain at that age
Brain changes
Nervous system continues to rapidly develop… Midbrain and medulla are most developed at birth; cortex is least developed
Synaptic development
Synapses connect neurons…
Synaptogenesis
Synaptic pruning
Occurs across the lifespan; gets more efficient
Denser synapses in children allows them to bounce back from brain harm more efficiently ➔ greater neuroplasticity
“Use it or lose it” – impact of environment
Synaptogenesis
The creation of synapses from the growth of dendrites and axons → Occurs rapidly in the first several years post-birth in spurts
Ongoing synaptogenesis = psychological changes linked to physical changes in the brain across the lifespan
Synaptic pruning
Unnecessary pathways and connections are eliminated
Myelinization
Creation of sheath around individual axons to insulate them from one another electrically
Improves their conductivity
Sheath made of myelin
Follows both cephalocaudal and proximodistal patterns • Why babies can move certain body parts before others
Fastest during first two years after birth; continues through adolescence
Reflexes
Changes, or lack thereof, can be key indicators of nervous system health… Humans are born with adaptive reflexes; some will disappear in infancy or childhood while others last a lifetime
Week or absent adaptive reflexes in newborns indicate the brain isn’t functioning as it should
Primitive reflexes
Primitive reflexes
Controlled by medulla and midbrain; their purpose is unclear
If primitive reflexes don’t disappear by 8 months of age, baby may have neurological problem
Sleep
Behavioural states
_______________ - States of consciousness: differing states of sleep and wakefulness
Five stages, in this order: deep sleep ➔lighter sleep ➔drowsy waking ➔ fussing ➔alert wakefulness
After feeding, return to drowsy state and then drop into deep sleep • Cycle repeats ~ every 2 hours
Newborns sleep up to 80% of the time
8 weeks: time awake increases and circadian rhythm begins to develop
6 months: sleeping ~13 hours/day, but more predictably
Crying
Behavioural states
________________ - Different cries for hunger, anger, and pain
Crying increase in frequency over first 6 weeks then tapers off
Cross-cultural similarity in strategies for soothing (i.e., picking up, holding, talking or singing)
Colic babies
Hunger
Behavioural states → crying
________________ - rhythmical pattern of cry, silence, breath, cry, silence, breath; whistling sound often accompanies in-breath
Anger
Behavioural states → crying
________________ - loud and intense
Pain
Behavioural states → crying
_______________ - abrupt onset (vs. whimpering or moaning to start)
Colic
Behavioural states → crying
_______________ - intense crying more than 3 hours/day, 3+ days/week, 3 or more weeks with no apparent cause and with nothing working to stop it
Motor skill development
Requires development in the brain, bones, muscles, lungs, and heart…. development follows cephalocaudal and proximodistal patterns
Relevant skills
Locomotor skills/gross motor skills
Non-locomotor skills
Manipulative skills/fine motor skills
Wide variability in these developmental milestones across cultures
Implications for standardization of developmental milestones
The sequence of development itself is virtually identical for all children, regardless of sex or the presence of physical or mental anomalies
Children with developmental challenges meet the milestones in the same sequence, just more slowly
Infants are motivated to meet these milestones – despite the risks they present – because of perceived benefits
Benefits: caregiver praise, exploring further and faster, and interacting with objects in new way
Bone development
(Motor skill development)
Changes to size, number, and composition
Changes in number and density result in improved motor coordination
Ossification
Ossification
(Motor skill development → bone development)
_________ - Bone hardening. Occurs steadily from final weeks of prenatal development through puberty
Necessary for motor development
Muscle development
(Motor skill development)
All muscle fibres are present at birth — Initially small with a high water to muscle ratio and a lot of fat
Water content is comparable to an adult’s by end of first year
Ratio of fat to muscle tissues begins decline by end of first year
These changes enable one-year-olds to begin walking
Lung + heart development
(Motor skill development)
Important for increasing stamina and strength in kids,
Lungs grow quickly and become more efficient during first two years
Heart muscles strengthen
Together, result in greater in two-year-olds (vs. newborns)
Toddlers can engage in fairly substantial periods of sustained motor activity without rest
Locomotor skills
(Motor skill development)
AKA gross motor skills — enable infant to get around their environment (e.g., crawling)
Non-locomotor skills
(Motor skill development)
Improve infant’s ability to interact with objects and people around them (e.g., controlling head movement)
Manipulative skills
(Motor skill development)
AKA fine motor skills — use of hands (e.g., stacking blocks)
Female babies
Develop more quickly in some areas… they may have a slight advantage in the development of manipulative skills (e.g., self-feeding) because of quicker separation of wrist bones
Male babies
more physically active, display more of a preference for rough-and-tumble play, and show greater physical aggression by two years-old
Breastfeeding
Consensus is that it is substantially better nutritionally than bottle-feeding (i.e., formula feeding)
Best-practice recommendation: only breastmilk until six months; partial breastfeeding until at least two years
Benefits: ideal nutrients, immune system development, digestion, bonding, mother’s mental health
Breast-fed children have lower short- and long-term risk of numerous illnesses and better cognitive function and academic achievement
Breastmilk is more gentle on a child’s digestive system too- breastfeeding also releases oxytocin in children, and signs it can reduce mother’s stress and strengthen the bond
BUT, any breastfeeding is better than none.
Maternal lifestyle, breastfeeding practices, environmental factors and ethnicity can affect quality of milk
IN some cases, breastfeeding not recommended cuz of recreational and medical substances passing thru in milk
Breastfeeding → Third variable
Mothers who are older, better educated, have higher incomes, and are not single parents are more likely to initiate and maintain breast-feeding
Higher socioeconomic status is also associated with better physical health, cognitive functioning, and academic achievement
Breastfeeding is time-consuming (2hr cycle often)
Misconception that breastfeeding is always “natural” and “easy” – can actually be quite challenging
Solid foods
Healthy, full-term six-month-olds can begin to be introduced to these
Should have a wide variety by age 1 years
Helps meet increasing nutritional needs
Order: iron-fortified infant single-grain cereal ➔pureed vegetables ➔fruits ➔ meat or meat substitutes
Gradual introduction helps identify food allergies
Malnutrition
Can impair baby’s brain because of the nervous system’s rapid development— Leading cause of death for children under 5 years old
Feeding issues
Specific types:
Macronutrient malnutrition
Micronutrient malnutrition
Marasmus
Kwashiorkor
Marasmus
(Malnutrition)
A severe caloric deficit results in a weight that is less than 60% of what it should be at their age.
Many infants suffer permanent neurological damage
Parasitic infections and chronic diarrhea are common and make marasmus difficult to treat
Treatment: dietary supplementation with formula, intravenous feedings, treatment for parasites
Macronutrient malnutrition
(Malnutrition)
Results from a diet containing too few calories
Micronutrient malnutrition
(Malnutrition)
Deficiency of certain vitamins and/or minerals. Less common in Canada because of food fortification
Vitamin D added to milk eliminating childhood ricket
Iodine added to table salt eliminating goitre
Vitamin A added to low-fat milk and butter substitutes reducing vision loss and blindness
Kwashiorkor
(Malnutrition)
Results from not enough protein. Can lead to numerous health problems including permanent brain damage
Baby healthcare
Well baby care = series of routine doctor visits — Includes physical exams, immunizations, & developmental screenings
More frequent when babies are younger because development is more rapid
Immunizations
(Baby healthcare)
A critical component of well baby care — Infectious diseases were previously a leading cause of death in childhood that have now been nearly eradicated thanks to mass immunization
Canadian Immunization Guide recommends that routine immunization starts at 2 months old and continues through adolescence
Respiratory illnesses
(Baby healthcare → illnesses in the first two years)
Over 50% of infants in Canada have a respiratory illness before they turn 1
Attending daycare increases the risk by up to twice as much depending on the size
BUT keeping babies too clean can also have negative effects as they may not develop as healthy of an immune system
Ear infections
(Baby healthcare → illnesses in the first two years)
Often caused by respiratory illness. Associated with attention disorders, language deficits, and learning disabilities
Temporary impairment in hearing may negatively impact brain development in regions essential for language learning
Cuz of “use it or lose it”
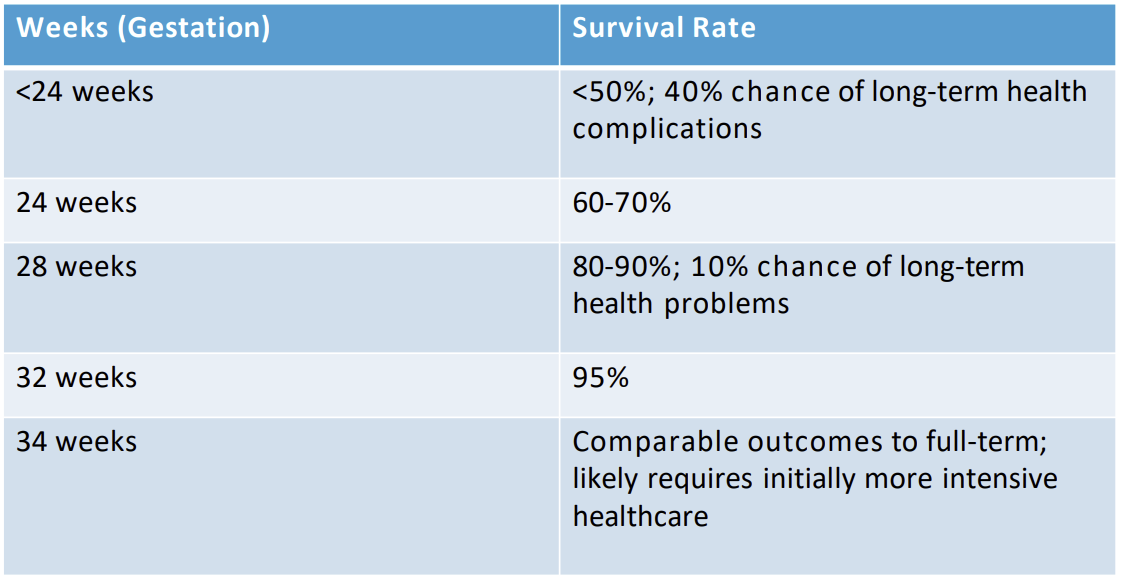
Preterm infants
Born live before 37 weeks gestation. Infants born before 32 weeks gestation may not have adaptive reflexes developed enough for survival (swallowing, sucking etc..)
Higher risk for neurological, cardiovascular, respiratory, gastrointestinal, and immunologic difficulties
Higher risk for long-term motor, cognitive, visual, hearing, behavioural, and growth problems (Kangaroo care results in more rapid development of preterm babies)
Canadian rate = ~8/100 live births
Significantly higher for multiple birth infants; however, ~80% of preterm births are singletons
24 weeks gestation is considered viability week
Low-birth-weight infants
Most, but not all, are preterm. Delay in meeting developmental milestones because maturationally younger.
If gestational age is corrected for, most timeline differences disappear
Gap disappears by age 2-to-3-years
Post-term infants
Infants born after 42 weeks gestation. Associated with higher risk of maternal medical complications and with fetal and newborn mortality
Substantial decrease in post-term deliveries in Canada – 0.3% in 2014
Decrease attributed to ultrasound dating and labour induction
Infant mortality
(In Canada)
Half occur before 4 weeks and the rest between 4 weeks and 1 year
2007 rate: ~5/1000 vs. 134/1000 in 1901 and 25/1000 in 1960s
Still not great – among comparable nations, tied with UK for second highest rate (US highest)
Lower socioeconomic status associated with higher infant morality
Particularly high rate among Indigenous people
Sudden infant death syndrome
A sudden and unexpected death of ostensibly healthy infant in first year of life. Cause of ~5% of infant deaths in Canada.
Causes are unclear but several factors that reduce risk have been identified:
Placing baby on back for sleeping
Eliminating quilts, duvets, pillows, soft toys, and crib bumpers from crib
Avoiding laying baby on soft surfaces or on loose bedding to sleep or nap
Having the baby sleep in a crib in same room as parent(s) for first 6 months
Avoiding co-sleeping
Making the home a smoke-free environment
Vision
(Sensory skills)
Newborns have poorer visual skills than older children — 5-10% of babies have some type of visual problem.
Visual assessment recommended at birth and at well baby checkups as w/o intervention, infant visual problems can lead to lifelong ones
Colour vision = about equal to adults
Visual acuity
Tracking
Visual acuity
(Sensory skills → vision)
A measure of the ability of the eye to distinguish shapes and the details of objects at a given distance.
At birth = 40x worse than average adult
8x worse by age 6 months
Adult level acuity reached by 7 years
Vision tracking
(Sensory skills → vision)
Process of following a moving object with your eyes
Inefficient at birth – can track for brief periods if target is moving slowly
By 6-10 weeks becomes quite skillful quickly
Necessary given limited motor skills
Hearing
(Sensory skills)
Can hear before birth but development continues up to adolescence
Auditory acuity
Detecting locations
Auditory acuity
(Sensory skills → hearing)
Ability to hear and distinguish sounds.
Newborn acuity comparable to adults with the exception of high-pitched sounds
Detecting locations
(Sensory skills → hearing)
Newborns can tell the general direction; however, their range of discrimination is less than an adult’s
Smelling + tasting
(Sensory skills)
As in adults, the two are intricately related. Newborns respond differentially to all five basic flavours
Appear to show preference for umami and sweet foods – may explain attraction to breast milk
Touch + motion
(Sensory skills)
Best-developed — Responsive to social touching – gentle touches on mouth, face, hands, soles of feet, and abdomen
Sensitivity to temperature – increase activity in cold room
Sensitivity to touch – becoming calmer when stroked and showing discomfort with irritants(e.g., rashes, scratchy clothes)
Study methods
(Perceptual skills)
Preference technique: baby shown two pictures/objects; time spent looking at each one measured
Habituation and dishabituation:
Present sight/sound/object over and over until baby stops displaying interest (habituation)
Present different stimulus and assess whether baby shows renewed interest (dishabituation)
Operant conditioning: use reinforcement to teach learned response to stimulus then change the stimulus
Looking
(Perceptual skills)
Visual stimulation is important for subsequent development of visual perception —Critical periods in infancy and childhood where a specific quality of visual stimulation is required for the development of normal visual perception
Introduction of visual inputs undetectable to infants can set the foundation for development of that perceptual ability
Sleeper effects for sensitivity to mid and high narrow-striped images, face processing, and facial identity based on spacing of certain features
First two months: visual attention guided by search for meaningful patterns; motion can also capture attention
2-3 months: attentional shift to what (vs. where) an object is
Babies don’t have a heightened interest in faces, but do have a preference for some faces over others
Depth perception
Depth perception
(Perceptual skills → looking)
_________________ - Ability to judge the relative distance of various objects. Can gauge through three types of information: binocular cues, pictorial information/monocular cues, and kinetic cues
Not yet clear how early infants can judge depth, nor which types of cues they use
Best guess: kinetic (~3 months) ➔binocular cues (~4 months) ➔ pictorial cues (~5-7 months)
Listening
(Perceptual skills)
Babies can discriminate between speech sounds as early as 1 month old
By 6 months, can distinguish between two-syllable words
Until ~6 months, can distinguish between all sound contrasts in any language better than adults can
Newborns can distinguish and prefer their mother’s voice from another female voice
Intermodal perception
(Perceptual skills)
The ability to integrate information from multiple senses or to transfer information gained from one sense to another sense
Possible as early as 1 month old; common by 6 months old
Nativist vs. Empiricist POV
(Perceptual skills)
Nativists’ POV: most perceptual abilities are innate
Evidence for nativists’ position: many skills are present in newborns or very young infants
Empiricists’ POV: most perceptual abilities are learned
Evidence for empiricists’ position: importance of early stimulation for long-term sensory outcomes
Nature and nurture – interaction between innate and experiential factors