Endocrine disorders - The Adrenal Gland: Hypoadrenocorticism 'Addisons'
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
23 Terms
Addison’s disease (HOC) - Reduced activity of the adrenal glands
Glucocorticoids
Mineralocorticoids - electrolyte balance
Adrenal sex hormones
Dogs > cats & Females > males
Addison’s disease (HOC) - Primary
Reduced adrenal production of all hormones

Addison’s disease (HOC) - Atypical primary
Reduced production of glucocorticoids but normal electrolytes
Mineralocorticoids can be sufficient, insufficient or deficient
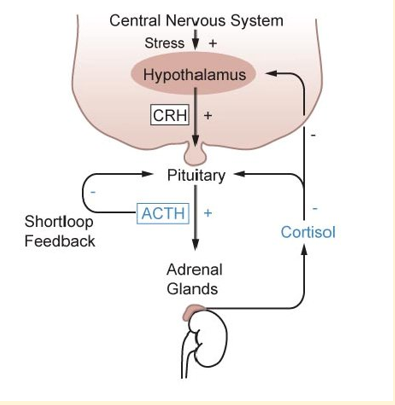
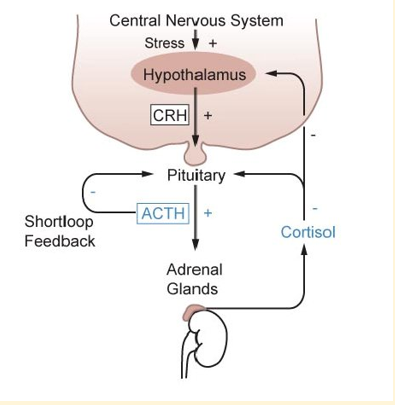
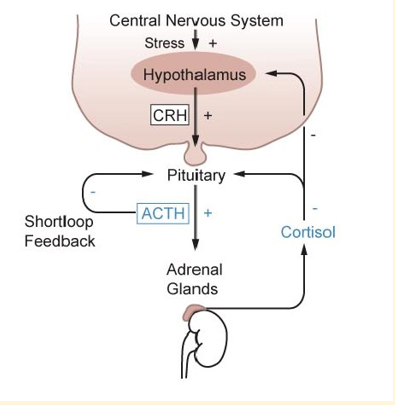
Addison’s disease (HOC) - Secondary
Reduced ACTH secretion
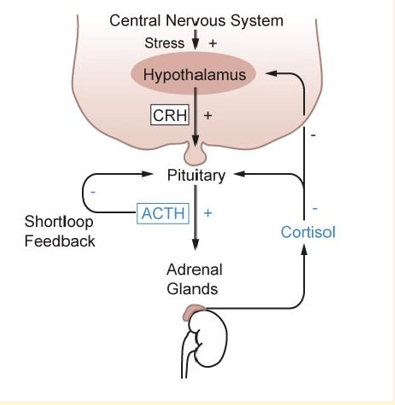
Addison’s disease (HOC) - Iatrogenic
Decreased due to exogenous steroid therapy (adrenal atrophy)
Activating the negative feedback loop by giving steroid - once steroids given then ‘iatrogenic’ can be caused
Clinical signs of 1st degree HOC - Chronic
Anorexia
Lethargy
Weakness
Vomiting
Diarrhoea
Polydipsia/polyuria
Hypotension
Bradycardia
Clinical signs of 1st degree HOC - Acute (addisonian crisis)
Medical emergency
Hypovolaemic shock
Hypotension
Collapse
Severe bradycardia
Vomiting
Diarrhoea
Diagnosis of 1st degree HOC - Haematology
Lack of stress leucogram
Diagnosis of 1st degree HOC - Biochemistry
Low sodium (hyponatremia)
Elevated potassium (hypokalaemia)
^Na:K (<25:1) - indicative
Azotaemia
Diagnosis of 1st degree HOC - ACTH stimulation test
Little or no increase in blood cortisol in response to exogenous ACTH
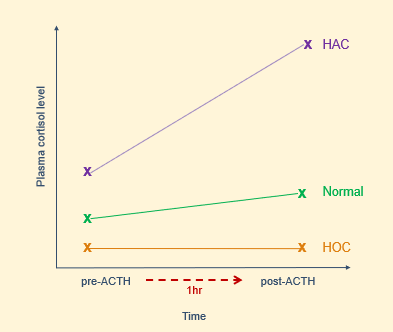
ACTH stimulation test - HOC
Low cortisol at the start, and low cortisol an hour later
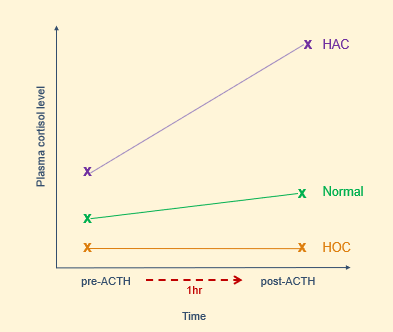
ATCH stimulation test - HOC - process
Fasted blood sample for baseline cortisol
Inject synthetic ACTH IV
Repeat cortisol blood sample 1hr later
Treatment of acute HOC
‘Addisonian crisis’
Intravenous fluid therapy
Glucocorticoids
+/- dextrose (if hypoglycaemic)
+/- sodium bicarbonate (if acidotic - care! - if correct in one direction and over-do it, it can be pushed in the other direction)
Treatment of acute HOC - Glucocorticoids
Methylprednisolone or dexamethasone IV
Hydrocortisone has both glucocorticoids and mineralocorticoid activity
Nursing care of the acute HOC patient
Likely to be recumbent initially
Monitor vital signs and clinical signs
Assist with diagnostic tests
IVFT
Administration of medication
Treatment of chronic 1st degree HOC - Mineralocorticoid
Deoxycorticosterone pivalate (Zycortal)
Subcutaneous injection
Approx 25days
Regular monitoring
Treatment of chronic 1st degree HOC - Glucocorticoid
Prednisolone (low dose)
Increase at times of stress/pre-surgery
Desoxycortone
A corticosteroid with predominantly mineralocorticoid action
Replaced the mineralocorticoid (aldosterone) = agonist
Desoxycortone - pharmacy
Administered by subcutaneous injection
Induvial variation in response with dosing interval between 20-46 days during licensing
Prednisolone
Acts like cortisol / glucocorticoid = agonist
Prednisolone - pharmacy
Variety of formulation available
generally administered in tablet form for this condition - range of tablet sizes allows for individual dose to the filtrated to suit need
80% bioavailability when administered orally
Highly plasma protein bound
Nursing care of the chronic HOC patient - if hospitalised
Reduce stress
Anaesthetic risk - often increase dose of glucocorticoids
Toileting (PU)
Water intake (PD)
Monitor closely - risk to acute-on-chronic
Nursing care of the chronic HOC patient - once home
Owner support
Long-term treatment
Regular checks
Clinical signs of deterioration
Assess with regular diagnostic tests