CALCULATING PARENTERAL FEEDINGS
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
96 Terms
PARENTERAL NUTRITION (PN) REQUIREMENTS [6]
What is the patient’s energy need? (kcal required/day)
How much protein/nitrogen does the patient need in a day?
How much fluid can the patient tolerate and need?
How much fat emulsion can the patient be given/tolerate?
How much dextrose is needed? The dextrose concentration?
Which electrolytes are needed and how much?
____ is the carbohydrate component of total parenteral nutrition (TPN)
Dextrose
TPN consists of ___, ___, and _____ which can contribute to the patient’s daily energy need differently.
protein, fat, fluid, and dextrose
Hence to know the patient’s daily energy using the TPN, the first thing you should always do is _______ in order to adjust the concentrations of the other components
compute for the total energy requirement
Equivalent calories per gram of nutrient
for every gram of carbohydrate, ____ calories
3.4
Equivalent calories per gram of nutrient
for every gram of lipids, ____ calories
9
Equivalent calories per gram of nutrient
for every gram of protein, ____ calories
4
PARENTERAL NUTRITION (PN) REQUIREMENTS
Type of micronutrients that may be needed by the patient in PN (Parenteral Nutrition)
electrolytes
Must be individualized → No one size fits all TPN solution
Standard concentrations of protein, carbohydrate, and fat that are available in standard volumes limit the degree of individualization when used
Mixing different formulas in calculated amounts can be used in developing feeding solutions for most patients
Dextrose solutions and lipid emulsions are common macronutrients used to provide energy in a parenteral solution
Nitrogen for protein synthesis is obtained from synthetic crystalline L-amino acid solutions
TOTAL PARENTERAL NUTRITION (TPN)
TOTAL PARENTERAL NUTRITION (TPN)
Nitrogen for protein synthesis is obtained from ________ solutions
synthetic crystalline L-amino acid
EQUATIONS IN DETERMINING ENERGY NEEDS [3]
HARRIS-BENEDICT EQUATION
ENERGY NEEDS BASED ON THE FOLLOWING SCALE
INDIRECT CALORIMETRY AND METABOLIC CART
DETERMINING ENERGY NEEDS
Most common formula used in the preparation of TPN or any individualized therapeutic regimen
HARRIS-BENEDICT EQUATION
HARRIS-BENEDICT EQUATION
Variables [4]
BEE: Basic Energy Expenditure or BMR: Basal Metabolic Rate
kg wt: Weight in kilograms
ht cm: Height in centimeters
age yr: Age in years
HARRIS-BENEDICT EQUATION
Refers to the variable of what your body naturally expends to function per day
BEE: Basic Energy Expenditure or BMR: Basal Metabolic Rate
To compute the total daily energy expenditure (TDEE):
result (BEE or BMR) x factor depending on the current level of activity (on a weekly basis)
HARRIS-BENEDICT EQUATION: Computing TDEE
Factors depending on the current level of activity (on a weekly basis) [5, and indicate their respective factors]
Sedentary: 1.2
Lightly active:1.375
Moderately active: 1.55
Very active: 1.725
Extra active: 1.9
(T/F)
The TDEE can also be used when you want to lose, maintain, or gain weight
T
<TDEE
Losing weight
=TDEE
Maintain weight
>TDEE
Gaining weight
Required Metabolic States for Certain Clinical Conditions
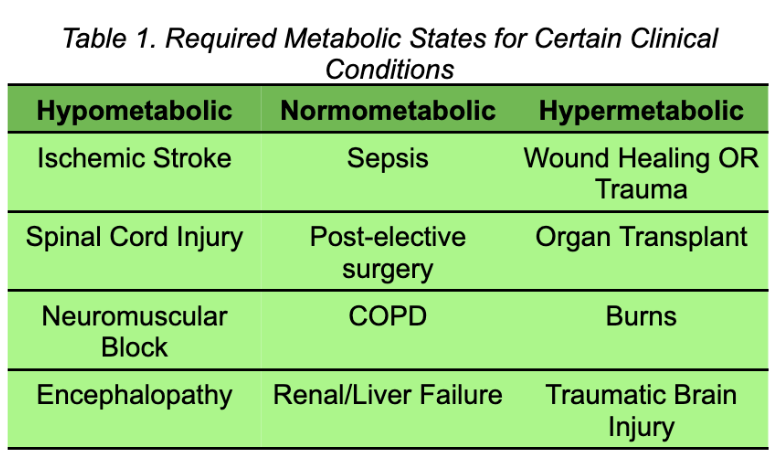
Are conditions where a patient’s metabolic rate of the patient is reduced and there is a need to regulate the caloric intake
Hypometabolic states
Are conditions where little effect are experienced by the patient’s metabolic rate and there are only minor adjustments needed to regulate the caloric intake
Normometabolic states
Are conditions where a patient would have a high BMR
Hypermetabolic states
Daily energy needs (in kcal/kg) per state (Hypometabolic, Normometabolic, Hypermetabolic)
Hypometabolic: 20-25 kcal/kg/day
Normometabolic: 25-30 kcal/kg/day
Hypermetabolic: 30-35 kcal/kg/day
During exams or activities, unless specified, when provided a range, ALWAYS UTILIZE WHAT VALUE?
THE AVERAGE OR MIDPOINT VALUE!
ENERGY NEEDS BASED ON THE FOLLOWING SCALE
for obese patients, what guidelines do we base them?
ASPEN Guidelines
FOR OBESE PATIENTS (ASPEN Guidelines)
According to the ASPEN guidelines, diet for critically obese patients
Implement high-protein, hypocaloric feeding (Low carbohydrate or calorie, high protein diet)
→ To preserve lean body mass
→ To minimize/reduce overfeeding
FOR OBESE PATIENTS (ASPEN Guidelines)
BMI for Critically obese patients
BMI: 30-50
1-14 kcal/kg/day of Actual Body Weight (ABW)
FOR OBESE PATIENTS (ASPEN Guidelines)
BMI for Morbidly obese patients
BMI: > 50
should receive 22-25 kcal/kg/day of Ideal Body Weight (IBW)
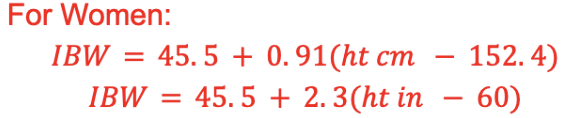
Ideal body weight formula for women (according to CDC)
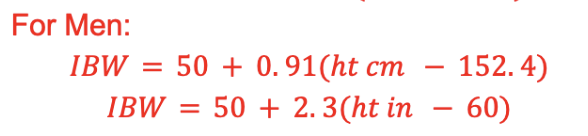
Ideal body weight formula for men (according to CDC)
FOR OBESE PATIENTS (ASPEN Guidelines)
Variables [3]
IBW: Ideal Body Weight (in kg)
ht cm: Height in centimeters
ht in: Height in inches
Patients look like they are contained inside a bubble. In it they are measuring the patient’s metabolic rate indirectly
Measures inspired and expired gas flow, volumes and concentrations of O2 and CO2
Determines energy requirements and response to nutrition over time
For patients with TPN, to be able to discuss the results of TPN, they can be subjected to devices like the one shown in the presentation. However, not all institutions are equipped with the equipment or device as it is expensive
INDIRECT CALORIMETRY AND METABOLIC CART
INDIRECT CALORIMETRY AND METABOLIC CART
Calculates [2]?
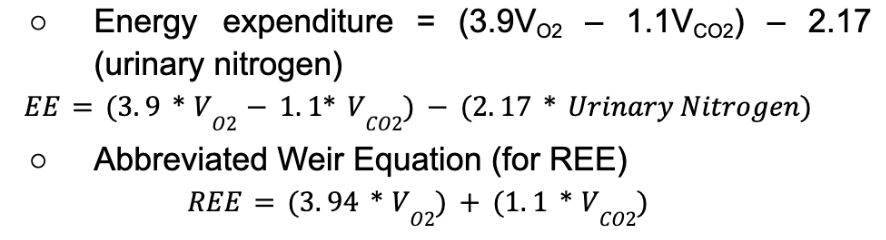
Respiratory Quotient (CO2 production/O2 consumption) and Resting Energy Expenditure (REE)
INDIRECT CALORIMETRY AND METABOLIC CART
The production of chemical energy is proportional to gas exchange
PI
→ i honestly dont know what PI means, walang nakalagay sa trans
INDIRECT CALORIMETRY AND METABOLIC CART
____ is used to calculate energy expenditure:
Weir equation
EXAMPLE:
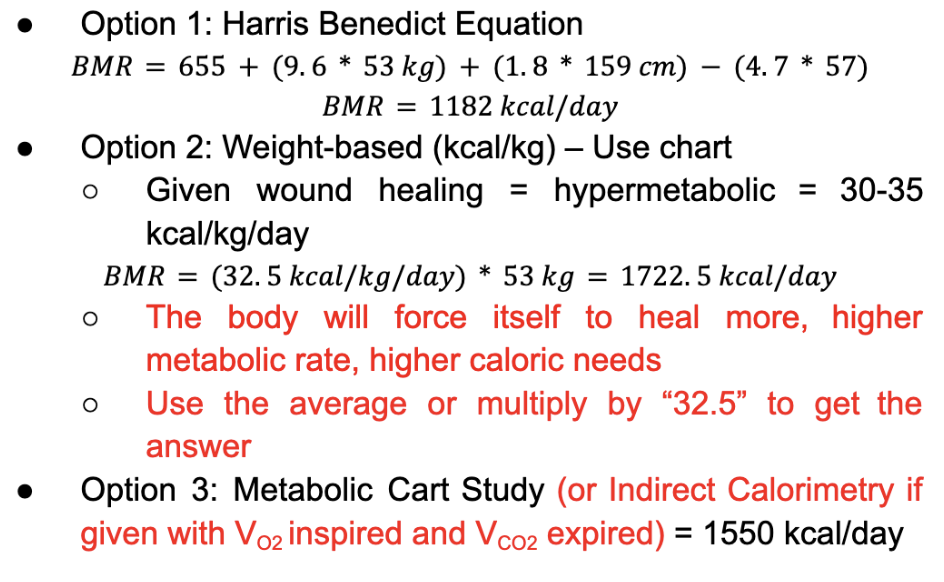
Patient 1: 57 year old female (53 kg, 159 cm) with ischemic bowel and history of physiologic short gut syndrome admitted for malnutrition. Patient has multiple decubitus ulcers/sacral wounds.
Compute using Harris Benedict Equation, Weight-based (kcal/kg) – Use chart, and Metabolic Cart Study (or Indirect Calorimetry if given with VO2 inspired and VCO2 expired)
NOTE:
→ mas gagamitin Option 1: Harris Benedict Equation, but still memorize the other 2 equations.
→ use the complete values (with exact decimals) for computation on activities
PROTEIN NEEDS
Protein is provided through?
amino acids
PROTEIN NEEDS
Protein (CHON) provides ?
4 kcal/g
PROTEIN NEEDS
Criteria/Requirements (status) - give the certain weight
Maintenance, unstressed: 0.8 – 1 g/kg
Mild stress: 1-1.2g/kg
Infections, post-Major surgeries, Cancer, Critically ill: 1.3 – 1.6 g/kg
Multiple trauma or congested heart infarction (CHI): 1.4 – 1.6 g/kg
Large wounds, Protein-losing enteropathy: 1.5 – 2 g/kg
>20% Total Body Surface Area burns: 2 – 3 g/kg
Prolonged TPN solutions should contain (how many?) amino acids. Enumerate the two.
two
Glutamine
Choline
PROTEIN NEEDS for prolonged TPN
Most abundant amino acid in the blood
Protects the gut epithelial tissue lining
Glutamine
PROTEIN NEEDS for prolonged TPN
Helps protect the liver from hepatic fat deposits (that hinder proper functioning)
Choline
FLUIDS ESTIMATION
In general, patients need a minimum of ____ to maintain hydration
30 cc fluid/kg body weight
for the range: 30-50 cc/kg
→ wherein 1 cubic centimeter (cc) = 1 mL
FLUIDS ESTIMATION
Most adults will tolerate ____ L/day of PN, comprising of water and other solutions
1.5 – 2.5 L/day of PN
Method for fluid estimation of patients
Holiday-Segar Method
Holiday-Segar Method: Daily Requirements
For pediatrics (3-10 kg)
100 ml/kg
Holiday-Segar Method: Daily Requirements
For patients with 11-20 kg
1000 mL + 50 mL/kg for each kg > 10
Holiday-Segar Method: Daily Requirements
For patients with >20 kg
1500 mL + 20 mL/kg for each kg > 20 kg
[SAMPLE PROBLEM]
Calculate the required fluid intake (RFI) for a patient weighing 17 kg.

[SAMPLE PROBLEM]
Calculate the required fluid intake (RFI) for a patient weighing 64 kg.

The amount depends on the TOTAL ENERGY needed
FAT NEEDS
FAT NEEDS
Requirement
1.0 – 2.5 g fat/kg (or 30-40% of the total calories needed)
→ Example: If you compute that the total energy needed is 2000 calories, 30-40% of the calories should come from fat and the remaining will come from carbs and protein
In TPN, CHO is given as ____
dextrose monohydrate
(T/F)
Dextrose and dextrose monohydrate have the same energy density (kcal/g).
True
Dextrose is available in 50 – 70% solutions, where in 50% solutions of _____, and 70% solutions of _____
D50W, D70W
Energy content of one liter (1000 cc) 50% Dextrose solution (D50W):


(T/F)
For diabetic patients, insulin regimens will need to be adjusted.
T
→ to keep the patient’s glucose under control
(T/F)
For diabetic patients, you must give regular insulin outside of PN.
T
(T/F)
For non-diabetic patients, there should be an increase the dextrose when glucose is >180 mg/dL.
F.
decrease of dextrose if >180 mg/dL
Determines how quickly a patient is storing/depleting the dextrose that they are being fed through the TPN
Glucose Utilization Rate (GR)
Glucose Utilization Rate (GUR) Formula

Glucose Utilization Rate (GUR) must not exceed __ mg/kg-min
4 mg/kg-min
→ fats provide calories for energy requirements; may result to overfeeding
MICRONUTRIENT NEEDS
Recommended Maximum Electrolytes: Sodium (Na)
130 mEq/L
MICRONUTRIENT NEEDS
Recommended Maximum Electrolytes:Potassium (K)
80 mEq/L
MICRONUTRIENT NEEDS
Recommended Maximum Electrolytes: Magnesium (Mg)
12-16 mEq/L
MICRONUTRIENT NEEDS
Recommended Maximum Electrolytes: Calcium (Ca)
10 mEq/L
MICRONUTRIENT NEEDS
Recommended Maximum Electrolytes: Phosphorus (P)
25 mmol/L
MICRONUTRIENT NEEDS
Trace Elements that are metabolized by the liver and should be omitted more than twice the upper limit of normal [2]
Mn & Cu
Anemia is a deficiency of what trace element?
Copper
Glucose intolerance is a deficiency of what trace element?
Chromium
Cardiomyopathy and other muscle pains is a deficiency of what trace element?
Selenium
Alopecia, dermatitis, poor wound healing and other muscle pains is a deficiency of what trace element?
Zinc
(T/F)
Add less of Zinc to the TPN for wound healing or excessive GI losses.
F. more
BIG NOTE!!
When it comes to adding or mixing ___ and ___ for preparing the TPN, there’s a limit because you want to avoid precipitation.
calcium, phosphate
→ higher likelihood of calcium turning into phosphate that is insoluble in water
OSMOLARITY (mOsm) Formula

FAT is _____ and does not contribute to Osmolarity
ISOTONIC
Hypertonic solutions may contribute to phlebitis therefore, the osmolarity of the parenteral nutrition solution should be between _________
900-1100 mOsm/L
Hypertonic solutions must be controlled (within 900-1100 mOsm/L) because?
uncontrolled solution can result to phlebitis (inflammation of the vein)
Hypertonic solutions must be administered (amount) _____ if peripheral administration
<900 mOsm/L
[SAMPLE PROBLEM]
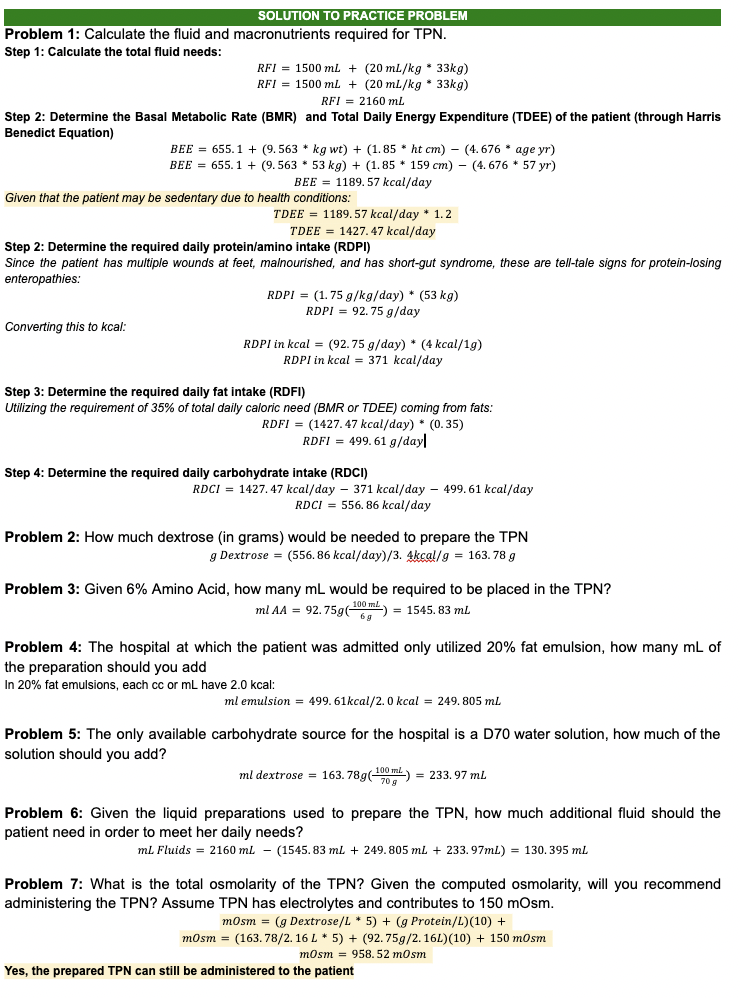
Patient 1: 57-year-old female (53 kg, 159 cm) with ischemic bowel and a history of physiologic short gut syndrome admitted for malnutrition. The patient has multiple decubitus ulcers/sacral wounds.
Calculate the fluid and macronutrients required for TPN.
How much dextrose (in grams) would be needed to prepare the TPN
Givenhttps://pmc.ncbi.nlm.nih.gov/articles/PMC6901066/ 6% Amino Acid, how many mL would be required to be placed in the TPN?
The hospital at which the patient was admitted only utilized 20% fat emulsion, how many mL of the preparation should you add
The only available carbohydrate source for the hospital is a D70 water solution, how much of the solution should you add?
Given the liquid preparations used to prepare the TPN, how much additional fluid should the patient need in order to meet her daily needs?
What is the total osmolarity of the TPN? Given the computed osmolarity, will you recommend administering the TPN? Assume TPN has electrolytes and contributes to 150 mOsm.
there are some parts na hindi alam ni leyan (these are in yellow highlight, pinic ko muna jic pinapalit)