caries interpretation
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
100 Terms
what is part of the caries assessment
pt history
clinical exam
radiographic exam
review of GV black classification
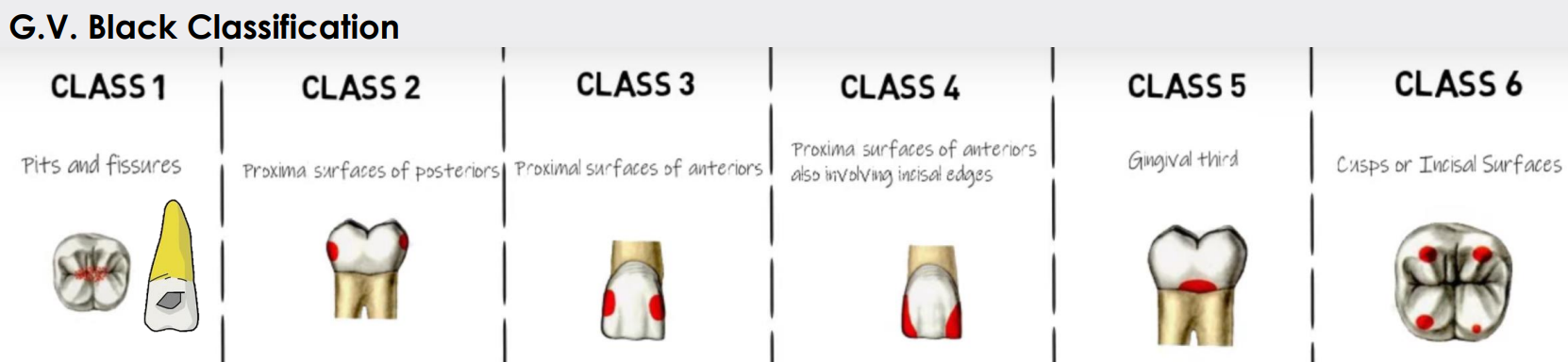
radiographs are most helpful for detecting which type of caries:
C I
CII and III
C IV
C V
CVI
CII and III (II more important)
_________can help identify CIII caries earlier
transillumination
what is the caries process and how it will eventually appear in a radiograph
demineralization → destruction → dec in density → greater x-ray penetration in carious area → radiolucency
rank PANO, CBCT, BWX, and PAs in order from highest to lowest spatial resolution
BWX
PAs
PANOs
CBCT
what is the role of BWX
to detect small interproximal caries before they can generate symptoms or become clinically visible
how should PANO be used in caries detection
caries that are visible are often large enough to be clinically apparent
should NOT rely to detect caries
how should CBCT be used in caried detection
should equivalent detection compared to intraoral modalities for NON-RESTORED teeth
should NOT use CBCT to solely detect caries
why should CBCT NOT be used for routine method of caries detection
beam-hardening and streak artifacts from metal objects are a limiting factor
inc pt dose
inc pt cost
what should be included in your radiographic evaluation
location- tooth and surfaces
depth- extent toward pulp
primary vs recurrent caries
what are primary caries
caries on an unrestored tooth surface
what are secondary caries
caries associated w an existing restoration
what are the classification systems of caries
international caries classification and management system (ICCMS)
international caries detection and assessment system (ICDAS)
ADA caries classfication system
what are the four radiographic stages of the merged ICDAS/ICCMS
sound surfaces- code 0
initial stage caries- RA
moderate stage caries- RB
extensive stage caries- RC
merged ICDAS/ICCMS code 0
no radiolucency
merged ICDAS/ICCMS RA
outer half of enamel- RA1
inner half of enamel w or w/o DEJ involvement- RA2
outer third of dentin- RA3
merged ICDAS/ICCMS RB
middle third of dentin RB4
merged ICDAS/ICCMS RC
inner third of dentin- RC5
reaches the pulp- RC6
we can reliably predict when tooth surface is cavitated and dentin is heavily infected when radiographic penetration is deeper than…
the outer 1/3 of dentin
___% of radiographic lesions that extended into the outer third of dentin show cavitation
32%
___% of lesions extending into the middle third of dentin or deeper were cavitated
72%
merged ICDAS/ICCMS categories
sound- 0
initial- A
moderate- B
extensive- RC
what are the stages of the ADA caries classification
sound
initial
moderate
advanced
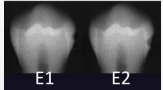
according to the ADA caries classification system, what is E1
outer ½ of enamel
according to the ADA caries classification system, what is E2
inner ½ enamel
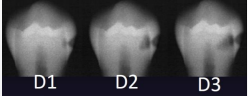
according to the ADA caries classification system, what is D1
to outer 1/3 dentin
according to the ADA caries classification system, what is D2
to middle 1/3 of dentin
according to the ADA caries classification system, what is D3
inner 1/3 of dentin
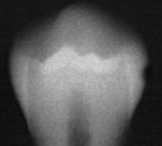
classify this according to radiographic presentation of the ADA
E1
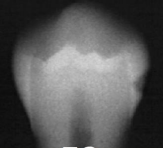
classify this according to radiographic presentation of the ADA
E2
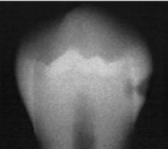
classify this according to radiographic presentation of the ADA
D1
classify this according to radiographic presentation of the ADA
D2
classify this according to radiographic presentation of the ADA
D3
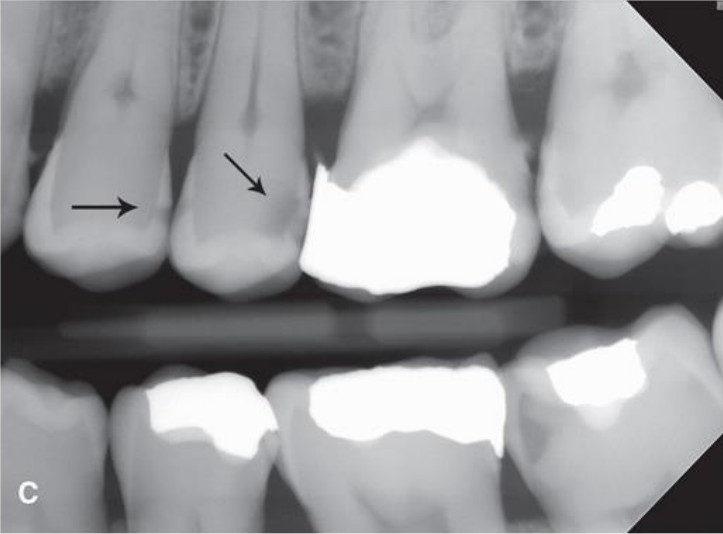
classify this lesion according to the ADA and ICDAS/ICCMS systems
caries within the outer half of the enamel: RA1, E1
classify this lesion according to the ADA and ICDAS/ICCMS systems
caries within the inner half of the enamel: RA1, E1
classify this lesion according to the ADA and ICDAS/ICCMS systems
caries within the outer 1/3 of the dentin: RA3, D1
classify this lesion according to the ADA and ICDAS/ICCMS systems
caries within the middle 1/3 of dentin: RB4, D2
classify this lesion according to the ADA and ICDAS/ICCMS systems
caries within the inner 1/3 of the dentin: RC5, D3
classify this lesion according to the ADA and ICDAS/ICCMS systems
caries in contact w pulp: RC6, D3
the decision to tx carious lesions surgically is based on what 3 things:
caries risk status of pt
depth of lesion
whether there is cavitation
when is conservative intervention indicated, be specific
when there is only involvement or the enamel or outer 1/3 of dentin- controversy
when is surgical management indicated, be specific
when the cavitation or lesion has reached the middle third of the dentin
difference in management is mostly based on … give an ex
caries risk status; higher risk would benefit from more proactive approach
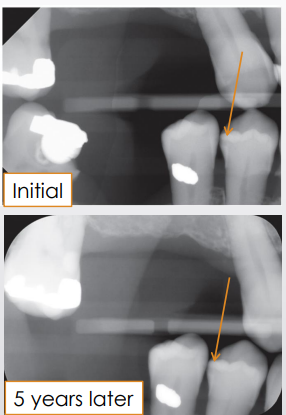
when decision is made to NOT manage the lesion surgically, what should be done to ensure proper monitoring of the lesion
follow-up period based on pts caries risk
new images should be as similar as possible for accurate comparison to see any progression
what is the susceptible zone
in proximal caries, is between the contact point of the teeth and gingival margins
what are incipient caries
caries DO NOT extend to DEJ; most often defined at extending ½ through enamel
what is the shape of incipient proximal caries
triangle w broad base at outer surface
why are incipient caries the shape that they are
demineralization occurs along long axes of enamel rods- oriented 90 degrees to enamel surface
what are primary caries
involves DEJ or extends through
what happens to the shape of primary caries once it reaches the DEJ
triangular shape gets lost, lesion gets bigger due to curvilinear or “s-shaped” arrangement of dentin tubules
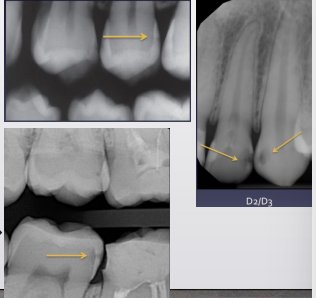

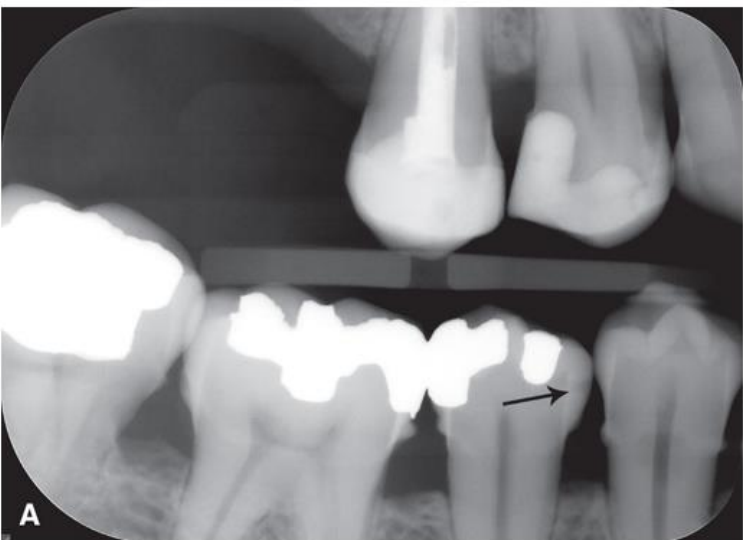
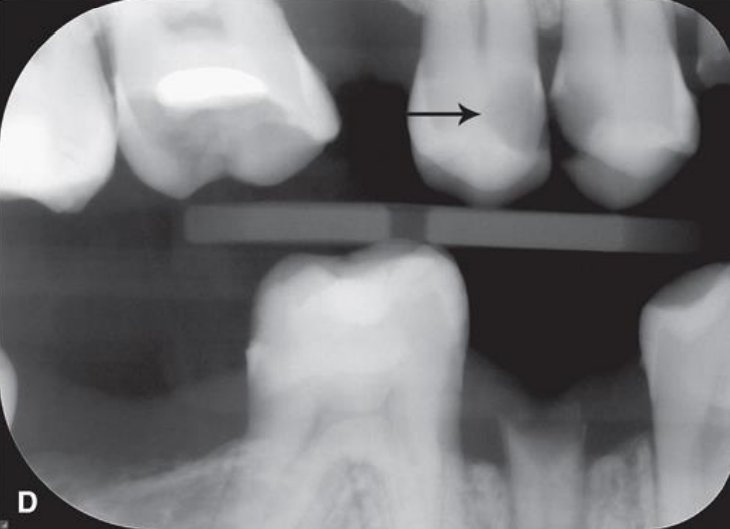
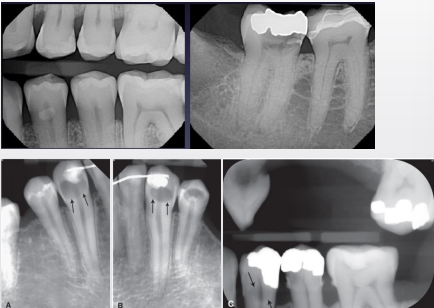
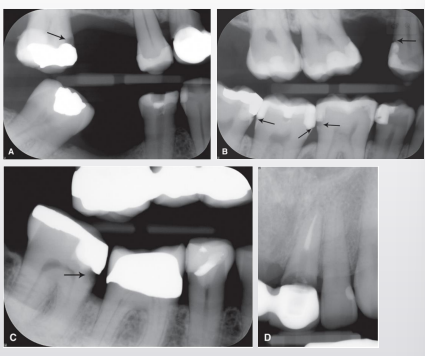
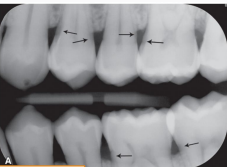
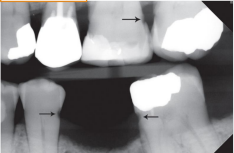
top arrow, classify this lesion based on the ADA caries classification system
D1

bottom arrow, classify this lesion based on the ADA caries classification system
D2

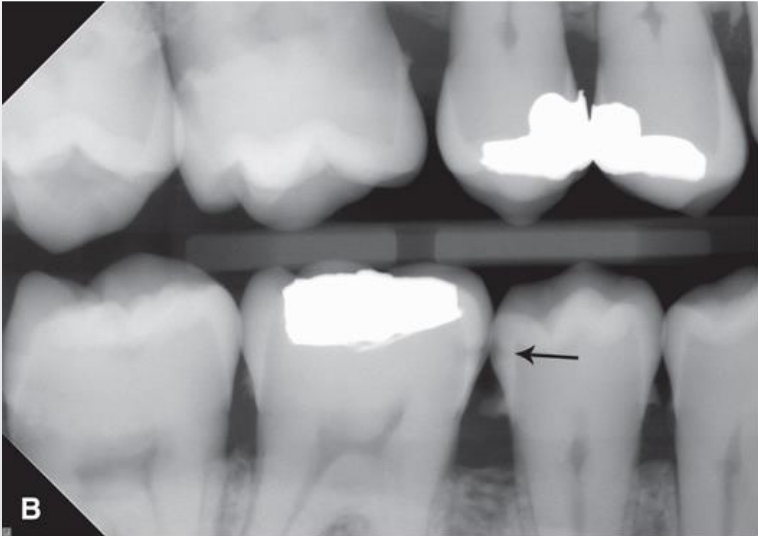
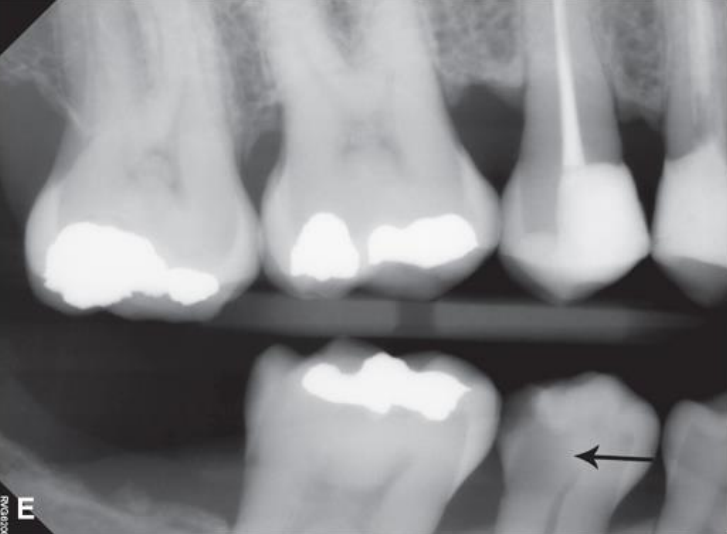
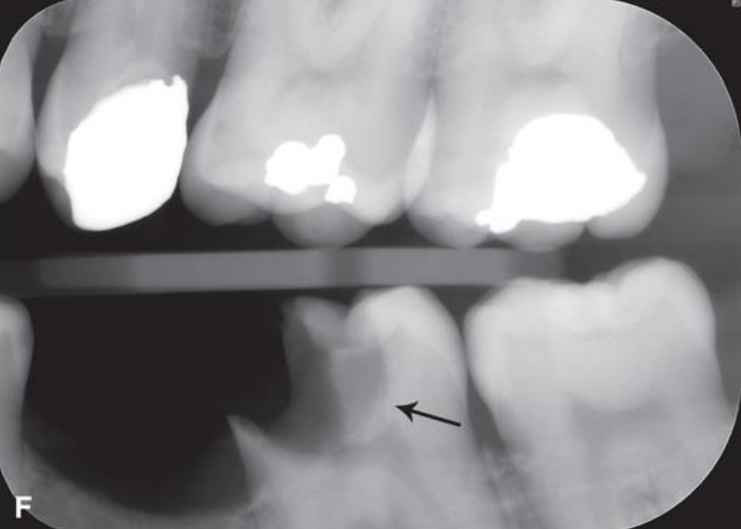
classify this lesion based on the ADA caries classification system
D3
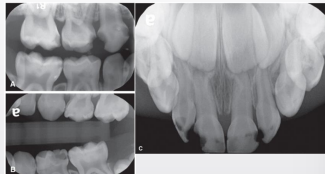
why is it important to monitor caries in primary dentition
primary teeth have thinner enamel
dentin is reached more quickly
more rapid progression of caries
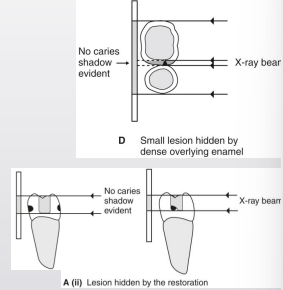
how can occlusal caries be read in radiographs
large lesions are easily observed
not very effective at detecting small lesions- nearly impossible to identify enamel-only lesions
what shape are occlusal lesions if they can be seen in a radiograph
thin line, triangle, or cup-shaped zone under enamel w base at DEJ

what type of radiograph would it be easier to identify occlusal caries; why
PANO- angle of the beam
why is the clinical exam important when identifying occlusal caries
high false negative rate in 2D radiographs
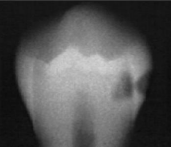
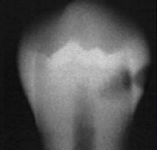
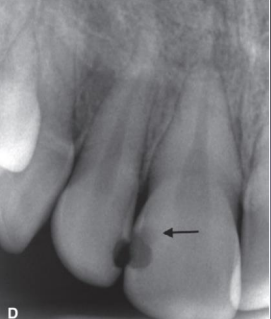
where do buccal and lingual caries typically arise
in cervical region, pits, or fissures
how do buccal and lingual caries show up in a radiograph
well-defined ovoid radiolucency
buccal/lingual caries may often be confused w occlusal caries due to superimposition, how can you sort of differentiate them
occlusal usually not as well-defined (pic shows B/L caries)
how can you tell solely based on the radiograph whether the pt has a buccal or lingual caries
SLOB rule!!
where do root caries typically arise
pt w gingival recession and/or bone loss, on B/L/proximal root surfaces of teeth involving cementum
shape of root caries on radiographs
saucer like irregular cavitation
root caries on radiographs can often be confused w…
cervical burnout
what are rampant caries
rapid progression w severe widespread involvement
would group of people are rampant caries most often seen in
young children- poor hygiene and dietary habits
pts w xerostomia- often secondary to head/neck radiation therapy
what are radiation caries
seen on surfaces and teeth that do not usually present carious- often cervical location
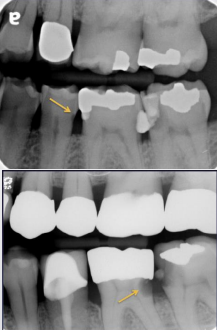
how can secondary/recurrent caries occur
can be caused by defective restoration and/or ineffective hygiene
what is the best imaging modality to use for recurrent/secondary caries, and why
BWX due to beam angulation
what are residual caries
represent areas of demineralization that remain when the original lesion has not completely removed
old composite restorations can look radiolucent on radiographs, how can you tell the difference between the restoration and recurrent caries
composite will be well-defined, caries are more diffused
what are limitations and pitfalls of 2D radiographs
false positives
cervical burnout
mach band affect
radiographic vs clinical depth
caries activity impact of angulation and superimposition
what are false positives
when a carious lesion is thought to be detected on image but tooth structure is actually intact
what is the most common source of false-positives
misinterpretation of cervical burnout
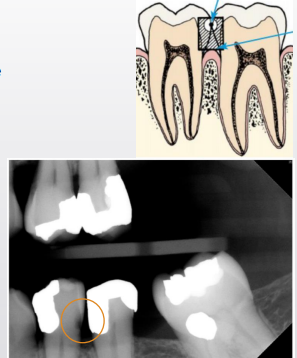
what is cervical burnout
artifact that can mimic caries commonly at or just apical to CEJ near alveolar crest
what is the cause of cervical burnout
x-rays passing tangentially through proximal area encounter less structure; shallow depression/concavity on M/D root surface can make area appear more radiolucent
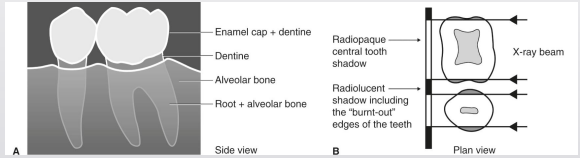
when thinking of cervical burnout, thinner tooth structures absorbs fewer x-rays, so it will appear more ________________ (radiopaque/radiolucent) on the radiograph
radiolucent
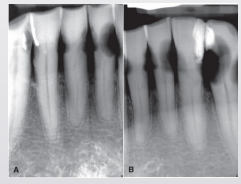
caries or cervical burn out
burnout
caries or cervical burnout
caries
what is the mach band effect
artifact caused by differential contrast between more opaque enamel and less opaque dentin → results in perception of a radiolucent band in the superficial dentin adjacent to DEJ

what causes the mach band effect
optical illusion from differential stimulation and inhibition of neighboring receptors into retina
retinal receptors overstimulated by enamel opacity inhibit adjacent receptors that perceive more radiolucent dentin
how can you overcome the mach-band effect
mask the more radiopaque enamel
if the radiolucent band disappears, not caries
if continues to be seen, caries
how can depth be a limitation to radiographic caries detection
caries are further advanced clinically than radiographs indicate
why can you not trust x-rays when evaluating the depth of the lesion
bacterial penetration of dentinal tubules and early demineralization do not produce enough change in density to affect x-ray attenuation
it is estimated that enamel demineralization must be _______% before a lesion can be observed on an image
>~35%
demineralization detected on an image does not equate to ________ carious lesions
active (can represent older, inactive/arrested lesion)
how is remineralization possible in early lesions
due to contact w calcium and phosphorus in saliva
what is required to differentiate active from arrested caries
a second image
the degree of radiolucency determined by the caries extent in what direction
the buccolingual plane

how is superimposition a limitation of 2D imaging
caries depth relative to the pulp; may appear the pulp is involved when it is not
tooth w a broad contact does NOT show caries as well as a greater density tooth structure surround caries
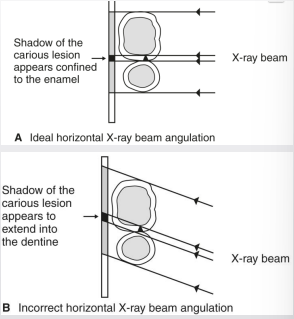
how is horizontal angulation a limitation of 2D imaging
change in angulation impacts ability to detect and stage carious lesions
what is horizontal angulation
contact overlap can obscure lesion and DEJ
changes of lesions relative to other structures→ DEJ and pulp
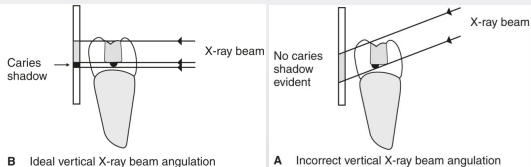
why is too much vertical angulation not a good thing
if looking at restorations particularly, if the angle is big → decay will be hidden under restoration
what should be on your differential dx for radiographs for detecting caries
unfilled cavity restoration
radiolucent restorations
cervical burnout
mach band effect
idiopatchis cervical resoprtion
dental anaomalies
tooth wear abfraction
can cervical burnout extend below the level of the bone
no, only caries
what is idiopathic cervical resorption
type of external resorption
describe how tooth wear can be seen in a radiograph
physiologic (attrition) or non-physiologic (abrasion/erosion) wear will result in low-density areas that may mimic caries
what is an abfraction
non-carious cervical lesions