A-Level AQA Psychology - Psychopathology
1/164
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
165 Terms
What is psychopathology?
The study of mental disorders in terms of their causes, development, course, classification, and treatment
What are the 4 definitions of abnormality?
Statistical infrequency.
Deviation from social norms.
Failure to function adequately.
Deviation from ideal mental health.
What is statistical infrequency?
Occurs when an individual has a less common characteristic, for example being more depressed or less intelligent than most of the population.
Why is statistical infrequency a mathematical method of defining abnormality?
Behaviour that is numerically rare/uncommon would fit this definition
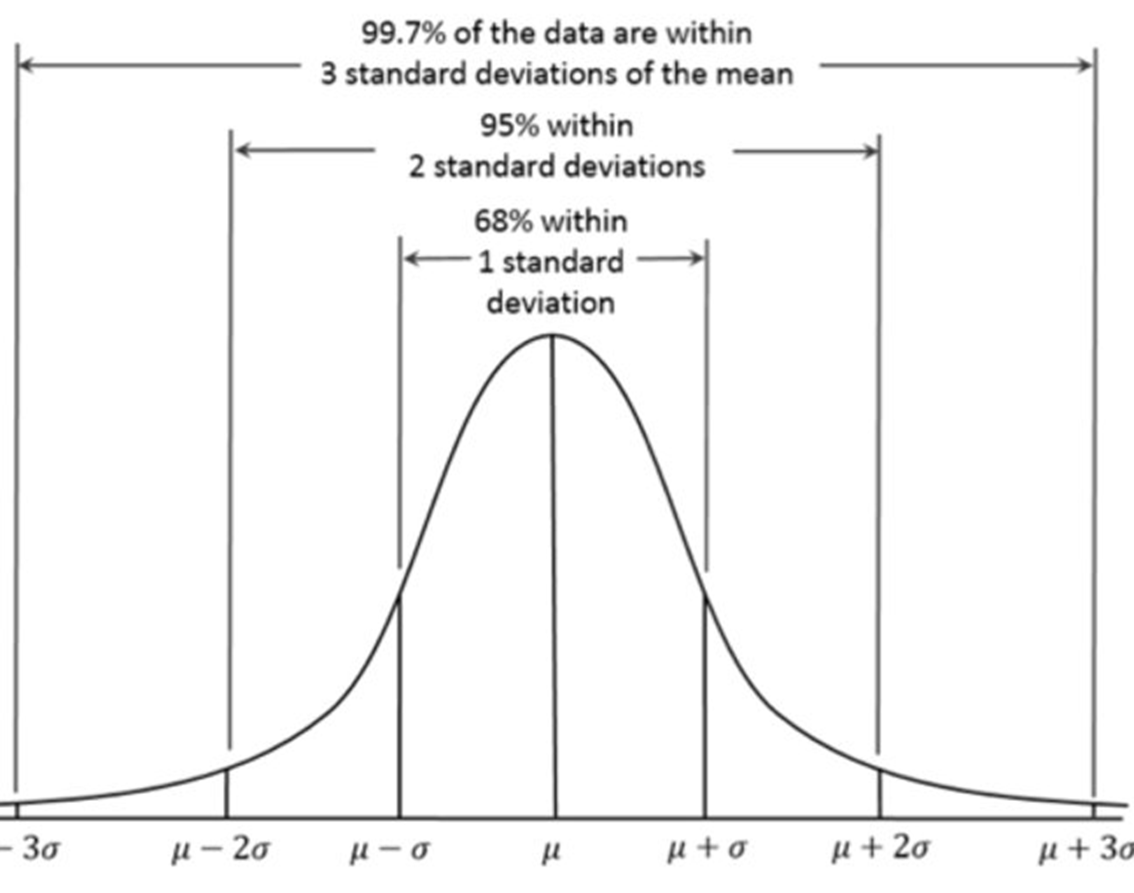
Human attributes fall into a normal distribution within the population
There is therefore a mean, with the population distributed symmetrically below and above it
Standard deviation used as the measure
Occupies the extreme ends of a normal distribution curve
Based on the quantity of behaviour measured in standard deviations from the mean (rather than quality)
What is an example of statistical infrequency?
IQ and intellectual disability disorder.
Why are IQ and intellectual disability disorder an example of abnormality in statistical infrequency?
The mean IQ is 100
The SD of IQ is 15
So, 68% of the population will score between 85-115
Scores below 70 and above 130 are therefore abnormal (top and bottom 2.5%)
Those individuals that score <70 are likely to be diagnosed with intellectual disability disorder
What is a strength of statistical infrequency? Real-world application.
P: One strength of statistical infrequency is its usefulness.
EE: Useful for Diagnosis e.g. intellectual disability disorder requires an IQ of below 70 (bottom 2%). The BDI (Beck Depression Inventory) uses statistical infrequency as a clinical diagnosis tool: a score of 30+ (top 5% of respondents) indicates severe depression.
L: This shows its value as part of clinical assessments
What is a limitation of statistical infrequency? Unusual can be positive.
P: One limitation of statistical infrequency is that infrequent characteristics can be positive as well as negative.
EE: For every person with an IQ below 70, there is a person with an IQ above 130. However, we would not think of someone with a high IQ as abnormal. Similarly, we would not think of someone with a very low depression score on the BDI as abnormal. These examples show that being unusual or at one end of a psychological spectrum does not necessarily make someone abnormal.
L: This subjective cut-off point means that S.I should not be used ALONE to make a diagnosis.
What is deviation from social norms?
Concerns behaviour that is different from the accepted standards of behaviour in a community or society. Dependent on cultural and societal norms and the historical context.
What is an example of deviation from social norms.
A person diagnosed with APD is impulsive, aggressive, and irresponsible
DSM-5: one important symptom is a “failure to conform to lawful and culturally normative ethical behaviour“
What is a strength of deviation from social norms? real-world application.
P: One strength of deviation from social norms is its usefulness.
EE: Deviations from social norms are used in clinical practice e.g. it can be used to diagnose Antisocial personality disorder and Schizotypal due to failing to conform to culturally acceptable ethical behaviour i.e recklessness, violating rights of others, aggression. Schizotypal personality disorder: eccentric behaviour, superstitions and beliefs.
L: This shoes that the deviation from social norms criterion has value in psychiatry.
What is a limitation of deviation from social norms? cultural and situational relativism.
P: One limitation of deviation from social norms is the variability between social norms in different cultures and even different situations.
EE: Social norms are culturally specific - they can differ significantly from one generation to the next and between different ethnic, regional and socio-economic groups. In some societies, such as the Zulu for example, hallucinations and screaming in the street are regarded as normal behaviour.
Social norms also exist within a time frame, and therefore change over time. Behaviour that was once seen as abnormal may, given time, become acceptable and vice versa. For example drink driving was once considered acceptable but is now seen as socially unacceptable whereas homosexuality has gone the other way. Until 1980 homosexuality was considered a psychological disorder by the World Health Organization (WHO) but today is considered acceptable.
Social norms can also depend on the situation or context we find ourselves in. Is it normal to eat parts of a dead body? In 1972 a rugby team who survived a plane crash in the snow-capped Andes of South America found themselves without food and in sub-freezing temperatures for 72 days. In order to survive they ate the bodies of those who had died in the crash.
L: It is therefore difficult to determine universal signs of illness
What is failure to function adequately?
Occurs when someone is unable to cope with ordinary demands of day-to-day living.
What 3 additional signs did Rosenhan and Seligman (1989) propose to determine when someone is not coping?
Failure to follow interpersonal rules (eye contact/personal space)
Experience of severe personal distress & to others
A person's behaviour becomes irrational/ dangerous
What is an example of failure to function adequately?
Intellectual disability disorder.
Why is intellectual disability disorder an example of failure to function adequately?
A diagnosis would not be made on this basis only- an individual must also fail to function adequately for a diagnosis.
What is a strength of failure to function adequately? threshold for professional help.
P: One strength of failure to function criterion is that it represents a sensible threshold for when people need professional help.
EE: Most of us have symptoms of mental disorder to some degree at some time. In fact, according to the mental health charity Mind, around 25% of people in the UK will experience a mental health problem in any given year. However, many people press on in the face of fairly severe symptoms. It tends to be at the point that we cease to function adequately that people seek professional help or are noticed and referred for help by others.
L: This is positive as it recognizes the patient’s experience as important in defining abnormality. It can use more objective measures too eg. poor attendance data at school/work
C/A: However, some people appear to function perfectly normally despite being seriously ill/disturbed. It is still a subjective judgment as to whether they need help.
What is a limitation of failing to function adequately? Discrimination and social controls.
P: One limitation of failure to function is that it is easy to label non-standard lifestyle choices as abnormal.
EE: In practice it can be very hard to say when someone is really failing to function and when they have simply chosen to deviate from social norms. Failing to function adequately (FFA) can be a normal reaction to events like bereavement or context-dependent, such as hunger strikes being a form of protest. Similarly, failure to keep a job might reflect economic factors rather than psychopathology.
L: This means that people who make unusual choices are at risk of being labelled abnormal and their freedom of choice may be restricted.
What is deviation from ideal mental health?
Occurs when someone does not meet a set of criteria for good mental health.
What 8 symptoms does Jahoda (1958) suggest means we are in good mental health?
We have no symptoms or distress.
We are rational and can perceive ourselves accurately.
We self-actualise.
We can cope with stress.
We have a realistic view of the world.
We have good self-esteem and lack guilt.
We are independent of other people.
We can successfully work, love and enjoy our leisure.
What is a strength of deviation from ideal mental health? Comprehensive definition.
P: Offers a positive and holistic approach to diagnosis
EE: Jahoda's criteria offers a comprehensive definition as it includes a range of criteria that can be used to distinguish mental health from illness. An individual's mental health can be discussed with a range of professionals who might take different theoretical views.
L: This suggests that IMH provides an all-inclusive checklist which we can use to assess ourselves and others from.
C/A: Very high standards- it is very difficult to attain all the criteria for mental health, and probably none of us achieve all standards at the same time or keep them for very long (e.g. only 1-2% of population self-actualize)
What is a limitation of deviation from ideal mental health? Culture-bound.
P: One limitation of the ideal mental health criterion is that its different elements are not equally applicable across a range of cultures.
EE: Some of Jahoda's criteria are rooted in Western individualist values, such as self-actualisation. This may be the end-goal for individualist cultures but not for collectivist cultures. Success and well-being is defined differently in different cultures.
L: This makes it difficult to apply the concept of ideal mental health universally, as its different elements are not equally applicable to all cultures.
What are the DSM-V categories of phobia?
All phobias are characterised by excessive fear and anxiety
Can be triggered by an object, place or situation
Fear is disproportionate to the phobic stimulus
What 3 categories has the DSM-5 classified phobias into?
Specific phobia.
Social anxiety (social phobia).
Agoraphobia.
What is specific phobia?
Phobia of an object, such as an animal or body part, or a situation such as flying or having an injection.
What is social anxiety (social phobia)?
Phobia of a social situation such as public speaking or using a public toilet. (social interactions).
What is agoraphobia?
Phobia of being outside or in a public place. (being in an unfamiliar, embarrassing or unescapable situation)
What are the 3 characteristics of phobias?
Behavioural.
Emotional.
Cognitive.
What are 3 behavioural characteristics of phobias?
Panic.
Avoidance.
Endurance.
What is panic?
Response to phobic stimulus
Adult responses: fleeing, crying, screaming
Children responses: clinging, freezing, tantrum
What is avoidance (flight)?
E.g., those who fear public toilets will limit the time spent outside to limit the chances of them having to use the toilet. This impacts their social, educational, and work life – aka negative reinforcement
What is endurance (fight)?
Choosing to remain in the presence of the phobic stimulus
E.g., arachnophobia- a person might choose to stay in the room with the spider and keep a wary eye
What are 3 emotional characteristics of phobias?
Anxiety.
Fear.
Emotional response is unreasonable.
What is anxiety?
Phobias are classed as anxiety disorders.
This involves an unpleasant state of high arousal which makes it difficult for the person to experience any positive emotions.
What is fear?
The immediate and extremely unpleasant response when we experience or think about the phobic stimulus.
What is emotional response is unreasonable?
The anxiety or fear is much greater than 'normal' and disproportionate to any threat posed.
What are 3 cognitive characteristics of phobias?
Selective attention to the phobic stimulus.
Irrational beliefs.
Cognitive distortions.
What is selective attention to phobic stimulus?
Hard to look away.
What are irrational beliefs?
Particularly salient with social phobias
Increases pressure in the phobic situation
What are cognitive distortions?
Inaccurate and unrealistic
E.g. someone with ophidophobia may see snakes as alien and aggressive-looking
What is depression?
A mental disorder characterised by low mood and low energy levels.
What are the 4 categories of depression and depressive disorders in the DSM-5?
Major depressive disorder.
Persistent depressive disorder.
Disruptive mood dysregulation disorder.
Premenstrual dysphoric disorder.
What is major depressive disorder?
Severe but often short-term depression.
What is persistent depressive disorder?
Long-term or recurring depression, including sustained major depression and what used to be called dysthymia.
What is disruptive mood dysregulation disorder?
Childhood temper tantrums.
What is premenstrual dysphoric disorder?
Disruption to mood prior to and/or during menstruation.
What are 4 behavioural characteristics of depression?
Activity levels.
Sleep disturbance.
Changes in appetite.
Aggression and self-harm.
Why is activity levels a behavioural characteristic of depression?
Typically reduced levels (lethargy): knock-on effect on the social and work life. In extreme cases a person cannot get out of bed
Psychomotor agitation
Why is sleep disturbance a behavioural characteristic of depression?
Sleeping significantly more (hypersomnia) or insomnia.
Why are changes in appetite a behavioural characteristic?
Significant weight changes
Eating less and losing weight OR eating more and gaining weight
What are 3 emotional characteristics of depression?
Lowered mood.
Anger.
Lowered self esteem.
Why is lowered mood an emotional characteristic?
“sadness” often used to describe the emotional state of depression BUT
Terms such as “worthless” or “empty” are often used by people with depression
Feelings of worthlessness
Why is anger an emotional characteristic of depression?
Feeling of negative emotion not limited to sadness
Also frequently experience anger or extreme anger: towards the self and others
Emotional characteristic BUT also behavioural (previous slide) as it can lead to harm
Why is lowered self-esteem an emotional characteristic of depression?
Emotional experience of how much we like ourselves
Can be quite extreme, with some people describing a sense of self-loathing (self-hate)
What are 3 cognitive characteristics of depression?
Poor concentration.
Attending to and dwell on the negative.
Absolutist thinking (black and white thinking).
Why is poor concentration a cognitive characteristic of depression?
Difficult to maintain attention.
Slower at responding to, or making decisions: can interfere with work.
Why is attending to and dwelling on the negative a cognitive characteristic of depression?
Paying more attention to negative aspects and ignoring the positives
Bias towards recalling unhappy events- the opposite bias to non-depressed people
Why is absolutist thinking (black and white thinking) a cognitive characteristic of depression?
Unfortunate situation can be seen as an absolute disaster.
What are 4 disorders does the DSM-5 recognise to have repetitive behaviour in common?
OCD.
Trichotillomania.
Hoarding disorder.
Excoriation disorder.
What is OCD (Obsessive Compulsive Disorder)?
A condition characterised by obsessions and/or compulsive behaviour. Obsessions are cognitive whereas compulsions are behavioural.
What is trichotillomania?
Compulsive hair-pulling.
What is hoarding disorder?
The compulsive gathering of possessions and the inability to part with anything, regardless of its value.
What is excoriation disorder?
Compulsive skin-picking.
What are 2 behavioural characteristics of OCD?
Compulsions: repetitive; reduce anxiety.
Avoidance.
Why are compulsions a behavioural characteristic of OCD?
Compulsions are repetitive
E.g. hand washing, ordering, counting, praying
Compulsions reduce anxiety
10% of sufferers have compulsions alone- no obsessions
For the majority- compulsion are attempts to manage anxiety caused by obsessions
E.g. hand washing to manage anxiety about germs, checking to see if the door is locked
Why is avoidance a behavioural characteristic of OCD?
Keeping away from triggering situations (people who wash compulsively may avoid encountering germs which can interfere with daily lives).
What are 3 emotional characteristics of OCD?
Anxiety and distress.
Accompanying depression.
Guilt and disgust.
Why is anxiety and distress an emotional characteristic of OCD?
Obsessions and compulsions accompanied by significant anxiety due to their often frightening nature. The urge to repeat a behaviour (compulsion) creates anxiety.
Why is accompanying depression an emotional characteristic of OCD?
Often accompanies the anxiety. Compulsive behaviour brings a temporary relief from anxiety
Low mood and lack of interest in activities.
Why is guilt and disgust an emotional characteristic of OCD?
Irrational guilt e.g minor moral issues (only spent £20 not £22 on brother’s bday gift)
Disgust directed against e.g. dirt, the self, etc.
What are 3 cognitive characteristics of OCD?
Obsessive thoughts.
Cognitive strategies to deal with obsessions.
Insight into excessive anxiety.
Why are obsessive thoughts a cognitive characteristic of OCD?
Unpleasant recurring thoughts (being contaminated by dirt and germs, impulses to hurt someone, etc.)
Present in 90% of sufferers
Why are cognitive strategies to deal with obsessions a cognitive characteristic?
Obsessions are a major aspect of OCD
Strategies that may appear odd to others but help to manage the OCD and distract the sufferer (obsessive guilt- excessive praying or meditating to manage anxiety)
Why is insight into excessive anxiety a cognitive characteristic of OCD?
Aware that the obsessions and compulsions are irrational (necessary for an OCD diagnosis)
Catastrophic thoughts about worst case scenarios
Hyper-vigilant & attention focused on potential hazards
What is the behavioural (behaviourist) approach?
A way of explaining behaviour in terms of what is observable and in terms of learning.
What is the 2-process model?
An explanation for the onset and persistence of disorders that create anxiety, such as phobias. The 2 processes are classical conditioning for onset and operant conditioning for persistence.
How are phobias acquired and learnt?
Classical conditioning.
How are phobias maintained?
Operant conditioning.
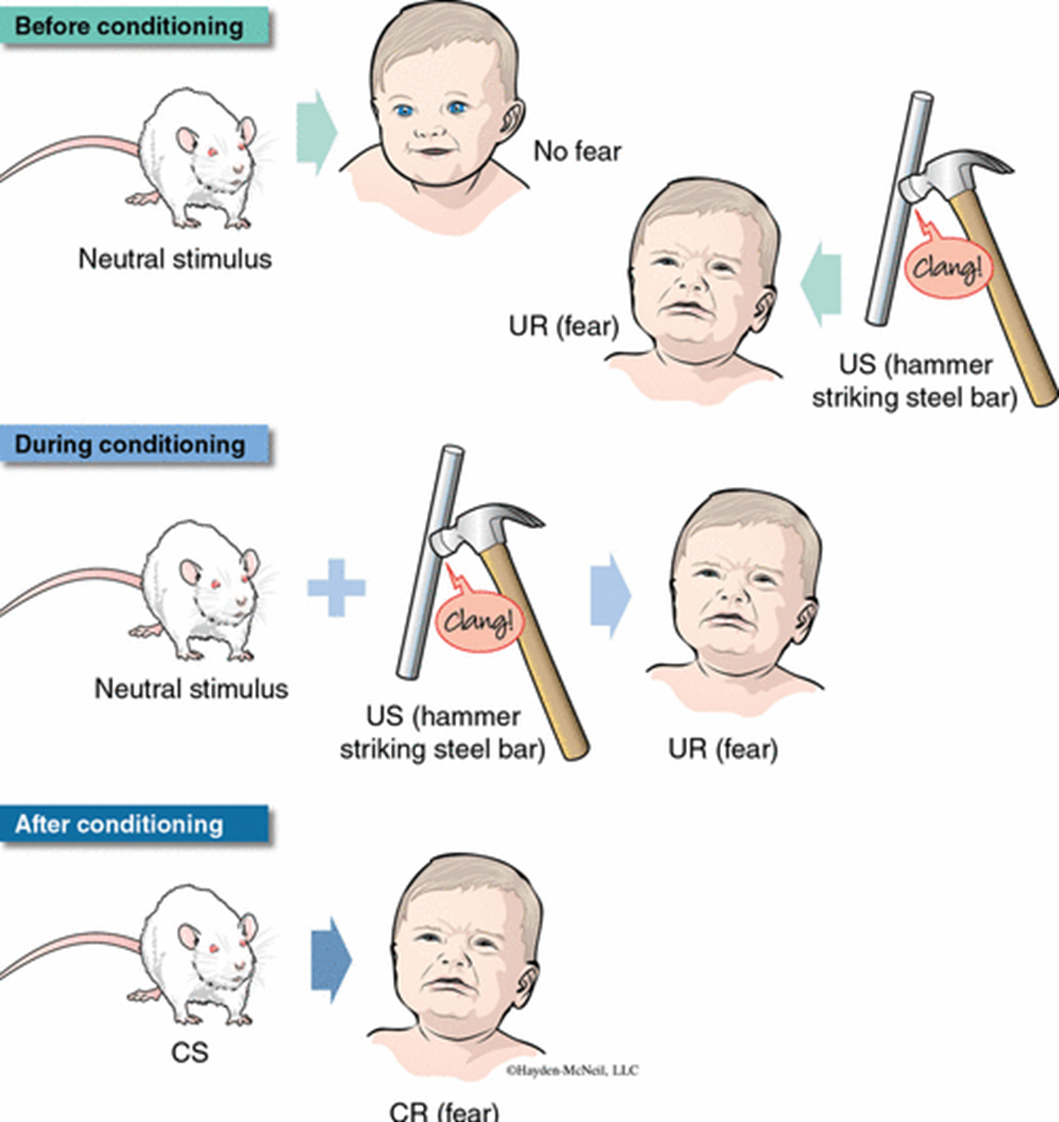
What did Watson and Rayner (1920) do?
Created a phobia of rats in a 9 month old baby: Little Albert.
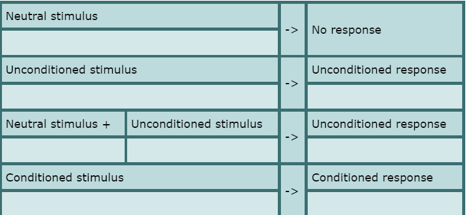
How does acquisition by classical conditioning work?
How did acquisition by classical conditioning work for Little Albert?
When does maintenance by operant conditioning take place?
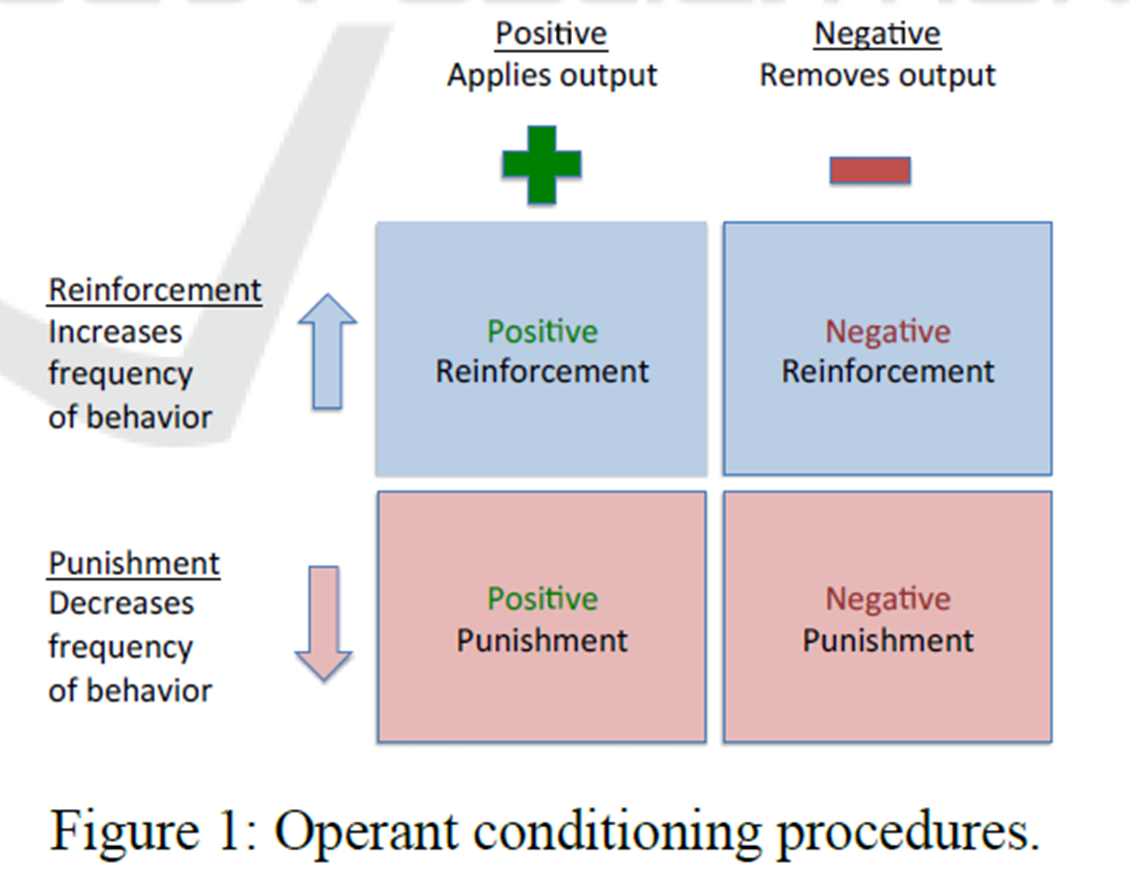
When our behaviour is reinforced or punished: reinforcement increases frequency of behaviour; punishment decreases punishment.
What are 4 operant conditioning procedures?
What is a strength of the behaviourist approach to explaining phobias? research support.
P: The 2 process model is a good explanation as there is evidence of a clear link between trauma and phobias (Research support)
EE:
The case study of Little Albert is evidence of the link b/w bad experiences and phobia; where he was classically conditioned to fear rats.
De Jongh et al. (2006): 73% of people with a fear of dental treatment (a phobia) had experienced a traumatic experience (dentistry or violent crime). This is significantly different to only 21% of people in the control group with low anxiety (no phobia) who had experienced trauma.
L: This confirms that phobias are learnt through associations (classical conditioning)
C/A P: However, learning theory cannot explain all cases of phobias (*it is environmentally deterministic).
EE: Not all phobias develop after a traumatic experience, and not all frightening experiences lead to phobias. For instance, snake phobias are found in populations where snakes are rare, and encounters with snakes are not necessarily traumatic.
L: Therefore, the association between frightening experiences and the development of phobias is not as strong as we would expect, challenging the completeness of the learning theory explanation. (*the theory overlooks the potential role of free will and individual differences in the development of phobias.)
What is a limitation of the behaviourist approach to explaining phobias? Reductionist.
P: The two-process model of phobias is an incomplete and oversimplified explanation (it is reductionist).
EE: While the model explains the behavioural aspects of phobias, such as avoidance, it does not account for cognitive factors, like irrational beliefs about the phobic stimulus. Cognitive psychologists argue that phobias may result from irrational thinking, not just learned and simple stimulus-response associations (*).
L: Therefore, it is a weak explanation as it fails to fully explain all symptoms of phobias.
What is a limitation of the behaviourist approach to explaining phobias? contrasting ideas.
P: Learning theory fails to explain why some objects or situations are more likely than others to form the basis for phobias.
EE: People are more likely to fear snakes than lambs and trees and this might be better explained by evolutionary factors. Fearing heights or snakes and avoiding them would have enhanced survival, providing an adaptive advantage. Therefore we might be genetically programmed to develop phobias of some stimuli which presented us with danger in our distant past. Seligman called this biological preparedness.
L: This suggests there is more to phobias than learning alone; it could be in our biology…
What is a strength of the behaviourist approach to explaining phobias? real-world application
P: The two-process model is a good explanation as understanding why we have phobias has allowed us to find effective treatments – it has real-world application.
EE: Exposure/behavioural therapies such as systematic desensitization & flooding have derived from the two-process model. If a phobia can be learnt (conditioning), it can be unlearnt (counter-conditioning). Mowrer’s Two-process model helps explain why people with phobias benefit from being exposed to the phobic stimulus: once the avoidance behaviour is prevented it ceases to be reinforced by the experience of anxiety reduction and so the avoidance declines and the phobia is treated.
L: This shows the value of the 2-process model – it has been useful in treating phobias.
What is systematic desensitisation?
A behavioural therapy designed to reduce an unwanted response, such as anxiety. SD involves drawing up a hierarchy of anxiety-provoking situations related to a person’s phobic stimulus, teaching the person to relax, and them exposing them to phobic situations. The person works their way through the hierarchy whilst maintaining relaxation.
What 3 processes are involved in systematic desensitisation?
The anxiety hierarchy.
Relaxation.
Exposure.
How is the anxiety hierarchy a process involved in systematic desensitisation?
Created by therapist and patient
A list of phobia-salient situations that induce anxiety, ranked from least to most frightening
How is relaxation a process involved in systematic desensitisation?
Therapist teaches patient to relax deeply: impossible to be afraid and relaxed at the same time [reciprocal inhibition]
Techniques: breathing, imagery, meditation, etc.
Sometimes medication such as Valium
How is exposure a process involved in systematic desensitisation?
Patient exposed to phobic stimulus gradually whilst in a relaxed state (3 x 45 mins sessions) (only move onto next stage once relaxed in previous stage).
Progresses according to the hierarchy (starting at the bottom)
Treatment successful= client can stay relaxed in situations high on the hierarchy
What is flooding?
A behavioural therapy in which a person with a phobia is exposed to an extreme form of a phobic stimulus in order to reduce anxiety triggered by that stimulus. This takes place across a small number of long therapy sessions.
How does flooding work?
Avoidance behaviour is not an option
The patient quickly realises the stimulus is not harmful
Extinction (classical conditioning term)
How might we explain extinction in classical conditioning terms?
When the CS (dog) is encountered without the UCS (being bitten), CS no longer leads to CR.
Exhaustion from anxiety may inadvertently lead to relaxation
Is flooding ethical?

What is a strength of systematic desensitisation? Evidence of effectiveness.
P: One strength of systematic desensitisation is the evidence base for its effectiveness.
EE: Gilroy et al. (2003) followed up 42 people who had SD for spider phobia in three 45-minute sessions. At both three and 33 months, the SD group were less fearful than a control group treated by relaxation without exposure.
L: This shows how SD is a useful and long-lasting treatment option
What is a strength of systematic desensitisation? Suitability.
P: One strength of systematic desensitisation is that it is suitable for a diverse range of patients.
EE: Unlike cognitive therapies, which require significant complex rational thought, SD is more accessible for patients with learning disabilities. Flooding, another alternative, can also be overwhelming and traumatic for some individuals. SD is generally preferred by patients, as shown by its low refusal rates (those refusing to start treatment) and low attrition rates (those dropping out of treatment).
L: This suggests that SD is often the most appropriate and preferred treatment
C/A: SD is time-consuming, when compared to alternatives such as flooding, as the person with the phobia needs to be trained in relaxation techniques and the gradual exposure can take many sessions…
What is a limitation of systematic desensitisation? effectiveness.
P: Systematic desensitisation is not effective in treating all phobias.
EE: Patients with phobias which have not developed through a personal experience (classical conditioning), such as a fear of snakes, are not effectively treated using systematic desensitisation. Some psychologists believe that certain phobias have an evolutionary survival benefit and are not the result of learning.
L: This suggests SD is ineffective in treating evolutionary phobias that have an innate basis – limiting SD’s value as a treatment.
What is a strength of flooding? cost-effective
P: One strength of flooding is it provides a cost-effective treatment for phobias.
EE: Research has suggested that flooding is equally effective as other treatments, such as systematic desensitisation (SD) and cognitive therapies, but achieves positive results much more quickly. Flooding can often work in just one session, whereas SD typically takes longer.
L: This suggests flooding can treat more people in less time.