3.1.2 - Transport In Animals Flashcards (PMT)
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
29 Terms
Why do multicellular organisms require transport systems?
Large size
Small SA:V ratio
Subsequently high metabolic rates
Demand for oxygen is high
Need a specialised system to ensure string supply to all respiring tissues
Summarise the different types of circulatory system.
Open
Blood can diffuse out of vessels (e.g. insects)
Closed
Blood confined to vessels (e.g. fish, mammals)
Single
Blood passes through heart once per circuit of the body
Double
Blood passes through heart twice per circuit of the body
Relate the structure of arteries to their function.
Thick muscular walls
To handle high pressure without tearing
Elastic tissue
Allows recoil to prevent pressure surges
Narrow lumen
To maintain pressure
Relate the structure of veins to their function.
Thin walls
Due to lower pressure
Require valves
To ensure blood doesn’t flow backwards
Have less muscular and elastic tissue
As they don’t have to control blood flow
Relate the structure of capillaries to their function.
Walls only one cell thick
Short diffusion pathway
Very narrow
Can permeate tissues
Red blood cells can lie flat against the wall
Effectively delivers oxygen to tissues
Numerous and highly branched
Providing a large SA
Relate the structure of arterioles and venules to their function.
Branch off arteries and veins
To feed blood into capillaries
Smaller than arteries and veins
So change in pressure is more gradual as blood passes through increasingly smaller vessels
What is tissue fluid?
A watery substance containing glucose, amino acids, oxygen, and other nutrients
Supplies these to the cells
Also removes any waste materials
What types of pressure influence formation of tissue fluid?
Hydrostatic pressure
Oncotic pressure
Where is hydrostatic pressure higher?
Higher at arterial end of capillary than venous end
What does oncotic pressure do?
Changes water potential of capillaries as water moves out
Induced by proteins in the plasma
How is tissue fluid formed?
As blood is pumped through increasingly smaller vessels
Hydrostatic pressure is greater than oncotic pressure
So some plasma leaks out of the gaps in the walls of the capillaries
To surround the cells of the body
Tissue fluid then exchanges substances with the cells
How does tissue fluid differ from blood and lymph?
Tissue fluid is formed from blood, but does not contain:
Red blood cells
Platelets
Various other solutes usually present in blood
After tissue fluid has bathed cells it becomes lymph
So contains less oxygen and nutrients and more waste products
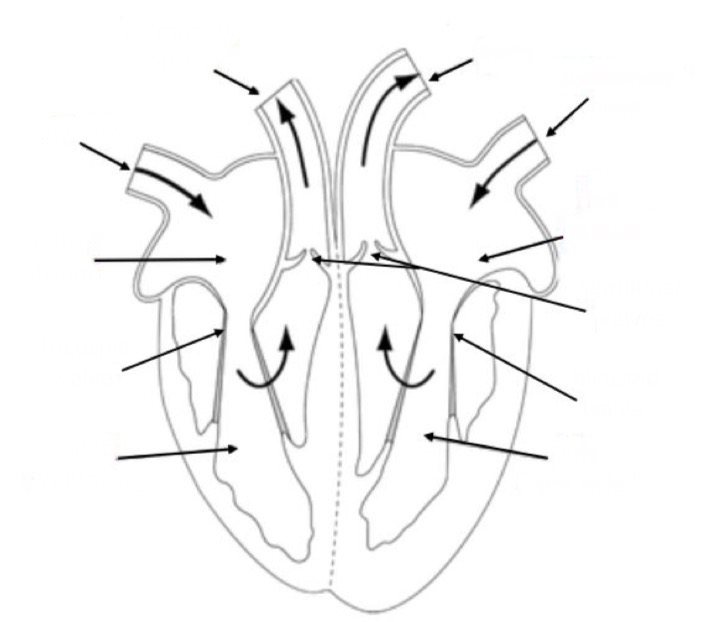
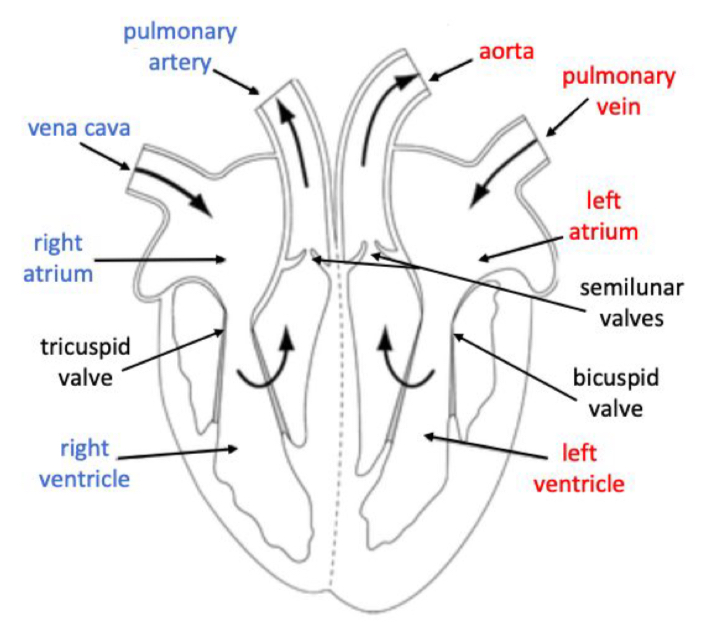
Label this diagram of the human heart.
Describe what happens during cardiac diastole.
The heart is relaxed
Blood enters the atria
Increases the pressure
Pushes open atrioventricular valves
Blood is thus allowed to flow into ventricles
Pressure in heart is lower than in the arteries
So semilunar valves remain closed
Describe what happens during atrial sytole.
The atria contact
Pushes any remaining blood into the ventricles
Describe what happens during ventricular systole.
The ventricles contract
Pressure increases
Closes the atrioventricular valves to prevent backflow
Opens the semilunar valves
Blood flows into the arteries
How do you calculate cardiac output?
Cardiac output = heart rate x stroke volume
What does myogenic mean?
The heart’s contraction is initiated within the muscle itself, rather than by nerve impulses
Explain how the heart contracts.
SAN initiates and spreads impulse across atria
Atria contract
AVN receives, delays, then conveys impulse down the bundle of His
Impulse travels into the Purkinje fibres which branch across the ventricles
Fibres contract from bottom up
What is an electrocardiogram (ECG)?
A graph showing the amount of electrical activity in the heart during the cardiac cycle
Describe types of abnormal activity that maybe seen on an ECG.
Tachycardia
Fast heartbeat (over 100 bpm)
Bradycardia
Slow heartbeat (under 60 bpm)
Fibrillation
Irregular, fast heartbeat
Ectopic
Early or extra heartbeats
Describe the role of haemoglobin.
Present in red blood cells
Oxygen molecules bind to the haem groups
Are carried around the body
Then released where needed in respiring tissues
How does partial pressure of oxygen affect oxygen-haemoglobin binding?
As partial pressure of oxygen increases, affinity of haemoglobin for oxygen increases
So oxygen binds tightly to haemoglobin
When partial pressure is low, oxygen is released from haemoglobin
What do oxyhaemoglobin dissociation curves show?
Saturation of haemoglobin with oxygen (in %)
Plotted against partial pressure if oxygen (in kPa)
Curves further to the left show the haemoglobin has a higher affinity for oxygen
Describe the Bohr effect.
As partial pressure of carbon dioxide increases, conditions become acidic
So haemoglobin changes shape
Affinity of haemoglobin for oxygen decreases
So oxygen released from haemoglobin
Explain the role of carbonic anhydrase in the Bohr effect.
Carbonic anhydrase present in red blood cells
Converts carbon dioxide to carbonic acid
Dissociates to produce H+ ions
These combine with haemoglobin to form haemoglobinic acid
Encourages oxygen to dissociate from haemoglobin
Explain the role of bicarbonate ions (HCO3-) in gas exchange.
Produced alongside carbonic acid
70% of carbon dioxide is carried in this form
In the lungs
Bicarbonate ions are converted back into carbon dioxide which we breathe out
Describe the chloride shift.
The intake of chloride ions across a red blood cell membrane
This repolarises the cells after bicarbonate ions have diffused out
How does foetal haemoglobin differ from adult haemoglobin?
Partial pressure of oxygen is low by the time it reaches the foetus
So foetal haemoglobin has for oxygen than adult
Allows both mother’s and child’s oxygen needs to be met