EKG Readings
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
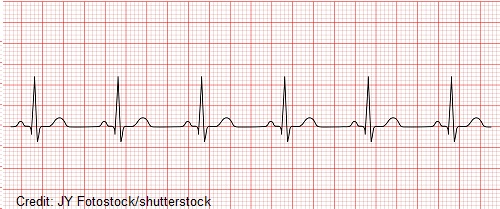
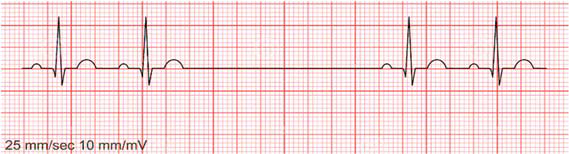
normal sinus rhythm
rate = 60-100 BPM or equivalent age-appropriate rate in children
QRS complex preceded by P wave
P waves upright in I and II, inverted in AVR
PR interval constant
QRS complexes <100 mm wide
sinus tachycardia
increased electrical impulses from SA node
heart rate >100 BPM
sinus bradycardia
rate: <60 BPM
regular rhythm
P waves upright, consistent, and normal
PR interval: 0.12-0.20 seconds
QRS complex: <0.12 seconds, consistent
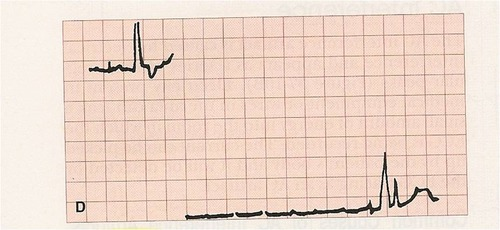
sinus arrest
sudden absence of electrical activity in SA node → no depolarization/contraction
6 second pause = medical emergency, call 911 and carry out emergency procedures
atrial flutter
narrow complex tachycardia
regular atrial activity @ ~300 BPM
loss of isoelectric baseline
sawtooth pattern and inverted at II, III, AVF

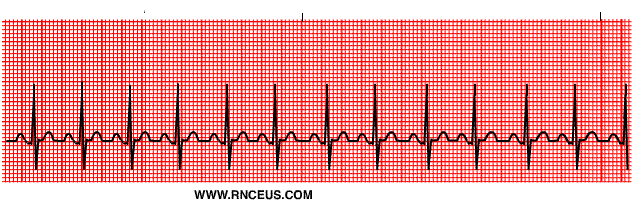
atrial fibrillation
irregular rhythm
no P waves
no isoelectric baseline
variable ventricular rate
QRS complexes usually <120 milliseconds

asystole
colloquially referred to as a flatline
complete cessation of electrical and mechanical activity in the heart

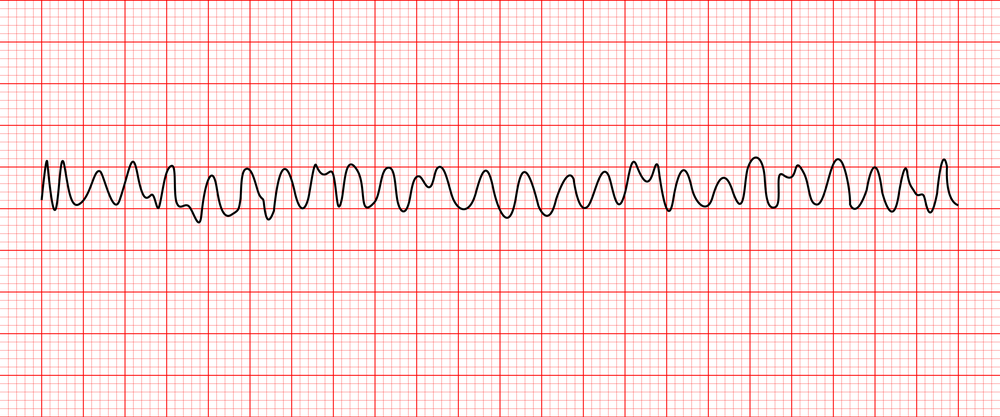
ventricular fibrillation
rate: 150-500 BPM
no identifiable waves
chaotic irregular deflections of varying amplitude
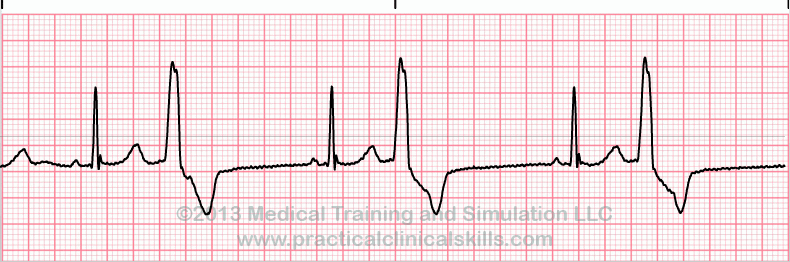
premature ventricular contraction
atrial rhythm is regular
ventricular rhythm is irregular
QRS complex is premature, wide, and/or distorted (>0.14 seconds)
premature QRS complexes occur in singles, pairs, or groups of 3
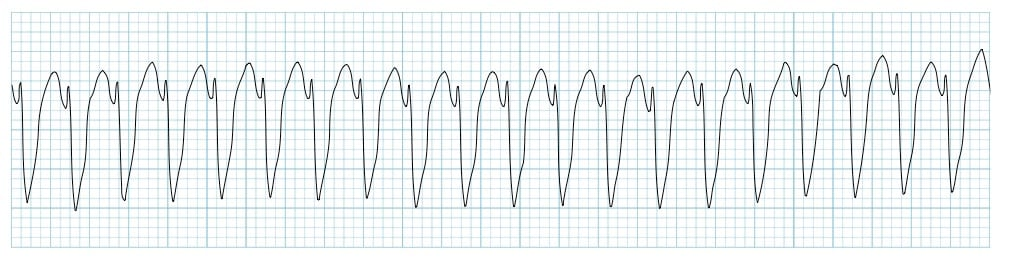
ventricular tachycardia
regular fast rhythm
large, irregular QRS complexes
P waves are either absent or random
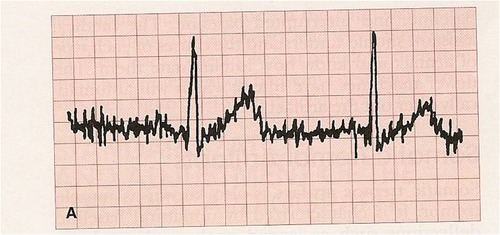
somatic tremor
caused by irregular muscle movement (Parkinson’s, shivering from cold, etc)
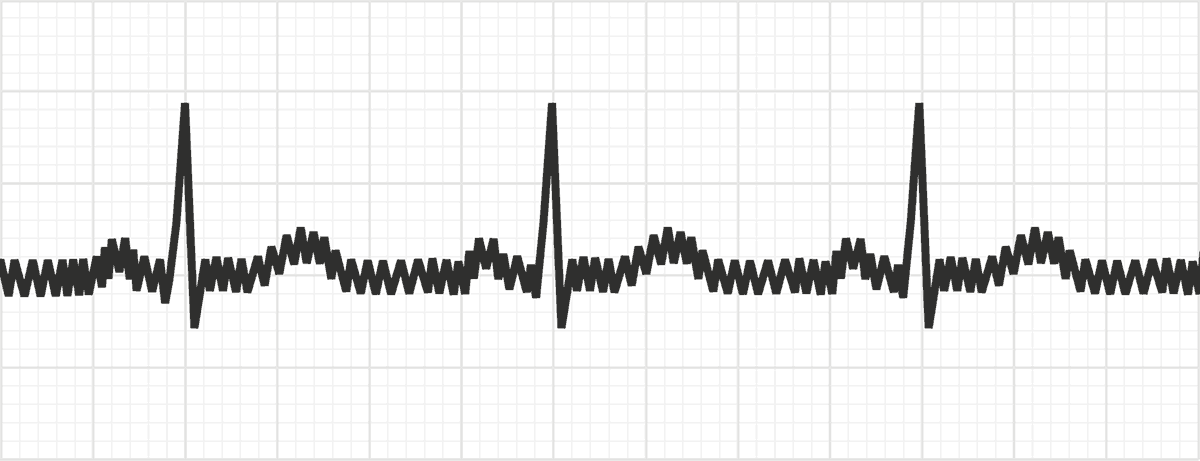
electrical/60-cycle interference
caused by poor grounding and external electricity interfering with tracing
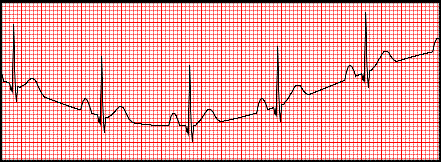
wandering baseline
caused by movement associated with unusual breathing or poor electrode connection
interrupted baseline
obvious break in the tracing
usually related to a disconnected or broken lead wire