U4 AOS 1 - Sleep
1/123
Earn XP
Description and Tags
zzz
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
124 Terms
Sleep
naturally occurring and reversible altered state of consciousness, characterised by a reduction in awareness and responsiveness to external surroundings.
Split into NREM Non rapid eye movement
N1- light sleep
N2 - deeper sleep
N3 - deep sleep
and REM rapid eye movement (dreaming)
Consciousness
Consciousness is the awareness of your own internal mental processes, including your thoughts, feelings, sensations and perceptions, and your awareness of the external world around you.
can consciousness be observed?
no, though it and psychological constructs can be supported by research evidence to qualify.
Partial Sleep Deprivation
Partial Sleep Deprivation, (PSD) is the experience of achieving INADEQUATE SLEEP IN TERMS OF QUALITY AND QUANITTY.
If question asks if someone is sleep deprived, you must take into account if they satisfied the sleep duration for their age and sleep quality
Moreover, if they have 17 hours of without sleep they are also sleep deprived
THIS IS TH EPRIMARY DEFINITION YOU FOOL, DO NOT MAKE THE SAME MISTAKE IN YOUR SACS EVER AGAIN
Full sleep deprivation and effects ABC
No sleep episode for 24 hours, effects/symptoms are more severe than partial sleep deprivation
EXAMPE,S
Affective-
Greater mood swings,
Behavioural -
Greater fatigue
Cognitive -
Poorer memory
Impairs physical wellbeing - ‘
Obesity, diabetes, heart problems, immune system collapse, death
Psychological wellbeing - hallucinations, depression,anxiety, depersonalisation
affective functioning
A persons expression and experience of their emotions
partial sleep deprivation effects on affective functioning
trouble regulating emotions
mood swings
emotional outbursts
sad or depressed
irritability
amplified emotional respomses
behavioural functioning
observable actions, usually motor skills.
partial sleep deprivation effects on behavioural functioning
daytime fatigue
sleepiness
lack of coordination adn muslce control
lack of self control
increase in REM Sleeps (when you do sleep)
cognitive functioning
Mental processes and funtioining related to that.
some impacts of partial sleep deprivation on cognitive functioning.
Reduced ability to concentrate
• Shorter attention span
• Difficulties completing problem-
solving and logic tasks
• Reduced ability to reason
•
Impaired memory
•
•
Increased difficulty completing both
simple and complex cognitive tasks
Impaired judgment
• Difficulty problem-solving
• Difficulty making decisions
psychological construct
A mental process that cannot be directly observed and measured through the collection of data.
consciousness requirements and existence
We believe consciousness exists; however, we can only indirectly measure it through qualities that are more easily assessed, such as physiological changes or observable behaviours, or through self-report methods.
Constructs however, DO need to be supported by research evidence.
normal waking consciousness
being aware of our internal and external environments we are awake and aware of regular levels of awareness in everyday activities.
altered states of consciousness
an altered state of consciousness is any state that differs in awareness from normal waking consciousness.
our levels of awareness are lower or higher than in normal waking consciousness.
natural occurring and induced
naturally occurring altered states of consciousness
Naturally occurring altered states of consciousness occur without any external influence, such as sleep or a state of fatigue.
Induced altered states of consciousness
Induced altered states of consciousness are brought about on purpose, such as an alcohol-induced state, an anaesthetised state for an operation or a meditative state.
Sleep percentages
NREM —> 80%
REM —> 20%
how many sleep cycles,
8 hours, 5 sleep cycles, 90 minutes
nrem
Non-rapid eye movement (NREM) sleep is a type of sleep characterised by a progressive decline in physiological activity.
NREM sleep consists of three distinct stages and takes up around 80% of a sleep episode in people of school age and older.
nrem 1-
Induced altered states of consciousness are brought about on purpose, such as an alcohol-induced state, an anaesthetised state for an operation or a meditative state.
It is the period when a person ‘dozes off’ to sleep and when they may most easily be woken up.
As a sleep episode progresses, a person may not experience much more time in N1.
If they are not disturbed for a couple of minutes in N1, a person quickly moves into NREM Stage 2 (N2).
NREM Stage 2 (N2)
is also considered light sleep, during which physiological responses continue to slow down.
A person still wakes relatively easily during N2; however, bursts of brain activity help resist being woken by environmental stimuli such as noises.
N2 is the stage of sleep that is experienced the most throughout a sleep episode.
NREM Stage 3 (N3)
NREM Stage 3 (N3) is considered to be deep sleep, during which physiological responses are at their slowest and a person is most difficult to wake up.
N3 is known as ‘slow-wave sleep’ due to brain activity being at its slowest.
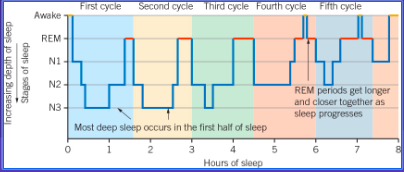
During a sleep episode, N3 is experienced more in the first half of the night than the second half of the night.
As a sleep episode progresses, a person experiences less N3 sleep, and may not experience it at all in the last one or two sleep cycles of a typical night.
It is thought that our body is repairing itself during NREM sleep.
REM rapid eye movement sleep, what is it
During rapid eye movement (REM) sleep, your eyes make quick darting movements behind their closed eyelids and your physiological activity increases.
During REM sleep, brain activity resembles wakefulness, and heart rate and breathing rate increase.
Voluntary muscles are seemingly paralysed and twitch only intermittently.
The most vivid and memorable dreams occur during REM sleep.
REM periods/durations and purposes
A period of REM occurs at the end of each sleep cycle, and these periods get longer and closer together as the sleep episode progresses, which means you have more REM in the second half of sleep than in the first half.
REM sleep also differs markedly across different ages, but typically takes up 20% of a sleep episode in people aged around 5 years and older.
If you have less sleep than normal, you may experience more REM sleep when you next sleep.
It is thought that our mind is repairing itself during REM sleep.
Hypnogram
A hypnogram is a line graph of a person’s sleep mapped over time.
A hypnogram displays the sleep architecture or patterns of a sleep episode, with a typical night’s sleep for an adult consisting of five sleep cycles featuring REM and NREM sleep.
Time x axis, stages y axis
shows a persons sleep cycles with rem sleep and three nrem stages
objective sleep measurements
can have measured evidence to support it.
Electroencephalography (EEG)
An electroencephalograph detects, amplifies and records electrical activity of the brain (brainwaves)
Non-invasive brain imaging technique that uses scalp electrodes to measure the voltage fluctuations induced by the mass electrical activity of neurons
The image it produces is an electroencephalogram
Brainwaves can be measured in both frequency (the speed - the number of brain waves per second) and amplitude (the strength - the deviation from the central point)
Brainwaves are associated with the level of alertness we experience
when frequency highest, amplitude lowest
Normal waking consciousness
Awake, alert and focused
High environmental stimulation
Brain working on several things at once
when frequency and high, amplitude low
Lower alertness
Awake but relaxed
Drowsy
Low environmental stimulation
frequency low, amplitude high,
Low alertness
Light sleep
Senses withdrawn from the external environment
Deep meditation
frequency lowest, amplitude highest
Lowest alertness
Deep N3 sleep
Dreamless sleep
Electromyography (EMG)
Detects, amplifies and records the electrical activity of the skeletal muscles
Can be used on face or body muscles
The image it produces is an electromyogram
Muscle movement/tension can be measured in both frequency (the speed) and amplitude (the strength)
In general, more muscle tension indicates greater alertness, so as a person drifts into deeper sleep, muscle movement decreases.
Additionally, no muscle movement is detected during REM sleep.
Electro-oculography (EOG)
This device detects, amplifies and records electrical activity of the muscles that allow the eye to move (it therefore only infers eye movement)
The image it produces is an electro-oculogram
‘Eye-movement’ can be measured in both frequency (the speed) and amplitude (the strength)
It is measure by placing electrodes around the eye
Activity levels of ‘eye-movements’ are associated with different stages of sleep
As you drift into deeper sleep, your eye movement decreases and slows down, and when you experience REM sleep, your eye movement increases.
Subjective sleep measurements
→ subjective descriptions of altered states of consciousness, sleeep
Sleep Diaries
Sleep diaries are often used when a person is experiencing sleep troubles (e.g sleep apnoea or insomnia) and help sleep experts understand the participant’s experience.
They are a self-reported record of an individual’s sleep & waking time activities.
Records can be kept of:
Time trying to fall asleep
Number, time and length of awakenings during sleep
How sleepy the individual feels at different times of the day
Factors that affect sleep e.g. number of caffeinated or alcoholic drinks consumed
Video monitoring
Video cameras are used to record externally observable physiological responses throughout a sleep episode
Recordings can also be shown to the participant to help them become aware of and understand their behaviour, for example, showing what they do when sleepwalking or even observing the effects of a snoring partner on their sleep.
Records may be kept of:
Changes in posture or body position
Amount of ‘tossing and turning’ restlessness
Sleep-related breathing problems (e.g. sleep apnoea)
What happens when awakening from a nightmare or night terror
Behaviour associated with sleepwalking
advantages when measuring consciousness/sleep of objective data
data is quantitative, which is easy to measure and compare.
minimal interpretations required, thus minimises bias.
more accurate and reliable data, allowing for replication.
disadvantages when measuring consciousness/sleep of objective data
can lack detail, as no insight gained as to why responses/measurements are obtained.
can be more artificial and lack external validity because measurements are taken in a laboratory.
cannot describe private and personal thoughts
advantages when measuring consciousness/sleep of subjective data
provides qualitative data, thus is more detailed.
can provide insight into mental processes that cannot be directly measured. eg. dreams.
disadvantages when measuring consciousness/sleep of subjective data
qualitative data, means it can be difficult to measure and compare.
requires personal judgements/ interpretation, meaning it is often influenced by bias
it is less valid and reliable due to bias and therefore, more difficult to replicate.
Circadian Rhythyms
Biological processes that coordinate the timing of activity of body systems over a 24 hour period
Ultraradian Rhythms
Biological processes which coordinate the timing of things less than 24 hours
Sleepin in terms of circadian and ultrradian
Wakefulness and sleep is circadian
Individual sleep stages is ultraradian
Suprachiasmatic nucleus (SCN) and influences
The suprachiasmatic nucleus (SCN) is found in the hypothalamus.
“master body clock”
influenced by external cues, known as zeitgebers, such as light, exercise, social acitivity, eating patterns and temperature.
zeitgebers
external cues influencing circadian rhythm the SCN, such as light, exercise
melatonin
the sleep hormone,more makes you drowsiness,
pineal gland
the glang producing melatonin which makes you feel drowsy
how melatonin produced
when low/no light detected by light sensitive neurons in retinas, → SCN suprachiasmatic nucleus, sends excitatory signal to pineal gland in human brain => the pineal gland releases melatonin
how melatonin inhibited
opposite of above flashcards,
detect more light → scn, sends inhibitory messages to pineal gland, inhibits release by pineal gland
SCN and melatonin levels in blood (internal stimulus)
when melatonin levels in the blood are high, the SCN signals to the pineal gland to reduce the secretion of melatonin.
negative feedback loop, stabilise body internal environment by opposing and counteracting of internal or external stimuli.
regulatory mechanism, where the output of a sytsem reduces or slows down the processes that led to that output, thus stabilizing the system.
Light Cues changing circadian rhythm
without light cues, circadian rhythm tends to run free and cycle for a little longer.
What does the total amount of sleep do across a lifespan
Decrease
Proportion of REM sleep X’a significantly from birth till 2
Decreases
Across lifespan, N3 trend and N2 trend
N3 sleep decreases, Replaced by N2 sleep
Adolescents go to sleep later, what is that called
Preference for going to sleep later
After adolescence, adult, going to sleep earlier, what called?
Circadian phase advance
Awakenings
Waking up from sleeping
Awakenings do what from adulthood to old age
Increase
Sleep efficiency
The percentage of time in bed that is spent asleep
Sleep efficiency over lifetime
Decreases
Neonatal period
0-1 month
Neonatal recommended hours and proportion of REM and NREM
14-17 hours
REM 50%
NREM 50%
Each episode lasts between 2-4 hours
Why is there a lot of sleep
Increase in amount of sleep for rapid growth development. Boost brain growth and development. , Muscle twitches in REM sleep typically immobile may be to help newborns develop their sensory motor system. 😭
infancy stage (age and rec hours and rem and nrem proportion)
2-12 months
13-15 hours,
each sleep episode, 5-8 hours
rem 35-40%
nrem 60-65%
explanation for infants,
→Infants begin to sleep for longer periods at a time as their circadian rhythm develops a more regular sleep pattern following day–night cycles.
This is due to the SCN and melatonin synchronising with a 24 hour circadian rhythm.
childhood stage
2-11 years
- 11 hours
REM 20%
NREM 80%
explanation for childhood
From the early to late childhood years, the timing of the circadian rhythm gradually delays, and sleep shifts to later in the evening.
2 - 5 years old: N3 makes up more than half of NREM sleep.
6 - 10 years old: N1 and N2 sleep increases and N3 decreases
adolescence stage
11-18 years
8 - 11 hours
(early adolescence sleep is longer)
REM 20%
NREM 80%
explanation for adolescents sleep patterns
Adolescents experience a delay in the circadian rhythm because of a hormonally determined shift in melatonin release to 1–2 hours later than other age groups. This can cause a preference for a later bedtime, resulting in fewer hours of sleep than needed because of early waking for school.
In this age group, increasing school-related requirements, increasing independence and easy access to constant entertainment and social networks also contribute to delayed bedtime.
early to middle adulthood
19-50 years
7-9 hours
REM 20%
NREM 80%
early to middle adulthoodexplaninnation
Total daily sleep and proportion of REM is settled for the moment - decreases as we age.
N3 continues to decrease and we spend more time in N1 and N2.
More frequent awakenings in middle adulthood.
Frequent awakenings and lifestyle choices (staying up, work, social pressure, alcohol consumption) leads to decreased quality of sleep.
older adult, age
50+ years
important pattenrs and explanation for older adults/elderly,
→ lifestyle changes?
→change to circadian rhythm
→changes to proportions of sleep?
→ changes to awakenings?
→sleep latency?
→melatonin?
Sleep patterns in older adults can alter because of lifestyle changes
e.g “retirement, health problems, more people dying, less social, etc.”
A circadian phase advance occurs, and less sleep may be achieved if a person resists the body’s preference for an earlier bedtime and earlier awakening.
Amount of N3 sleep continues to decline and may not occur at all, replaced with N2 sleep or more frequent awakenings.
During older adulthood there is an increase in sleep latency (the time taken to fall asleep).
Melatonin concentrations continue to decline.
The shorter total sleep in this stage may be due to the impaired ability to obtain sleep, rather than a reduced need for sleep.
sleep onset trends for all age groups,
neonatal
infants
children
adolescents
adults
elderly
Sleep onset (circadian rhythm determined)
Neonatal (no circadian rhythm, many sleep episodes over 24 hours)
Infants (circadian rhythm becomes established, longer sleep blocks overnight starting ~9-10pm, several naps during day)
*Children (1-2 naps in early childhood, sleep onset gets earlier when naps are dropped 5-7 and shifts later again in late childhood ~7-8pm)
*Adolescents (sleep onset moves later again ~9-10pm as circadian rhythm shifts later than both childhood and adulthood by a couple of hours)
*Adults (varies but ~8-12pm)
*Old age (varies but generally a bit earlier than when an adult)
sleep awakenings
Sleep awakenings
Neonatal (many over 24 hrs, awake generally not longer than 20-90 min, sleeping pattern is erratic!)
Infants (several short to medium periods awake to feed overnight for ~30-60 min overnight until ~6 months of age, awake periods between naps during the day)
Children (occasional brief to short awake periods overnight)
Adolescents & Adults (stays relatively the same/stable⇒ several brief awakenings overnight)
Old age (many more brief to short awakenings overnight )
Melatonin production and age
Neonatal
minimal melatonin production
= no night/day cycle, mostly asleep with regular short period of being awake - SCN not active?
Infants
rapid increase in melatonin
= night/day cycle and establishment of circadian rhythm
Children
melatonin still high = fewer but longer naps, and night sleep
Adolescents
melatonin starts to drop = puberty and night sleep only
circadian rhythm delayed by 1-2 hours
Adulthood
Slow decline in melatonin
Old age
low melatonin production
why lower melatonin production in older people?
Older people:
Cortisol levels lower = less blood glucose = less energy -> less active during day & significantly less active at night (maybe also less light entering eyes overall?)
Suprachiasmatic nucleus fires less during day and night = fewer messages to pineal gland to produce & release melatonin
-> less melatonin produced during day and night, and ends earlier in night = less sleepy & less deep sleep, shorter duration sleep
*Still tend to spend the same amount of time or more time in bed compared to adults but less time sleeping effectively
circadian rhythm sleep disorders
A category of sleep disorders characterised by a persistent pattern of sleep disruption due to a misalignment between the circadian rhythm and the sleep–wake schedule required by a person.
what they cause often
The misalignment causes excessive sleepiness, insomnia, distress or impairment of a person’s functioning.
These disorders may cause a person to be unable to sleep and wake at the appropriate times needed to attend school, go to work or participate in social activities.
symptoms (know some)
General fatigue
Excessive sleepiness
Amplified emotional responses
Impaired cognition
Slowed reaction time
Reduced self-control
Reduced emotional awareness
Difficulty falling asleep
Difficulty staying asleep
Waking up too early and not being able to get back to sleep
causes
Exposure to light at unusual or irregular times
The colour of light a person is exposed to before bedtime
Unhealthy or irregular sleeping habits
Shift work
Travelling (particularly between time zones)
Other underlying health conditions
Delayed Sleep Phase Syndrome [DSPS]
Delayed Sleep Phase Syndrome (DSPS) is a circadian rhythm sleep disorder characterised by a delay in the timing of sleep onset and awakening, compared with the timing that is desired.
how long delay
2+ hours, person falling asleep later than what is conventionally accepted
why it affects? common amongst whom? main effect
The delay in sleep onset contributes to a sleep disorder when a person is unable to achieve their recommended amount of sleep
teens and young adults, due to SCN delaying melatonin release.
main effect is sleep deprivation, becaues reduces total sleep gotten.
Advanced Sleep Phase Disorder
Advanced Sleep Phase Disorder (ASPD) is a circadian rhythm sleep disorder characterised by an advance in the timing of sleep onset and awakening compared to the timing that is desired.
A person may fall asleep usually two or more hours earlier
when someone with this tries to shift to a more reasonable later bedtime
, they may continue to have an early wake time due to the shift in their circadian rhythm.
common amongst? even though they say quality and quantity is fine, some struggle to —?
amongst - middle aged to older adults
struggle to stay awake early evening and they feel sleepy.
causes of delayed sleep phase syndrome
Adolescence & social pressures
Irregular sleep schedule
Confined to bed for an extended period
Lack of exposure to light
Jet lag
causes of advanced sleep phase disorder
A family history of ASPD
Older age
Too much exposure to morning light
Environmental factors, such as work schedules
ASPD don’t affect how ___ you sleep, but _____ you sleep
they don’t affect how long you sleep for, they affect when you sleep.
shift work sleep disorder (NOT APPROVED ABBREIVATION SWSD)
Shift work can cause a circadian rhythm sleep disorder when a person regularly works outside of normal business hours, particularly at night and the very early morning.
e.g consistent night shift, or rotating schedule
Shift work can put sleep wake schedule opoiste to regular day night hours, causing distress dysfunction, sleepiness, bad sleep.
Estimated workers affected by this shift work sleep disorder
10-40%
to ease into this, rotaions
min 3 weeks at a time, to adjust.
shift forward, like morn shift, to afternoon shift, to evening shift to night shift, to adjust well
or return to good day routine
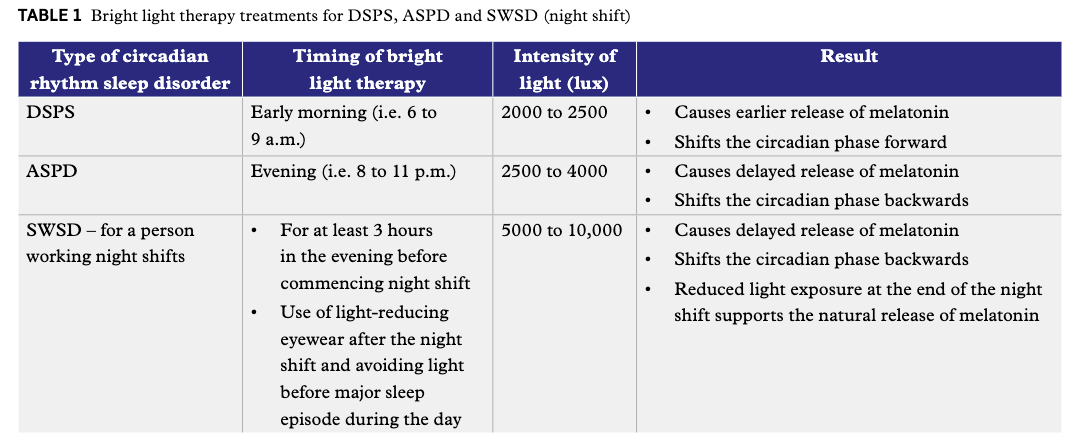
bright light therapy
exposing people to diff light intensities to reset sleep wake cycle.
around 2-60 mins, recc, over several days.
bright light therapy for aspd,
evening (8-11 pm),
light intensity 2500-4000 lux
result:
later melatonin release, delays sleepiness o appropriate time, shifting it forward.
bright light therapy for DSPS
early morn (6 am - 9 am)
-limiting night time light exposure + gradually going to bed earlier each night over several weeks.
light intensity 2000-2500 lux
reduces melatoni release in morning, so reducing drowsiness.
Shift s circadian rhythm backwards.
right light therapy for Shift work sleep disorder
min 3 hours in evening, b4 night shift.
light reducing eyewear after night shfit
avoidinf light before major sleep of day
light intensity 5000-10,000
results:
dleays release of mleatonin at night
shift circadian phase backwards
reduced light exposrue during the ay supports reease of melatoinin.
bright light therapy revise in this photo