Pulm Step 1
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
Lung Embryology
What are the 5 stages?
What age does lung development end?
What stage do Type 2 pneumocytes form?
1. Embryonic (~Week 4): Lung bud derives from foregut; Tracheoesophageal fistula.
Pseudoglandular (~5-16 Weeks): Develops up to terminal bronchioles.
Canalicular (~16-26 Weeks): Develops up to alveolar ducts; respiration possible at the end of the period; Type 2 pneumocytes form.
Saccular (~26 Weeks - Birth): Primitive alveoli form.
Alveolar (Birth - Age 10): Alveoli continue to develop.
Flashcard #2Term: What age does lung development end? Definition: Lung development ends approximately at age 10.
Flashcard #3Term: What stage do Type 2 pneumocytes form? Definition: Type 2 pneumocytes form during the Canalicular stage (~16-26 weeks).
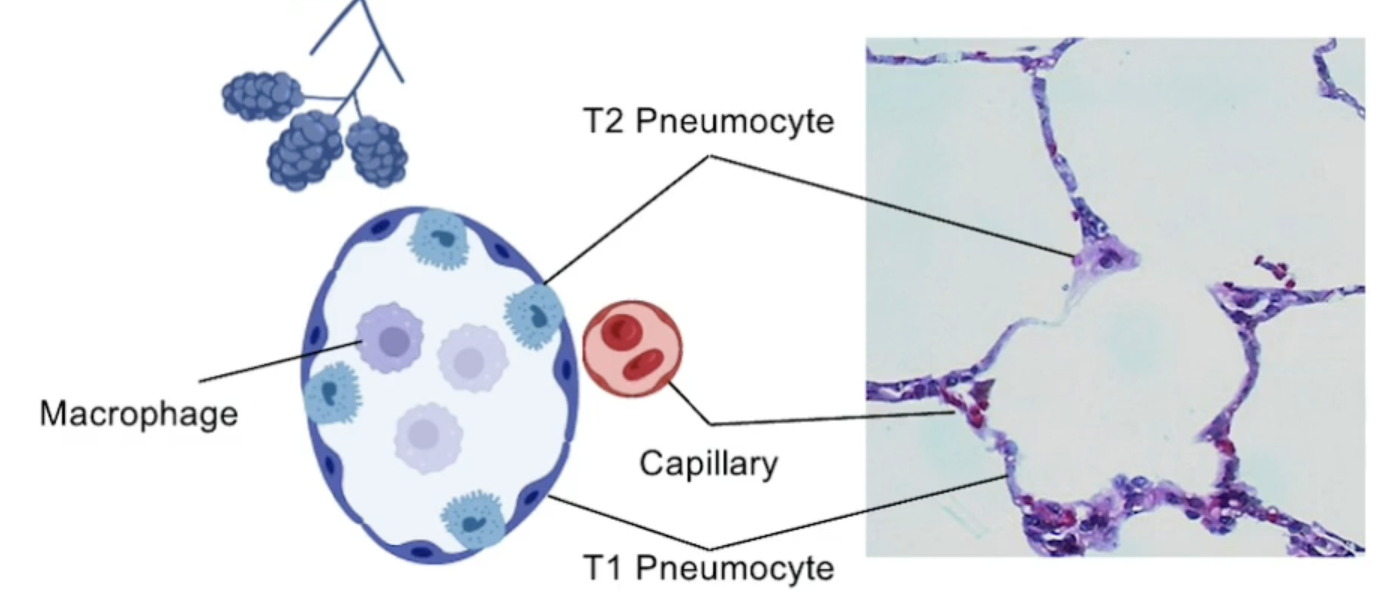
Type 1 Pneumocytes vs Type 2 Pneumocytes
Type 1 Pneumocytes: Squamous epithelial cells that make up approximately 90-95% of the alveolar surface area, responsible for gas exchange.
Type 2 Pneumocytes: Cuboidal cells that produce surfactant, which reduces surface tension in the alveoli and helps prevent alveolar collapse. They also play a role in the repair of the alveolar epithelium.
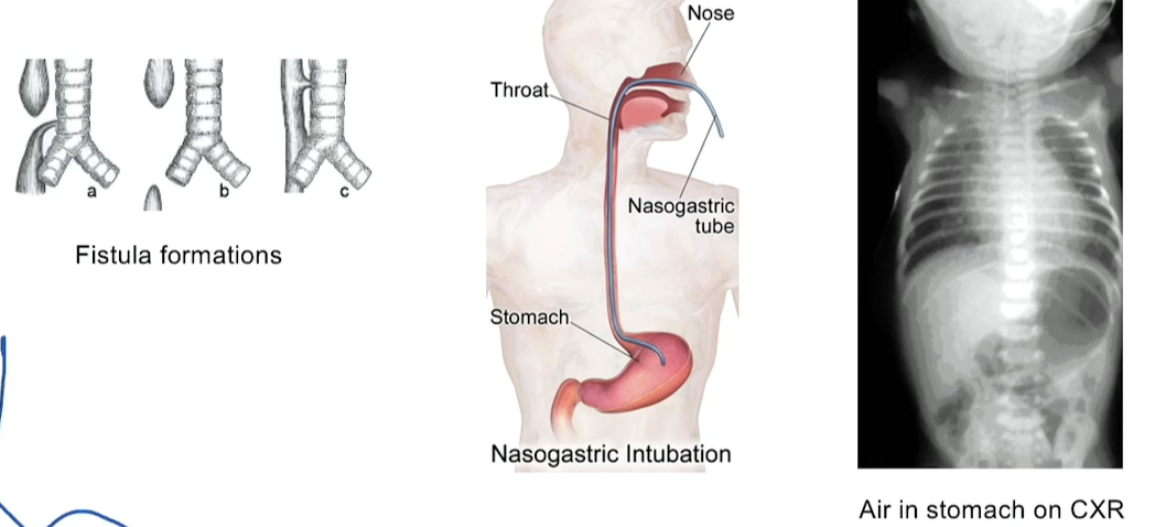
Tracheoesophageal Fistula
From embryonic stage (recall lung bud derives from foregut)
Sx
cant pass NG tube
polyhydraminos (bb cant swallow fluid so it builds up)
Drooling, vomitting, choking on 1st feed
Air in stomach on CXR
What type of cells are in the trachea?
Pseudostratified ciliated columnar epithelium with goblet cells
Bc goblet cells needed to trap dirt and dust etc. (unlike esophagus which need stratified squamous epithelium. If it had goblet cells producing mucus, the food would just scrape it as it moved down)
What two things can cause pulmonary hypoplasia?
(1) Renal agenesis (Potter sequence). Baby will not be able to produce fluid (aka pee it out) so it will not have fluid to swallow —> usually swallowing fluid is what helps the alveoli expand so without it, the lungs do not expand to their full lung volumes
(2) Congenital diaphragmatic hernia (pleuroperitoneal membrane does not form —> herniation of abdominal contents into the thorax, restricting lung development.
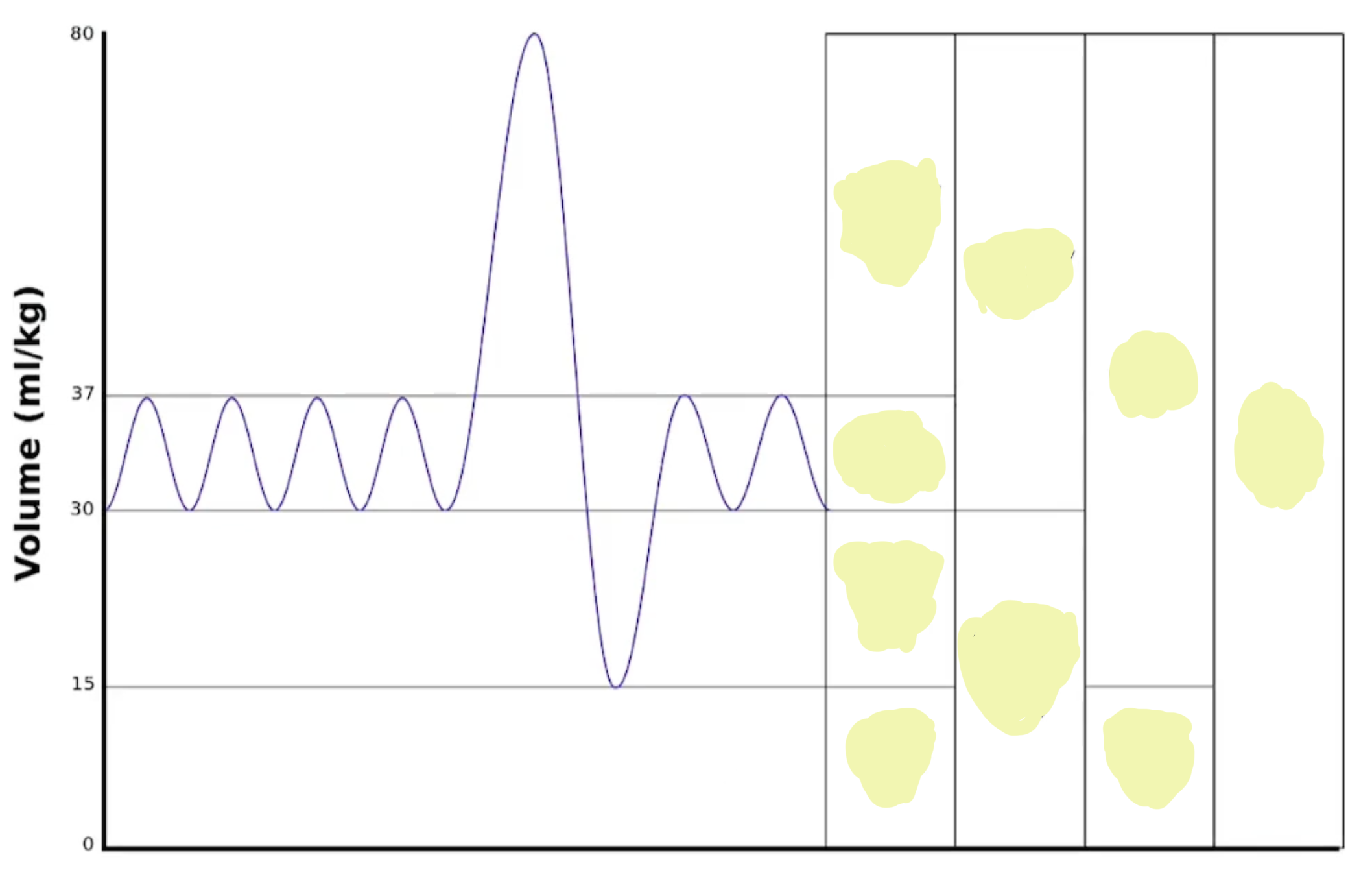
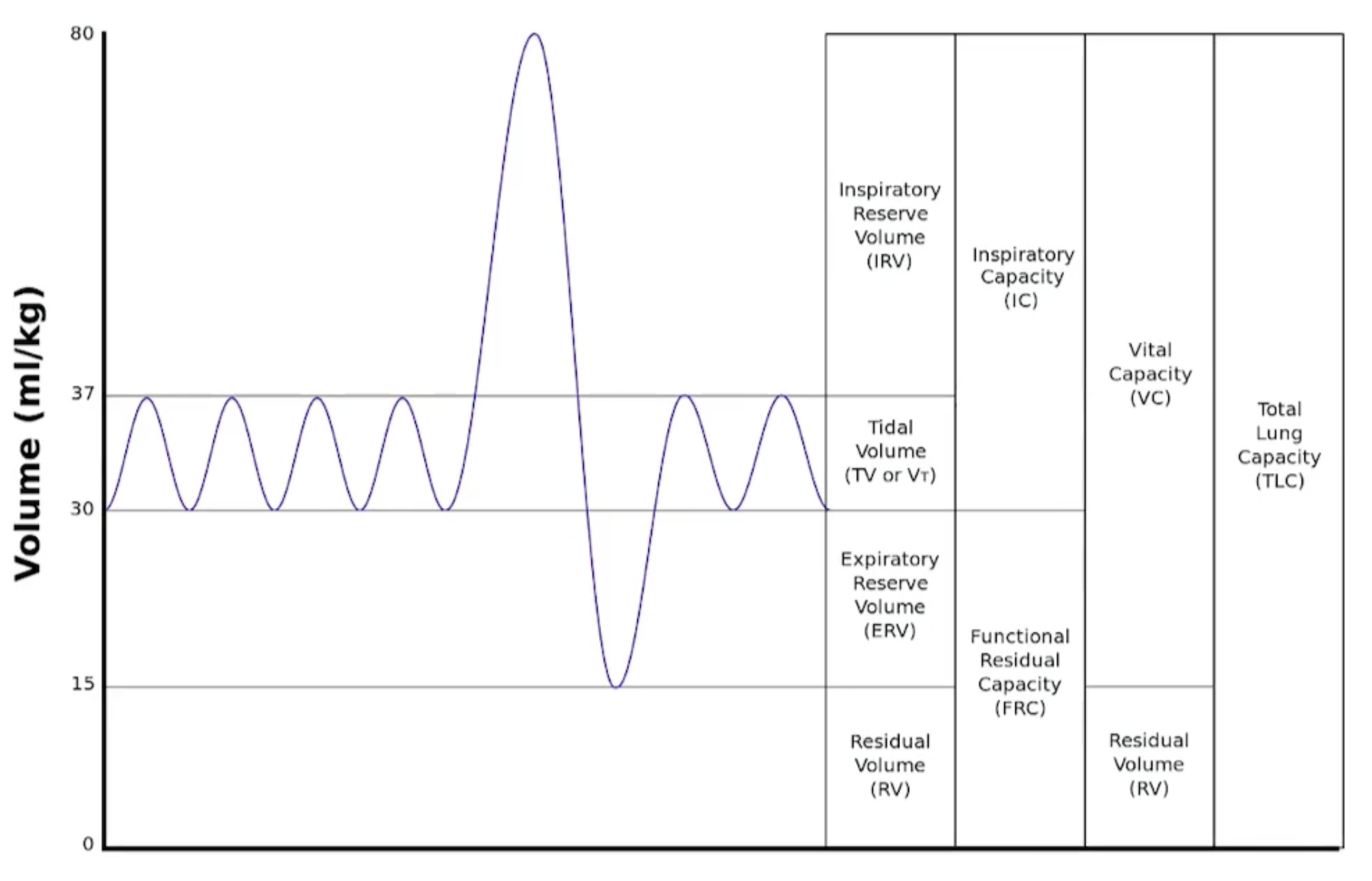
Name these lung volumes & lung capacities
The four primary lung volumes include:
Tidal Volume (TV) - the amount of air inhaled or exhaled during normal breathing.
Inspiratory Reserve Volume (IRV) - the maximum amount of air that can be inhaled after a normal inhalation.
Expiratory Reserve Volume (ERV) - the maximum amount of air that can be exhaled after a normal exhalation.
Residual Volume (RV) - the amount of air remaining in the lungs after a forced exhalation.
The lung capacities are:
Total Lung Capacity (TLC) - the total volume of air in the lungs after a maximum inhalation.
Vital Capacity (VC) - the maximum amount of air that can be exhaled after a maximum inhalation.
Functional Residual Capacity (FRC) - the volume of air remaining in the lungs after a normal exhalation.
Inspiratory Capacity (IC) - the maximum volume of air that can be inhaled after a normal exhalation.
Physiological Dead Space
What is it?
What is the equation?
Physiological dead space refers to the portion of the respiratory system where gas exchange does not occur, including both anatomical dead space (e.g., trachea and bronchi) and any alveoli that are ventilated but not perfused.
Where
Vt = tidal volume
PaCO2 = Arterial pressure of Co2
PeCO2 = Expired pressure of CO2

Minute Ventilation
Amount of air entering lungs per minute
Ve = Vt * RR
Tidal volume * respiratory rate
Surfactant
Where is it produced & held?
What is its role?
In what diseases is lack of surfactant the main pathology?
Surfactant is a substance composed of lipids and proteins that is produced by type II alveolar cells (pneumocytes), particularly the lamellar bodies.
Its primary role is to reduce surface tension in the alveoli, preventing their collapse during exhalation and facilitating gas exchange.
Lack of surfactant is a key pathology in conditions such as neonatal respiratory distress syndrome and acute respiratory distress syndrome (ARDS).
Compliance
What is it?
Give an example of high compliance disorder
Give 2 examples of low compliance disorders
Is asthma a low, normal or high compliance disorder?
Compliance is how willing a lung is to expand (in other words, how much the lung volume will change with a given change in pressure)
High Compliance Disorders —> means that for a given change in pressure, the lung volume will change a lot. Occurs bc the lung is not trying to snap back because it is more "floppy" or has less elastic recoil, commonly seen in conditions like emphysema.
Low compliance disorders —> means that for a given change in pressure, the lung volume will not change a lot, in other words, either the lung is VERY elastic or there isn’t a lot of surfactant to fight the surface tension Ex. ARDs (less surfactant) Ex. Pulm edema (bc water dilutes surfactant) Ex. Pulm fibrosis (bc lungs are more elastic/stiffer)
We usually think of obstructive lung diseases as being high compliance but in the case of asthma, the compliance is normal, the problem is just broncho-constriction
Airway Resistance
What is it? Where is it the highest vs lowest for individual? Total?
How does airway resistance play into chronic bronchitis & asthma?
Airway resistance refers to the opposition to airflow within the respiratory tract. It is highest in a small airway, lowest in a big ariway. However, if we are looking at things as TOTAL airway resistance, the small ariways have a much lower airway resistance because there are so many of them, followed by big airways bc they’re big, and lastly, medium airways because they are neither big nor are there a lot of them
In conditions like chronic bronchitis and asthma, airway resistance increases due to inflammation and bronchoconstriction, leading to difficulty in airflow. In chornic bronchitis, pressure drops significantly after passing a mucus plus —> EPP gets closer to alveoli
Work of breathing
How do RR and tidal volume change in obstructive lung diseases vs restrictive lung diseases in order to minimize the work of breathing?
The work of breathing refers to the energy expenditure required for breathing, involving muscle contractions to inhale and exhale.
In obstructive lung diseases, patients often decrease their respiratory rate (RR) while breathing at high lung volumes (bc at high volumes there is less resistance and resistance is what they struggle with the most)
If patients breathe too quickly, they don't have enough time to exhale completely.
This causes air trapping and dynamic hyperinflation.
Therefore, they tend to breathe:
Slowly (↓ RR)
Deeply (↑ tidal volume)
In restrictive lung diseases, patients commonly adopt a higher RR with lower lung volumes to maximize lung expansion despite reduced lung capacity.
In restrictive disease:
The lungs are stiff (↓ compliance).
Every deep breath requires a lot of pressure and muscular effort.
Because of this, patients minimize the work required by taking:
Small tidal volumes
Rapid respiratory rates
They maintain minute ventilation by increasing RR:
Minute ventilation=RR×VT\text{Minute ventilation} = RR \times V_TMinute ventilation=RR×VT
instead of increasing tidal volume.
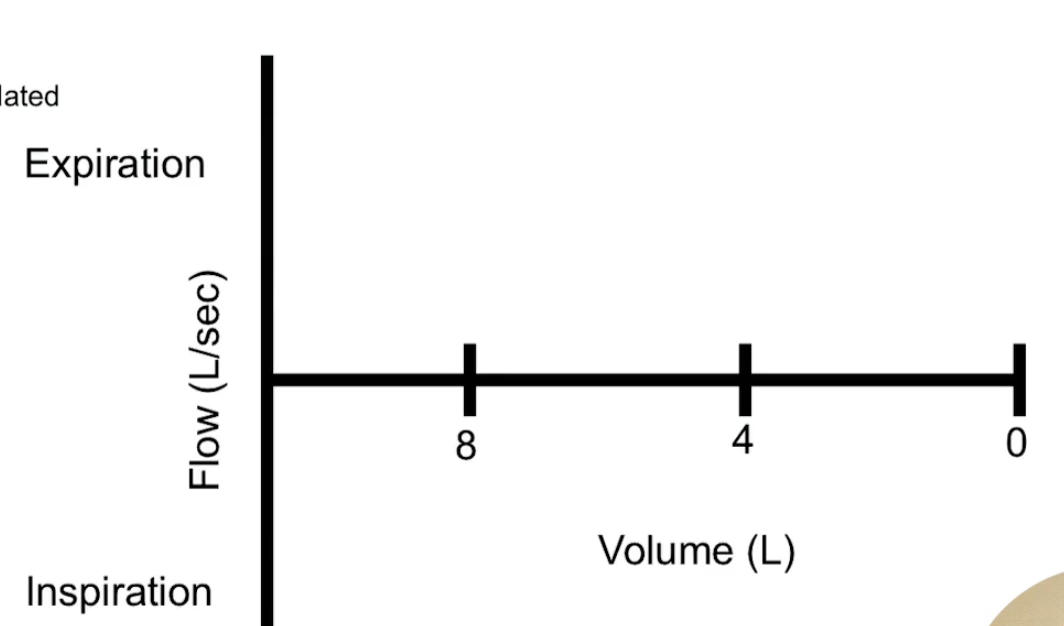
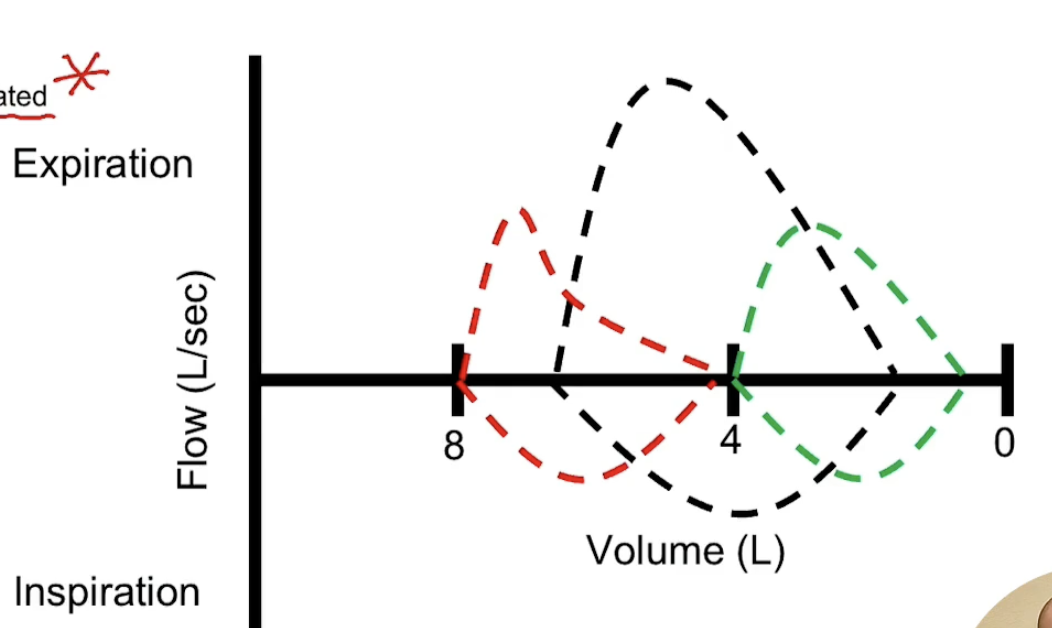
What would a normal flow volume loop look like?
One for obstructive disease? One for restrictive disease?
Black is normal
Red is obstructive
Green is restrictive
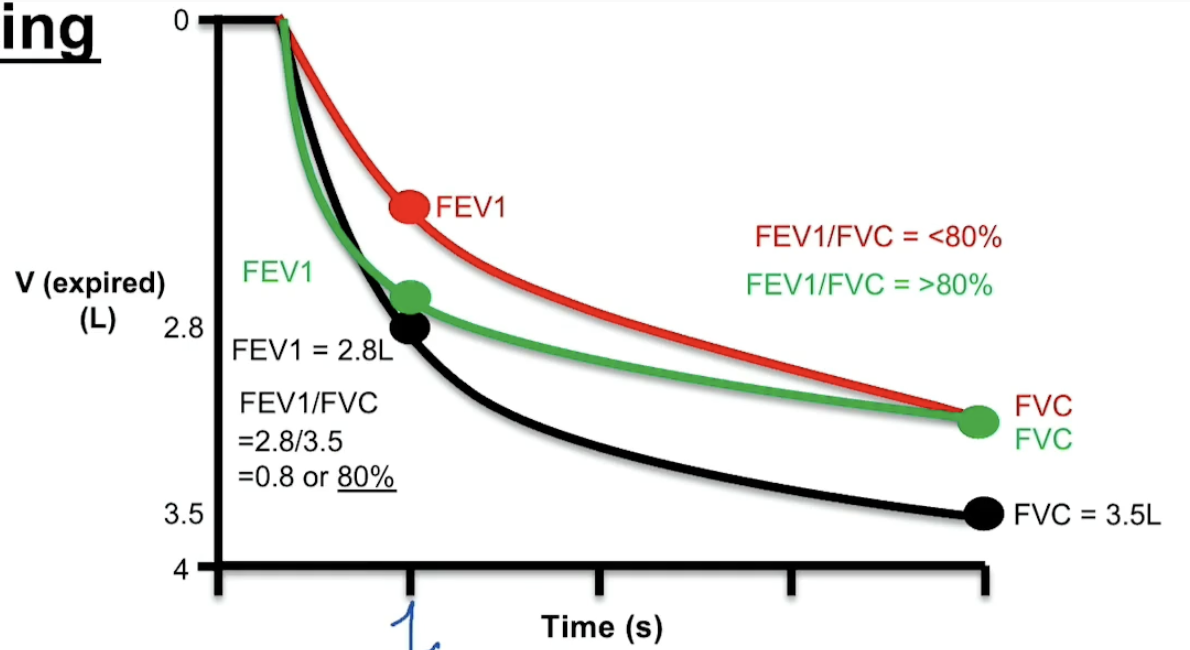
Pulmonary Function Test
What are the 2 important values we get from this?
How do these values vary based on it being normal vs obstructive vs restrictive?
The 2 values are:
FEV1 = expiratory volume over 1 min
FVC = forced vital capacity which measures the amount of air forced out in one breath after maximum inhalation
In healthy lungs, FEV1/FVC = 0.8
In obstructive, FEV1 is decreased relative to normal bc there is an obstruction so harder to push air out. FVC will be slightly less bc hard to breath out sooooo FEV1/FVC < 0.8
In restrictive, FEV1 will be slightly lower just bc not a lot of lung volume to begin with, BUT FVC will be greatly decreased soooo FEV1/FVC = normal or >0.8
Hypoxic Pulmonary Vasoconstriction
How does that relate to fetal circulation?
Hypoxic pulmonary vasoconstriction is the physiological response where pulmonary blood vessels constrict in response to low oxygen levels, directing blood flow to better-ventilated areas of the lung.
In fetal circulation, this mechanism is crucial as the fetus relies on placental oxygen exchange; pulmonary blood flow is minimized in the hypoxic fetal lungs, enhancing overall gas exchange efficiency by diverting blood away from the non-functioning lungs. So pressure is high in R side circulation. This allows for shunts like the foramen ovale and the ductus arteriosus to remain open, ensuring that oxygenated blood from the placenta bypasses the non-functioning lungs.
Howeverrrr, when a baby takes their first breath all that is reversed, leading to decreased hypoxia, pulmonary vasodilation, increased blood flow to the lungs, and subsequent closure of shunts like the foramen ovale and ductus arteriosus, as the lungs become oxygenated and begin functioning in gas exchange.
Pathological V/Q Mismatches
Shunt
Regular V/Q Mismatch
Dead Space
Explain what it is for each, what causes it, and any special considerations
(1) Shunt:
This occurs when blood flows through the lungs without being oxygenated, due to an obstruction. Hypoxic pulm vasoconstriction will occur in response.
So, V = 0 so V/Q = 0
WILL NOT respond to 100% oxygen bc blockage
(2) Regular V/Q Mismatch:
This refers to areas of the lung that ventilate well but do not perfuse adequately (high V/Q) or perfuse well but do not ventilate adequately (low V/Q), leading to a mix of oxygenated and deoxygenated blood Ex. pulmonary edema, pna,
WILL respond to 100% O2; however, give slowly or else massive vasodilation when alveoli actually isnt in a state to accept CO2 so CO2 will build up —> Hypercapnia
(3) Dead Space:
This occurs when ventilation is present without perfusion, often seen in conditions like pulmonary embolism, where a blockage in a blood vessel prevents blood flow to ventilated areas.
Since Q= 0 then V/Q = infinity
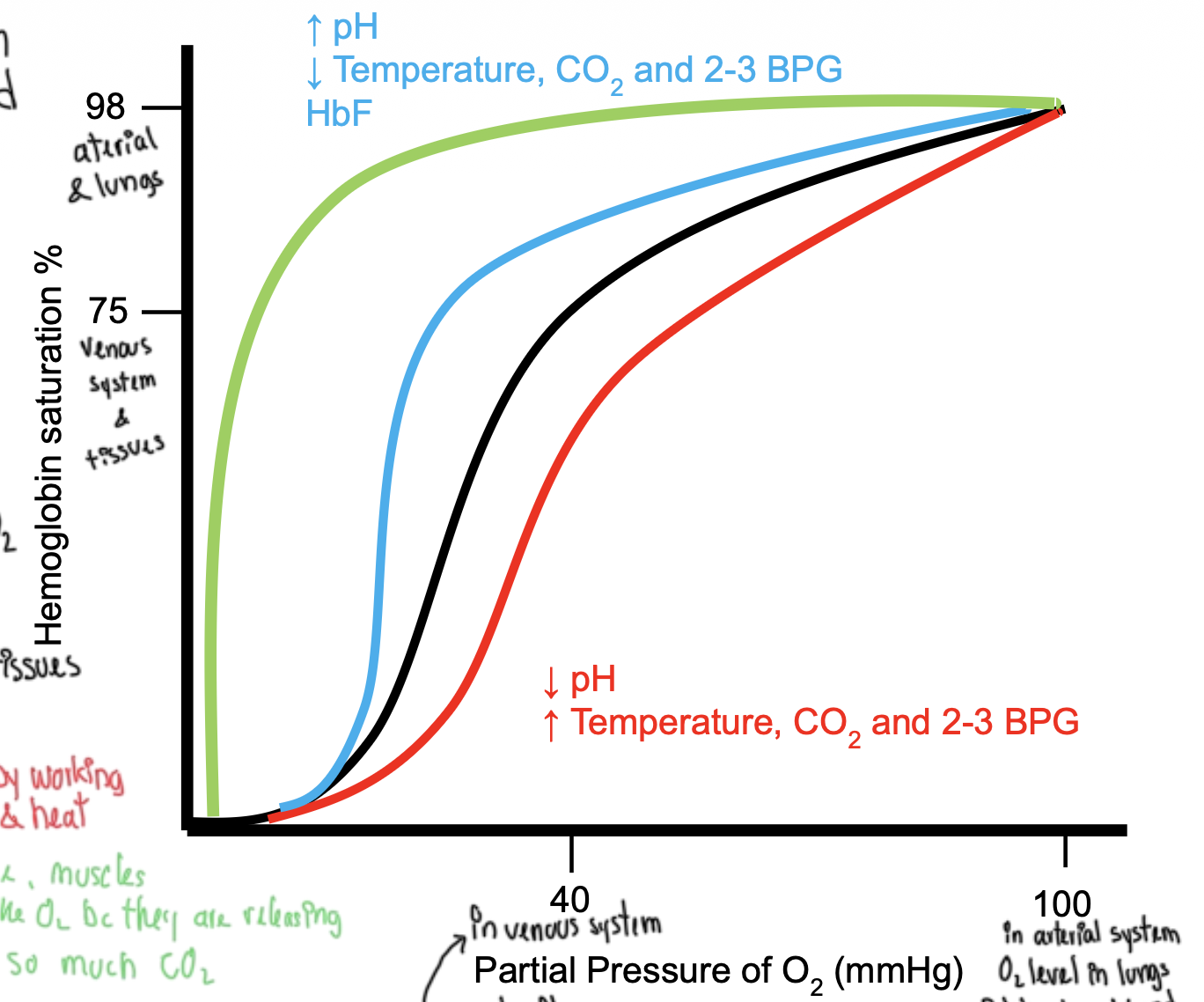
Hemoglobin
What is its structure?
What is its curve? What makes the curve shift left or right?
What are fetal hemoglobin and myoglobin/ how are they different? What are their curves?
4 subunits with Fe in the middle, 2 a and 2 b subunits. The b subunits exhibit cooperativity
Its curve is an s shape. The curve will shift left (or decrease its affinity to oxygen, in other words be more willing to let to go) with things associated with a working muscle like increased CO2 (and remember CO2 —> HCO3 —> H+ soooo) decreased pH, increased temp and increase 2,3-BPG. The curve will shift right (or increase its affinity to oxygen) with the opposite conditions (decreased CO2, increased pH, lower temperature, or decreased 2,3-BPG)
*NOTE: 2,3 BPG lowers affinity for oxygen. It is only produce in RBCs from 1,2 BPG in glycolysis. It increases in chronic hypoxia.Fetal HgB has 2 y subunits instead of 2 b subunits and it very tightly binds oxygen. Myoglobin doesn’t have b subunits so no cooperativity. It is VERY attached to oxygen (Think of it like "a backup for the muscles, holding onto oxygen until it's needed").
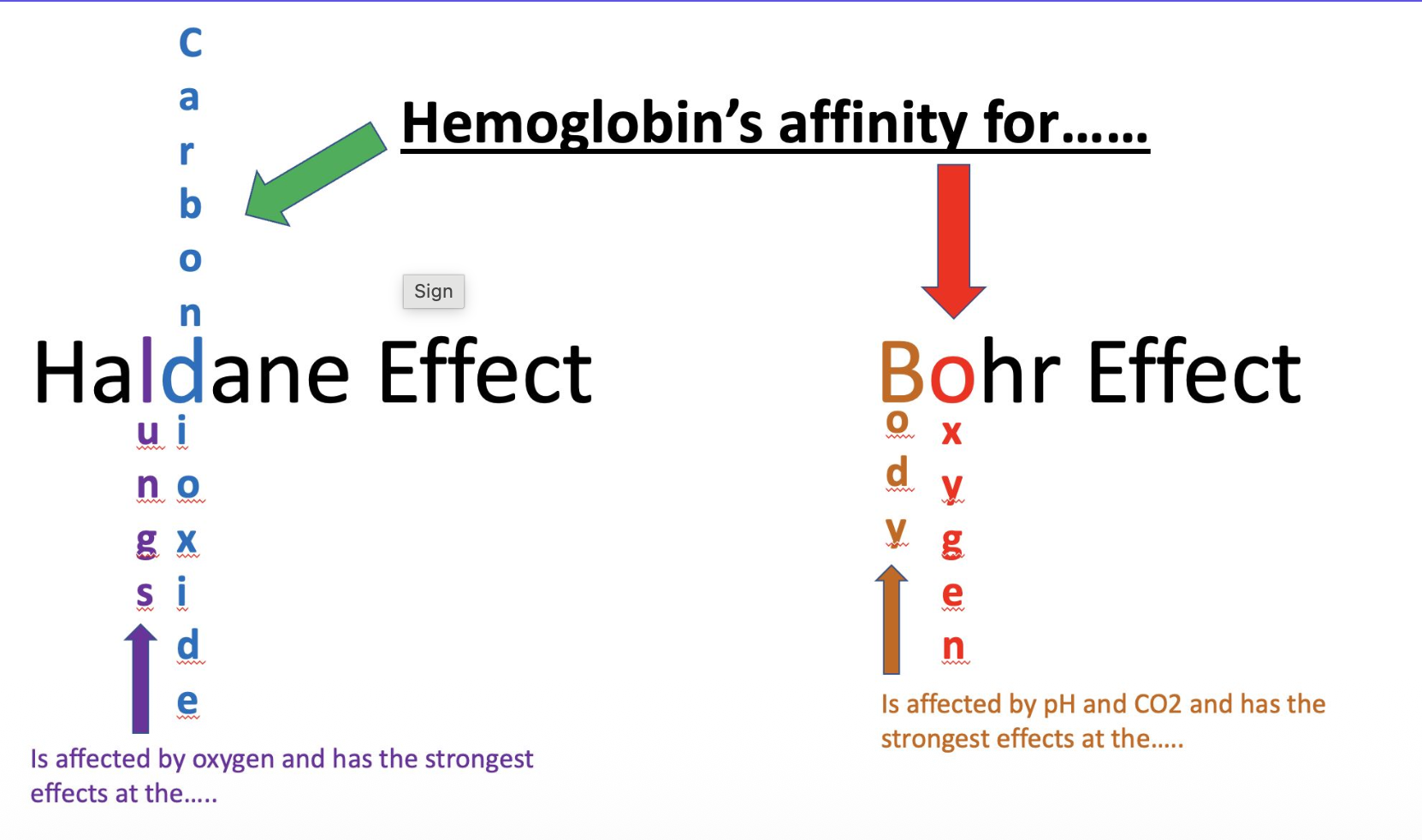
What is the Haldane Effect?
What is the Bohr Effect?
Haldane:
At the lungs, when HgB carrying CO2 sees high oxygen, it will drop that CO2 and snatch up that oxygen
Bohr:
In the rest of the body, when HgB carrying oxygen sees high CO2, it will drop oxygen and snatch up that CO2
Carbon Dioxide
Is the solubility high or low? What are the implications of this?
Through what mechanism can someone become hypercapnic or hypocapnic? How does it affect the pH?
What influences partial pressure of CO2?
Transport:
How does the majority of CO2 make it to the lungs?
What role does bicarbonate play in transport of CO2?
Solubility is high so moves easily through blood and tissue fluids (Faces little barrier crossing the alveolar-capillary membrane & Reaches equilibrium quickly, making diffusion into the alveoli very efficient)
That’s why even though CO2 has a smaller pressure gradient than oxygen, it still diffuses out of the blood into the alveoli very easily.
VERY easy to diffuse. Will always diffuse even if there is a diffusion problem in the alveoli.
Partial pressure comes from CO2 dissolved in blood
Majority of CO2 gets to lungs via bicarbonate (HCO3-) form in plasma
CO2 levels change when exhaled out. Sooo….
If you hyperventilate —> Blow out a lot of CO2 so hypocapnia (and if less CO2, then less H+) AND alkalosis
If you hypoventilate —> You are not blowing out CO2 so hypercapnia (and if more CO2, then more H+) AND acidosis
CO2 is converted to HCO3- but CA in the RBCs —> HCO3- leaves RBC & in order to maintain electric, Cl- ion comes in, with it goes H2O (so cell swells). When CO2 is being offloaded into alveoli, CA will convert HCO3 into CO2 so it can diffuse and be exhaled
Why does the partial pressure of O2 increase by 60 mm Hg upon inhalation, but CO2 only drops 5 mm Hg on exhalation?
Oxygen is much less soluble than CO2
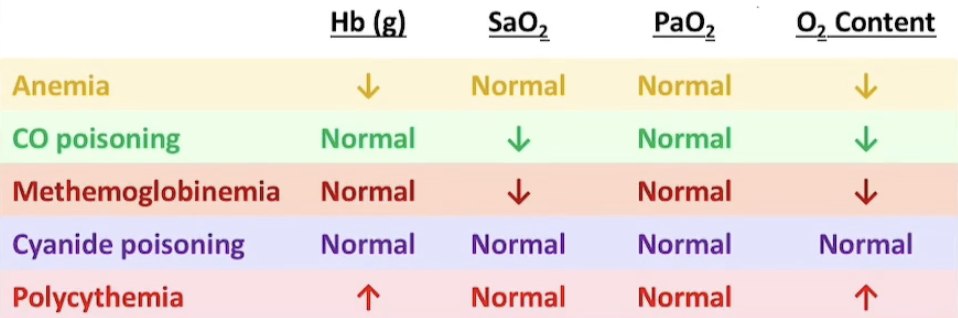
Fill out this table
Methemoglobinemia is when Fe2+ is oxidized to Fe3+ so O2 cannot bind.
Cyanide poisoning binds to cytochrome c oxidase, inhibiting cellular respiration and preventing aerobic production of ATP. In order to solve this, you add nitrates which will induce MethgB which will then bind to the cyanide and reduce its toxicity by preventing it from binding to cytochrome c oxidase. This allows some oxygen transport to occur despite the cyanide.
Diffusion Limited vs Perfusion Limited Gases
Give at least one example for each
A perfusion limited gas will always equilibrate across alveoli and capillary. Example: Oxygen in healthy lungs or NO2. So limited by how much blood is passing through
A diffusion limited gas will not equilibrate across alveoli and capillary. Example: Carbon monoxide or oxygen in fibrotic lungs. So limited by time in contact with membrane
Diffusion Capacities of the Lungs of CO (DLCO)
DLCO measures the diffusion capacity of the lungs for carbon monoxide. It assesses the transfer of gas from alveoli to bloodstream. It does that by inhaling CO, then measuring how much is exhaled. The amount that is not exhaled indicates the amount absorbed into the bloodstream, reflecting the efficiency of gas exchange in the lungs.
Condition with low DLCO is pulmonary fibrosis or emphysema, where the lung tissue is damaged and unable to effectively transfer gas.
High Altitude
What happens to body? Treatment?
Decreased atmospheric pressure so lower PaO2. Results in:
Increased EPO —> polycythemia
Increased ventilation —> respiratory alkalosis (bc blowing off CO2)
Tx: Acetazolamide (which blocks CA, preventing HCO3 from being reabsorbed and aiding acclimatization) and oxygen supplementation in severe cases.
A-a Gradient
The A-a gradient measures the difference between the alveolar and arterial oxygen concentrations. It helps assess the efficiency of gas exchange in the lungs, indicating conditions like shunting or diffusion impairments.
Everyone has a gradient due to physiologic bronchial shunt
Epiglottitis
What is it? What causes it? What is the presentation (Ex. Lung sound, tracheal deviation, percussion)? Imaging?
"Inflammation of the epiglottis due to H influenze type b infection (now not as common due to Hb vaccine)
Presentation: Child with high fever, drooling, dysphagia & in the tripod position (hands on knees and head titled) to get more air
"Hand on my knees, Hb, epligottis"" Think of Thot Sh** by Meg thee Stallion
Tracheal deviation & percussion: None
Lung sound: Respiratory stridor
Imaging: ""Thumb sign"" on lateral neck X-ray

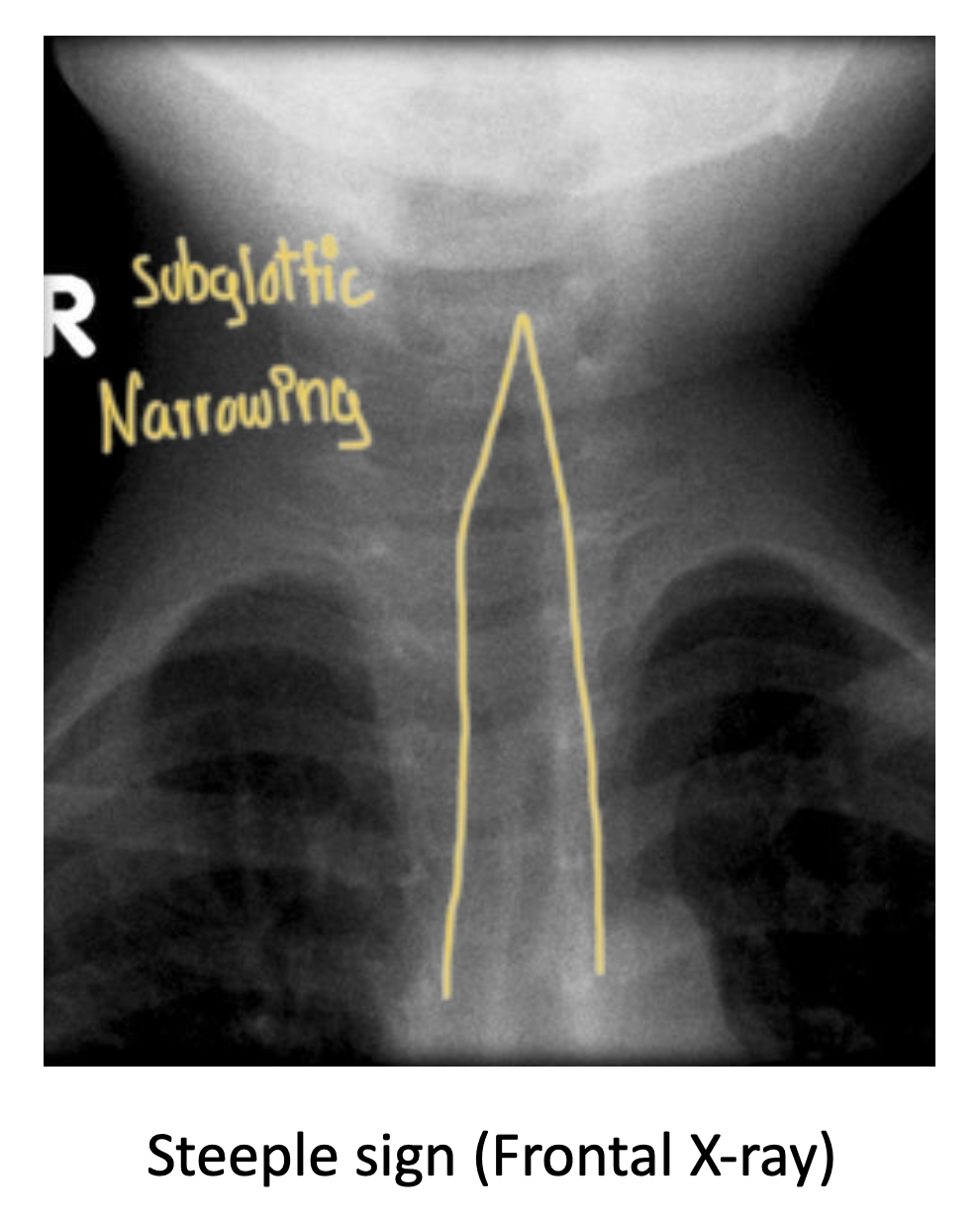
Laryngotracheobronchitis (Croup)
What is it? Cause? Presentation? Lung sound? Imaging?
Tracheal deviation & percussion?
"Inflammation of the larynx and trachea usually caused by Parainfluenza virus
Presentation: Child with fever, barking "seal-like"" cough
*croup = poop on a seal in a church; churches have steeples and a big influen(za)ce
Lung sound: Inspiratory stridor
Tracheal deviation & percussion: None
Imaging: "Steeple sign"" on frontal neck x-ray (subglottic narrowing) *Difference b/w epiglottitis & croup
Bronchiolitis
What is it? Cause? Presentation? Lung Sound?
Inflmmation of the bronchioles caused by RSV
Presentation: Very young child (<2 yrs) with fever
Lung sound: Wheezing (bc narrowing & inflammed bronchioles)
Pneumonia
What is it? Presentation? Lung sounds? Lung exam? Tracheal deviation?
Three Patterns
1. Pattern #1 Name (Microbe? 4 steps?)
2. Pattern #2 Name (Microbe?)
3.Pattern #3 Name (Microbe?)
Infection of lung tissue
Presentation: Fever. Cough (productive in lobar/bronchopneumonia & non-productive in interstitial) Sputum is yellow-green due to myeloperoxidase *looks like yellow* in neutrophils
Lungs sounds: Rales (sounds like rice crispy: snap, crackle & pop open) & bronchial breath sounds over lung paryenchma
Lung exam: Increased fremitus & dullness to percussion
Tracheal Deviation: None
Three Patterns
(1) Lobar (typical) Intra-alveolar exudates --> lobe consolidation; Cause: Strep pneumoniae
Congestion (<2 d): Microbe causes alveolar macrophages to release cytokines --> vasodilation + bacterial exudate
Red hepatization (2-4 d): Hepatization = bc lungs firm up like liver; Exudate begins to include RBCs (hence red), nuetrophils, firbin
Grey hepatization (4-6 d): RBCs become lysed and degraded thus loses red color & looks grey instead
Resolution: Macrophages replace neutrophils and digest the fibrinous exudate + Type 2 pneumocyte hyperplasia (which give rise to new Type 1 pneumocytes since they were destroyed by inflammation)
(2) Bronchopneumonia: Infection similar to typical/lobar but focused in bronchioles and nearby alveoli in lobes --> patchy opacities in lobes; Cause: Staph Aureus
(3) Interstitial (Atypical): Infection of interstitium (b/w alveoli) --> patchy diffuse opacities; mild course including low grade fever; Cause: Viral, Legionella, Mycoplasma
A quick Step 1 memory story
Imagine entering a lung:
🏠 One entire neighborhood is flooded → Lobar → Strep pneumo.
🎨 Someone splattered paint everywhere in little patches → Bronchopneumonia → Staph aureus.
🚶♂ Two unusual visitors—Mycoplasma and Legionella—refuse to enter the houses and instead walk between them → Interstitial (atypical).
This story ties the pathology to the organisms, making it much easier to recall than memorizing isolated facts.
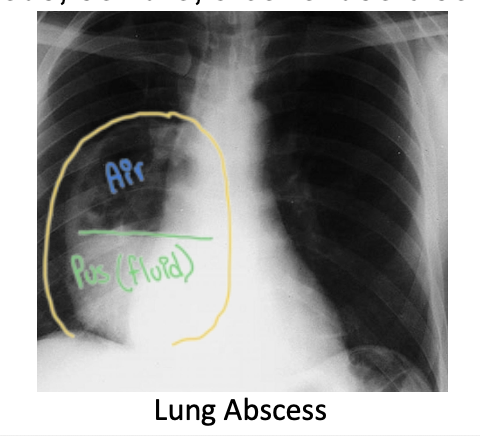
Lung Abscess
Cause? Presentation? Imaging?
Contained and localized pus collection in lungs; Cause: Aspirated oral flora anaerobes or S aureus
Presentation: Fever, night sweats, weight loss & cough with foul-smelling sputum (bc of pus)
Imaging: X-ray shows ""air-fluid level"" cavitation filled with pus
Asthma
Definition
Presentation (lung sounds & percussion)
Diagnosis
Pathological Sputum Findings
Subtypes
Definition: Episodic & reversible bronchoconstriction
Presentation: Coughing, dyspnea, hypoxemia but asymptomatic between episodes
Lung Sounds: Wheezing
Percussion: Hyperresonant during attack
Diagnosis
Normal when asymptomatic so must induce asthmatic episode via methacholine challenge (chilinomimetic like acetylcholine --> bronchoconstriction) and do spirometry:
Decreased FEV1/FVC AND Decreased Inspiration/expiration time (1/2 --> 1/4)
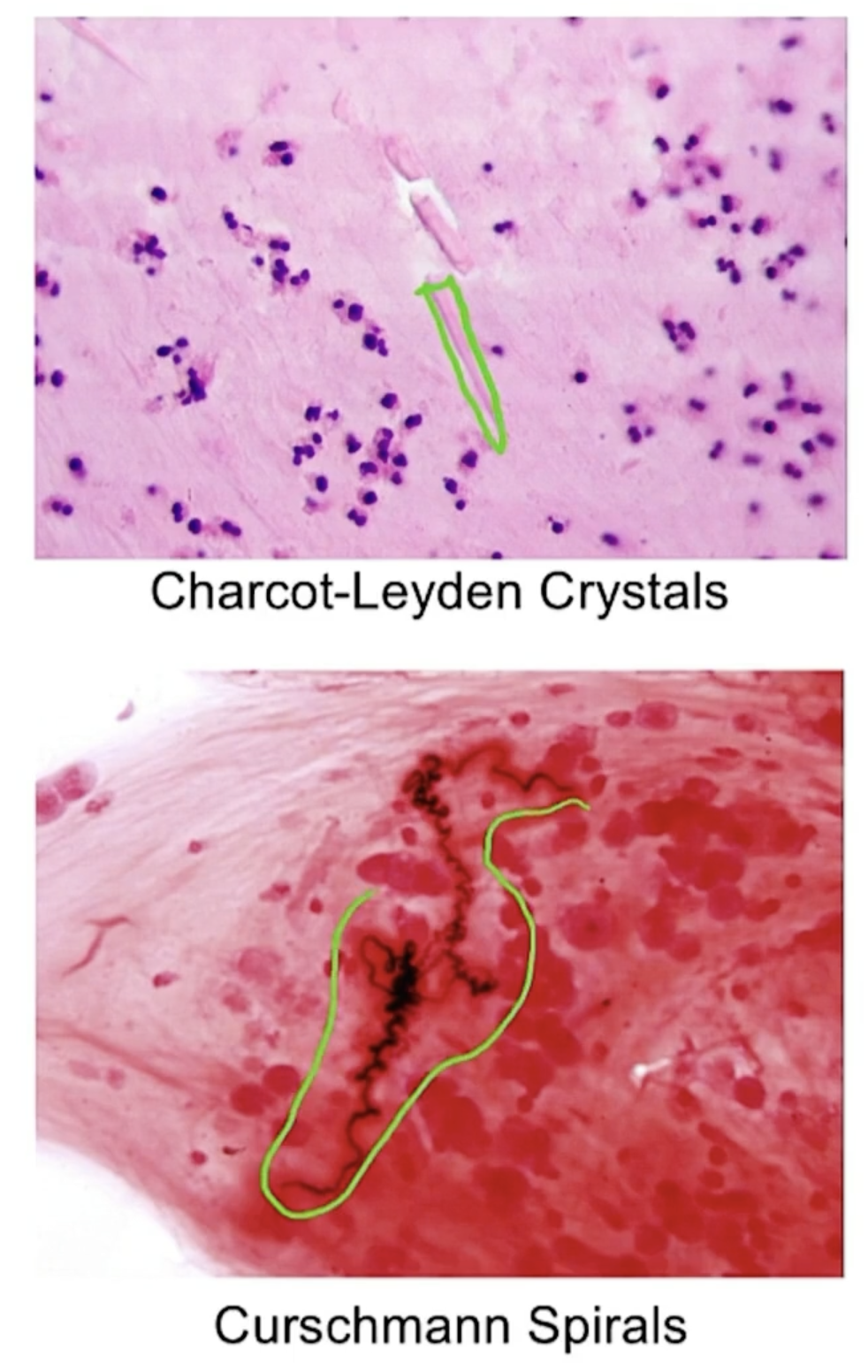
Pathological Sputum Findings
More esosinophils
Charcot-Leyden crystals (eosinophil granules)
Curschmann spirals
Subtypes:
(1) Atopic (extrinsic) - Type 1 hypersensitivity rxn due to allergn. Usually childhood onset with hx of atopic triad (atopic dermatitis or allergic rhinitis)
Classic triggers include; pets, dust & pollen
(2) Non-atopic (intrinsic) - No identifiable allergen. Usually follows viral infection, stress or exercise
(3) Status asthmaticus: Acute severe asthma --> unremitting & possibly fatal
(4) NSAID-Induced Asthma: Occurs in adults; NSAIDs block COX pathway, thus increase production of leukotriene through LOX pathway. Associated with nasal polyps (in adults - unlike CF where it is in children) and chronic rhinosinusitis"
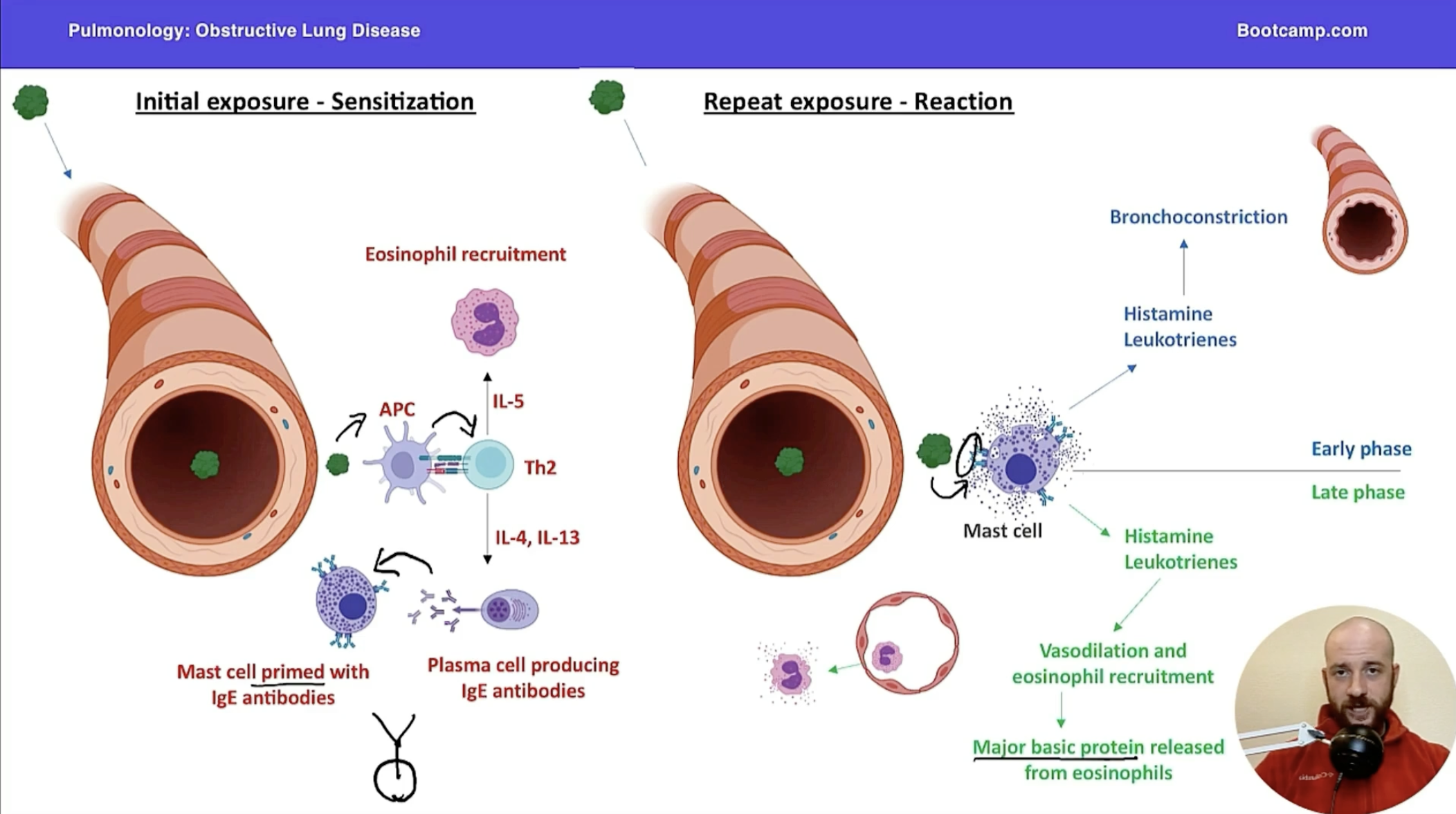
Atopic Asthma Pathophysiology
2 Phases
What is involved?
Phase 1: Sensitization
(1) Initial exposure to allergen --> Th2 cells presented with antigen by antigen present cell (APC)
(2) Th2 --> does 2 things
First, IL-5 for eosinophil recruitment
Second, IL-4 and IL-13 which leads to plasma cell producing IgE antibodies against allergen
(3) End result: Mast cell primed with IgE antibodies
Phase 2: Reaction (repeat exposure)
(1) Antigen binds to IgE on mast cell and mast cell degranulates releasing histamine & leukotrienes
(2) Early phase: Histamine & leukotriene cause bronchoconstriction
(3) Late phase: Histamine & leukotriene lead to vasodilation and eosinophil recruitment
Eosinophil releases major basic protein --> inflammation and mucus production
What leads to bronchoconstriction/ bronchodilation?
Bronchoconstriction: Parasympathetic activation (muscarinic via acet), leukotrienes, & histamines
Bronchodilation: Sympathetic activation (B2 via Epi) & cAMP
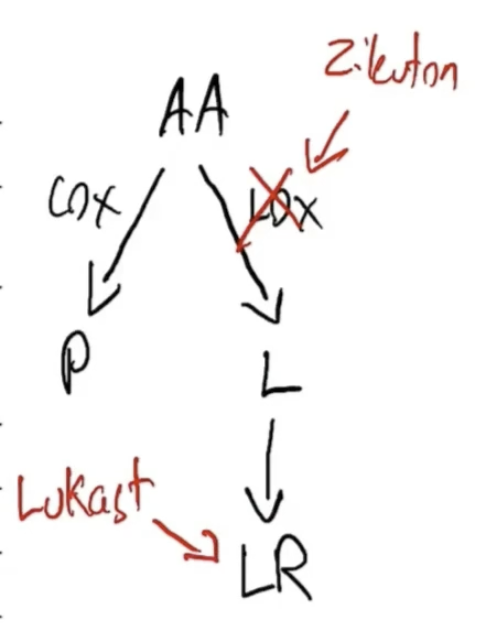
Zileuton
Block conversion of AA into Leukotrienes via LOX pathway
Anti-lipoxgenase (LOX)
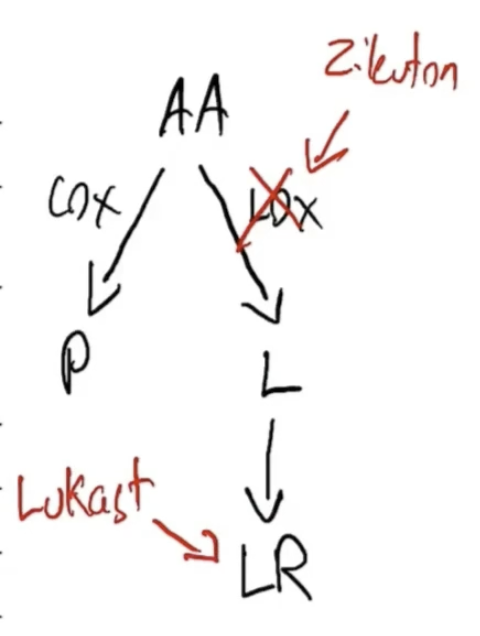
Lukast Drugs
Inhibit Leukotriene receptor Antagonists (LTRAs) used in asthma treatment, blocking the action of leukotrienes to reduce inflammation and bronchoconstriction.
Cromolyn Sodium