Macrocytic Anemias
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
33 Terms
Cell appearance
- MCV > 100fL
- MCHC is normal
Classified as
- megalobalstic
- non-megaloblastic
Megaloblastic
- Delayed nuclear maturation prevents cell division
- nuclear cytoplasmic asynchrony
Megaloblastic causes
- folate and B12 deficiency
- lack of intrinsic factor
- Myelodysplastic syndromes
- Acute Erythroid Leukemia (FAB-M6)
- Congenital Dyserythropoietic Anemia
- Reverse transcription inhibitors
Megaloblastic effects
- intramedullary hemolysis and disrupted DNA synthesis= anemia
- cell changes in other cells: skin, vaginal, uterine, cervical
Nonmegaloblastic
normoblastic maturation
- reticulocytes
- DNA is fine
Nonmegaloblastic causes
- newborns
- Reticulocytosis
- Chronic alcoholism
- Liver disease
- Bone marrow failure
B12 and Folate deficiency cause
thymidine nucleotide is impaired
- substitutes uridine
- causes apoptosis from breaks in strands
- cells that escape bone marrow, undergo ineffective hematopoiesis
Folate function
transfer carbon units (methyl groups) from donors to receptors
- in blood as 5-methyl-tetrahydrofolate (THF)
B12 and folate function
In the cell, a methyl group transfers from 5-methyl THF to homocysteine, converting it to methionine and generating THF
- requires vitamin B12
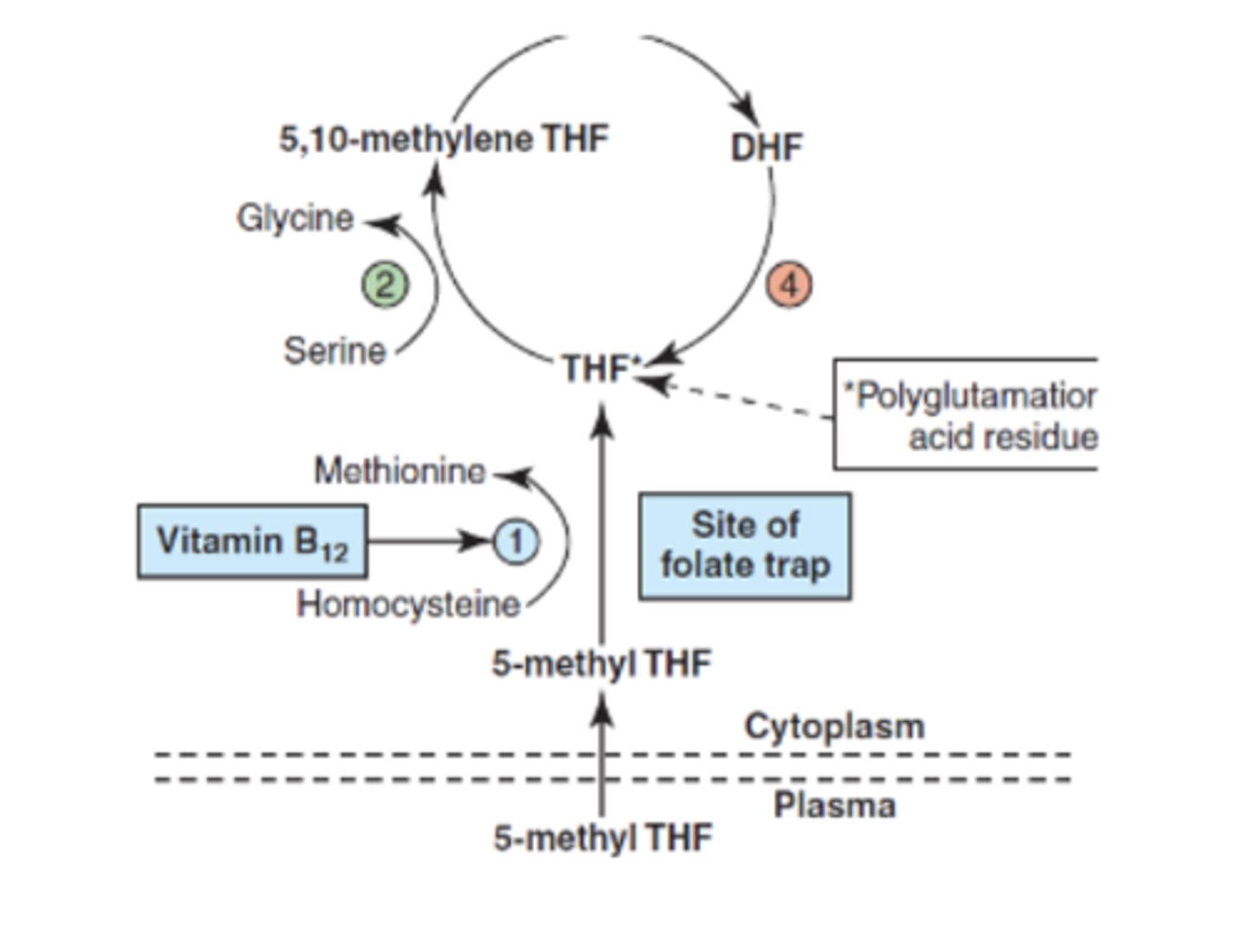
Folate deficiency
- Transported unbound
- Preventing the methylation of dUMP
Vitamin B12 decifiency
preventing the production of THF from 5-methyl THF
Folate source
- diet
- heat labile
Causes of folate deficiency
- malnutrition
- malabsorption
- drugs
- loss (dialysis)
Folate deficiency clinical
- megaloblastic anemia
- open tube neural defect
B12 daily requirements
- intake= 5 ug
- body stores= 2-5 mg
- 0.1% loss in urine and feces
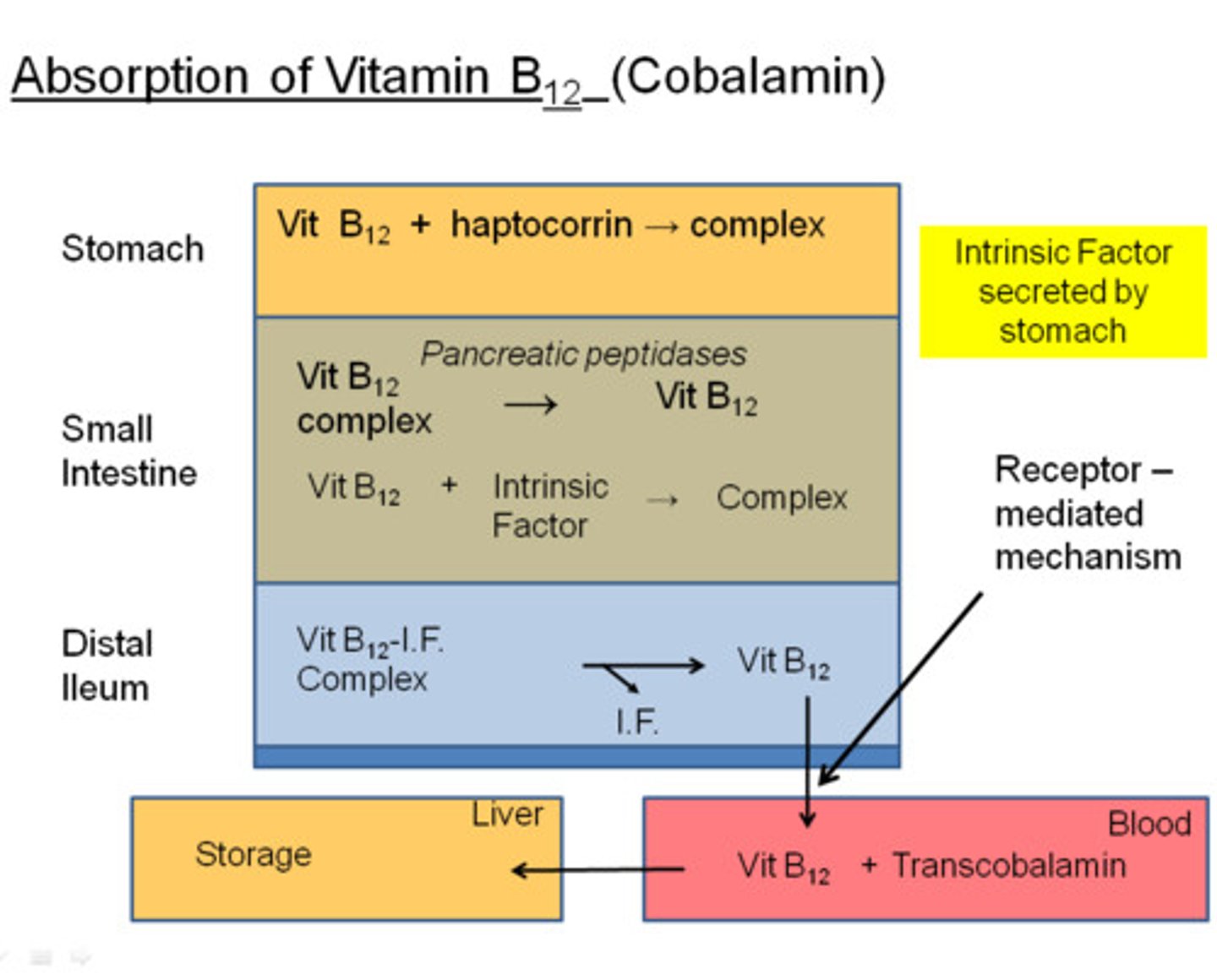
Absorption of B12
- dietary= cobalamin (CBL)
- binds to R protein (haptocorrin) from salivary glands
- trypsin cleaves and bind to intrinsic factor
- released from IF, and transported as transcobalamin (TC)
Malabsorption of B12
- can't separate from food
- can't cleave from R-protein
- lack intrinsic factor
Bacteria
- H. pylori infection= parietal cells destroyed
- D. latum= can split CBL from IF
Pernicious Anemia
autoimmune impaired absorption of vitamin B12 from IF deficiency

Pernicious antibodies
- blocking= block b12 from IF= specific
- against parietal cell
screens for megaloblastic
- CBC
- Retic count
- WBC differential
- Serum bili
- LD
CBC for megaloblastic i
- pancytopenia
- decreased hgb and hct
- MCV= 100-150 fL
- reticulopenia
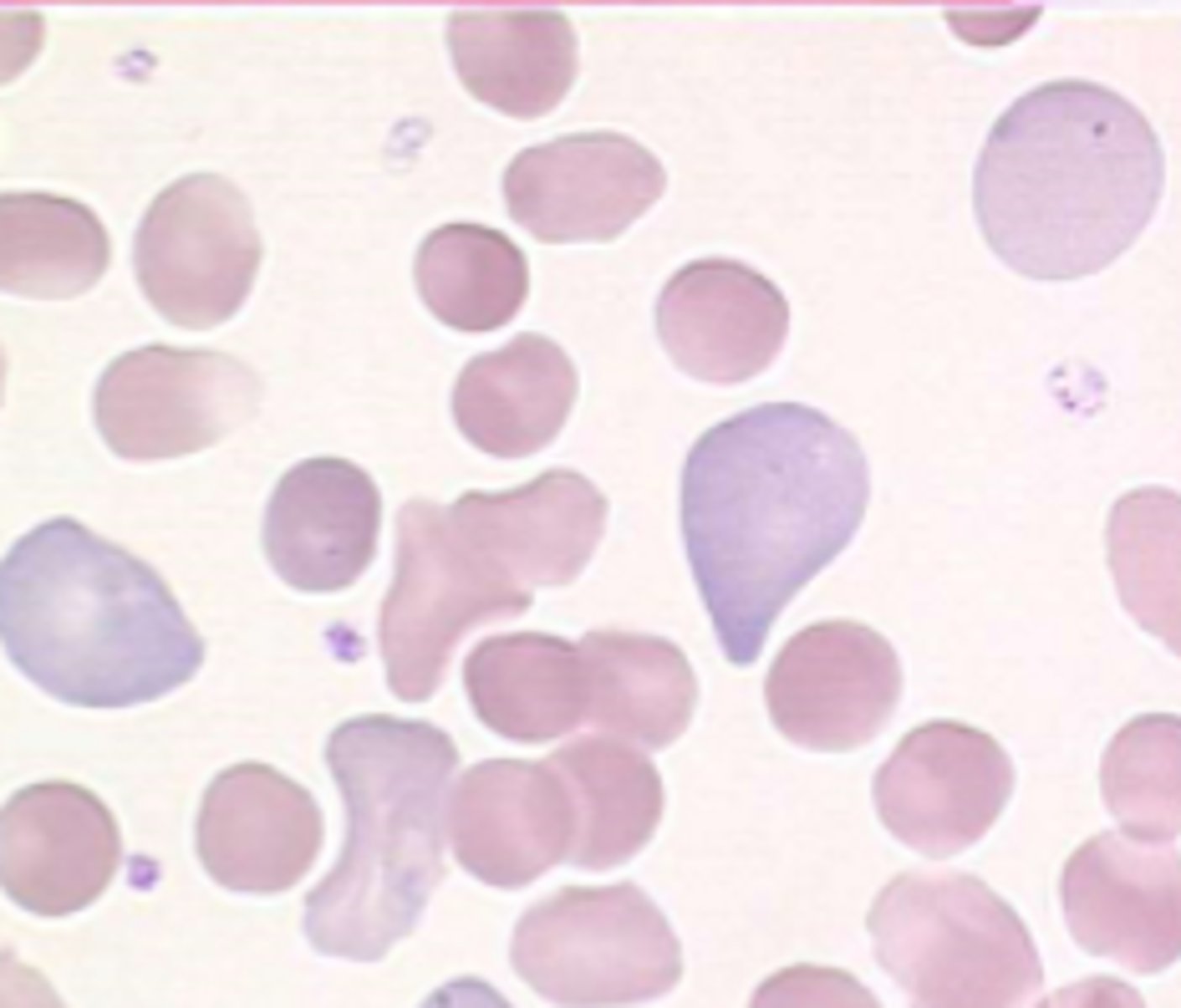
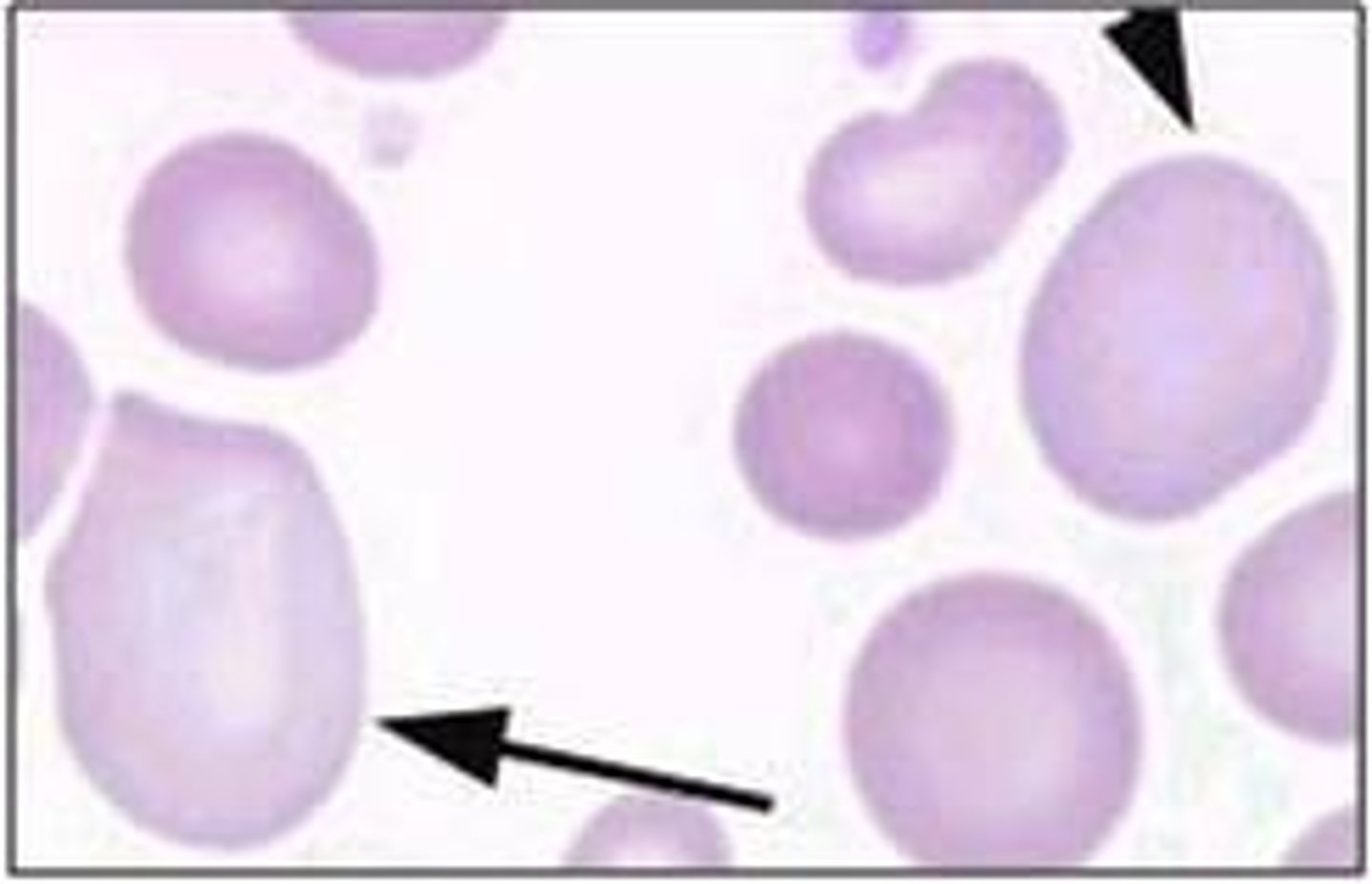
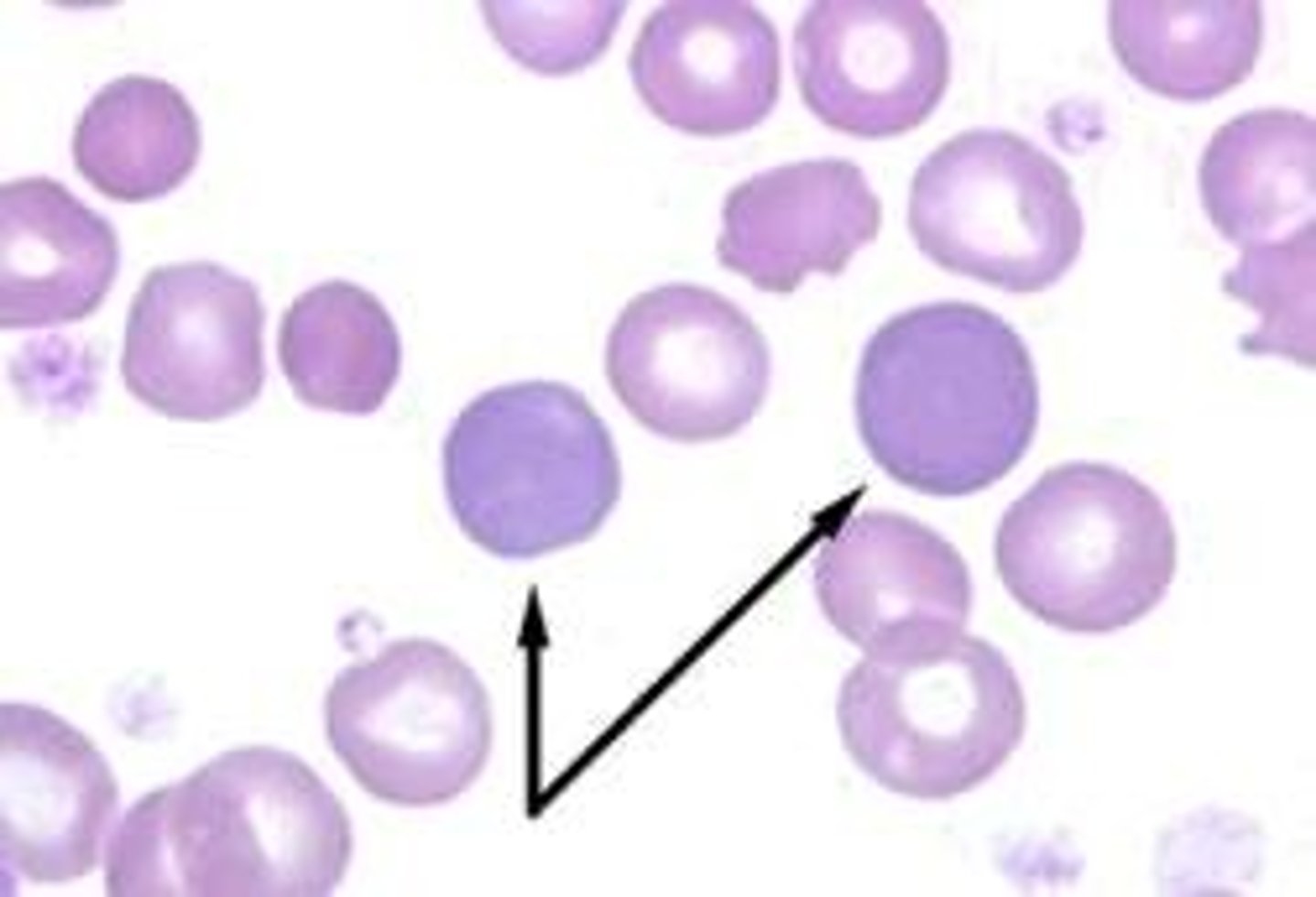
PB for megaloblastic
- oval macrocytes
- hypersegmented neutrophils
- aniso and poikilo-cytosis
- RBC inclusions
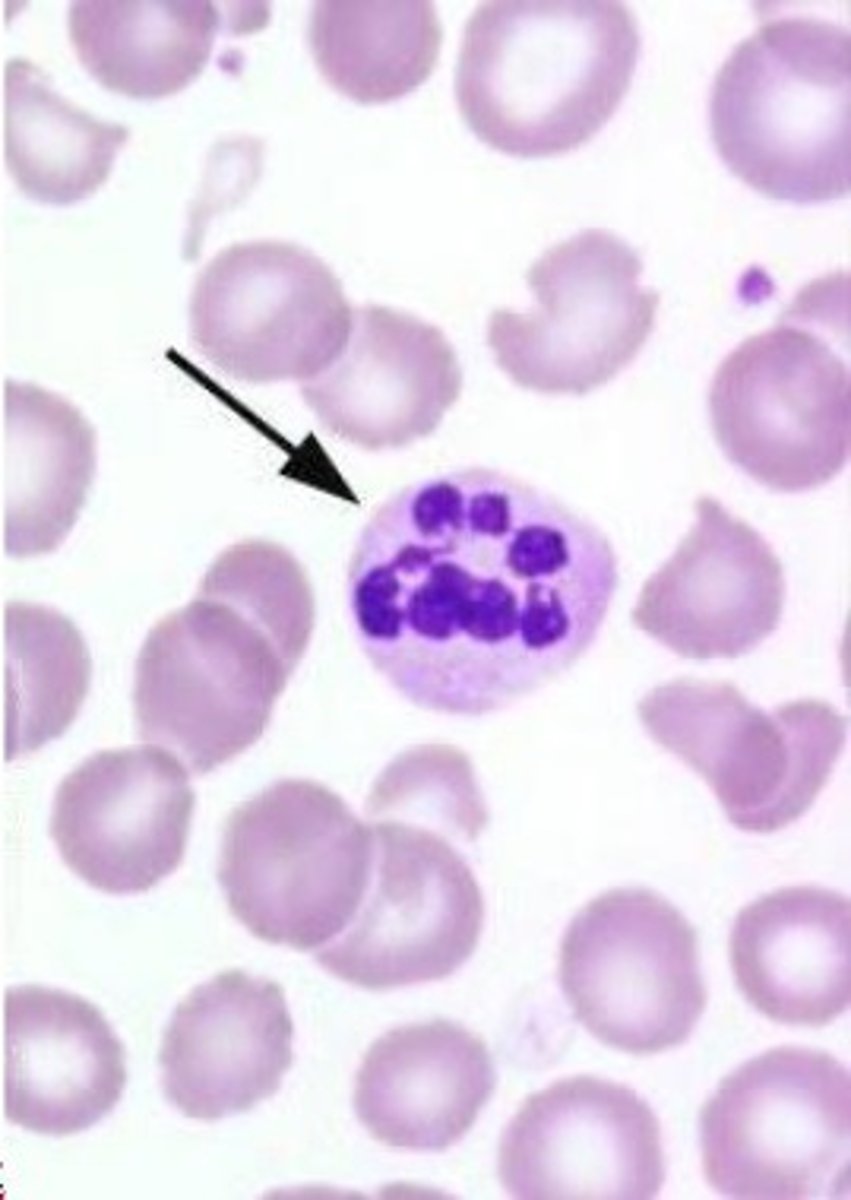
Reporting hypersegmentation
- 5 five-lobed neutrophils per 100 WBCs
- 1 six lobed
- should be >3
RBC life span is
short
- 27 - 75 days
- hemolysis
Chemistry tests in megaloblastic
- increase= bilirubin, urobilinogen, LDH are elevated
- Haptoglobin decreased
- Iron, ferritin, and EPO may be elevate
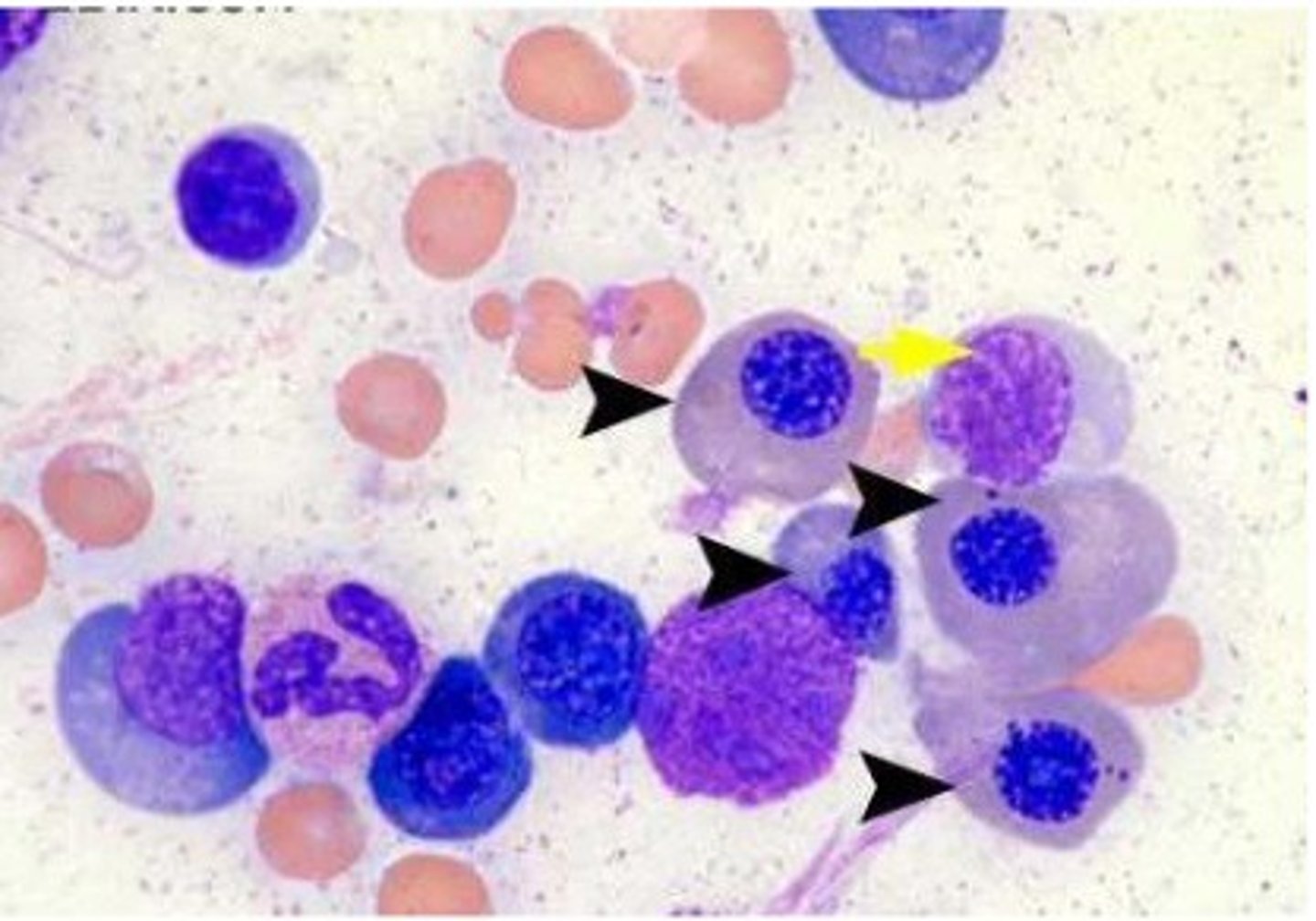
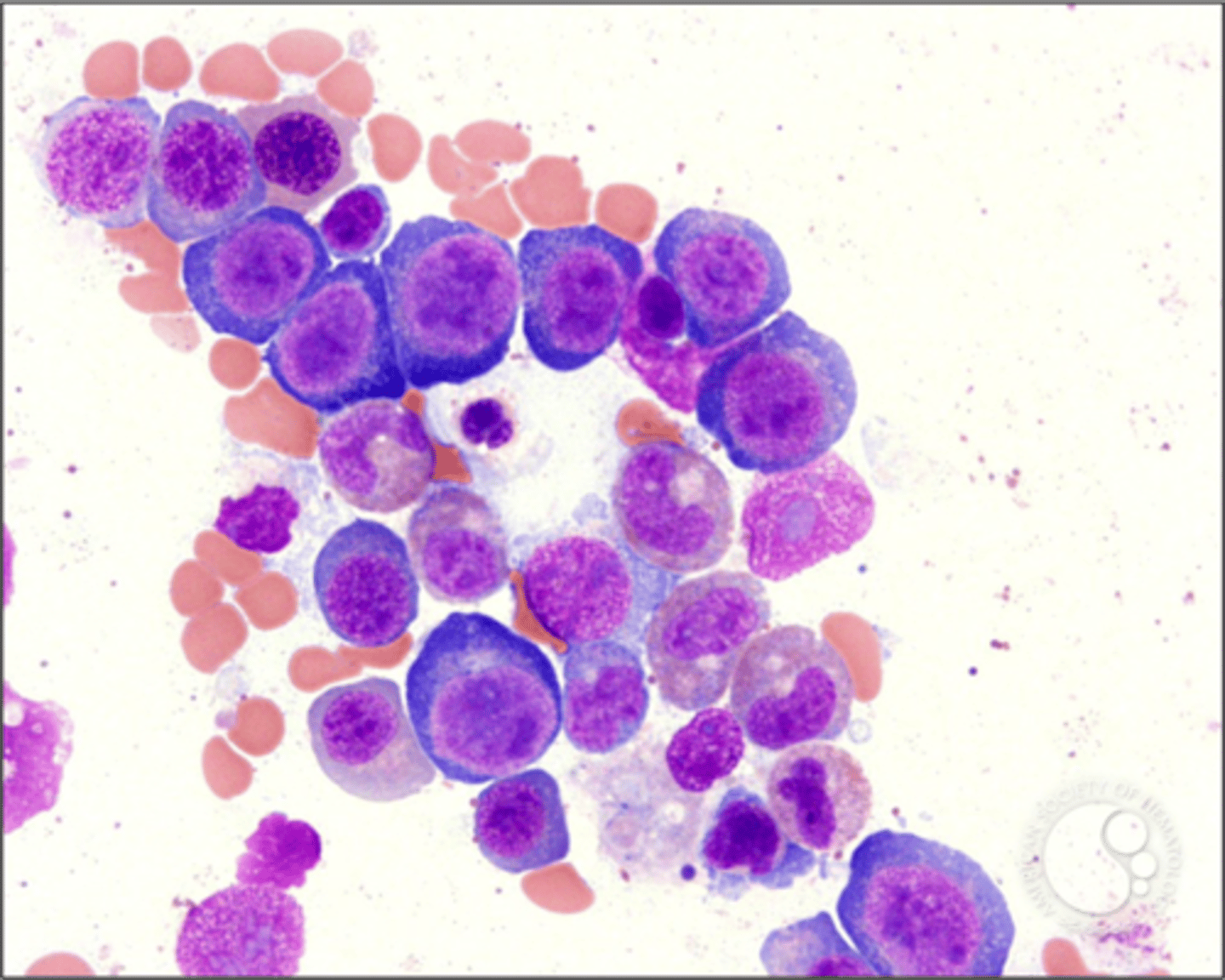
Bone marrow megaloblastic
- hypercellular
- ME ratio decreased (1:1, 1:3)
- nucleus doesn't mature with cytoplasm
- bands and giant metamyelocytes
- megakaryocytes= hypogranulation and hyperseg
diagnosis of megaloblastic
- Vitamin B12 levels
- Serum or RBC folate
- Methylmalonic acid (MMA) (increase in B12 def)
- Homocysteine levels (increase in both vitamin B12 and folate def)
megaloblastic treatment
treatment folate and B12 deficiencies
Macrocytic Non-megaloblastic Anemias
Macrocytosis without impairment of DNA synthesis
- liver disease
- alcoholism
alcohol effects
- Folate deficiency dietary decreased intake
- Reticulocytosis
- Bleeding, Hemolysis, Vacuolization of RBC
Liver disease lab
- macrocytes <115 fL
- target cells and acanthocytes (lipids)
- macrocytosis from lipids