ANSC 300 Lactation
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
32 Terms
Mammary Gland
evolved from modified secretory exocrine skin glands that have evolved to produce milk
nourishes neonate by providing nutrients and immunity (colostrum)
is a reproductive organ that develops over time from prenatal period through pregnancy, parturition, and beyond
Monotremes
early mammals simply secreted milk on to their skin
egg laying
Marsupials
developed teats, but still have relatively less developed mammary systems
metatherians
Eutherians
fully developed mammary gland producing complex milk
placental
Stages of Mammary Gland Development
Mammogenesis
Lactogenesis
Galactopoiesis
Involution
Mammogenesis (STAGE 1)
growth of gland
prenatal
repubertal
puberty
pregnancy
Lactogenesis (STAGE 2)
transition from pregnancy to lactation
parturition
initiation of lactation is tied to changes in hormones occuring at the end of pregnancy
rapid onset from no milk production to high milk production in a matter of hrs/day
E2/P4 are not enough to induce milk production, need other hormones
Galactopoiesis (STAGE 3)
maintenance of lactation
suckling, nursing
hormonal requirements for maintenance of lactation includes thyroid hormone, prolactin, cortisol, GH
removal of milk from the mammary gland is required for continuous milk synthesis
Involution (STAGE 4)
transition to non-lactating period
dry period, weaning
Mammary Growth
Primary Bud: grows slowly in response to insulin
Puberty: cyclic changes in estrogen and progesterone promotes ductal growth, branching and lobule-alveolar development
Cortisol synergizes with E2/P4 and prolactin
Progesterone blocks milk synthesis before parturition
Prenatal Development
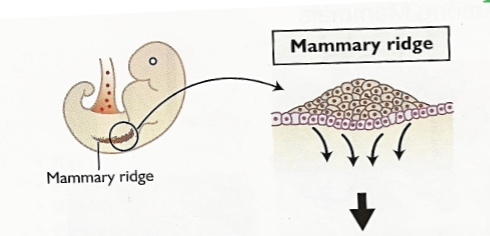
Mammary Ridges
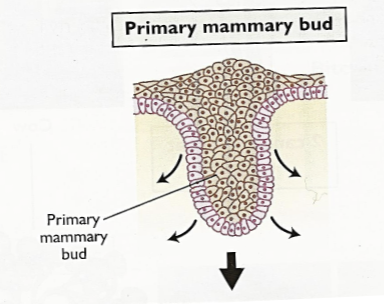
Primary Mammary Bud
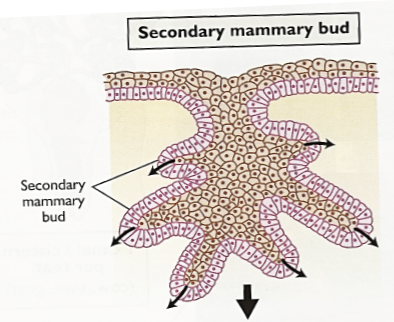
Secondary Mammary Bud
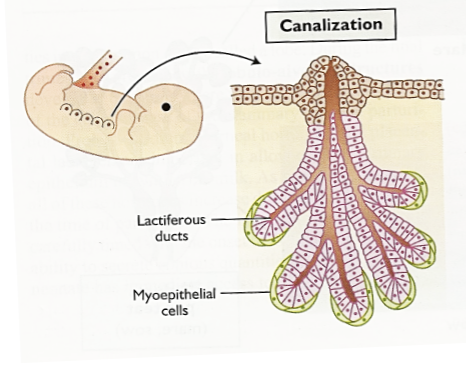
Canalization
Mammary Ridges (STAGE 1)
are thickened epidermal tissue that give rise to the mammary gland
forms from axillary to inguinal regions
number and placement of glands is species specific
Primary Mammary Bud (STAGE 2)
the thickened epidermal tissue begins to develop inward and penetrate into the mesenchyme (dermis)
Secondary Mammary Bud (STAGE 3)
the primary mammary bud begins to send out branches that further penetrate into the dermis
Canalization (STAGE 4)
the fingerlike secondary buds begin to lengthen and branch out. Finally, they begin to form canals that will form the duct system of the gland. Myoepithelial cells surround the terminal portions of the developing gland.
Puberty
ovarian activity — increased estrogen and progesterone
estrogen stimulates ductal growth and branching
progesterone stimulates alveolar development and ends bud formation
multiple reproductive cycles cause further ductal growth, elongation, branching, and ends bud formation
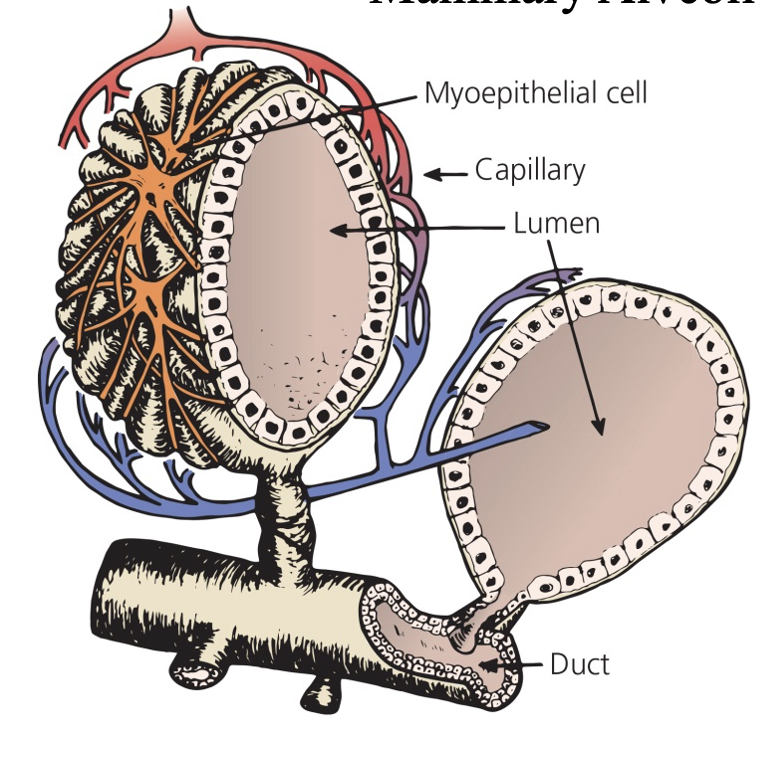
Mammary Alveoli
secretory epithelium
apical and basal side
synthesizes milk components (protein, fat, sugar)
secretes into lumen of alveoli
water followed by osmosis
myoepithelial cells contract to squeeze milk into ducts
Why is Timing of Parturition and Lactation Important?
there needs to be enough milk in order to feed neonate immediately after parturition
surges in hormones keeps lactation stable
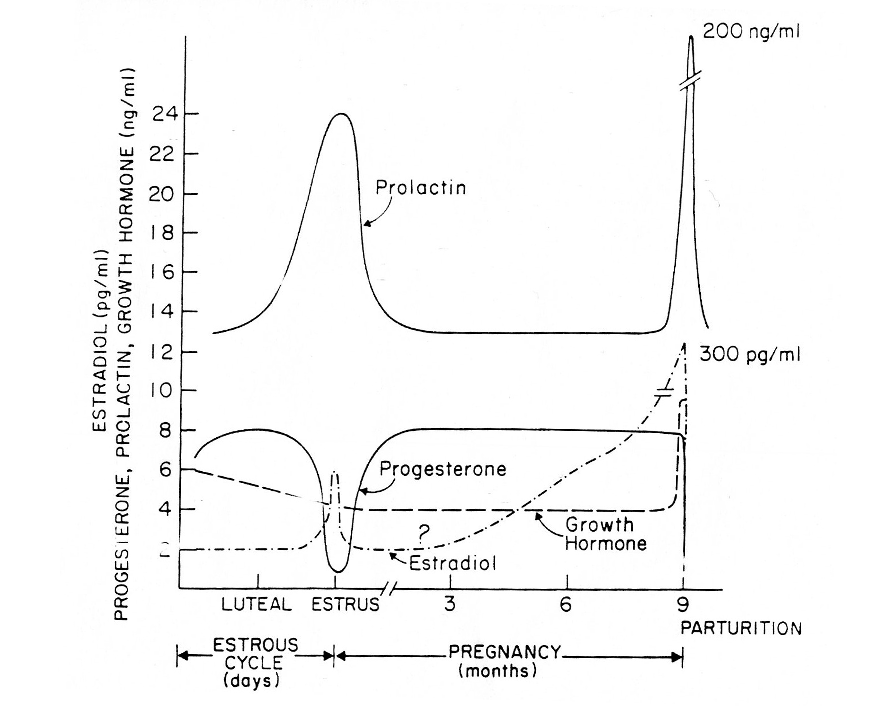
Profiles of Various Hormones During Pregnancy
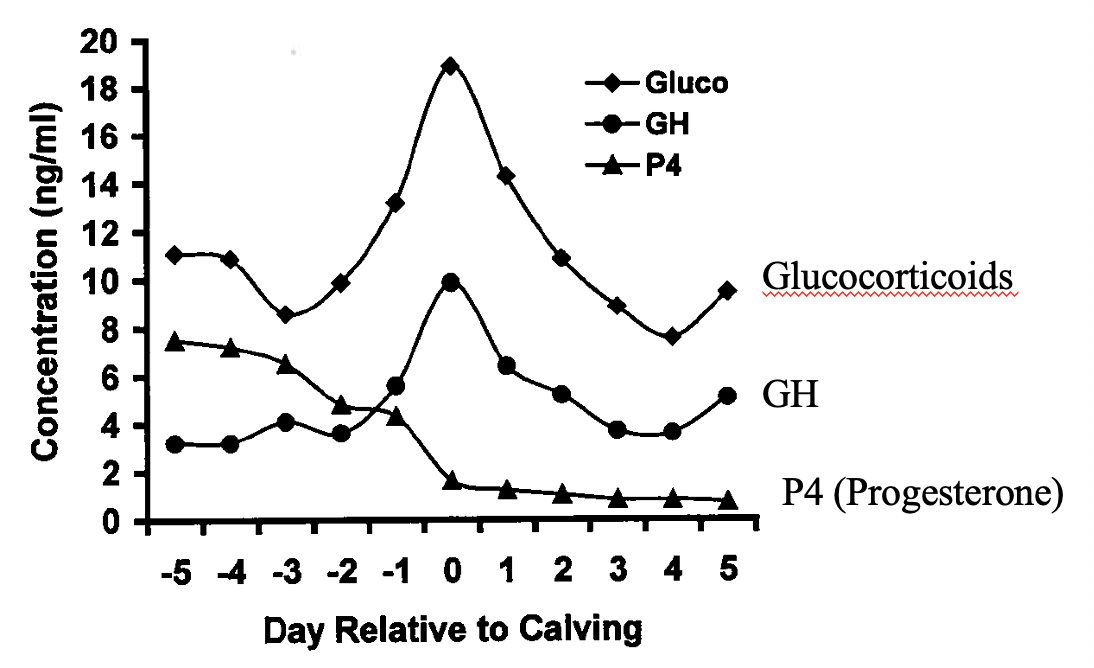
Endocrine Changes Near Parturition
Progesterone (LACTOGENESIS)
P4 blocks induction of PRL and GR receptors on mammary gland cells
blocks transcription of a-lactablbumin and casein mRNA in mammary cells
blocks protein synthesis of casein, a-lactalbumin and lactose synthesis
Prolactin (LACTOGENESIS)
removal of pituitary gland in pregnant women or animal leads to a marked decrease in the subsequent lactation
blocking prolactin secretion before parturition severely reduces milk yield
prolactin synergizes with cortisol to induce lactation
when P4 secretion is blocked after mid-pregnancy the minimal hormone requirement for initiation of milk secretion is cortisol and prolactin
stimulated by suckling: important in nonruminants
Cortisol and Prolactin are _______
synergistic
____ and ____ have No Direct Mammary Actions.
LH and FSH
Thyroid Hormone
ablation results in significant reduction in milk production
supplementing thyroid hormone will:
increase milk production by 15-20%
increase metabolic rate, heart rate, etc.
only effective for a limited time
Why?
idk
Growth Hormone
GH has no lactogenic activity in vitro
no evidence of GH-R in mammary cells
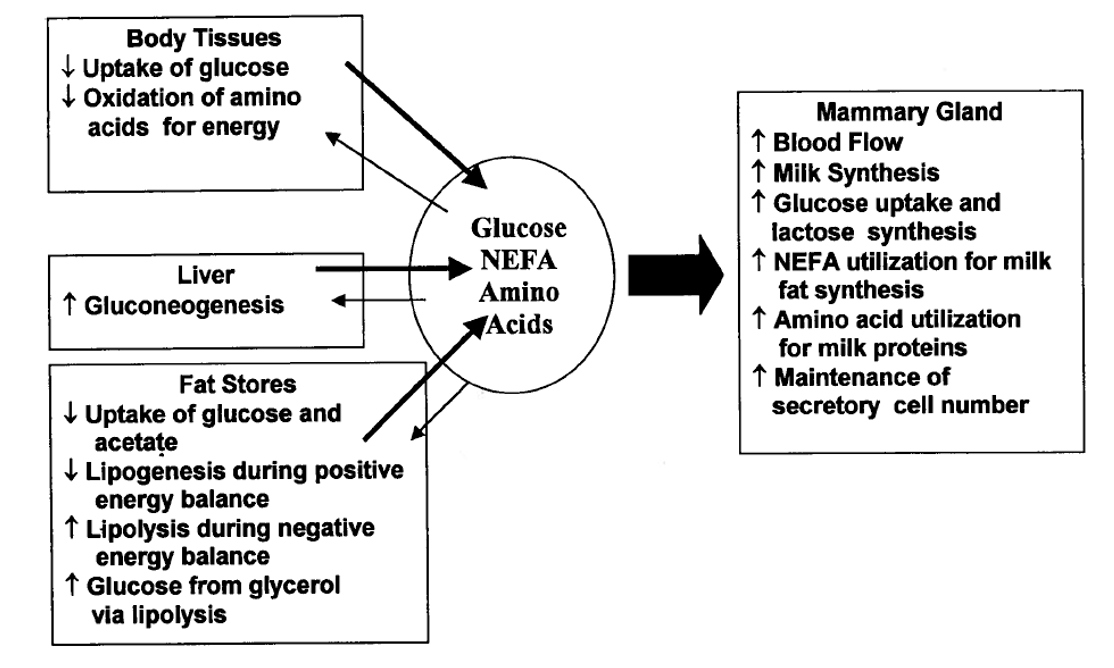
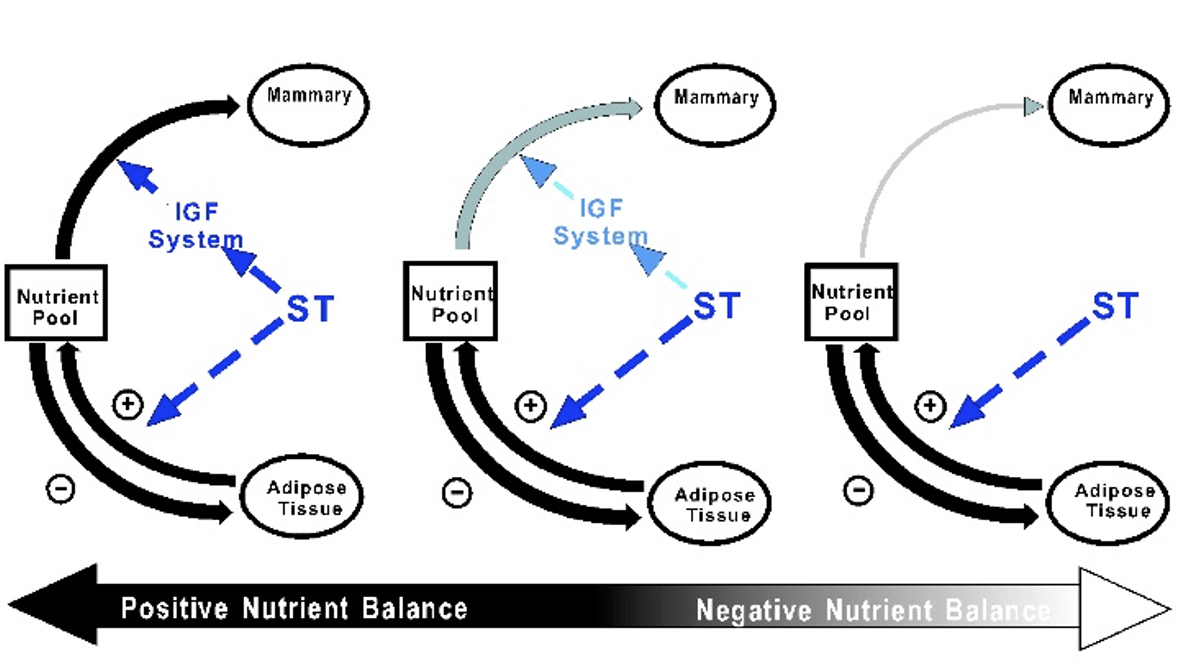
GH enhances gluconeogenesis and suppresses fat synthesis in adipose tissue to support lactogenesis
acts indirectly through induction of IGF-1 and modulation of metabolism
GH Orchestrates the Metabolism of Body Tissues
coordination involves many tissue and physiological processes
coordination involves all nutrients classes
carbohydrate, lipid, protein, and minerals
Metabolic Effects of GH
Effect of Nutrition on IGF-1 Secretion to bST
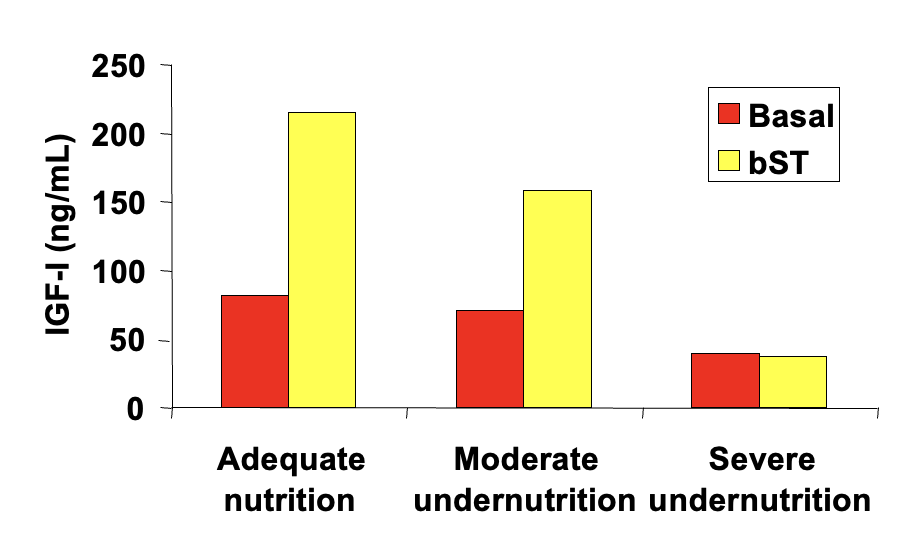
Nutritional Status Modulates Response to GH
Insulin-Like Growth Factor-1
70 amino acid peptide with 50-60% sequence homology to insulin and 76% homology to IGF-II (human)
human IGF-1 is identical to bovine IGF-1
produced in many tissues of the body
necessary for normal growth and development
high levels have been associated with some cancers
no difference in rbST and non-bST treated cows
rbST and Milk Safety
protein hormones inactive when taken orally
rbST is species-specific
no composition difference between rbST and non-rbST milk
extensively researched in >3,000 scientific studies
human safety declared by medical and health associations, scientific societies, and government regulatory agencies