Abnormal Fetal Chest, Abdomen, and Pelvis
1/126
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
127 Terms
Gastroschisis
Membrane-free ventral wall defect with protrusion of abdominal contents lateral to umbilical cord
Hirschsprung disease
Congenital lack of nerves in the colon
What does hirschsprung disease cause?
Fecal impaction and a megacolon
Hydrops
Accumulation of fluid in fetal tissue, peritoneum, and pleural cavities
Meconium ileus
Bowel obstructed by mucus
Midgut volvulus
Bowel obstructed due to bowel twisting
Congenital clavicle anomalies can include absent or short clavicles that are associated with:
Cleidocranial Dysplasia
Holt-Oram Syndrome
Cleidocranial Dysplasia
Abnormal fontanel closure
protruding mandible
frontal bossing
hypertelorism
cleft palate
short stature
scoliosis
Holt-Oram Syndrome
Autosomal dominant
Thumb and clavicle absence
UE anomalies
CHD
Pleural Effusion AKA:
Hydrothorax
Pleural Effusion
Accumulation of fluid in pleural cavity
What is the most common type of hydrothorax?
Chylothorax
Chylothorax
Rt sided lymph fluid collection
Polyhydramnios due to esophageal compression
Immune cause of pleural effusion:
Rh hemolytic disease
Non-immune causes of pleural effusion:
CHF
CHromosoma anomaly
CCAM/CPAM Bronchopulmonary sequestration
CDH
hamartoma
PV atresia
lymphangiectasis
Pleural Effusion U/S appearance:
lung “floats” in fluid
possible shift of mediastinal structures
compression of heart
diaphragm inversion
lung compression
leads to pulmonary hypoplasia

What is the prognosis of pleural effusion?
poor w/ hydrops
50% mortality d/t pulmonary hypoplasia
What treatment can help pleural effusion prognosis?
insertion of thoracoamniotic shunts → allows for lung growth in 2nd trimester (must be placed by 32 wks)
Pulmonary Hypoplasia
Decreased overall lung size → small inadequate underdeveloped lungs
Causes of pulmonary hypoplasia:
prolonged oligohydramnios
small thorax (constriction)
severe FGR
PROM
kidney malformations
Intra-thoracic masses
CDH
cardiac defects
skeletal dysplasia
chromosomal anomalies
Pulmonary hypoplasia prognosis:
Poor → 80% mortality rate after birth
How do we diagnose pulmonary hypoplasia?
Thoracic measurements & lung volumes that measure <5%ile
Pulmonary Sequestration
Extra lobe of the lung separated from the normal tracheobronchial tree
Non-functional tissue with systemic blood flow (thoracic aorta & IVC)
Pulmonary Sequestration signs / appearance:
dense solid mass usually in lower lung lobes
can resemble CCAM / CPAM
hypoplastic lung on affected side
hydrops
what are findings associated with pulmonary sequestration?
CDF
GI & Lung anomalies (hypoplasia)
Intralobar Pulmonary Sequestration
Present in pleural lung sac
spherical in shape
favorable prognosis
Extralobar Pulmonary Sequestration
inferior border of lung has its own pleural sac
left sided more common
cone / triangular shape
can be located below diaphragm
poor prognosis → hydrops
CCAM / CPAM
Congenital Cystic Adenomatoid Malformation
Cystic Pulmonary Airway Malformation (CPAM)
CCAM / CPAM
Multicystic mass within lung made up of primitive lung tissue and bronchial-type structures

What causes CCAM?
Bronchopulmonary foregut malformation
A bronchopulmonary foregut malformation is described as:
An embryologic alteration in lung development at approx 8 weeks GA
What is CPAM assictaed with?
can involve ≥1 lung lobes
rarely bilateral
mass can communicate w/ bronchial tree
Type 1 CCAM / CPAM
1 or more large macrocystic cysts (>2 and up to 10 cm)
replace normal lung tissue
favorable outcome
Type 2 CCAM / CPAM
Multiple cysts <1cm
macrocystic w/ microcystic component
poor prognosis
Type 2 CCAM is associated with:
chromosomal anomaly
renal agenesis
pulmonary anomalies
CDH
Type 3 CCAM / CPAM
microcystic, large, noncystic lesion
entire lobe is echogenic
poor prognosis
Type 3 CCAM associated findings:
lung compresssion
hydrops
polyhydramnios
Abdominal Ascites
fluid in the peritoneum
ALWAYS abnormal
commonly seen w/ hydrops but can be isolated

The potential causes of abdominal ascites are:
bowel perforation
urinary ascites from bladder outlet obstruction
Congenital Diaphragmatic Hernia (CDH)
herniation of abdominal viscera into chest
rarely bilateral
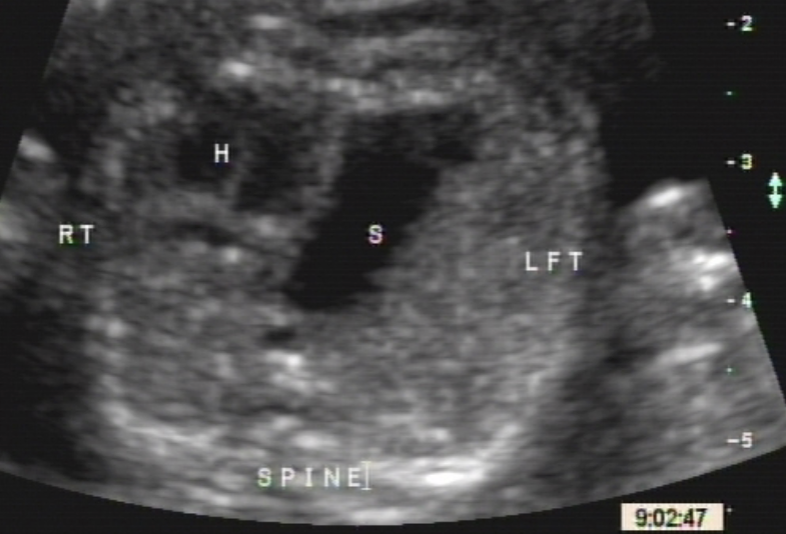
CDH of Left Side
90% posterior/lateral left side
allows left sided organs to enter chest thru opening
2/3 have portion of liver herniated = poor prognosis
How does left-sided CDH present?
heart shifted to right
small bowel and colon can be present (collapsed difficult to see)
small compressed lungs
CDH of Right Side
Anterior / Medial through the Foramen of Morgagni
Can communicate w/ pericardial sac
Right sided CDH appears on ultrasound as:
liver in chest
collapsed bowel
heart located to the far left of chest
stomach below diaphragm but located to right
gallbladder may be visualized → appears as thoracic cyst
What are the complications associated with CDH?
pulmonary hypoplasia
PHTN d/t thick hypertrophied PA’s
CDH prognosis:
associated w/ Trisomy 18 and 21
20% association w/ cardiac defects
30% CNS malformations
renal anomalies
vertebral defects
facial clefts
At 20 weeks or less, the renal pelvis should measure:
5mm or less
At 20-30 weeks, the renal pelvis should measure:
8mm or less
From 30 weeks to term, the renal pelvis should measure:
10mm or less
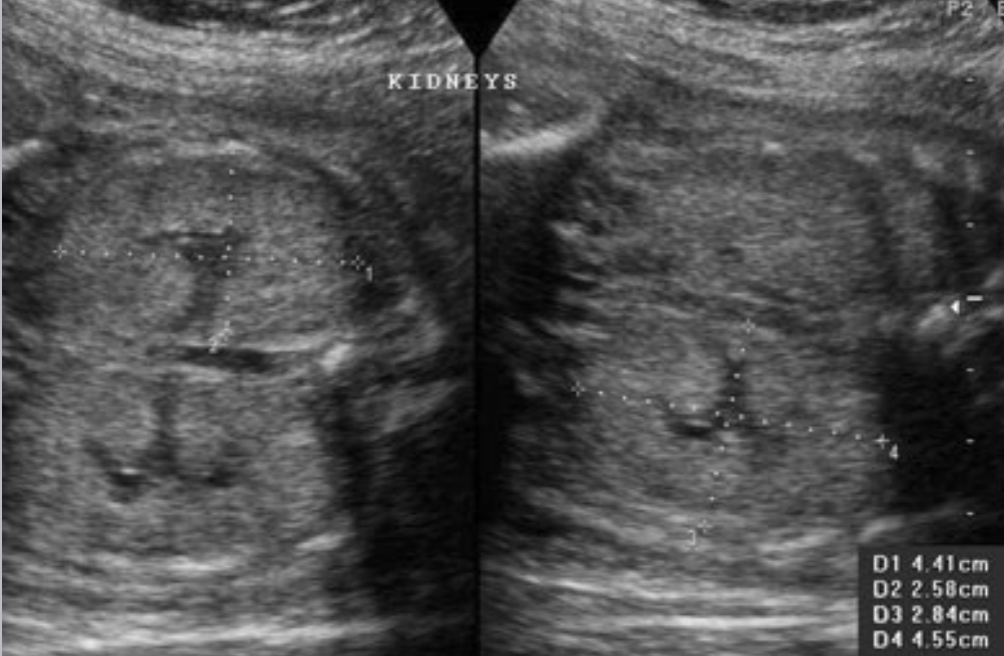
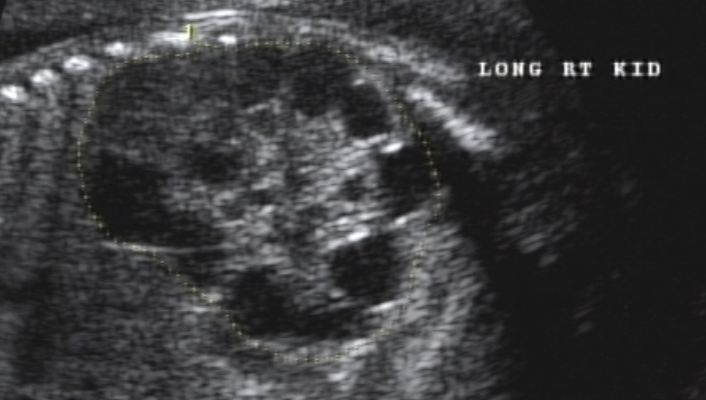
Hydronephrosis
Occurs due to blockage at some level in urinary system
urine backs up into kidney
How does hydronephrosis appear on ultrasound?
dilated renal pelvis communicates w/ calices
pyelectasis = renal pelvis 5-9 mm
hydro = renal pelvis >10-15 mm
unilateral or bilateral
What is the most common fetal anomaly?
hydronephrosis
Renal Agenesis
Congenital absence of one or both kidneys (commonly males)
Renal Agenesis appears on ultrasound as:
kidneys / bladder absent on US
severe oligohydramnios or anhydramnios
Check for Renal Artery flow w/ PD
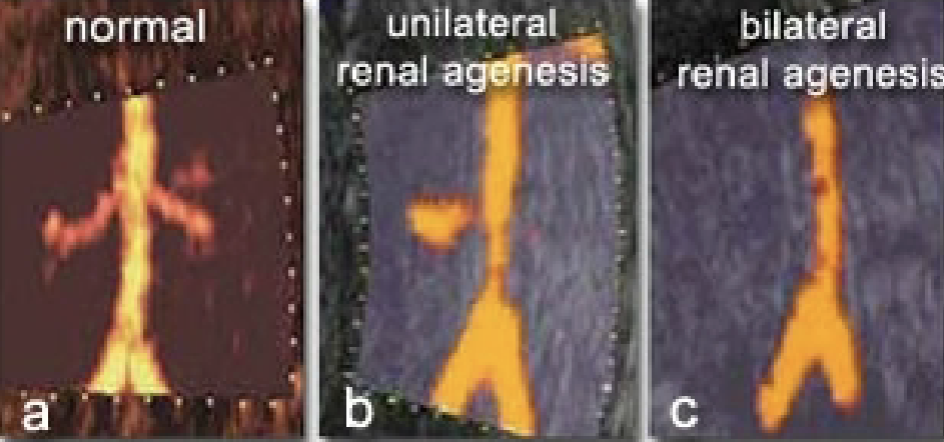
What is the prognosis for bilateral renal Agenesis?
Incompatible with life
Unilateral Renal Agenesis
more common
Present may be larger than normal
Usually normal AFV
What organ takes the place of the absent kidney in the fossa?
Adrenal gland
Associated findings of Renal Agenesis:
cardiac defects
Sirenomelia
Absent radius and fibula
Digit anomalies
Sacral Agenesis
CDH
Cleft palate
Hydrocephalus
Menigocele
Cephalocele
Holoprosencephaly
Microcephaly
Duodenal atresia
Imperforate anusu
Tracheoesophogeal fistula
Omphalocele
Why may renal Agenesis associated anomalies be hard to visualize?
Due to anhydramnios
Sirenomelia
mermaid syndrome
Lower extremities fused together
Large association w/ renal Agenesis
Potters Syndrome AKA:
Potter’s Sequence
Oligohydramnios sequence
Potters Syndrome
Describes the typical appearance of fetuses who have oligohydramnios or anhydramnios secondary to renal anomalies
Potters Syndrome is associated with:
renal Agenesis
Oligohydramnios
Pulmonary hypoplasia
Abnormal faces
Malformed hands and feet
What are the four types of Cystic Dysplastic Kidney Disease?
Infantile Polycystic Kidney Disease
Multicystic Dysplastic Kidney ( MDK)
Autosomal Dominant Polycystic Kidney Disease
Cystic Renal Dysplasia
What are the most common types of Cystic Dysplastic Kidney Disease?
Types II and IV
Infantile Polycystic Kidneys (IPKD)
autosomal recessive
Symmetric kidney enlargement
Most severe cases = renal failure
Infantile Polycystic Kidney U/S appearance:
echogenic parenchyma
Small / absent bladder and oligohydramnios
Kidneys become so large they fill entire abdomen
What is the most common form of cystic renal disease in childhood?
Multicystic Dysplastic Kidneys
Multicystic Dysplastic Kidneys
Multiple smooth walled non-functional, non-communicating cysts varying in size and number
Multicystic Dysplastic Kidneys US appearance:
renal tissue replaced by cysts
Renal A may be hypoplasia or absent
Bilateral Multicystic = oligohydramnios and absent bladder = lethal
Unilateral = normal AFV and bladder
Adult Dominant PCKD
Bilateral cystic dilation of the nephrons
autosomal dominant
What are the signs and appearance of adult dominant PCKD?
enlarged echogenic kidneys → usually no cysts
Bladder WNL
Normal AFV
Almost 100% bilateral
Obstructive Cystic Dysplasia
Renal dysplasia secondary to obstruction in the first or early second trimester
Obstructive Cystic Dysplasia U/S appearance:
Echogenic kidneys with cortical cysts
Bilateral
Keyhole bladder
Hydronephrosis
thick-walled bladder
severe oligohydramnios
Utteropelvic Junction (UPJ) Obstruction
Unilateral
Normal AFV
Urinoma, urinary ascites
What is the most common cause of hydronephrosis?
UPJ obstruction
Uterovescical Junction (UVJ) Obstruction
Dilation of lower end of the ureter
stenotic ureteral valve
Dilated renal pelvis & tortuous dilated ureter
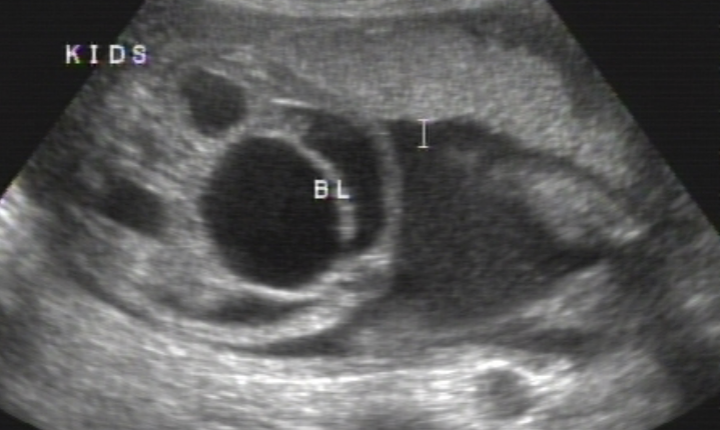
Posterior Urethral Valves (PUV’s)
Bladder outlet obstruction caused by membrane in posterior urethra
MALES
What is the ultrasound appearance of PUV’s?
Thick walled bladder
Dilated posterior urethra
keyhole sign
hydrureter
hydronephrosis
oligohydramnios
hypoplastic lungs

Prune Belly Syndrome AKA’s:
Urethral Obstruction Malformation complex
Eagle-Barret Syndrome
Triad Syndrome
Prune-Belly Syndrome
The triad of urinary tract dilation, a deficiency of the abdominal wall musculature, and a failure of testicular descent
What are findings associated with Prune Belly Syndrome?
distended abdomen
oligohydramnios
mild-severe hydronephrosis
ascites
hypoplastic lungs
cryptorchidism
agenesis of abd wall musculature
mega ureter
bladder outlet obstruction
Situs Invertus
Can be total or partial reversal of thoracic and abdominal organs
Partial Situs Invertus
More severe than total
Stomach may or may not be reversed
What are the two types of partial situs invertus?
Asplenia
Polysplenia
Partial Situs Inversus Asplenia
Normal position of Liver and Gallbladder
Absent spleen
Displaced Aorta and IVC
99% have cardiac anomalies
90-95% mortality
What are the cardiac defects associated with Partial Situs Invertus Asplenia?
Endocardial cushion defects
Hypoplastic Left Heart
TOGV
Partial Situs Inversus Polysplenia
More than one spleen
Transposition (inversion) of liver and stomach
No gallbladder
IVC disruption
What are associated findings of Partial Situs Inversus Polysplenia?
Heart blocks
90% have cardiac anomalies
80% mortality rate
Total Situs Inversus
Usually normal outcome
Rt sided heart axis and aorta
transposition of liver, stomach, and spleen
left sided GB
What is Total Situs Inversus associated with?
20% have Kartageners Syndrome (affects lungs)
GI, GU anomalies and NTD
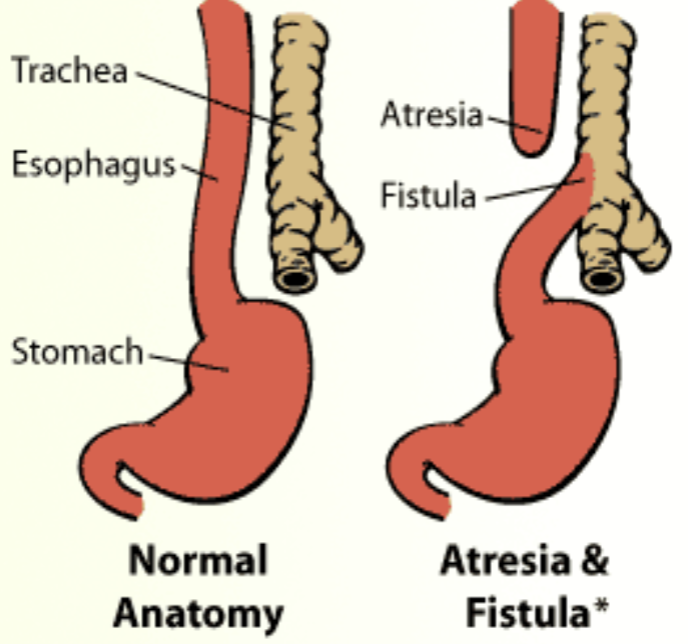
Esophogeal Atresia
Congenital blockage of esophagus
Esophageal Atresia is associated with:
Polyhydramnios & absent stomach
50% have fistula
50-70% have anorectal atresia
40% IUGR
Associated with Trisomy 18 and 21
What are the VACTERALS associated with esophageal atresia?
Vertebral defects
Anal atresia
Cardiac defects
Tracheo-Esophageal fistual
Renal anomalies
Limb and Spinal anomalies
Duodenal Atresia
Blockage of duodenal lumen by membrane
Prohibits passage of swallowed amnionic fluid
Fluid backs up in duodenum and stomach
Double Bubble Sign
What congenital disorder is associated with duodenal atresia?
Trisomy 21
Duodenal Atresia U/S appearance:
2 anechoic structures in upper abdomen
polyhydramnios
cardiovascular anomalies
horseshoe kidneys, ectopic kidneys
Imperforate anus
Atresia of small bowel
Esophageal atresia
Symmetric FGR
AFP in amniotic fluid d/t ↓ swallowing

What is the earlist manifestation of cystic fibrosis in some patients?
Meconium Ileus
Meconium Ileus
Small bowel disorder → presence of thick meconium
occurs in newborns w/ cystic fibrosis
What is meconeum ileus associated with in newborns w/ cystic fibrosis?
pancreatic disease
respiratory problems