W9 PRE Thyroid gland
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
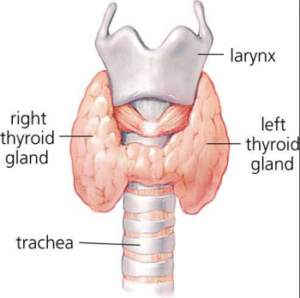
Thyroid gland location
Over trachea, caudal to/level of larynx (two lobes)
Made of follicles, within connective tissue capsule
Parafollicular cells (C cells)
Between follicles and produce calcitonin (regulate blood calcium)
Thyroid gland hormones
Throxine T4
Triiodothyroxine T3
Calcitonin (Thyrocalcitonin)
T4 / T3
Regulate metabolic rate
Release of T4 control
Thyrotropin-releasing hormone (hypothalamus)
Thyroid-stimulating hormone (pituitary gland)
T4 to T3
Act on all cells; essential for normal growth
Effect skin, skeleton, cardiovascular system, neurological and reproductive
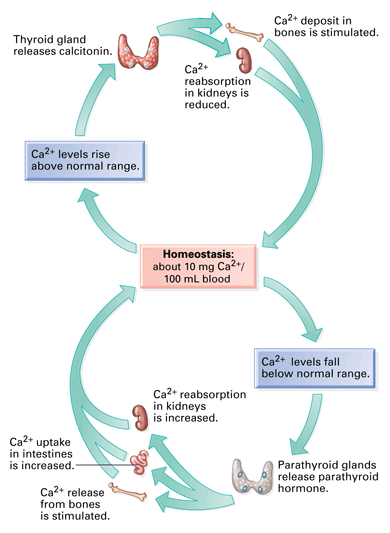
Calcitonin (Thyrocalcitonin)
Decrease blood calcium by slowing resorption from bone
Decreases calcium reabsorption from GI tract, increases excretion through urine
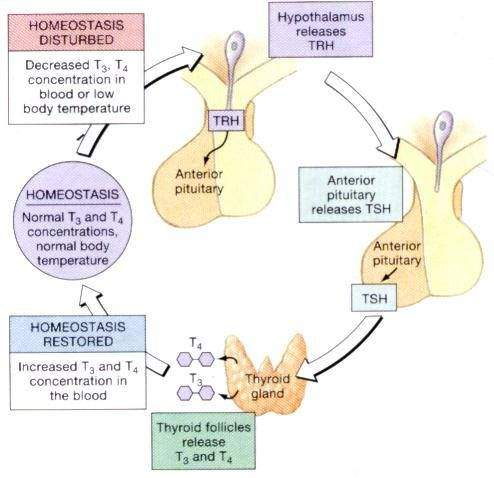
Release of T4 into bloodstream
Hypothalamus produces Thyrotropin releasing hormone (TRH)
Pituitary gland - stimulates secretion of Thyroid stimulating hormone (TSH)
Thyroid - stimulates Thyroxine T4 release into blood
Feedback signal: Normal levels - body decreases hormone amount produced through negative feedback
Calcium
Functions in nerve transmission, blood clotting and muscle contraction.
High level Calcium
Calcium deposites within kidney
Heart rhythm abnormalities
Neurological disturbances
Calcitonin negative feedback mechanism
And parathyroid hormone ensures blood level remain appropriate
Blood Calcium:Phosphorus
1-1.5 Calcium : 1 Phosphorus
T4 to T3 Conversion
Thyroid-releasing hormone (TRH) released by hypothalamus to stimulate pituitary gland to release thyroid-stimulating hormone (TSH)
Thyroid gland releases T4, converted into T3 within tissues
T3 (active hormone form) sets metabolic rate
Hypothyroidism
Lack of thyroxine thf T3, due to atrophy/lymphocytic infiltration of thyroid gland
Primary - (excess TSH) destruction of thyroid gland, either lymphocytic thyroiditis (immune disease) or idiopathic
Secondary - (Lack TSH), Rarely pituitary tumour prevent TSH production
Hypothyroidism signs
(reduced metabolic rate, slow tissue regeneration, healing)
Lethargy, exercise intolerance
Obesity
Bradycardia
Hypothermia
Dermatological condition e.g. alopecia, seborrhoea
Hyperpigmentation, pyoderma
Hypothyroidism diagnosis
CE
Blood test Total T4, free T4 and TSH
Low T4
High TSH
Low fT4
Hypothyroidism treatment
Lifelong medication (supplement thyroxine with synthetic T4)
Levothyroxine - Soloxine, Thyforon

Thyroxine medications
Pregnant handle with caution
Wear gloves, washing hand after administering/handling
Thyforon
synthetic levothyroxine increase T4 levels
Per os
Overdosing hyperthyroidism, weight loss, hyperactivity, excitability, panting, tachycardia, polydipsia, pu/pp
Split tablets stored blister pack, Wash hands after administration. Pregnant care
Hyperthyroidism signs
Accelerated metabolism - agression, overgroom, hyperactive
Polyphagia, weight loss emaciatione
Tachycardia, hypertension, heart murmur
V/D
Primary - Overactive gland typically from benign hyperplasia, result overproduction of thyroxine
Secondary - TSH secreting pituitary adenoma

Hyperthyroidism similarity to CKD
Increased activity, restless, aggression, weight loss despite PP key differences
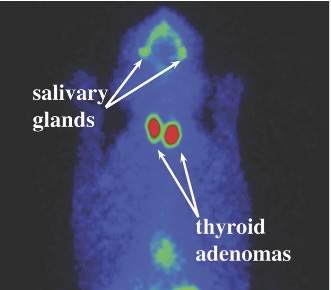
Hyperthyroidism diagnosis
T4 blood tests, additional scintigraphy
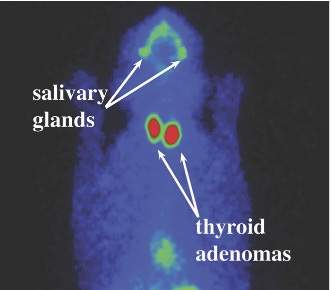
Ectopic thyroid tissue
Ectopic thyroid tissue in chest, highlighted in green.
Identifying areas of extra-thyroid tissue useful when determining treatment option
Hyperthyroidism treatment
Anti-thyroid medication, thyroidectomy, radioactive iodine therapy (RIT), dietary
Anti-thyroid medication
Methimazole (coated tablet) active form
Carbimazole (prolonged release) metabolised into methimazole by liver
Thiamazole (solution)
Side effects: V/D, inappetence, iatrogenic hypothyroidism (consequent renal failure)
Facial pruritus, jaundice, cytopaenia, immune disorder
Transdermal methimazole gel
Ear pinnae application to inappetent/fractious cats
Not licensed, used under prescribing cascade, specially formulated by company

Thyroidectomy
Bilateral/unilateral surgical removal of thyroid gland
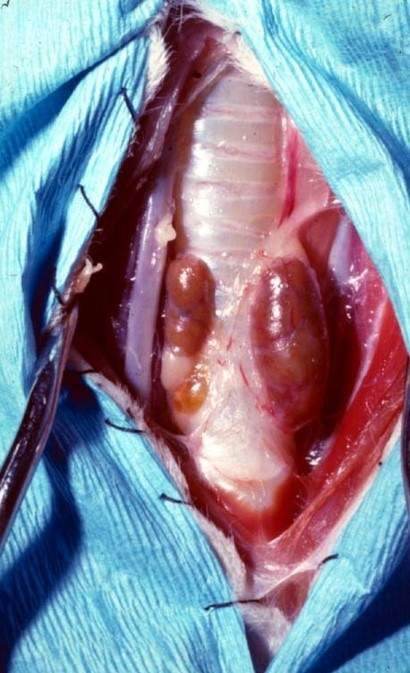
Thyroidectomy issues
Medical treatment administered prior surgery to ensure patient euthyroid (normal function), lowering bp, hr and reduce anaesthetic risk
Parathyroid tissue can be damaged/removed with diseased tissue, lead to hypoparathyroidism, hypocalaemia
Post surgery thyroidectomy
Monitor low blood calcium levels, implement IV calcium gluconate
May require life supplementation of calcium and vitamin D
Remaining tissue produce thyroxine - persistent signs of hyperthyroidism
Radioactive iodine therapy (RIT)
SC/ oral administration of radioactive iodine isotope
Iodine and bound radioactive isotope collects in thyroid, killing thyroid tissue due to radioactive iodine build up in gland
RIT handling
Strict safety protocols, isolation following administration
Safe housing, disposal of radioactive waste

Dietary management
Prescription diet manage thyroxine production
Diet restrict iodine within food, starving thyroid gland of nutrient require to synthesise thyroxine
ONLY consume this food, several month full effect