ANAT1012 Upper Limb (full credit to Isabellacw04)
1/211
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
212 Terms
1st
Which costal cartilage articulates with the manubrium immediately below the clavicular notch?
clavicle
scapula
proximal humerus
manubrium of the sternum
The bones involved in the joints of the shoulder region include the
clavicle and the first rib.
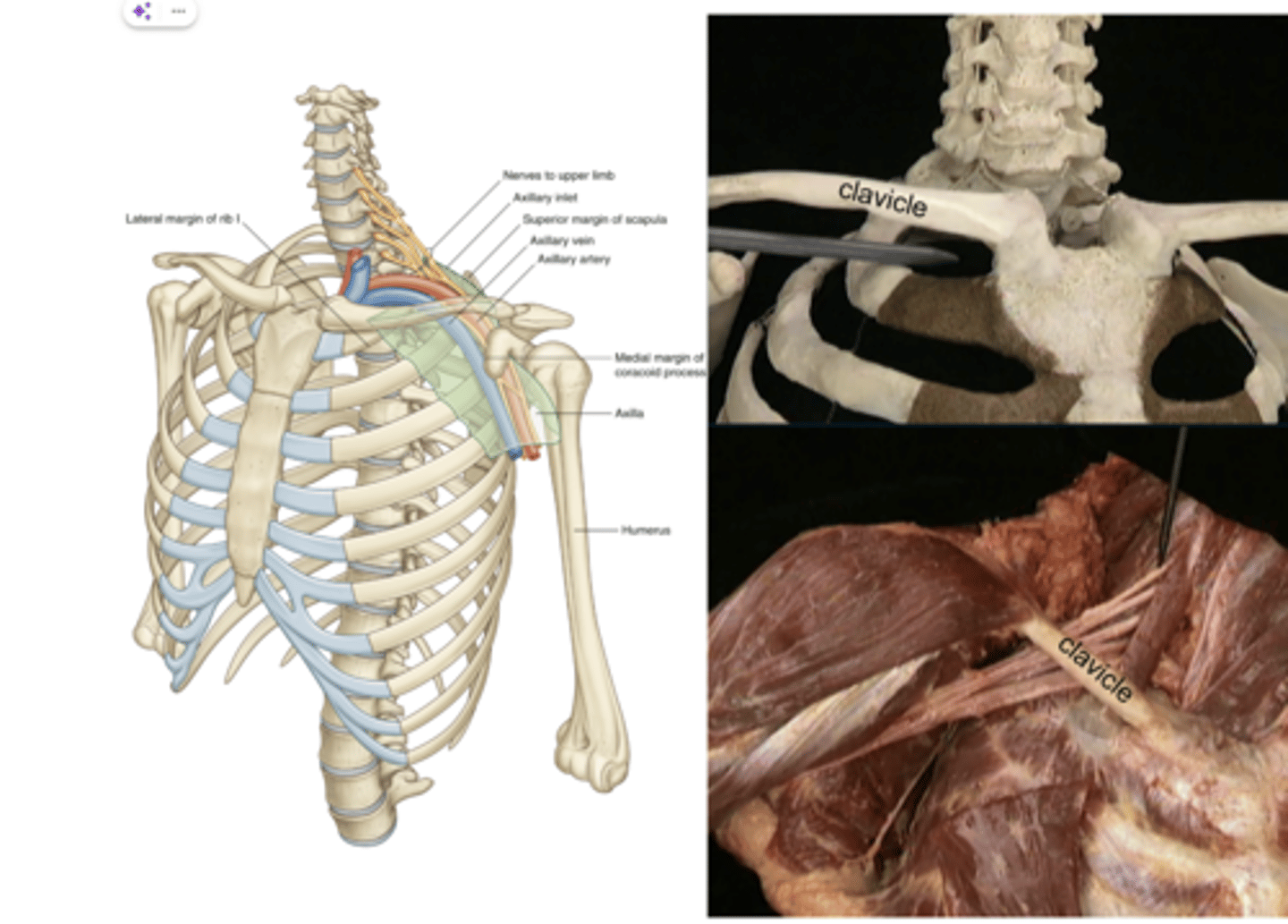
The costoclavicular space lies between the
subclavian artery, subclavian vein, and the brachial plexus. Constriction may lead to neurovascular compromise
what passes through the costoclavicular space?
conoid and trapezoid
Coracoclavicular ligaments

middle third
The usual site of fracture of the clavicle is the:
inferior and medial displacement of the lateral fragment
Following a typical fracture of the clavicle, which of the following best describes the usual deformity?
T7
In standing with the upper limbs resting by the sides, the inferior angle of the scapula is normally level with which thoracic spinous process?
T3
In standing with the upper limbs resting by the sides, the root of the spine of the scapula is normally level with which thoracic spinous process?
30 degrees internally rotated from the frontal plane
In standing with the upper limbs resting by the sides, which of the following describes the normal position of the scapula?
Greater tubercle
Which bony feature of the shoulder region projects furthest laterally?
Sternoclavicular joint (SCJ)
Acromioclavicular joint (ACJ)
Glenohumeral joint (GHJ)
The 3 anatomical joints of the shoulder region are the
Synovial saddle joint between:
-the medial end of the clavicle and
-the sternum & 1st costal cartilage
The size of the articular surface offers little to no bony stability, but its important that its stable due to position of vital anatomical structures (trachea, brachiocephalic trunk, internal jugular vein, subclavian artery and vein) and it's the only articulation between the upper appendicular and axial skeletons.
Sternoclavicular joint: where is it and comment on stability
Passive stability of the SCJ is obtained by the ligaments & articular disc:
Anterior sternoclavicular ligament
Posterior sternoclavicular ligament
Interclavicular ligament
Costoclavicular ligament
Meniscus /articular disc
What ligaments and other structures contribute to SCJ stability?
The synovial plane joint between:
-lateral end of the clavicle &
-the clavicular facet on the medial aspect of the acromion
The motion of the ACJ is limited by its small surface area.
The articular surfaces offer no bony stability.
Acromioclavicular joint: where is it and comment on stability
the superior and inferior acromioclavicular ligaments provide the greatest resistance to displacement of the joint
resist rotation of the clavicle and vertical translation of the clavicle relative to the scapula.
- Trapezoid ligament
- Conoid ligament
- Sup/inf acromioclavicular ligaments
ACJ - what ligaments provide stability?
Minor injuries typically involve the AC ligaments. The conoid and trapezoid ligaments injure with more forceful impact.
Acromioclavicular joint dislocations typically involve:

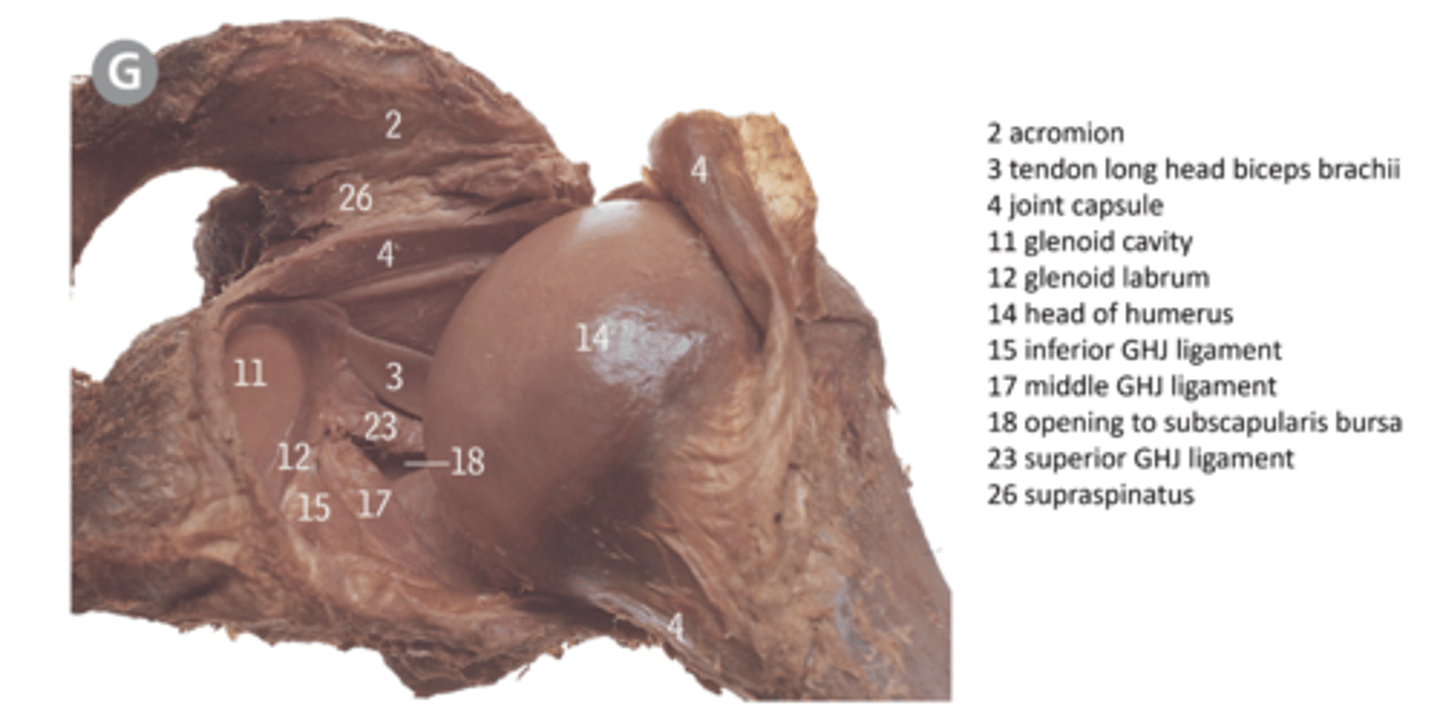
Synovial ball & socket joint between:
-head of humerus
-glenoid fossa
The disparity in the size of the articular surfaces and the shallow glenoid fossa provide almost NO bony stability.
Glenohumeral joint: location and comment on stability
The glenoid labrum
is a fibrocartilage rim attached to the margin of the glenoid fossa. It increases the depth of the glenoid fossa & increases the articular contact area.
The glenohumeral joint capsule attaches:
medially to the glenoid neck
laterally to the anatomical neck of humerus
The loose inferior capsule (axillary pouch) permits the large range of GHJ F and Abd.
Glenohumeral joint ligaments
GHJ stability relies on:
The GHJ capsule is reinforced anteriorly by 3 ligaments:
-Superior glenohumeral ligament (SGHL)
-Middle glenohumeral ligament (MGHL)
-Inferior glenohumeral ligament complex (IGHLC)
The coracohumeral ligament (CHL) extends from the coracoid process across the superior aspect of the joint as 2 bands to attach to the greater and lesser tubercles. The two bands blend with the superior joint capsule.
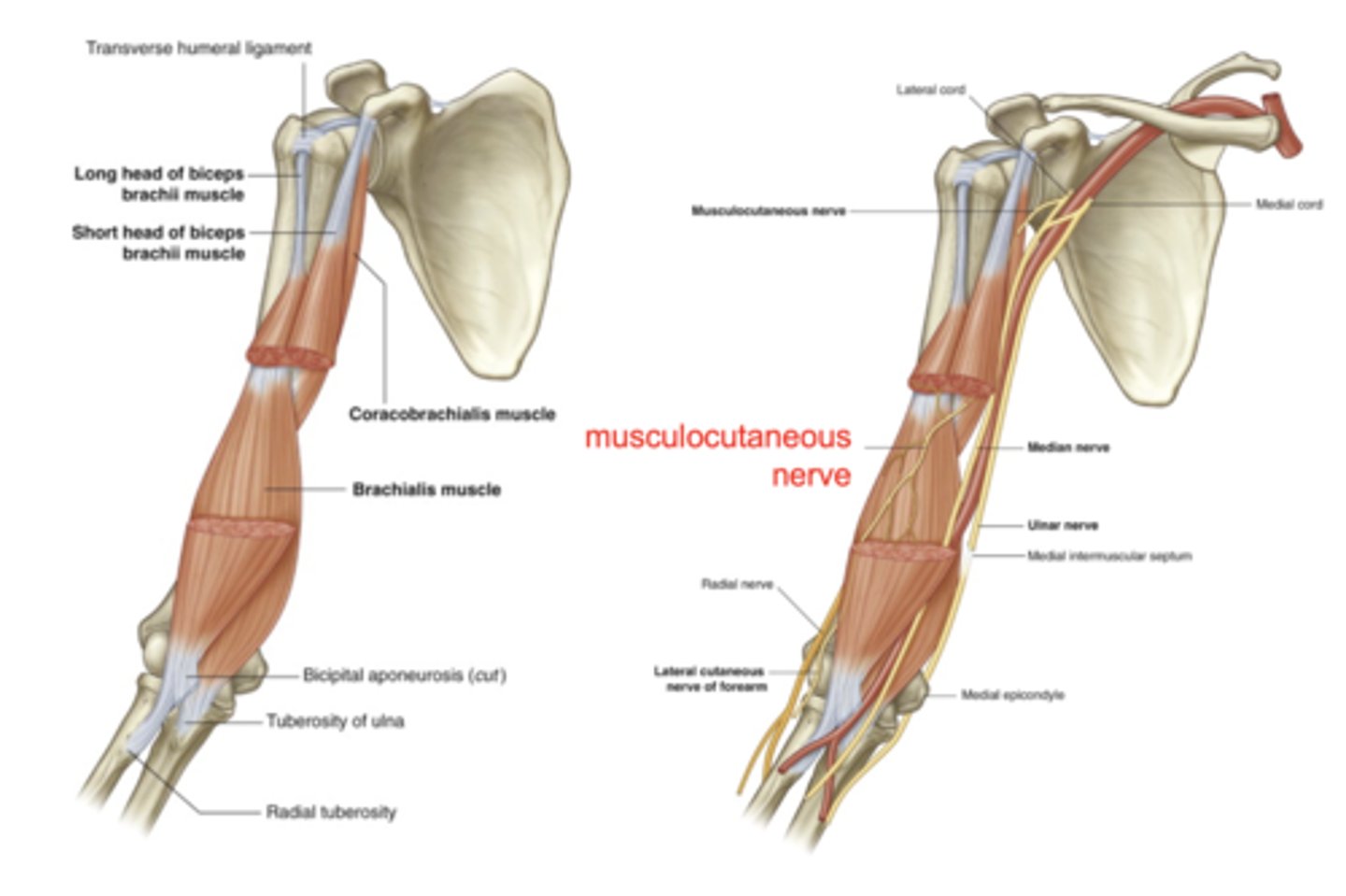
The transverse humeral ligament attaches to the lesser and greater tubercles. It stabilises the tendon of the long head of biceps brachii in the intertubercular sulcus.
GHJ ligaments
- subacromial / subdeltoid bursa (5) - located between the acromion, coracoacromial ligament and deltoid muscle above, and the superior capsule below. This bursa does not communicate with the GHJ cavity.
- The subscapularis bursa (6) between the subscapularis tendon and the capsule. This bursa is continuous with the joint through a space between the superior and middle glenohumeral ligaments.
Bursae of the GHJ
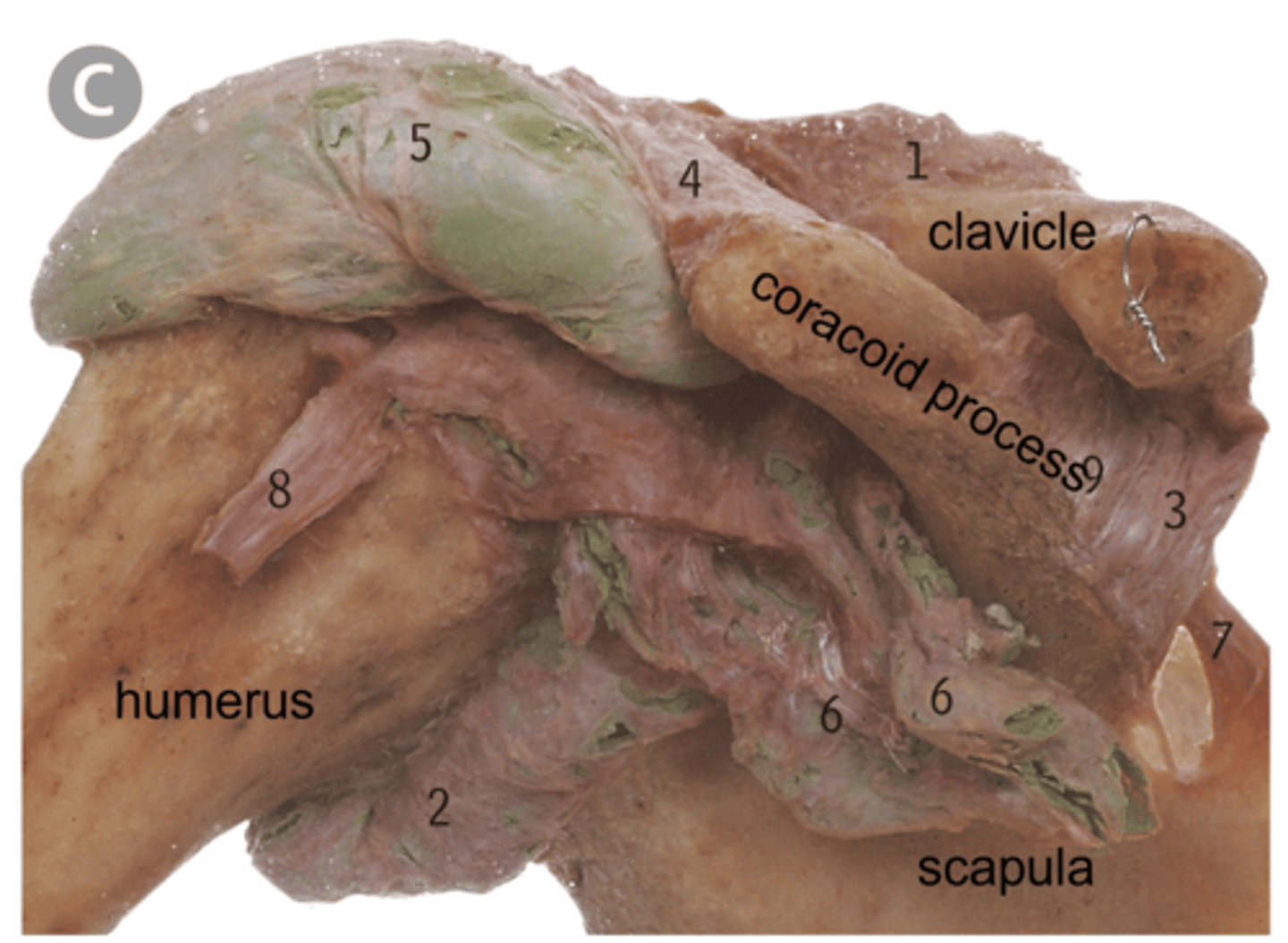
Connects the coracoid process and acromion.
The coracoacromial arch comprises the inferior surfaces of the:
-acromion
-coracoacromial ligament (CAL)
-coracoid process
-acromioclavicular (AC) joint
The coracoacromial arch forms a roof above the subacromial space. The subacromial space lies between the coracoacromial arch and the head of humerus.
Coracoacromial arch
1. subacromial bursa,
2. supraspinatus tendon
3. tendon of long head of biceps brachii
4. coracohumeral ligament
5. superior glenohumeral ligament
What is included in the subacromial space?

- The most common mechanism of injury is a combination of excessive abduction and external rotation.
- The most frequent direction of dislocation is anterior-inferior / subcoracoid.
- The acromiohumeral distance will be increased in an anterior-inferior GHJ dislocation.
GHJ dislocations
in the medial clavicle above the costoclavicular ligament
The axis for sternoclavicular joint (SCJ) elevation-depression and protraction-retraction is located:
elevation of the lateral end of the clavicle
In the case of moderate acromioclavicular dislocation what would be the typical presenting deformity?
muscles
Stability of the glenohumeral joint (GHJ) within the normal limits of motion is mainly reliant on:
anterior band inferior glenohumeral
Which ligament supports the anterior aspect of the glenohumeral joint in a position of 90o abduction and external rotation?
anterior-inferior
What is the most common direction of GHJ dislocation?
7-11mm
What is the normal acromiohumeral distance on anterior-posterior x-ray?
supraspinatus tendon
Which structure is likely to be in the subacromial space in an upper limb position of 90o abduction and 70o internal rotation?
Movements of the clavicle, scapula and humerus during abduction of the scapular plane

sternoclavicular joint
Movements of the clavicle occur at the:
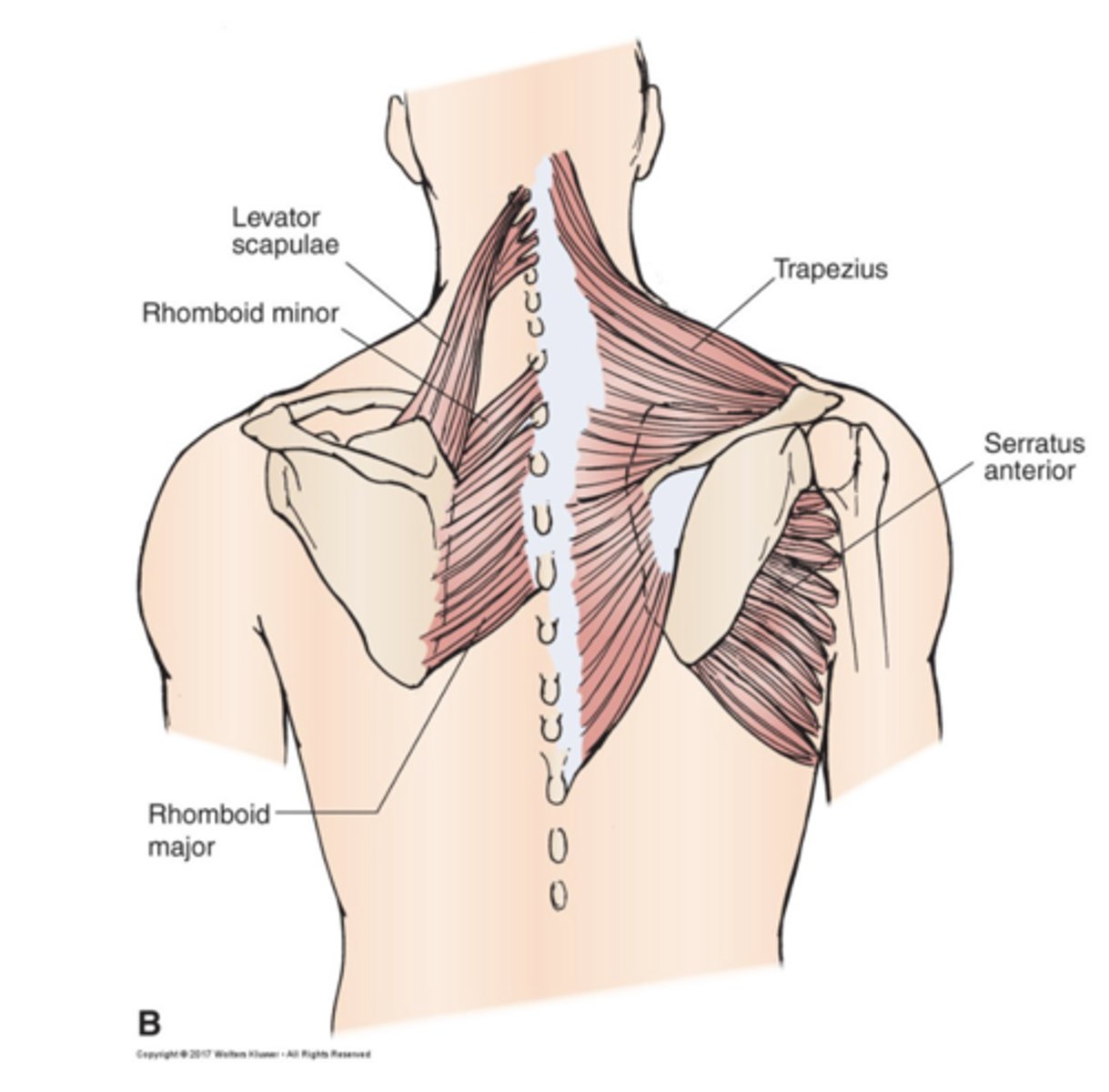
1. Trapezius
- superior
- middle
- lower
2. Levator scapulae
3. Rhomboid minor
4. Rhomboid major
5. Serratus anterior
Posterior axioclavicular and anterior axioscapular muscles
Superior trapezius:
O: superior nuchal line and ligamentum nuchae
I: posterior border lateral 1/3 clavicle
Middle trapezius
O: C7 & T1
I: acromion and spine of scapular
Lower trapezius
O: below T1
I: deltoid tubercle of scapula
Origin and insertion of:
Superior trapezius
Middle Trapezius
Lower Trapezius
- creates a stable base for the glenohumeral joint
- optimises scapulohumeral muscle length
- moves coracoacromial arch upward & posteriorly maintaining subacromial space
The benefits of normal scapular dynamics during upper limb elevation
1. Scapular dynamics
- prime mover of scapular upward rotation and is involved in scapular posterior tilt and external rotation, weakness or fatigue in serratus anterior will affect these movements
2. Scapular posture
- 'Winging' of medial border during static weight-bearing posture
Serratus anterior weakness or fatigue affects
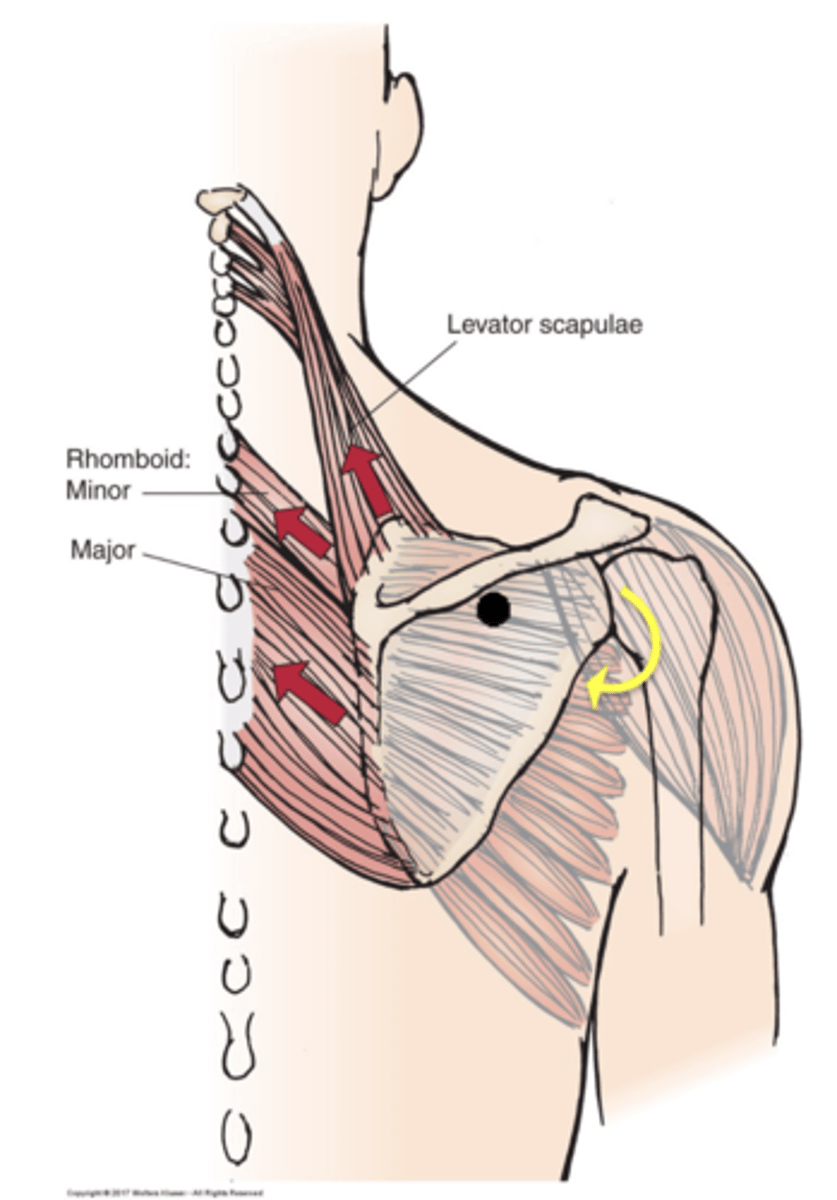
Levator scapulae
(Scapular retraction)
Scapular elevation
Scapular downward rotation
Rhomboid minor
Scapular retraction
Scapular elevation
Scapular downward rotation
Rhomboid major
Scapular retraction
Scapular elevation
Scapular downward rotation
In terms of the scapula, what actions do the following allow:
1. Levator Scapulae
2. Rhomboid minor
3. Rhomboid major
retraction from levator scapulae & rhomboids
Protraction from pectoralis minor cancels the
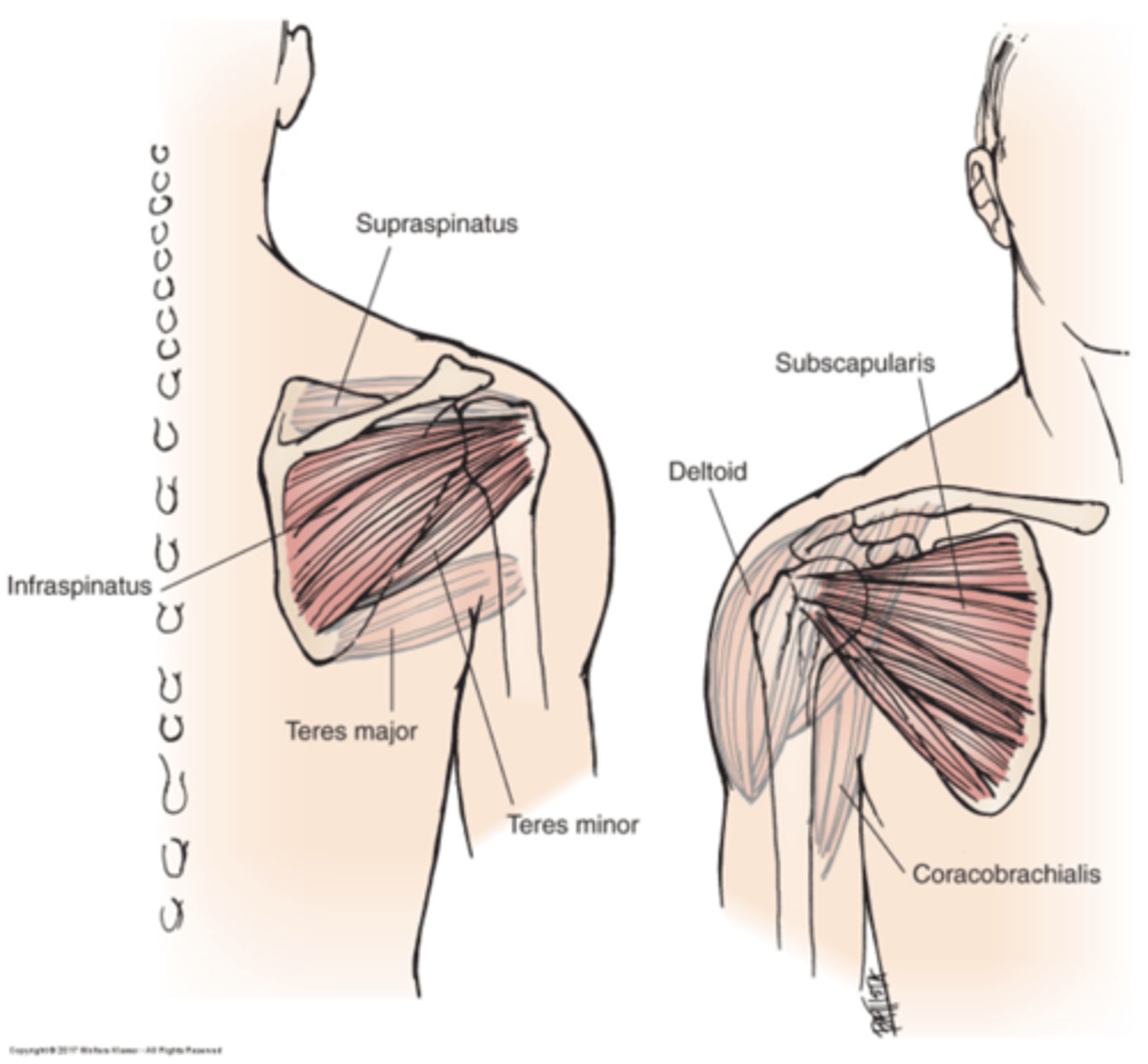
1. deltoid
2. supraspinatus
3. infraspinatus
4. teres minor
5. subscapularis
6. teres major
7. coracobrachialis
Scapulohumeral muscles
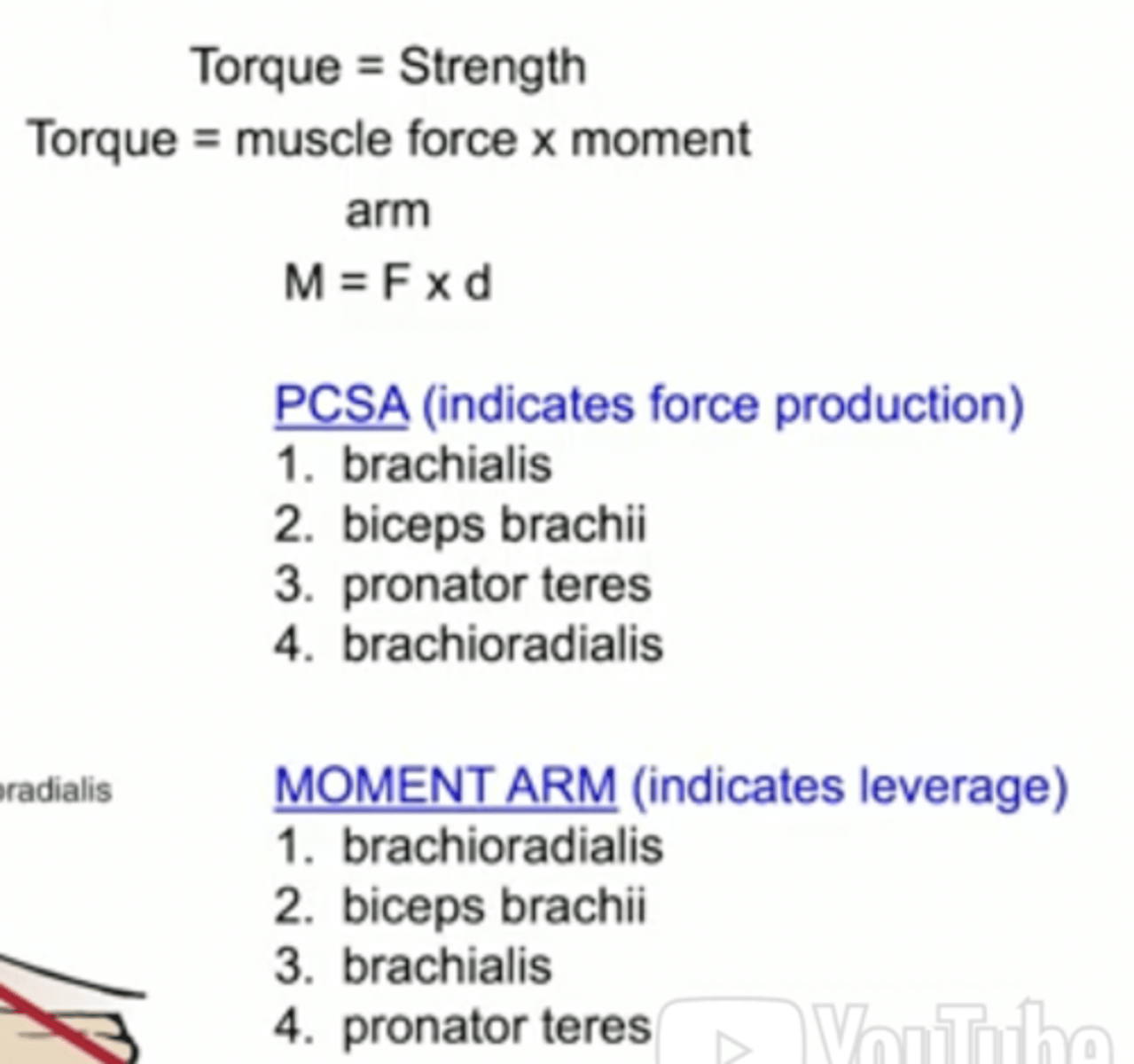
force x moment arm
muscle torque = muscle strength
Torque (Moment of force) =
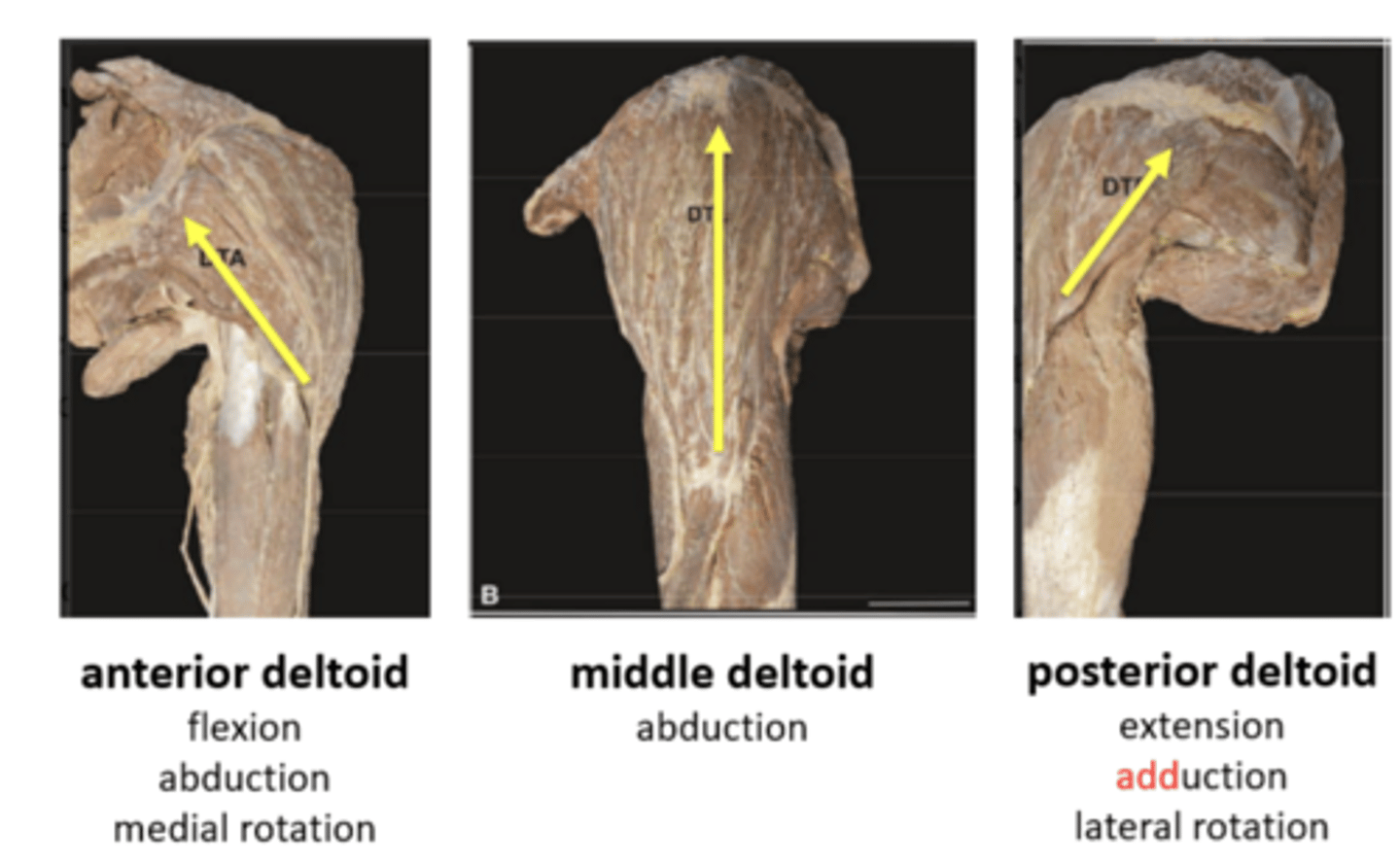
3 anatomical segments of the deltoid
1. subscapularis
2. supraspinatus
3. infraspinatus
4. teres minor
Rotator cuff muscles
Pectoralis major:
Two parts: clavicular part and sternocostal part based on proximal attachments.
All fibres adduct and medially rotate the arm.
- clavicular part = flexion from an extended - position
- sternocostal part = resisted extension from a flexed position
Latissimus dorsi:
Active in GHJ medial rotation, adduction and extension.
Powerful adduction and extension against resistance from a flexed or abducted position.
Axiohumeral muscles
- C5 & C6 ventral rami combine to form the superior trunk,
- C7 continues as the middle trunk, and
- C8 & T1 unite to form the inferior trunk.
Supraclavicular parts of the brachial plexus
- neural or vascular compromise of the brachial plexus and associated vasculature as they travel from the cervical region, down the superior thoracic wall into the axilla.
-Often results due to compression of: interscalene triangle,
costoclavicular space, coracopectoral tunnel.
- Most patients with TOS report pain in the upper extremity and neck. TOS can be vascular, neurogenic, or both. Neural signs and symptoms are pain, paraesthesia, and muscle weakness. Vascular symptoms may include swelling, and pale or bluish appearance in the limb.
Thoracic outlet syndrome (TOS)
The interscalene triangle is formed by the:
1. anterior scalene
2. middle scalene
3. 1st rib
The roots and trunks of the brachial plexus and the subclavian artery are located within the interscalene triangle.
Interscalene triangle

The costoclavicular space is located between the clavicle and the 1st rib. Scapular retraction and depression reduce the size of the costoclavicular space.
Costoclavicular space
The coracopectoral tunnel is deep to pectoralis minor. Hyperabduction of the upper limb may tension the pectoralis minor across the neurovascular bundle
Coracopectoral tunnel

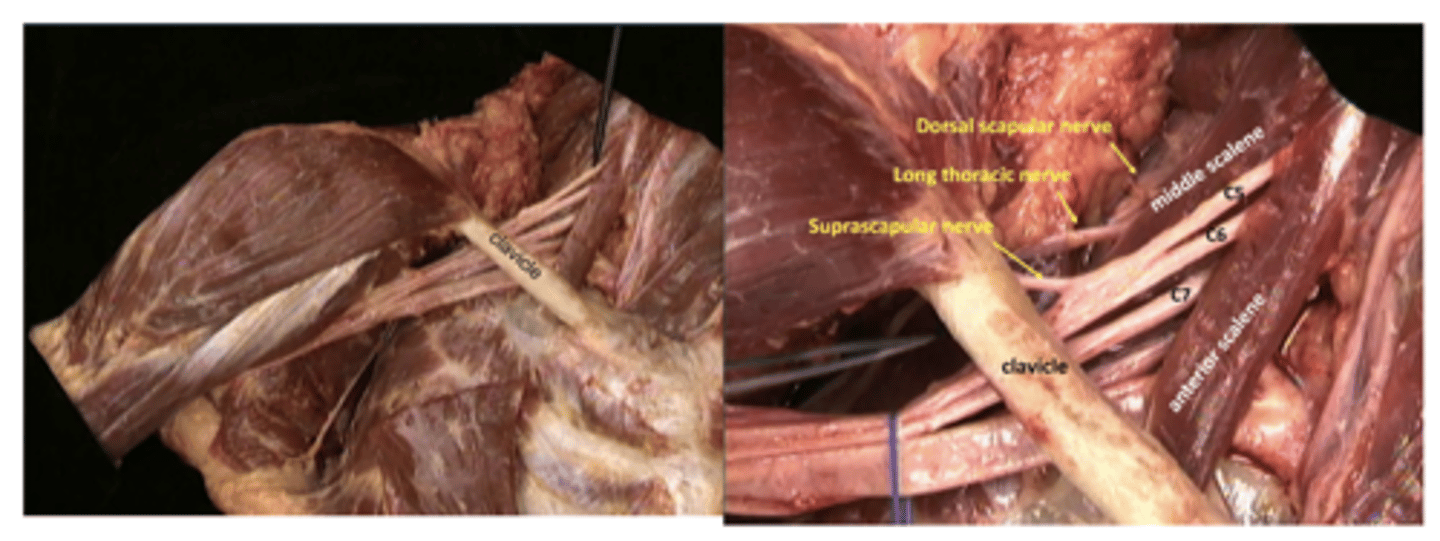
Arise from roots and trunks
Branches from roots:
- Dorsal scapular C5
- Long thoracic C5,6,7
Branches from trunks:
- Suprascapular C5,6
- Subclavian C5,6
Supraclavicular branches
"winging of the scapula" general weakness of serratus anterior muscle
long thoracic nerve injury
Potential sites of injury include:
- The suprascapular foramen
- The spinoglenoid notch
Most cases involve repetitive overhead activities such as throwing, tennis and volleyball. Pathology may be a result of compression or stretching. Movements associated with injury include repeated excessive external rotation in abduction (throwing, tennis) or repeated shoulder adduction and internal rotation (volleyball).
Suprascapular nerve entrapment
The suprascapular nerve at the suprascapular foramen carries sensory fibres to the coracohumeral & coracoacromial ligaments, subacromial bursa, ACJ & GHJ, and motor fibres to supraspinatus and infraspinatus.
Injury at the suprascapular foramen results in:
- poorly localised posterolateral shoulder pain
- supraspinatus & infraspinatus weakness & wasting
The supracapular nerve at the spinoglenoid notch carries only motor fibres.
Injury at the spinoglenoid notch results in:
- infraspinatus weakness & wasting
Injury at the suprascapular foramen results in:
Lateral cord:
Lateral pectoral C5,6,7
Musculocutaneous C5,6,7
Medial cord:
Medial pectoral C8,T1
Medial cutaneous of arm C8,T1
Medial cutaneous of forearm C8,T1
Ulnar C7,C8,T1
Lateral and medial cords:
Median C6-T1
Posterior cord:
Upper subscapular C5,6
Lower subscapular C5,6
Thoracodorsal (Middle subscapular) C6,7,8
Axillary C5,6
Radial C5-C8
Infraclavicular branches arise from cords. Name the branches that arise from certain cords.

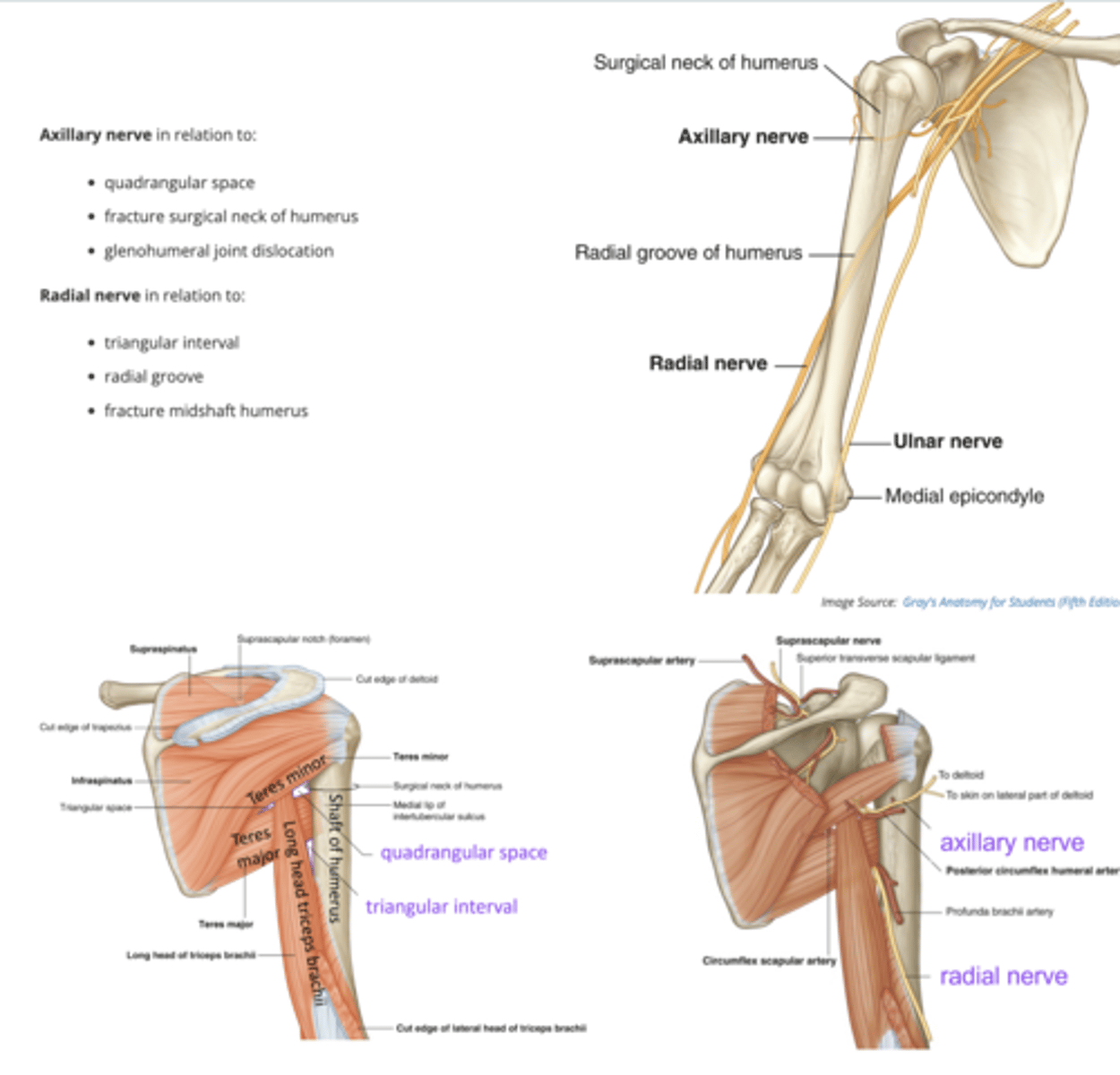
Axillary nerve in relation to:
quadrangular space
fracture surgical neck of humerus
glenohumeral joint dislocation
Radial nerve in relation to:
triangular interval
radial groove
fracture midshaft humerus
Two infraclavicular branches that may be compromised in the shoulder region are the:
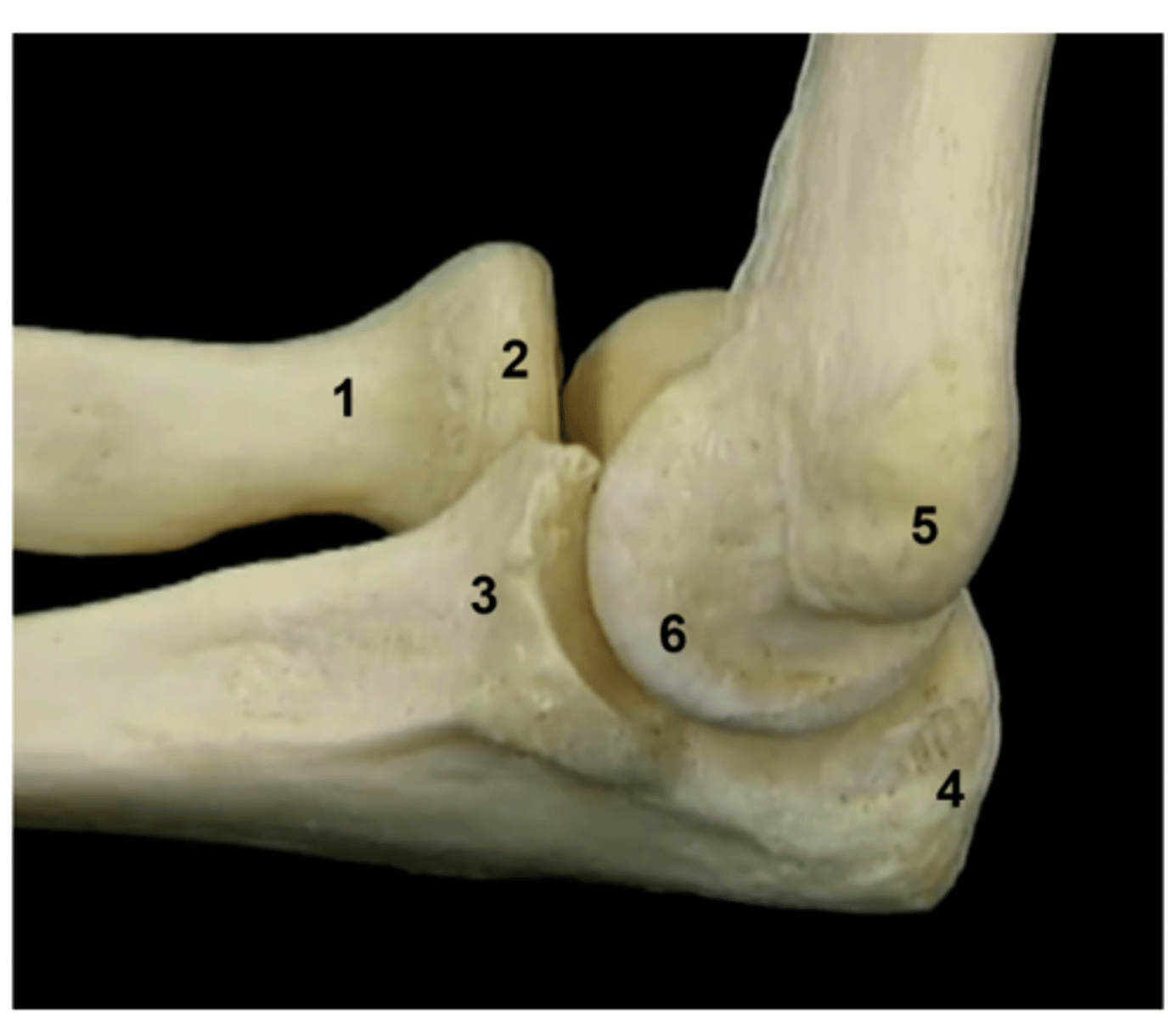
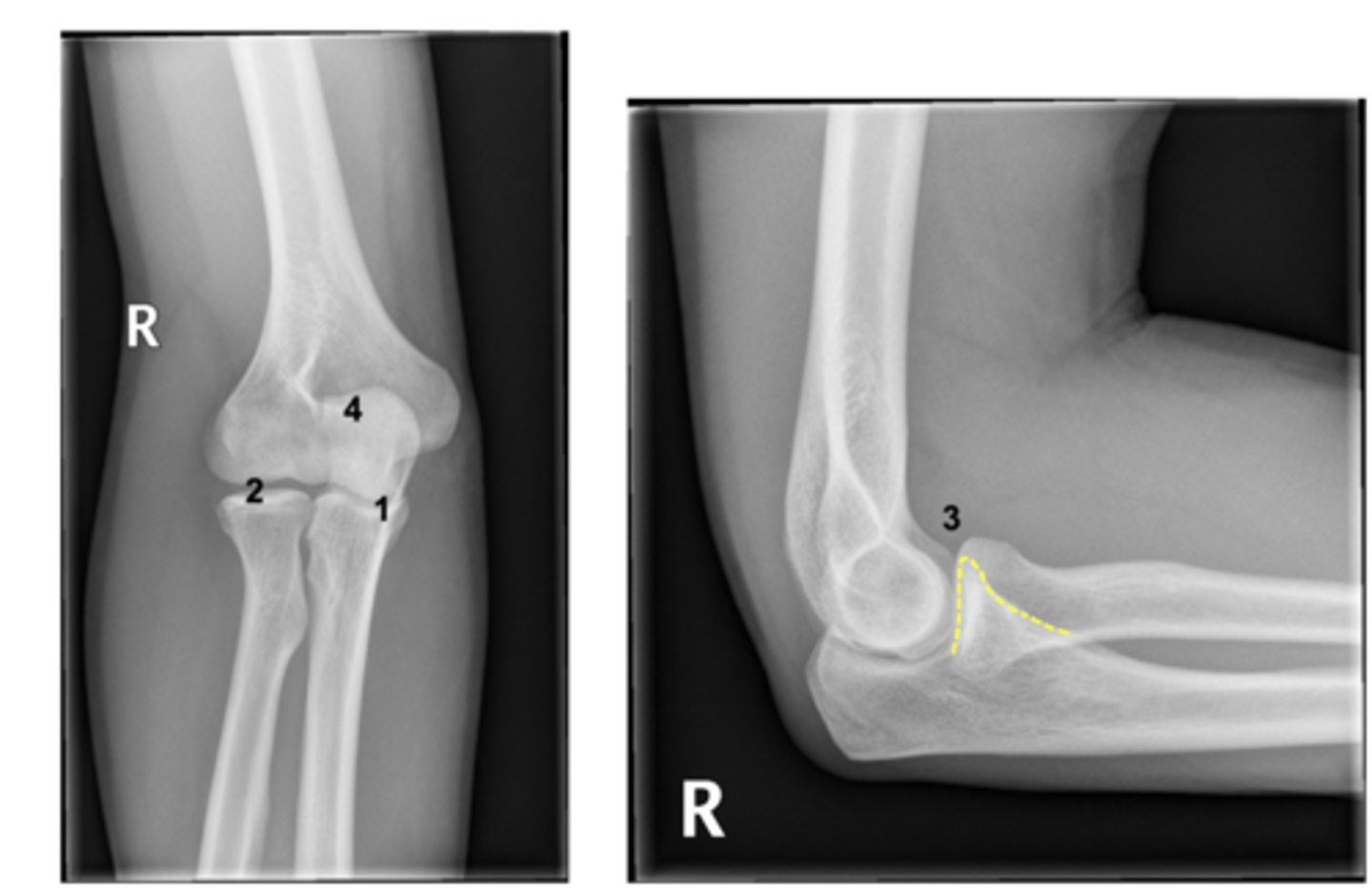
Inverse card: label the image
1. Neck of radius
2. Head of radius
3. Coronoid process
4. Olecranon
5. Medial epicondyle of humerus
6. Trochlea
1. Humeral External Torsion
- humeral shaft is rotated externally around its long axis, aligning the distal humeral condyle close to the coronal plane such that elbow flexion brings the hand anteriorly and toward the clavicle.
2. Anterior curve distal humeral shaft
- The distal shaft curves anteriorly, directing the articular surfaces more anteriorly and thus favouring flexion.
3. Inferomedial joint axis
- medial edge of the trochlea extends farther distally than the lateral, creating an inferomedial joint axis and partly explaining the lateral orientation of the ulna with respect to the humerus.
What three features affect orientation/ROM of the elbow joint?
10-15 degrees. Commonly referred to as 'carrying angle'.
Normal elbow valgus
lateral deviation of distal segment relative to the proximal segment
Valgus

medial deviation of distal segment relative to the proximal segment
Varus

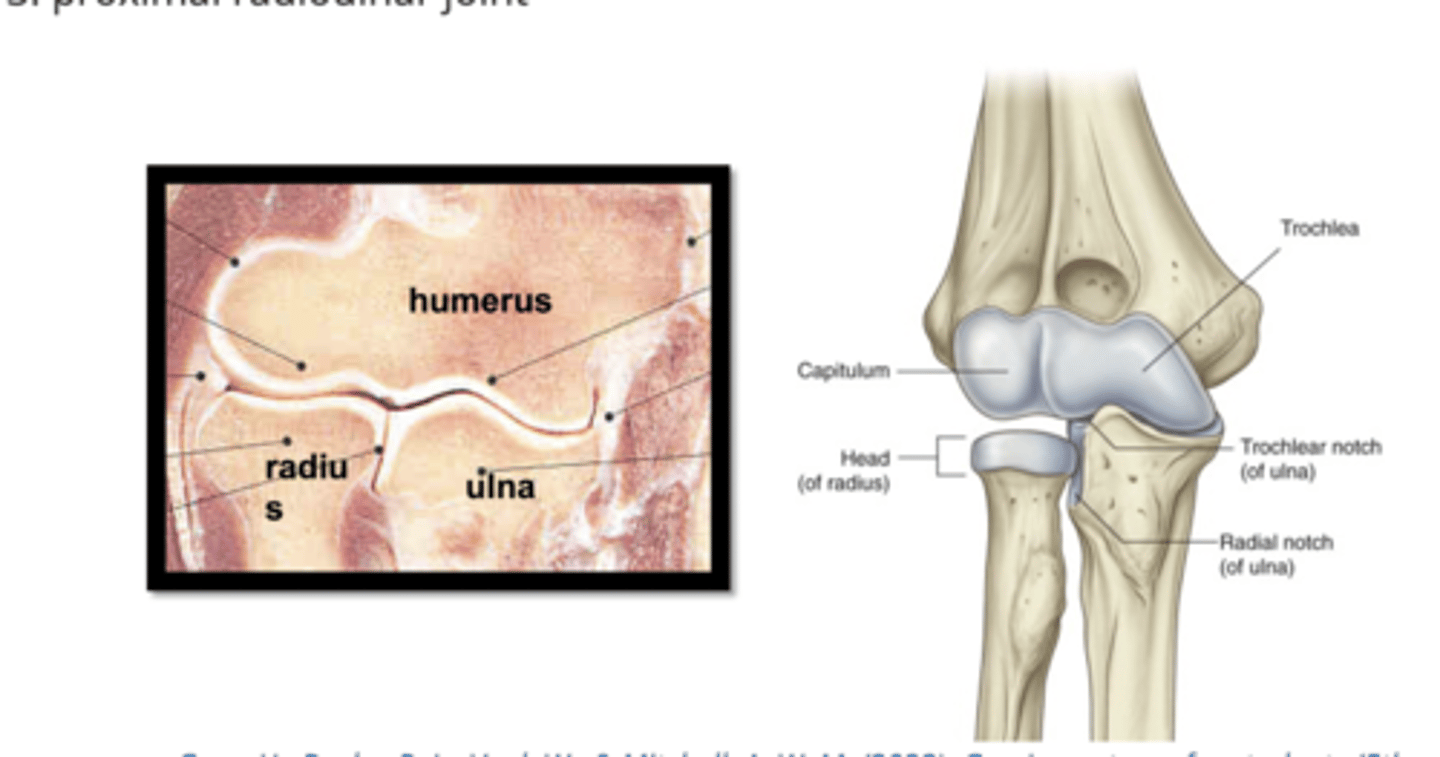
1. humeroulnar joint
2. humeroradial joint
4. proximal radioulnar joint
Elbow joint complex
- Thin to permit range of flexion/extension.
Elbow joint capsule
1. head of radius
2. trochlear notch of ulna
What do the following articulate with:
1. Capitulum of humerus
2. trochlear of humerus
- radiocapitellar = 58%
- ulnotrochlear = 42%
Relative distribution of axial load in full extension is approximately:
1. valgus instability
2. varus instability
3. posterior instability
4. posterolateral rotary instability (pathological supination of ulna on humerus)
4 main reasons of instability in elbow joint
1. congruency of articular surfaces
2. joint capsule
3. ligaments
4. interosseous membrane
Static/passive stabilisers of elbow joint
- muscles that cross the joint
dynamic stabilisers of elbow joint
- A PRIMARY constraint is defined as a constraint where release of that structure causes a laxity of the joint.
- A SECONDARY constraint is a constraint where release alone is insufficient to cause laxity, but where release after division of the primary constraint increases the laxity of the joint.
Primary and secondary constraints: definition and application to elbow stability

1. The width and interlocking structure of the humeroulnar articulation provides primary constraint against valgus and varus forces
2. The radiohumeral articulation is a secondary passive constraint against valgus forces
3. The olecranon engages in the olecranon fossa @ 0° to 20°F
4. The coronoid process is a primary stabiliser against posterior dislocation of the ulna on the humerus
Elbow joint complex: bony stability
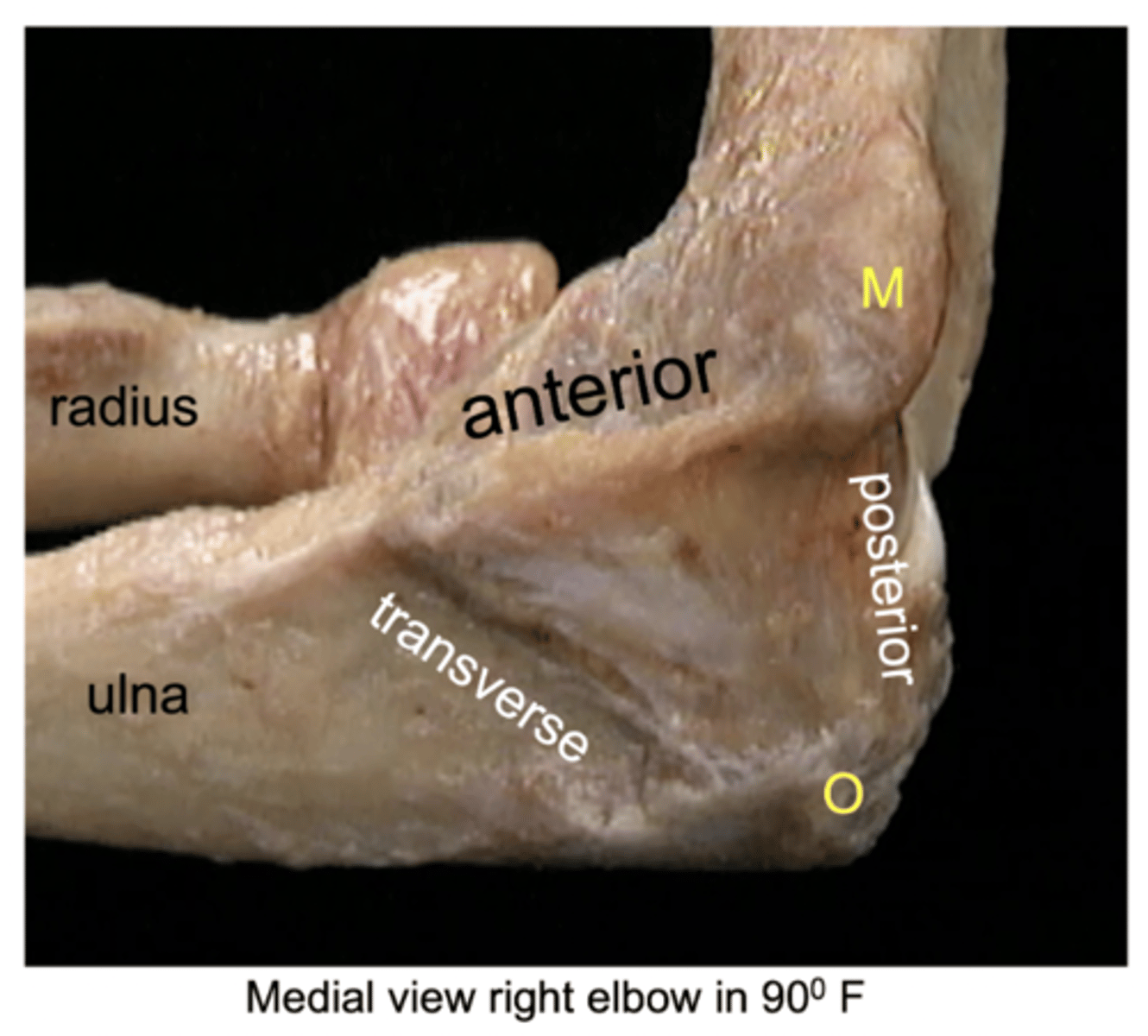
1. anterior band (AMCL) - well defined
2. posterior band (PMCL) - weaker
3. transverse band (TMCL) - no contribution to elbow joint stability
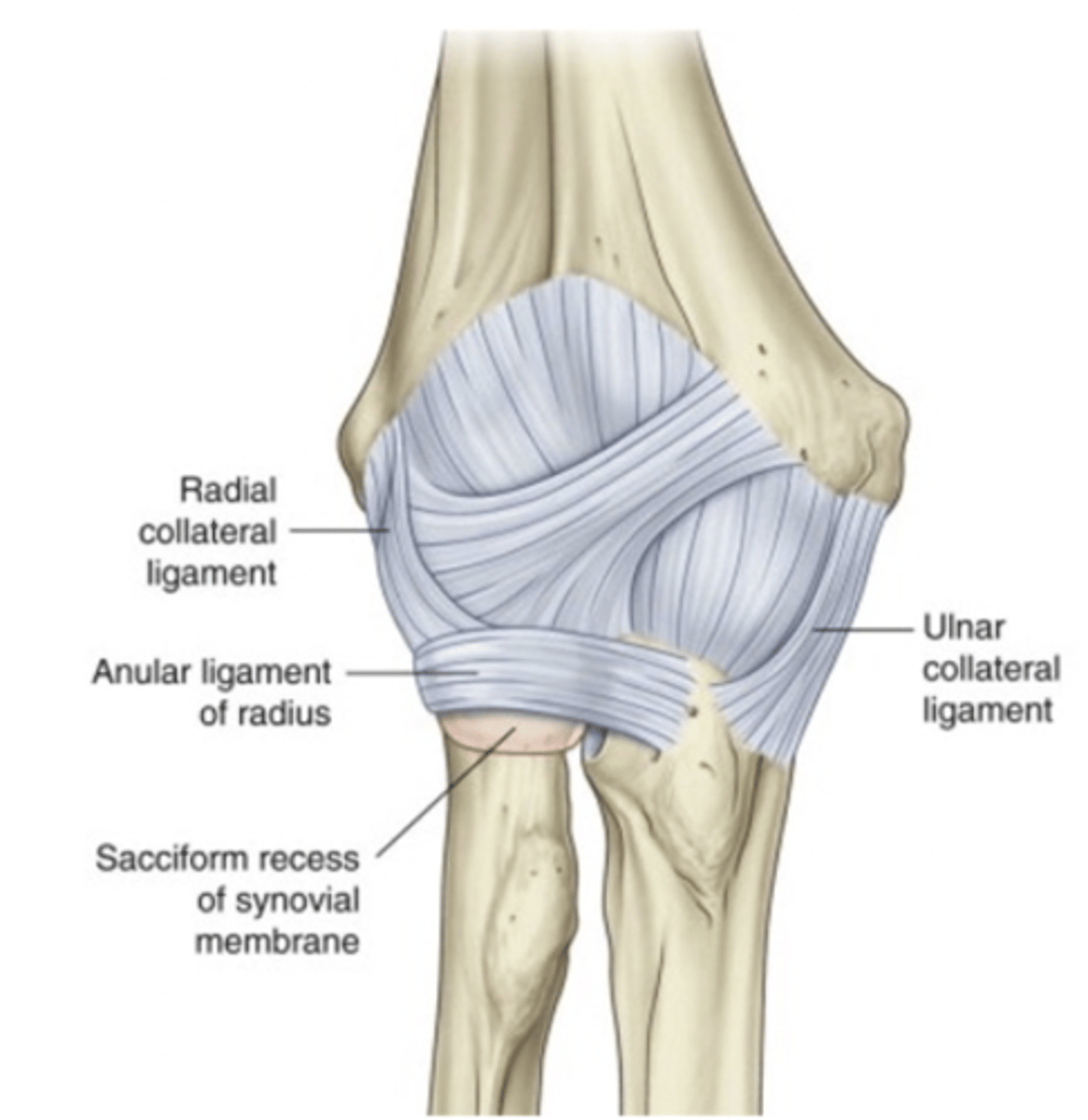
Medial collateral ligament
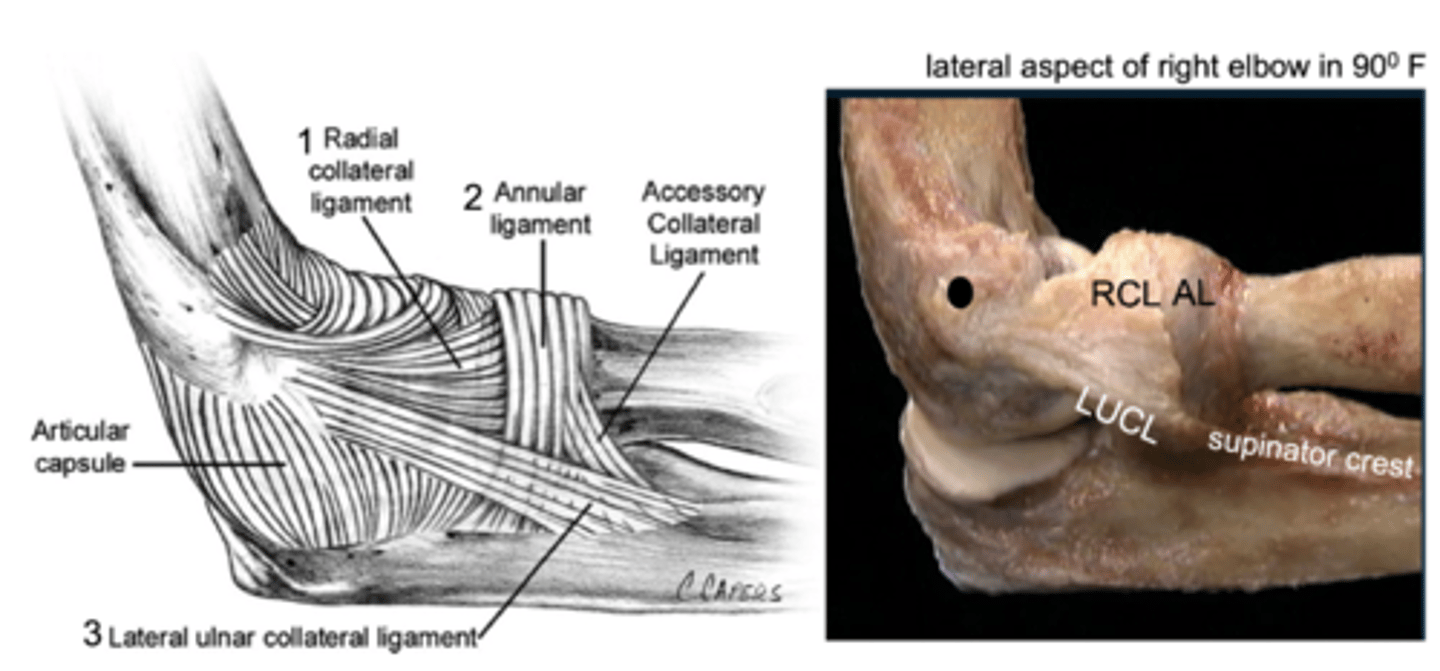
LCLC is a primary constraint to varus forces
1. lateral / radial collateral ligament (LCL or RCL)
- from lateral epicondyle to annular ligament
2. annular ligament (AL)
- attaches to anterior & posterior margins radial notch
3. lateral ulnar collateral ligament LUCL)
- lateral epicondyle to supinator crest of ulna
- LUCL is the primary constraint to posterolateral rotary instability
Lateral collateral ligament complex
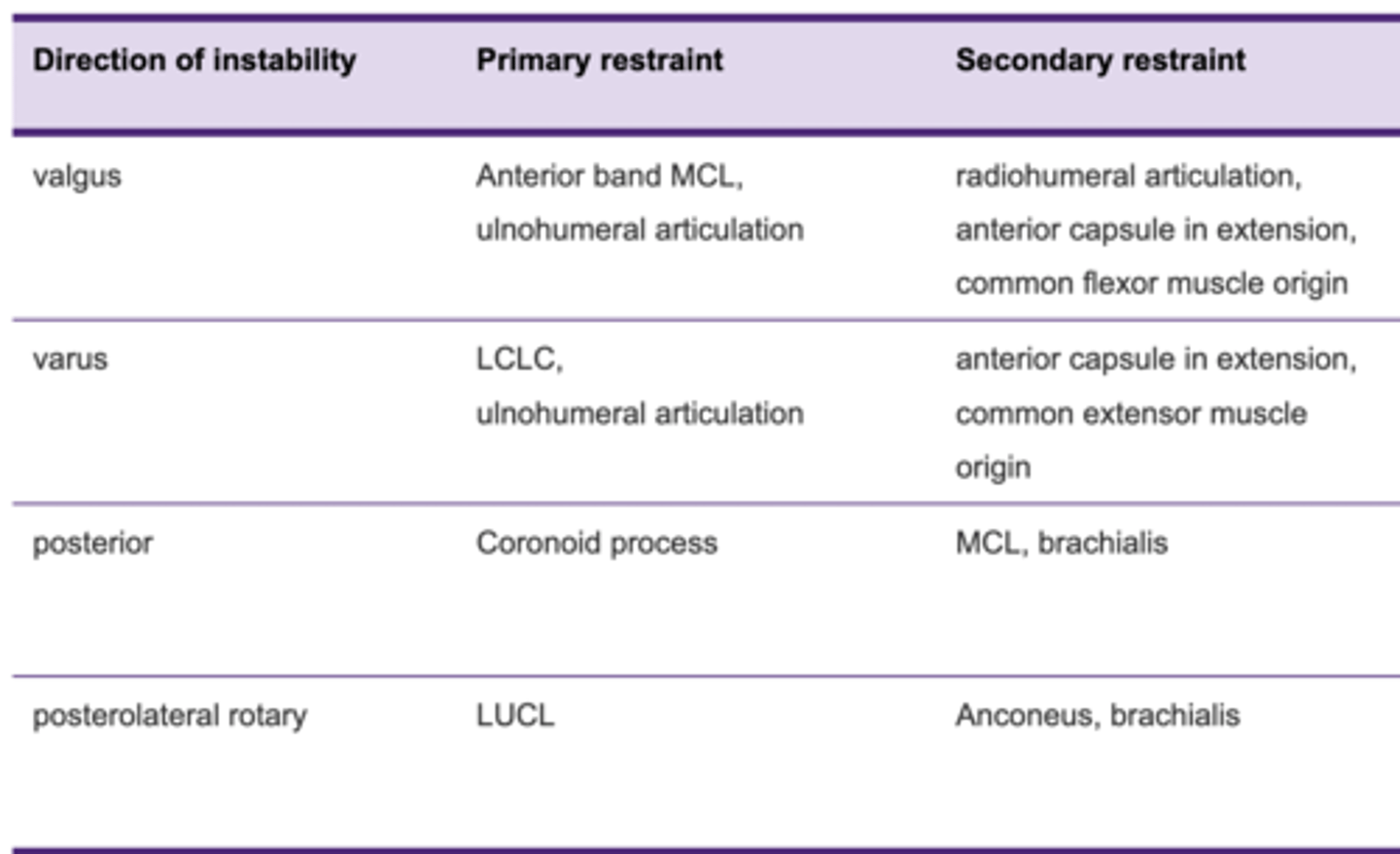
Primary and secondary restraints for the following:
1. Valgus
2. Varus
3. Posterior
4. Posterolateral rotary
0 degrees E - 140 degrees F
Normal range of elbow motion
supraglenoid tubercle
The proximal attachment of biceps brachii long head is:
radial tuberosity
The distal attachment of biceps brachii is:
ulnar tuberosity
The distal attachment of brachialis is:
infraglenoid tubercle
The proximal attachment of triceps brachii long head is:
- coracobrachialis
- biceps brachii
- brachialis
3 muscles of anterior compartment of arm
PCSA: Physiological cross-sectional area = indicates force production (rank)
Then, rank the same 4 muscles in order or longest to shortest moment arms (mechanical leverage)
Analysis of elbow flexors
Triceps brachii, three heads:
1. long
2. lateral
3. medial
- The long head originates on the infraglenoid tubercle of the scapula so its activity may be affected by GHJ position.
- The lateral and medial heads originate on the shaft of the humerus above and below, respectively, the radial groove.
- The 3 heads insert on the olecranon which is elongated to lengthen the moment arm of triceps brachii for elbow extension strength.
Posterior compartment of the arm
79%
Triceps brachii is the strongest elbow extensor.
Anconeus assists elbow extension.
Elbow extensor torque is approximately __% of elbow flexor strength
C5 & C6
Which spinal levels innervate the three main elbow flexors?
C6
What is the myotome level for elbow flexion?
Musculocutaneous and radial
Which peripheral nerves innervate the three main elbow flexors?
70-90 degrees
At what range of elbow flexion are the elbow flexors capable of producing the greatest torque?
triceps brachii lateral and medial head
During an isometric elbow extension task @90°F, which muscles contribute the greatest torque?
C6, 7, 8
Which spinal levels innervate the elbow extensors?
radial
Which peripheral nerve innervates elbow extensors?
C7
What is the myotome level for elbow extension?
1. proximal radioulnar joint (PRUJ)
2. interosseous membrane (IOM)
3. distal radioulnar joint (DRUJ)
Forearm complex structure
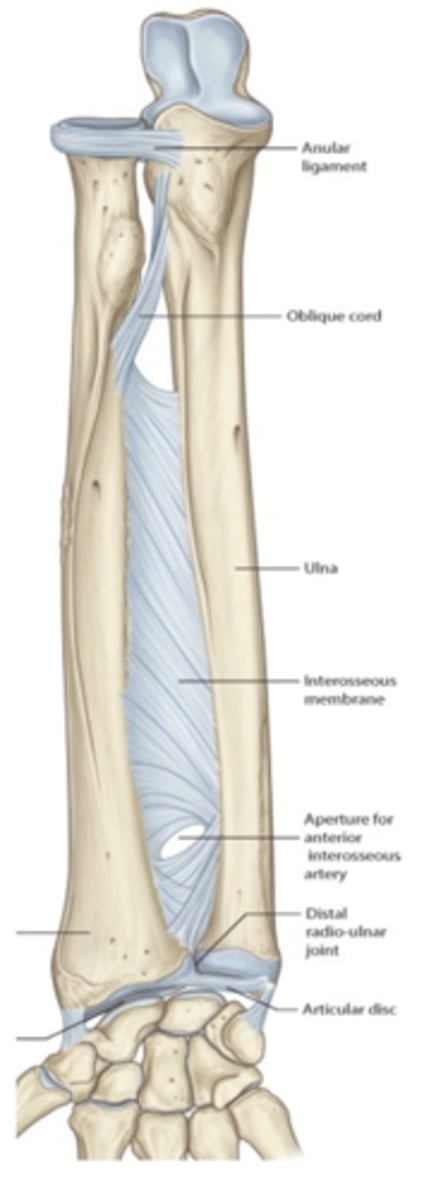
- head of radius articulates with radial notch of ulna (pivot)
- primary stabiliser = annular ligament
Proximal radioulnar joint

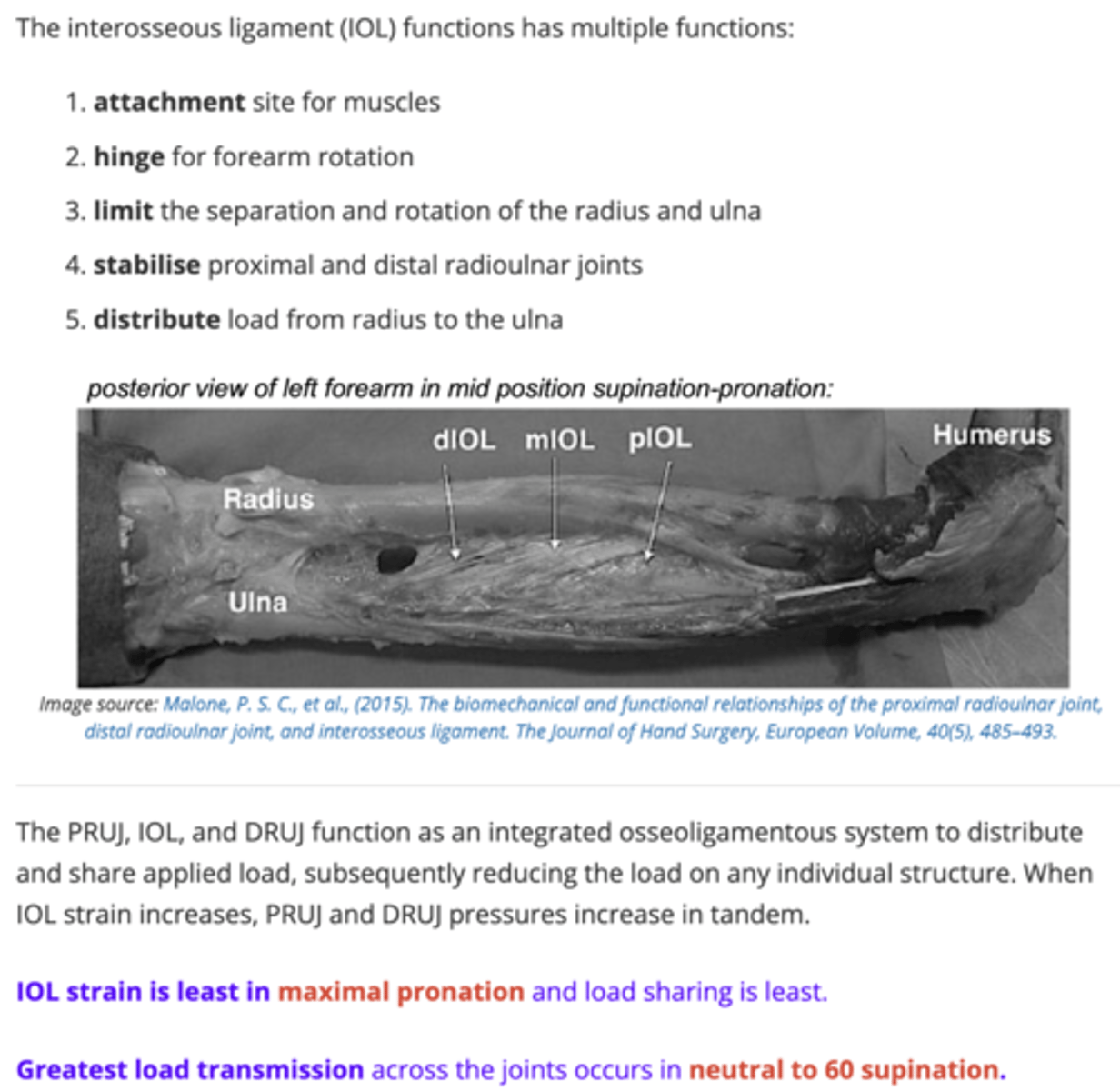
- IOM contains proximal and distal membranous portions
- mid section if a ligament complex, the interosseous ligament (IOL) comprising of the proximal (pIOL), middle (mIOL), and distal (dIOL) parts
Interosseous membrane (IOM) and interosseous ligament (IOL)
- L shaped
- vertical part = distal ulna articulates with triangular fibrocartilage disc
- synovial plane
- primary passive stabiliser = triangular fibrocartilage complex (TFCC)
Distal radioulnar joint
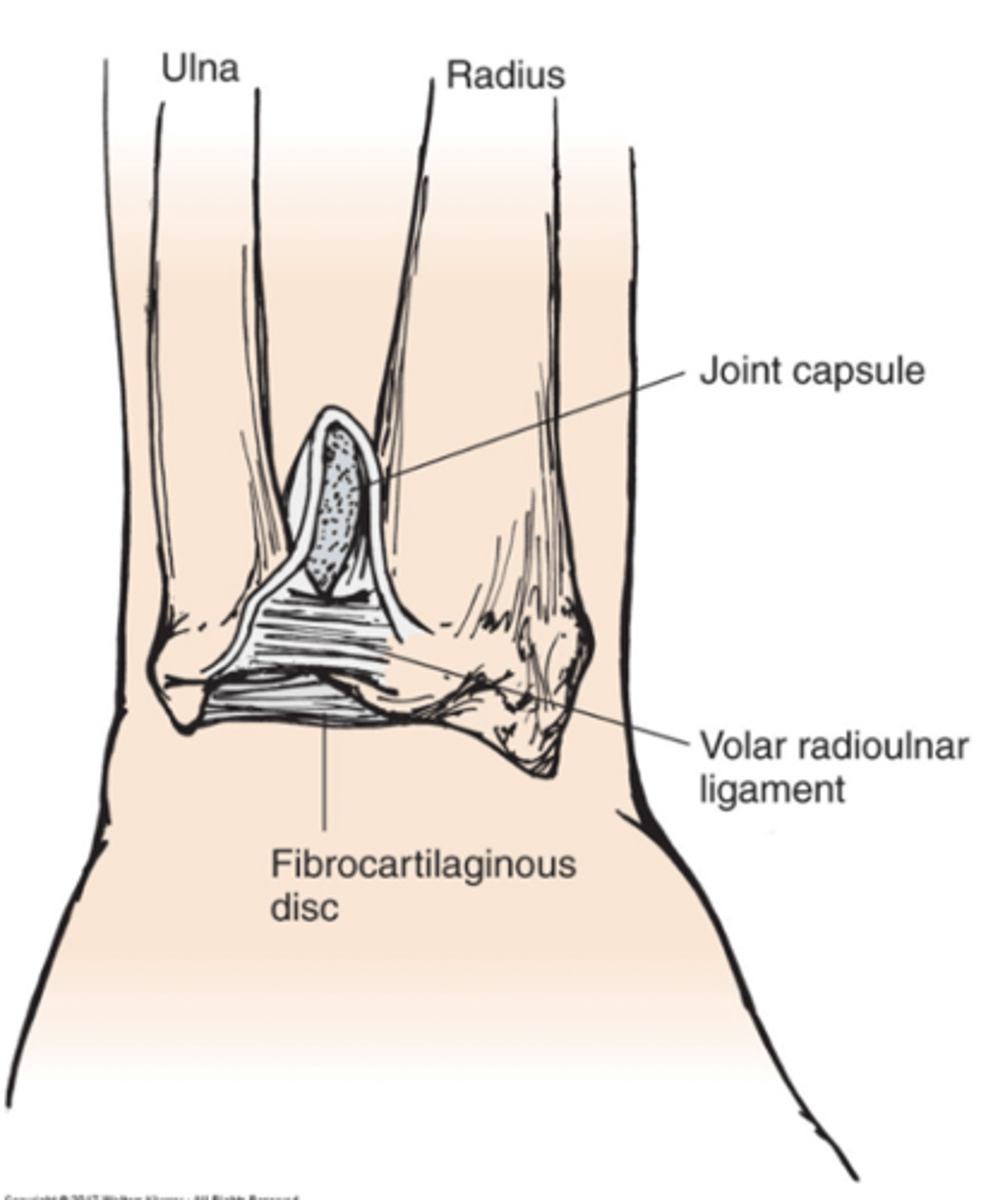
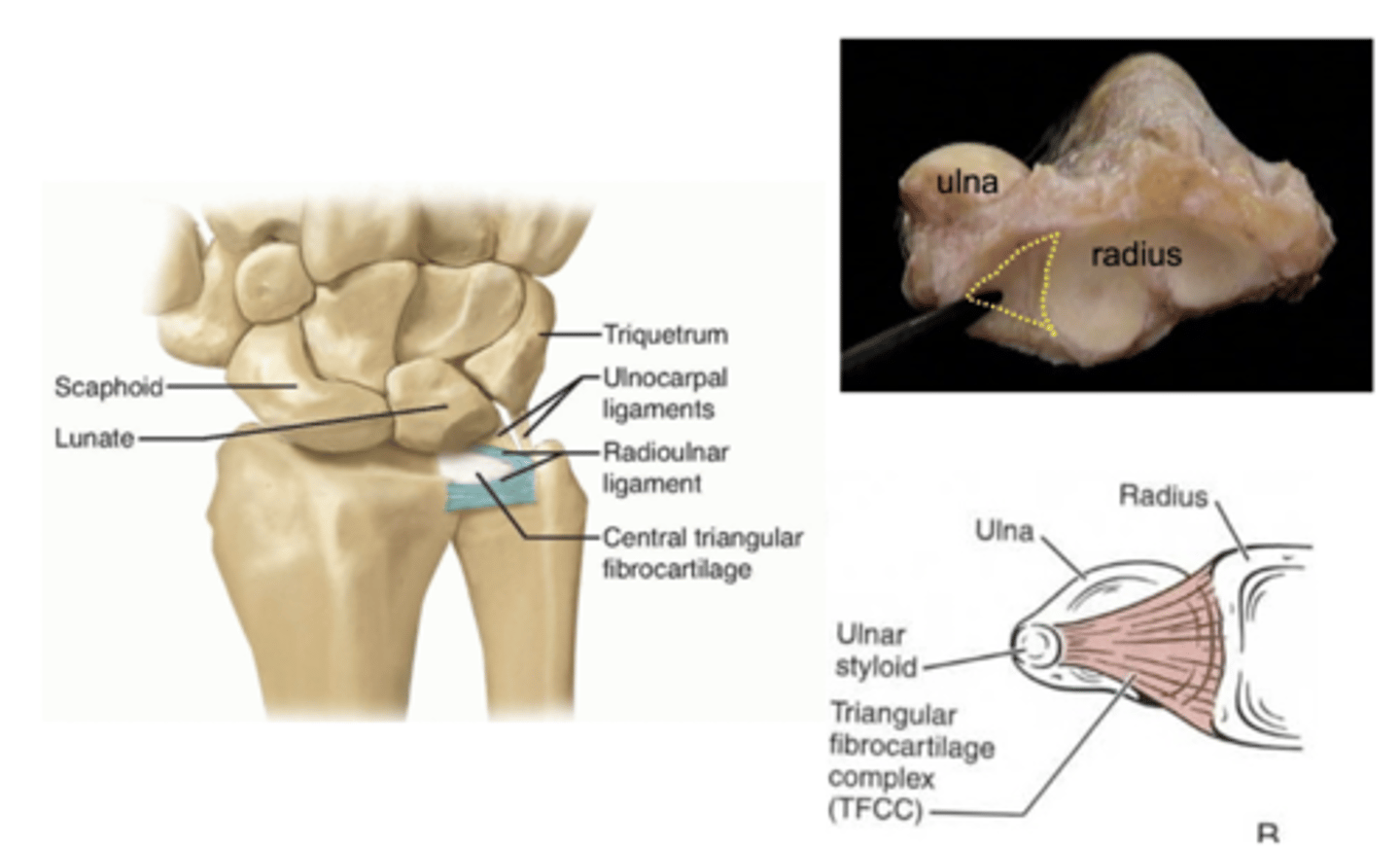
triangular fibrocartilage complex consists of:
- triangular fibrocartilage
- dorsal and palmar radioulnar ligaments
TFCC
- relative lengths of the distal articular surfaces of the radius and ulna.
neutral UV = both the ulnar and radial articular surfaces at the same level
positive UV = ulnar articular surface > 2.5 mm distal to that of the radius
negative UV = ulna is >2.5 mm proximal to the radius
Ulnar variance

Forearm rotation
- normal ROM 75-85° pronation to 80-90° supination
Axial load transmission
The three components of the forearm function together to achieve:
50degrees pronation-50 supination
What range of pronation - supination is required to accomplish most activities of daily living?
Full pronation
The interosseous ligament is most lax in which position of forearm rotation?
neutral to 60 degrees supination
Greatest axial load transmission across the proximal and distal radioulnar joints occurs in
Biceps brachii and supinator
Two forearm supinators
