INTRAOP PT.2
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
37 Terms
Methods of Administration of Regional Anesthesia
Topical Application
Anesthetic agent applied directly into the mucosal membrane to a serous surface or into an open wound.
It blocks the peripheral nerves around the incision site.
They are available as
creams
ointments
solutions
eye drops
gells
sprays
may be applied such as the skin, inside the mouth or throat, in the nose, or in the eyes.
Local Infiltration Anesthesia/ Local Anesthesia (LA)
injected into the tissue around the incisional area
producing temporary loss of sensation in a limited area.
Field Block
Anesthetic agent is introduced around the operative field through a series of injections
to block the nerves supplying that area, providing anesthesia for larger regions than local infiltration.
Peripheral Nerve Block (PNB)
administered directly into or around one nerve or group of nerves into the involved area that control sensation and movement to a specific part of the body.
Intravenous Block ( Beir block )
often used for arm, wrist and hand procedure
is a type of regional anesthesia where a local anesthetic is injected into a vein, causing temporary numbness and loss of sensation in the distal part of the limb.
an occlusion tourniquet is applied to the extremity to prevent infiltration and absorption of the injected IV agents beyond the involved extremity
Caudal Anesthesia/Caudal Block
Is produced by injection of the local anesthetic into the caudal or sacral canal or anesthesia in the perineum
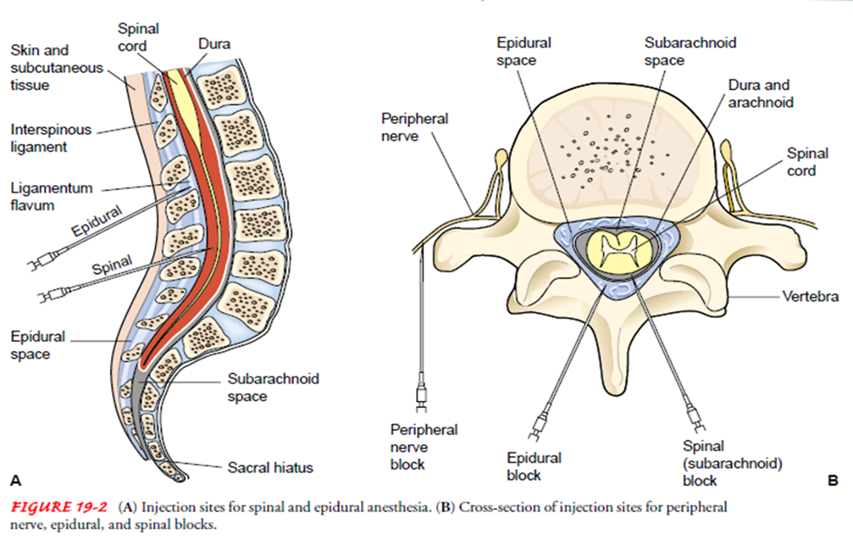
Spinal Anesthesia/Sub-arachnoid Block (SAB)
Anesthetic agent is introduced into the cerebrospinal fluid (CSF) in the subarachnoid space
Epidural Anesthesia
Administered into the epidural space.
It involves injecting a local anesthetic into the epidural space around the spinal cord, providing pain relief for surgeries or labor.
Sometimes a small tube or catheter is inserted into the epidural space, which allows the anesthesiologist to administer more medications as needed.
often used when long term pain relief is needed
Types of Epidural Anesthesia
Continuous Lumbar Epidural Anesthesia (CLEA)
Combined Spinal Epidural Anesthesia (CSEA)
Continuous Thoracic Epidural Anesthesia (CTEA)
Continuous Lumbar Epidural Anesthesia (CLEA)
continuous injection of an anesthesia solution into the sacral and lumbar plexuses within the epidural space to relieve the pain of childbirth
also used in general surgery to block the pain pathways below the navel.
Combined Spinal Epidural Anesthesia (CSEA)
a regional anesthetic technique, which combines the benefits of both spinal anesthesia and epidural anesthesia.
The indwelling epidural catheter gives the ability to provide long lasting analgesia and to epidural and to titrate the does given to the desired effect.
Continuous Thoracic Epidural Anesthesia (CTEA)
Thoracic epidural analgesia remains a critical tool for anesthesiologist to use in acute pain.
Is particularly effective for reducing pain after thoracic and abdominal surgery, and rib fractures
Injection Sites
Dangers During Operation Under Anesthesia
ANAPHYLACTIC SHOCK - caused by idiosyncrasy of the anesthetic.
ASPIRATION - may occur during abolition of throat reflexes when the patient is unconscious.
BRONCHOSPASM & LARYNGOSPASMS - are caused by certain allergic conditions.
CEREBRAL EDEMA - from cerebral hypoxia. As prevention, move anesthetized patient gently & slowly to allow the circulation to adjust to position to change
CEREBRAL HEMORRHAGE - caused by sudden increased in blood pressure.
CARDIOVASCULAR OCCLUSION - from sudden drop of blood pressure.
CORONARY THROMBOSIS - from severe hypoxia.
CIRCULATORY DEPRESSION OR SHOCK - caused by hemorrhage, fast moving of the unconscious patient, rough handling of tissues, or severe fright.
CARDIAC ARREST - a sudden cessation of cardiac function.
CONVULSIONS - caused by carbon dioxide retention, air embolism, over dosage of regional drugs.
EMBOLI - air embolism may result from accidental introduction of air into the circulatory system.
HEMORRHAGE - may cause shock, cardiac arrhythmia, or even death
Draping
Procedure of covering the patient and surrounding areas to create and maintain an adequate sterile field
An effective barrier eliminates or minimizes passages of microorganisms between nonsterile and sterile areas
Also promotes/protects privacy of the patient
Purpose: to create and maintain an adequate sterile field during operation.
Counting
Method of accounting for items placed on the sterile table for use during the surgical procedure
Sponges, sharps and instruments should be accounted for all surgical procedures
Usually done 3 times
Baseline count
1st closing count
2nd closing count
Baseline count
during set-up for the surgical procedure
As scrub nurse touches each item, he/she and the circulator count each item ALOUD until finished.
Circulator then documents count for each type of item
Counting should not be interrupted
If the scrub/circulator is PERMANENTLY relieved by another person during surgery, the incoming person should verify all counts.
1st closing count
done before the surgeon starts the closure of a body cavity or a deep large incision
Field count – surgical field
Table count – Mayo stand and instrument table
Floor count – materials recovered from the floor
2nd closing count
done during skin closure
Circulator totals the field, table and floor counts
If final count = total in the tally sheet, circulator informs the surgeon that counts are correct
Incorrect count
The surgeon is informed immediately
The entire count is repeated
Circulator – searches the trash receptacle, under the furniture, floor, laundry hamper and throughout the room
Scrub – searches the drapes and items in the OR table and Mayo stand
Surgeon – surgical field and wound
Circulator – inform OR supervisor to check count and assist with search
If all measures exhausted: X-ray
Circulator – completes an Incident Report (IR)
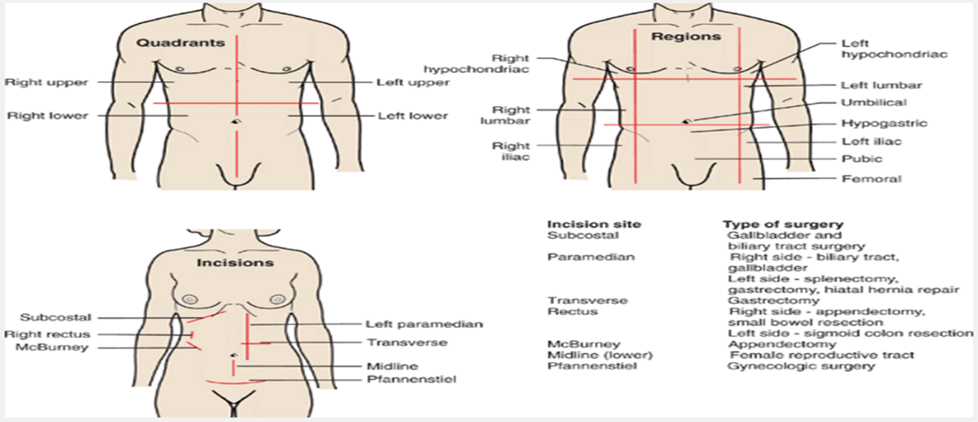
Common Surgical Incision
Butterfly incision – for craniotomy
Limbal incision – for eye surgeries
Halstead / Elliptical incision – for breast surgeries
Abdominal incision – for abdominal surgeries
McBurneys incision – for appendectomy
Pfannenstiel – for CS
Lumbotomy or transverse incision – for kidney surgeries
The choice of the incision is made by the surgeon with the following considerations:
Type of surgery (anatomical location)
Maximum exposure
Ease and speed of entering (for emergency surgery)
Possibility of extending the incision
Maximal post operative wound strength
Minimal post operative discomfort
Cosmetic effect
Five Main Layers of Abdominal Cavity
Skin – interrupted stitch, cutting needle is used
Subcutaneous (yellow) - not always sutured, round needle
Fascia (white) – interrupted stitch, cutting needle
Muscle (red) – interrupted stitch
Peritoneum (white) – continuous stitch, round needle viscera
****Uterus (dark violet) – continuous stitch, round needle is used
Skin Closure
Ligature/”tie”: A material that is tied around a blood vessel or any hollow organ to occlude its lumen
Suture: Any material used to sew, stitch or hold tissue together until healing occurs
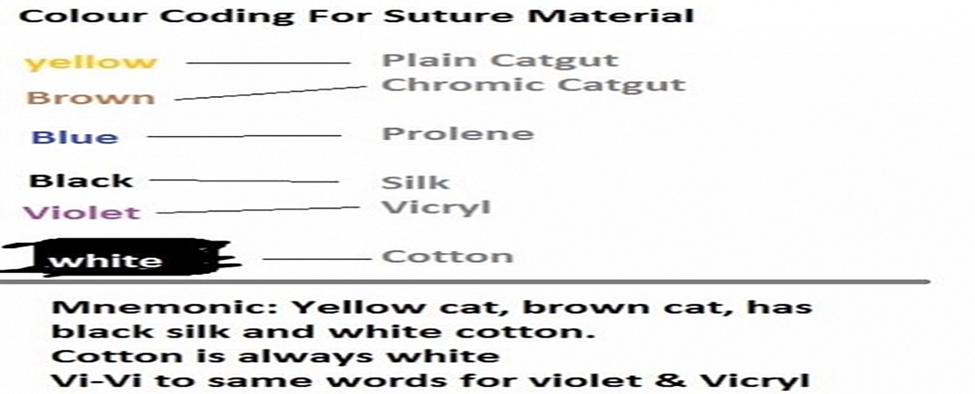
Types of Suture
Absorbable suture
digested by body enzymes during the wound healing process
e.g. surgical gut (catgut) collagen and synthetic
Non-absorbable suture
made from various materials that are not affected by the digesting enzymes
remains encapsulated when buried in tissues and is removed post-operatively when used as skin sutures
e.g. Surgical silk, Surgical cotton, Dacron, Nylon, Polythylene, Stainless steel
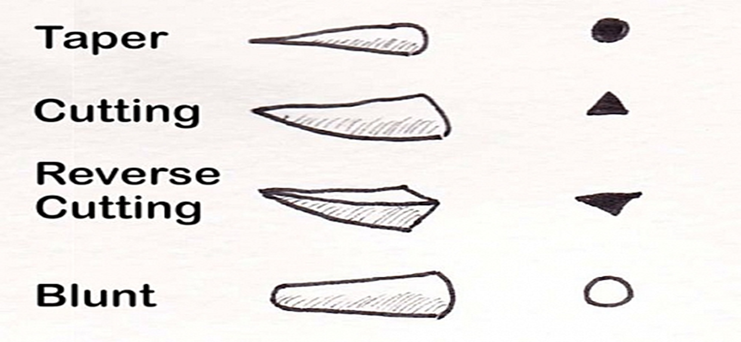
Needle types edges in surgical sutures
Sizes and Needles of Surgical Sutures
Just as in Canula, the higher the number on surgical sutures, the smaller the size.
The sizes range from sizes 1.0 to 7.0 but in chromic suture, it is larger than 1.0
Types of Suture Needles
Cutting needles- cross-section is triangular, it is very sharp and/traumatic and is used for skin
Non-traumatic needle- cross section is round, used for subcutaneous tissue and bowel
Time frame taken for absorption or removal of sutures after surgery
1. Non absorbable sutures take about 7-10 days
2. Sutures used on the Head and neck can be removed after 3-5 days
3. Chest wall and upper limb takes 5-7 days
4. Abdomen takes 7-10 days
5. Lower limb takes 10-14 days.
These are highly determined by blood supply to the affected area. The more the blood supply, the less the time it takes for the surgical wound to heal, hence the sutures can be removed early.
Intraoperative Complications
Hypoventilations & Hypoxemia
Nausea/Vomiting
Oral trauma (broken teeth, oropharyngeal, or laryngeal trauma)
Hypotension
Cardiac Dysrhythmia
Hypothermia
Headache
Peripheral Nerve Damage
Malignant Hyperthermia
Malignant Hyperthermia
A rare reaction to anesthetic inhalants (notably sevoflurane, enflurane, isoflurane, and desflurane) and muscle relaxant, succinylcholine
Caused by abnormal and excessive intracellular accumulations of calcium with resulting hypermetabolism, increased muscle contractions, and elevated body temperature
Treatment consists of discontinuing the anesthetic inhalant, administration of IV dantrolene sodium (Dantrium), and applying cooling techniques (e.g. cooling blanket, iced saline lavage)
Nursing Process of Intraoperative Period: Assessment
Classify the client’s physical status for anesthesia
a. no organic or systemic disturbance
b. mild disturbances like mild cardiac disease, mild diabetis mellitus
c. severe systemic disturbances like poorly controlled diabetes mellitus, pulmonary complications
d. life-threatening systemic disease like severe renal or cardiac disease
e. moribound with little chance of survival like rupture aortic aneurysm
2. Assess the client’s record for appropriate documentation including the ffg.:
a. current signed consent form
b. completed history and physical assessment record
c. recent laboratory and diagnostic reports
d. evaluation of the client’s overall physiologic, emotional and psychological status
3. Specifically ask the client about any known allergies.
4. Verify client identification & that the correct surgery is scheduled.
5. Assess for special surgical considerations and precautions
a. locations where an electric grounding plate can be safely placed on the client
b. avoiding areas where metal or a prosthesis is present
c. shielding with a lead apron if radiation is involved if the client is pregnant
6. Assess the client’s risk for accidental hypothermia or malignant hyperthermia during anesthesia administration and surgery
Nursing Process of Intraoperative Period: Nursing Diagnosis
Risk for fluid volume deficit or excess
Risk for hypothermia or hyperthermia
Risk for infection
Risk for altered tissue perfusion cardiac, respiratory and peripheral
Risk for injury
Nursing Process of Intraoperative Period: Planning
The major goals for the client during the intra-operative period may include maintenance of fluid balance, maintenance of normothermia, prevention of infection, adequate tissue perfusion and absence of injury
Nursing Process of Intraoperative Period: Implementation
Promote measures that maintain adequate fluid and electrolyte balance
a. monitor intake & output accurately; use a urometer if needed
b. assess the client for dehydration to include skin turgor & mucous membranes
c. assess the client for circulatory overload to include breath sounds, peripheral edema and jugular vein distention
d. monitor pertinent electrolyte values.
2. Promote measures that maintain the client’s normal temperature of 36.6 C to 37.5C
a. ensure that OR temperature is between 20C & 25C
b. warm all intravenous and irrigating solutions
c. monitor the client’s temperature continuously
d. remove all wet gowns and drapes promptly & replace with dry to prevent heat
3. Promote measures that decrease risk of infection
a. maintain sterile procedures and techniques during surgery
b. apply sterile dressings to all wounds
c. unscrubbed personnel refrain from touching or contaminating anything that is sterile
4. Promote measures that ensure adequate tissue perfusion in the client during surgery.
a. Assess the client’s vital signs continuously.
b. Asses the client’s respiratory status, & assist with mechanical ventilation.
c. Assess the client’s cardiovascular status.
d. Assess the client’s peripheral vascular status.
5. Ensure the client’s safety in the OR
a. Set room temperature & humidity to prevent hypothermia
b. Remove any potential contaminants
c. Curtail unnecessary room traffic.
d. Keep room noise & talk at a minimum.
e. Recheck electrical equipment for proper operation.
f. Make sure that necessary equipment & supplies are available.
g. Ensure that instruments, sutures, & dressings are ready.
h. Count & record sutures, needles, & instruments, & sponges.
i. Make sure that staff call the client by name & provide individualized attention.
j. Assist in transferring the client to the OR table.
k. Cover the client with a warm blanket, & attach the safety strap
L. Remain at the client’s side during anesthesia induction.
m. Verify proper client positioning to protect nerves, circulation, respiration, & skin integrity.
Always pad pressure areas.
n. Ensure that newly requested items are quickly supplied to the anesthesia or scrub team by the circulating nurse.
6. Perform other actions as appropriate.
a. Act in the role of client advocate, providing privacy & protection from harm.
b. Follow established procedures & protocols.
c. Document all OR care.
d. Help coordinate health team activities.
e. Promote ethical behaviors (eg, respect, confidentially).
f. Monitor blood, fluid, & other drainage output.
g. Maintain a quiet, relaxing atmosphere. Remember, the client can hear
h. Apply grounding pad.
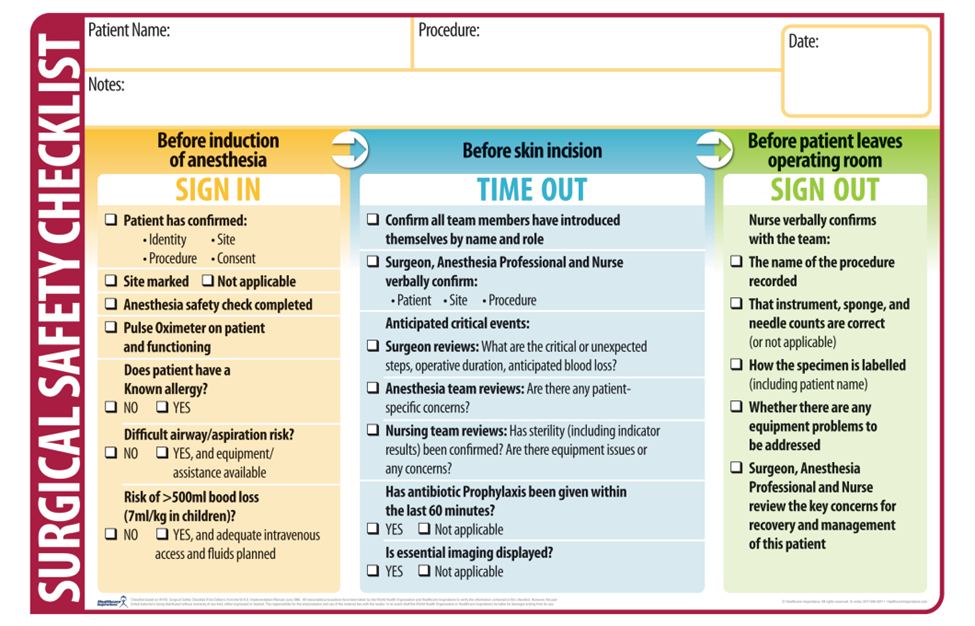
The Surgical “Time Out”
“an immediate pause by the entire surgical team to confirm the correct patient, procedure, and site,” was introduced in 2003, when The Joint Commission’s Board of Commissioners approved the original Universal Protocol for Preventing Wrong Site, Wrong Procedure, and Wrong Person Surgery for all accredited hospitals, ambulatory care centers, and office-based surgery facilities.
represents the last part of the Universal Protocol and is performed in the operating room, immediately before the procedure is initiated.
The "time out" represents the final recapitulation and reassurance of accurate patient identity, surgical site, and planned procedure
have active involvement of the entire surgical team. This means there is 100% oral or visible agreement (nod or gesture) following the time out statement.