PSY 202Z MIDTERM #2 UNIVERSITY OF OREGON
1/191
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
192 Terms
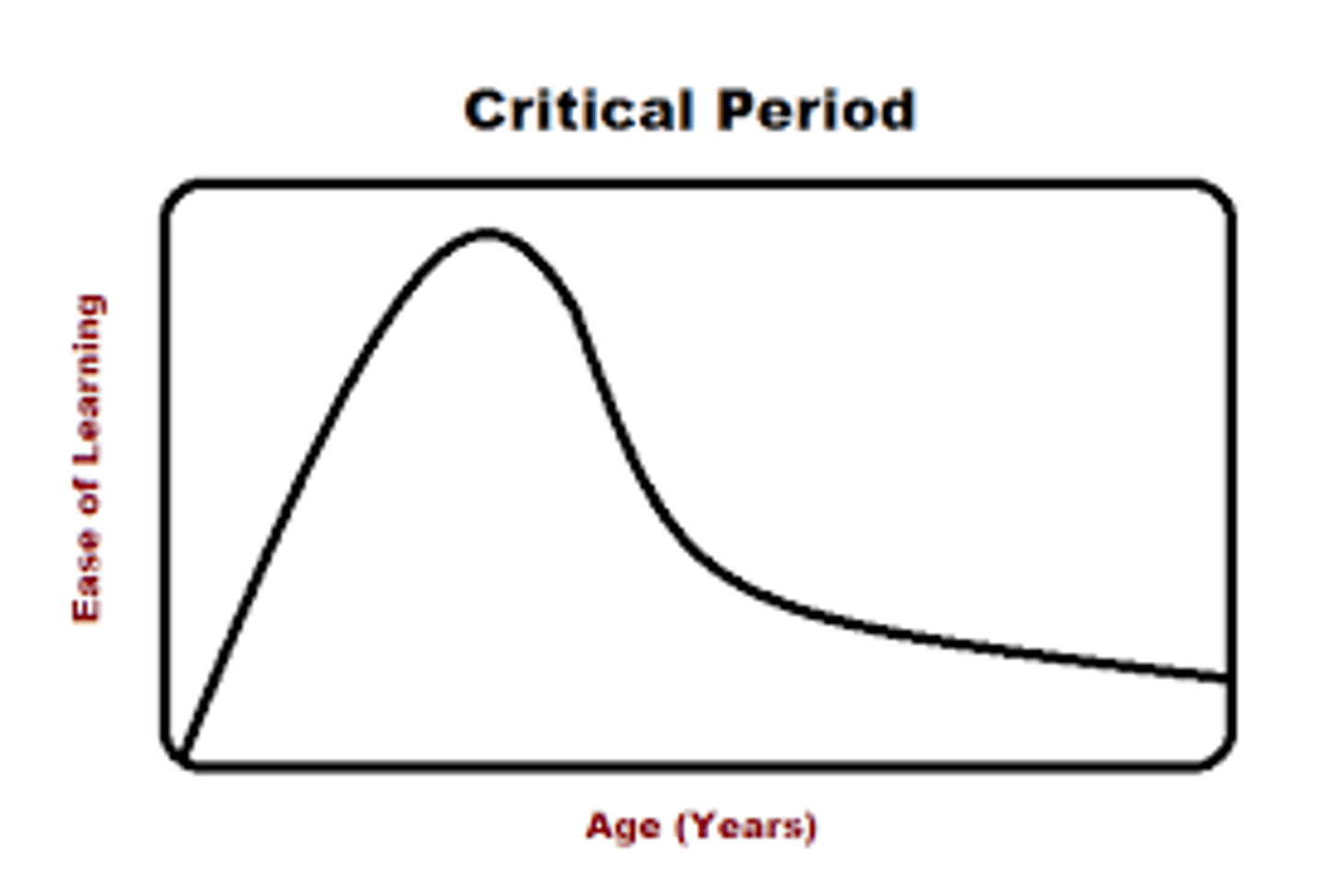
Critical Period
Age range during which certain experiences must occur for development to proceed normally; precisely defined; narrow ranges of time.
- Start & endpoints: clear; discontinuous/ drop-off.
- Ex. prenatal development, acquisition of one's native language.
Sensitive Period
An optimal age range for certain experiences, but if experiences occur at another time, normal development is still possible.
- Start & endpoints: more gradual; continuous.
- Ex. second language, attachment to primary
caregivers, identity formation.
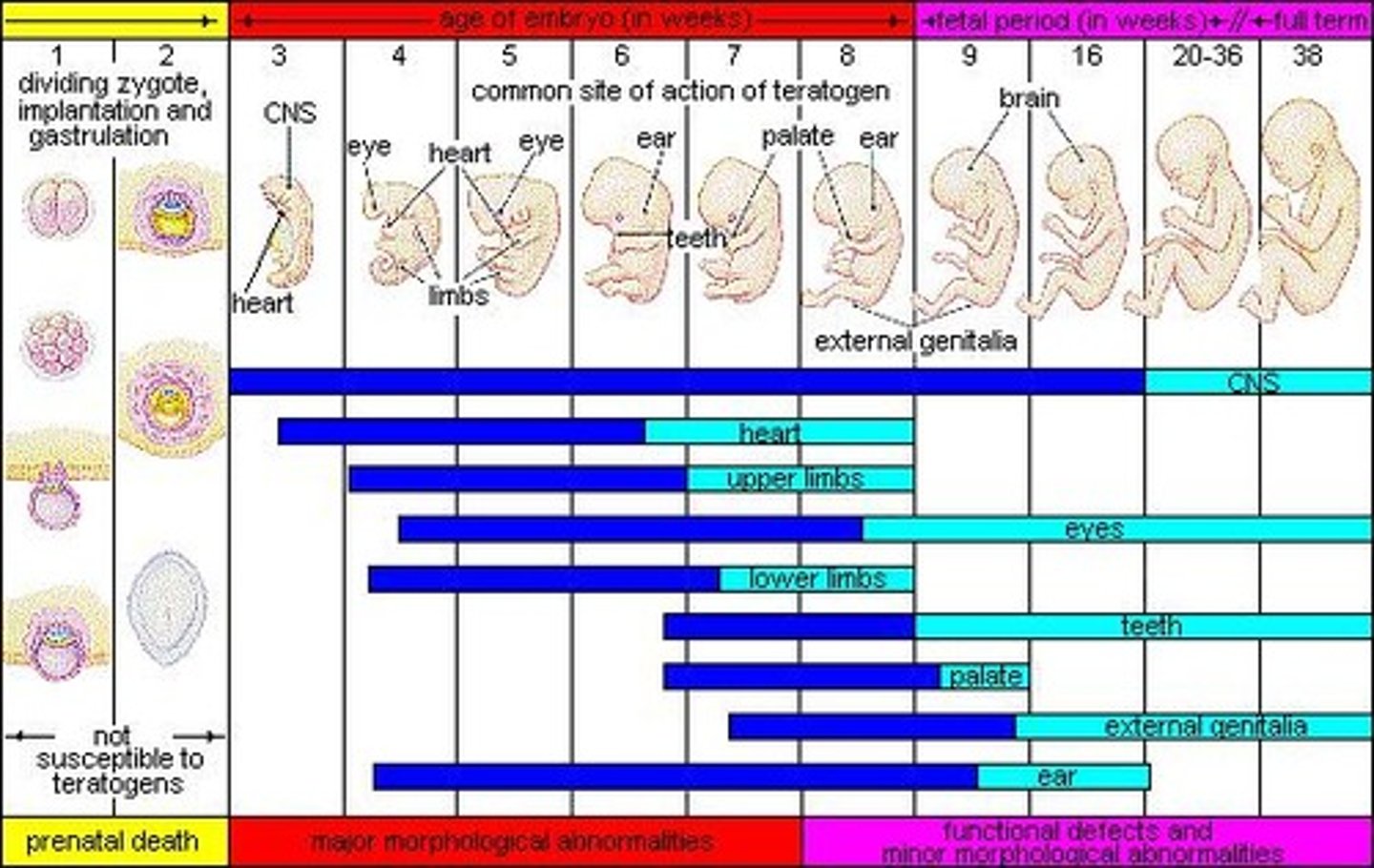
Teratogens (Post/Pre-Natal):
"Developmental toxicity"
Pre-Natal: some medications, recreational drugs, tobacco products, chemicals, alcohol, certain infections, and high stress in pregnant people.
Post-Natal: social deprivation.
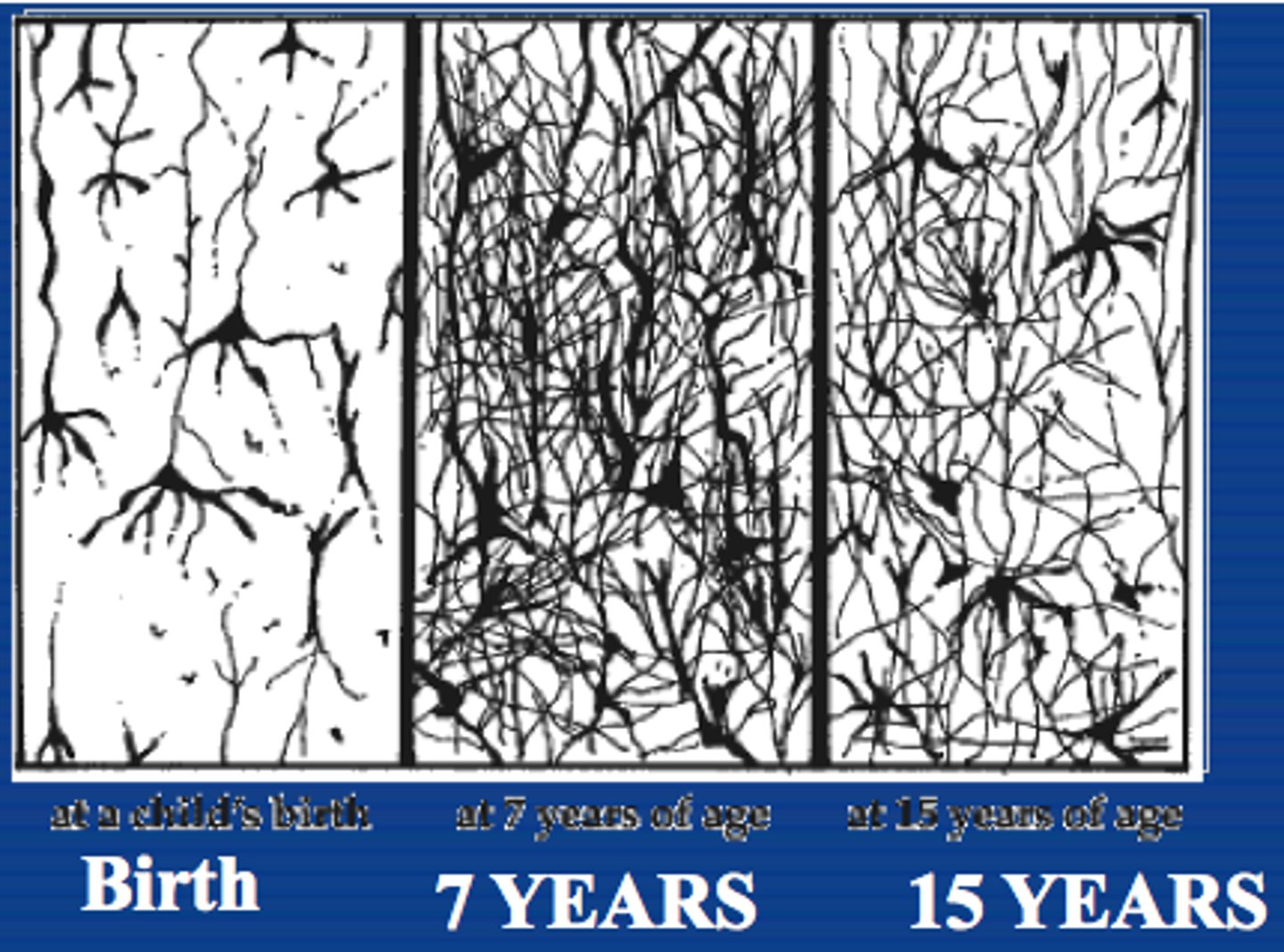
Synaptic pruning
a process whereby the synaptic connections in the brain that are used are preserved, and those that are not used are lost
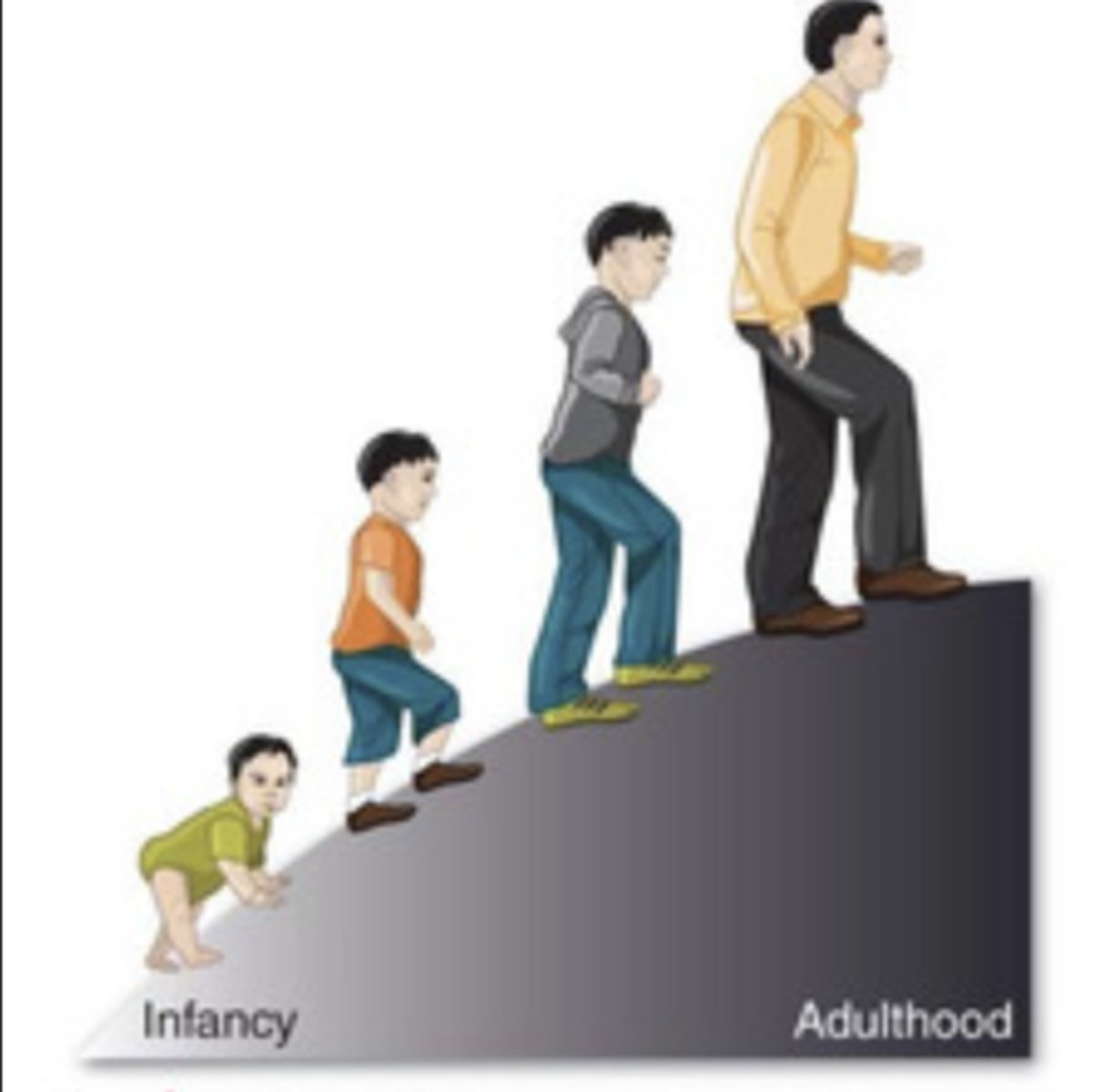
Continuous development
gradual alteration of behavior or capacity
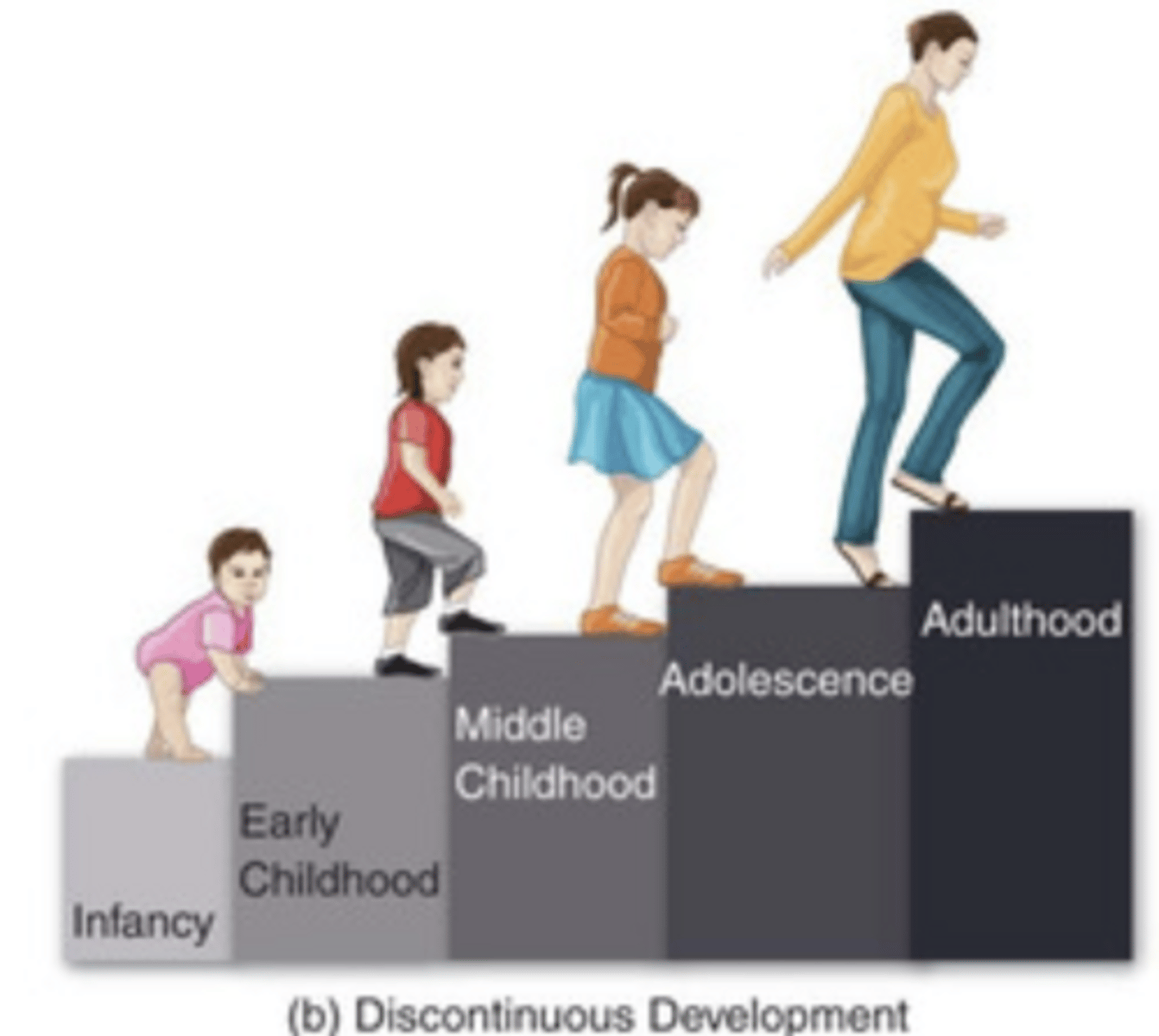
Discontinuous development
stages of growth that are qualitatively different from one stage to the next
Nativistism
The view that certain skills (e.g., language) are
"native" or hard-wired into the brain at birth.
AND: environmental inputs are insufficient to account for how fast we learn language… “biological predispositions.”

Empiricism
The view that the brain has inborn capabilities
(e.g., to detect patterns and irregularities) for learning from
the environment (e.g., can learn language)..."learning
mechanisms and environment."
Plasticity
The brain's ability to change, especially during childhood, by reorganizing after damage or by building new pathways based on experience
How do nature and nurture shape development?
- We are embedded in socio-cultural contexts that shape our development.
- Contexts and the influences of our environments change with time/historical periods.
Dynamic Systems Theory:
• Development is a self-organizing process that emerges through interactions between our biology and environment as we confront new task demands.
• Development advances as a person encounters the environment, receives feedback from the environment, and incorporates/updates/changes behaviors.
Language development: Significance of first vs. second language learning (check)
Role of Language in Cognitive Development
- Language provides a way for information to be transmitted:
- Intellectual adaptation: Language not only helps in communication but is also an important tool that facilitates thinking.
Language development: Stages of language learning
Birth to 3 months:
- actions generate sounds
• 3 to 5 months:
- begin cooing & laughing
• 5 to 7 months:
- babbling (da, ma, ba)
• 7 to 8 months:
- canonical babbling (bababa)
• Approx. 12 months:
- first word
• 18 to 24 months:
- telegraphic speech (”Me hungry”)
Language development: Understand how and why infants/children go from being able to learn any language to losing that capacity (as well as the exceptions to this loss).
• (6 mo old) can discriminate actual speech sound patterns in any
language from non-speech patterns.
• This ability is nearly gone for non-native languages by 12 months; babies are now "culture-bound" language learners.
• Babies are learning the "statistical patterns" of their language.
• But, you can maintain this discrimination through continued person-to-person exposure to a non-native language.
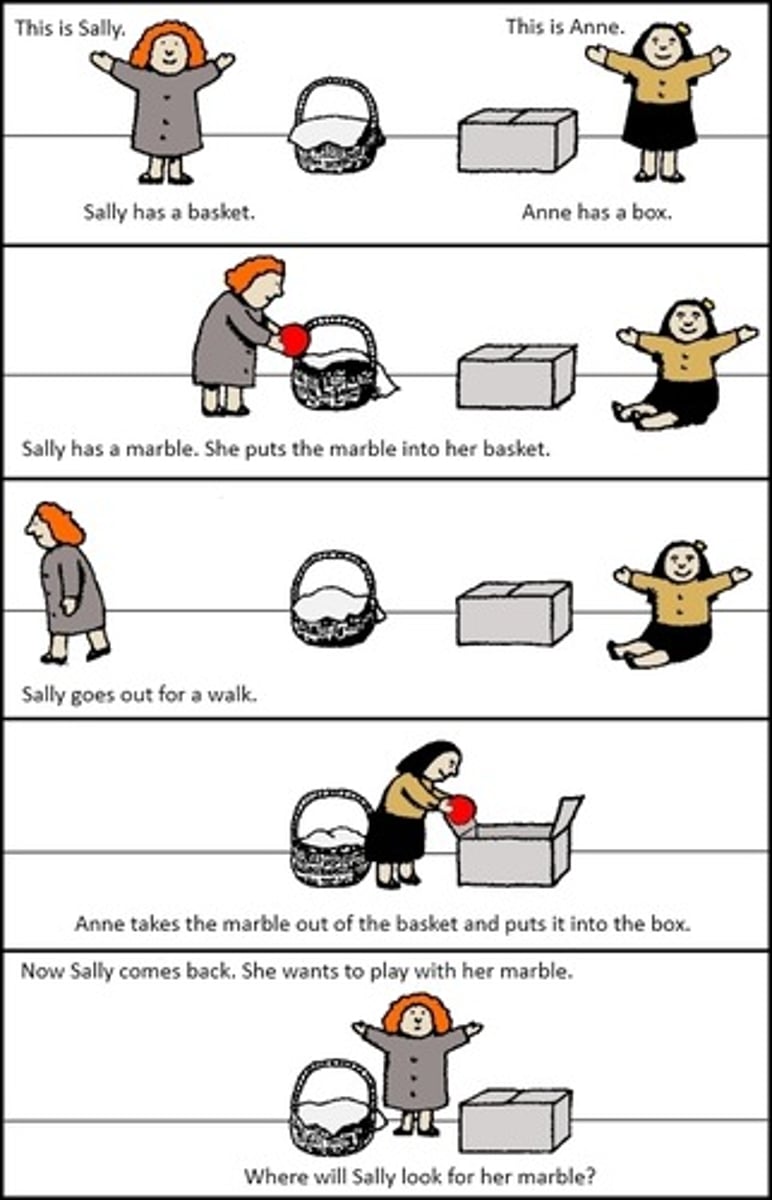
Theory of Mind (ToM): how to describe and what is gained with the acquisition of ToM
We begin to understand that others can think and want differently from us.
- Key aspect of Social Cognition.
- Also in learning deception.
Piaget's theory of learning: schemas, equilibrium, & disequilibrium
Schemas: The basic building blocks of knowledge; mental models used to organize and interpret information.
Equilibrium: A state of balance where a person’s existing schemas can explain new, incoming information.
Disequilibrium: A state of cognitive conflict, confusion, or "unpleasantness" that occurs when new information cannot be understood through existing schemas (which motivates individuals to adjust their thinking through accommodation to regain equilibrium).
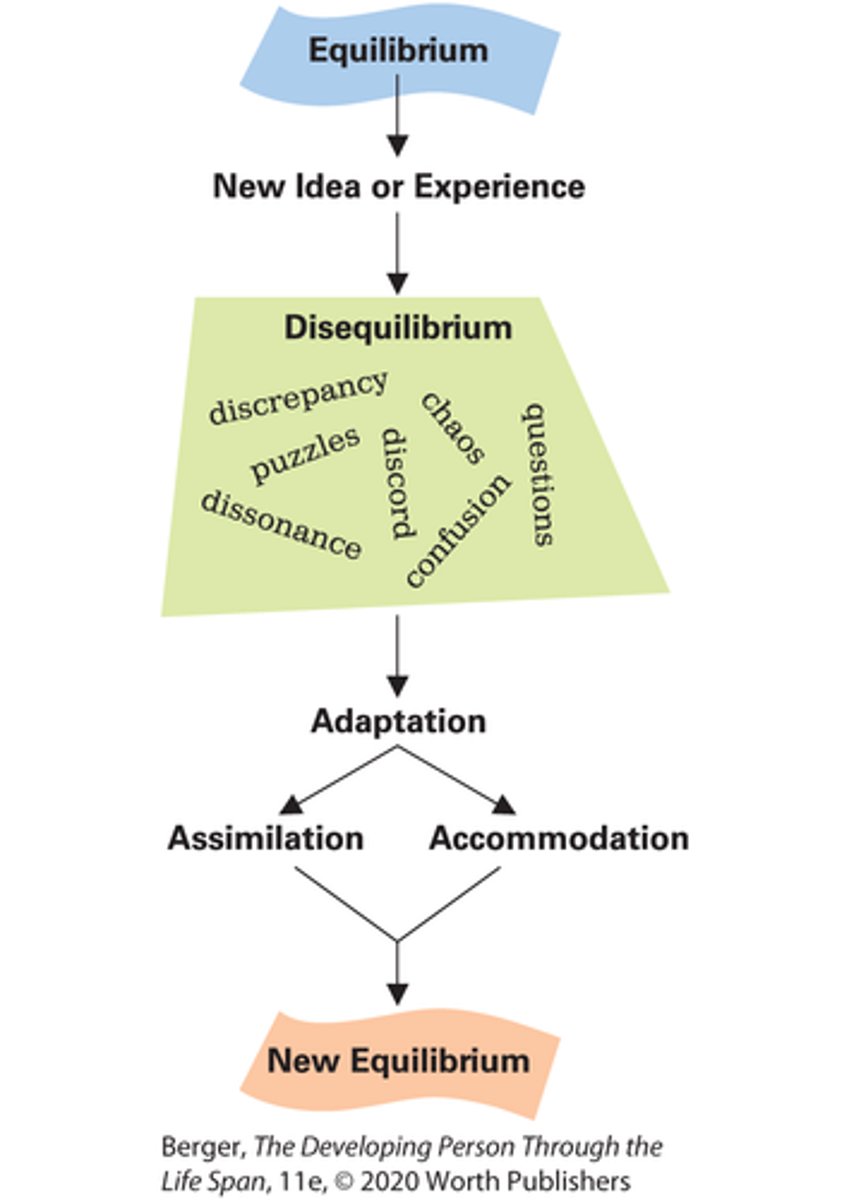
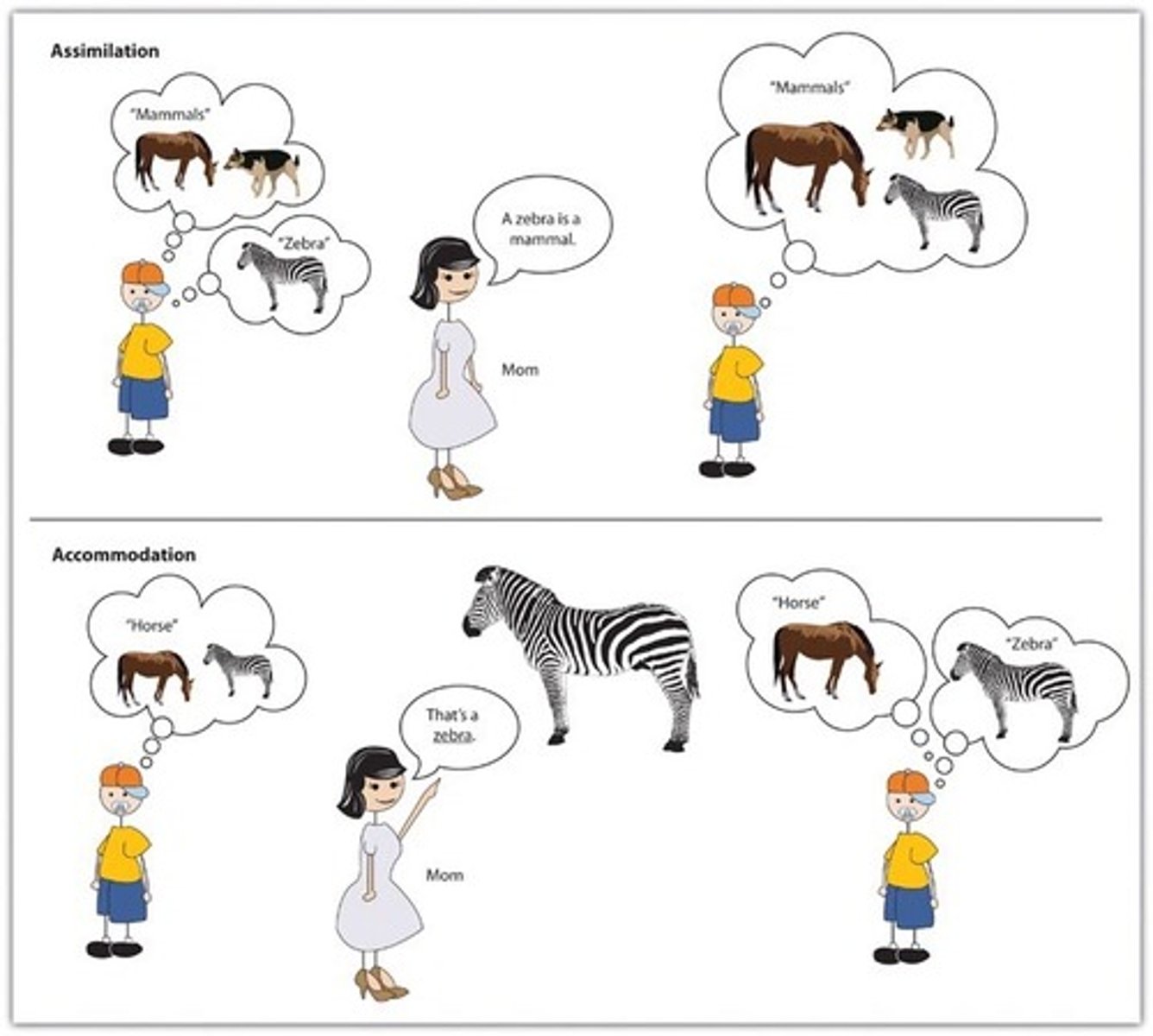
Piaget's theory of learning: assimilation & accommodation
Assimilation:
- Process of fitting new info into pre-existing cog. schemes.
- New experiences are reinterpreted to fit into, or assimilate with, old ideas.
Accommodation:
- The process of taking new info and altering pre-existing schemas in order to fit in the new info.
- This happens when the existing schema (knowledge) does not work and needs to be changed to deal with a new object or situation.
Piaget's stages of cognitive development: Sensorimotor
- Birth to 2 years
1. Acquire information through their senses and motor exploration.
2. Early motor and cognitive development is highly intertwined
3. Earliest schemas are reflex patterns (i.e., rooting)
4. By 2 months, awareness of self as an agent of action; begins to act intentionally.
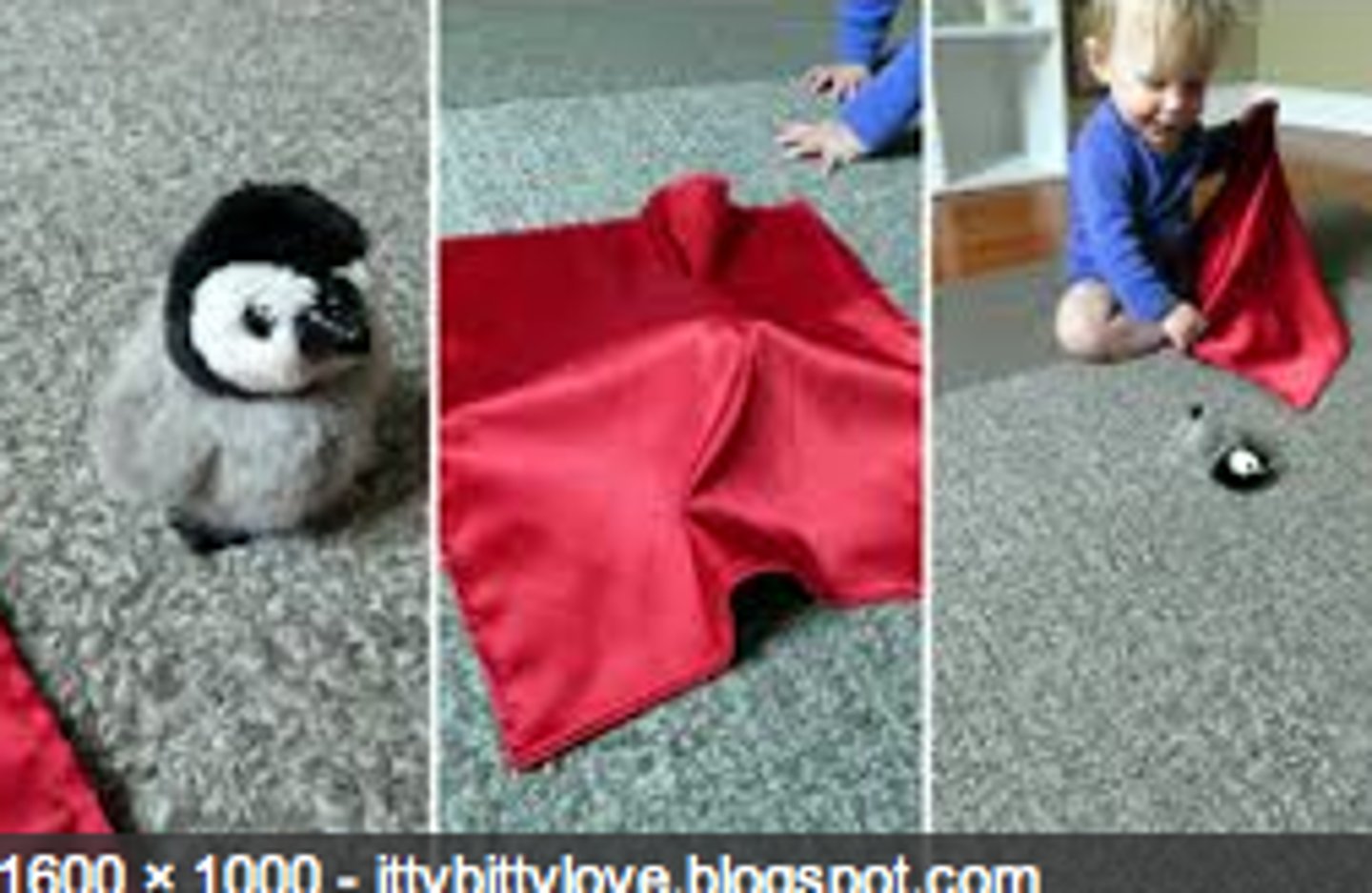
5. Achievement of object permanence; sometime around 6-8 months
Object Permanence
Knowing that objects still exist when out of sight
Results:
- Memory Development
• Problem-Solving Skills
• Separation Anxiety
Piaget's stages of cognitive development: Preoperational
- 2 to 7 years
1. Uses language, begins to represent objects with images and words
2. Reasons intuitively and largely based on appearance
3. Centration / lack of conservation
- Young pre-opp thinkers cannot focus on other
relevant features of a situation; they are “stuck” on what they see and understand initially.
4. Egocentric thinking (early months of stage): cannot take another’s viewpoint
Centration
The process of concentrating on one clearly visible but limited aspect of a stimulus and ignoring other aspects

Piaget's stages of cognitive development: Concrete Operational
- 7 to 12 years
1. Achieves Conservation
2. Increased classification skills using multiple features (i.e., size, shape, quantity)
3. Beginning of logical (if then) reasoning
4. End of egocentrism
5. Still unable to reason abstractly (even if told to do so)…very “concrete.”

Conservation
Knowledge that an object's essence (shape, quantity) can be distinct from the object's arrangement and physical appearance.
Piaget's stages of cognitive development: Formal Operational
- 12 years and older
1. Able to think logically and abstractly
2. able to generate and systematically test hypotheses
3. able to consider multiple viewpoints at once
4. Cognitive limitations related to limited experience:
-Ex. thoughts/feelings of invincibility.

Criticisms of Piaget's Stage Theory
1. Piaget underestimated the age at which some skills come online or what motivates a skill.
2. Children move back and forth within and between stages.
3. Young children have more innate knowledge than Piaget thought.
4. Not much room for differences across individuals or across cultures...yet vast individual and cultural variations exist.
5. Piaget underestimated the role of others in infant/child learning.
Vygotsky's Zone of Proximal Development
A caregiver helps to bridge a child's current level and abilities with experiences and attainments that would otherwise be outside of their reach.
- Use "scaffolding" to create this bridge.
- Different cultures think differently about when a child is ready and able to learn.

Socialization
Where knowledgeable "teachers" introduced us to (and we hopefully internalize) the social and cultural norms of our immediate communities.
• Develop the social, cognitive, and emotional capacities necessary to manage a complex interpersonal world.
• 2 key processes: Primary & Secondary socialization
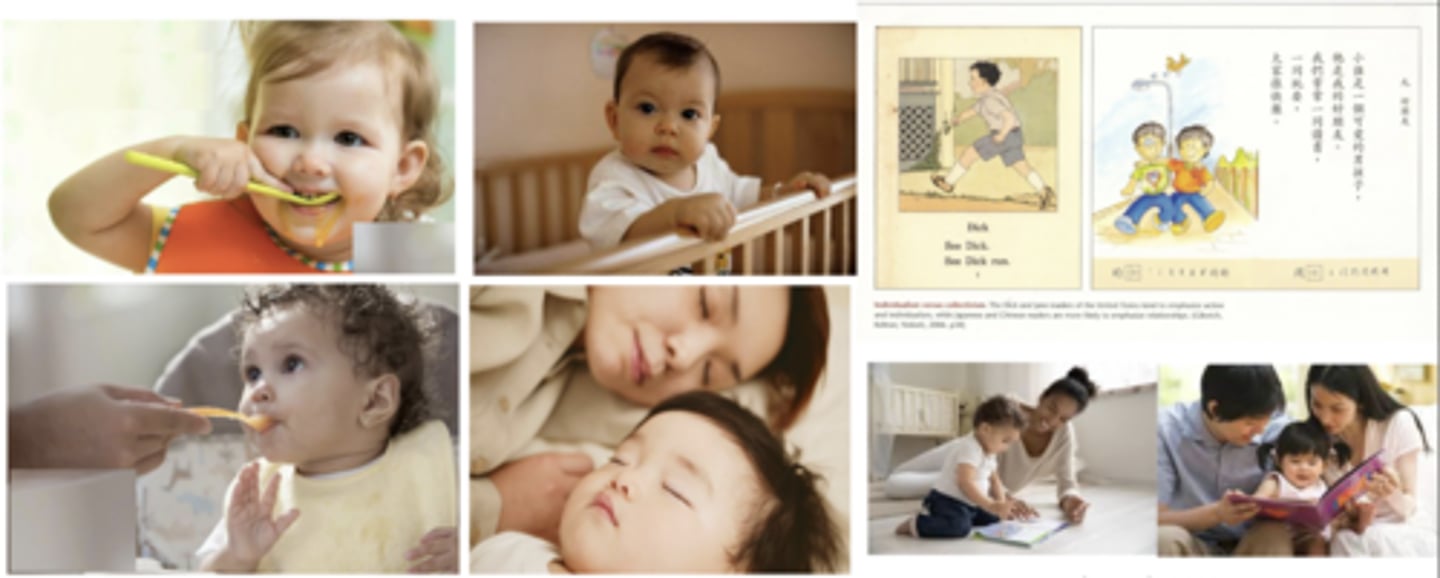
Socialization: cultural differences (PRIMARY)
PRIMARY:
1. Co-sleeping is a dominant model worldwide:
- Independent cultures like the U.S. (kids in crib)
- Collectivist cultures like Japan (kids in bed with parents)
2. Feeding:
- Ind. cultures like the U.S. (kids learn to eat themselves quicker)
- Coll. cultures like Japan (kids are fed by parents longer)
3. Reading:
- Ind. cultures like the U.S. (books emphasize independence and action)
- Coll. cultures like Japan (books emphasize relationships)
Socialization: cultural differences (SECONDARY)
SECONDARY:
WESTERN:
- emphasis on balancing academics w/ extra curriculars
- personal interests
- well-being/self-esteem foregrounded
- success seen as ability-based
EASTERN:
- emphasis on academic success as a moral duty
- family honor
- success seen as a reflection of effort
Industrialized VS Rural or lower-income contexts:
- INDUSTRIALIZED: Adolescence often includes a prolonged transition to adulthood (thru 20's).
- RURAL: Adolescents assume adult-like responsibilities earlier—work, caregiving, or household management.
Primary Socialization
Occurs in early childhood when a child is taught and learns the basic skills needed to survive in a specific society or as a member of a particular culture.
• Ex: How to dress, hygiene, eating with utensils, first language, how to act/self-regulate emotions.
Secondary Socialization
Refers to the process of continual learning throughout life about the norms, values, and behavior of the larger society, but also within smaller, more specific groups/new roles, and new social situations.
• Key agents of secondary socialization (Think: parents punch sock-wearing rat monsters):
- parents (still)
- peers
- school settings
- workplace
- religion
- media
Examples of secondary socialization:
Schooling & Education:
- Learning discipline, cooperation, competition, and cultural knowledge.
Peers & Friend Groups:
- Developing social skills, adopting slang, and conforming to group norms.
Workplace Socialization
– Learning professional norms, teamwork, and organizational culture.
Media & Technology:
– Adopting cultural trends, political views, and societal
expectations.
Religious Institutions:
– Understanding moral values, community roles, and traditions.
Clubs & Organizations:
– Learning teamwork, leadership, and responsibility in structured groups.
Government & Legal System:
– Understanding laws, rights, and civic responsibilities.
Attachment as a biological system
A biobehavioral system that:
- Promotes proximity (for survival) and exploration (for learning and, eventually, reproduction).
- Is shaped by daily interactions with primary caregivers that support or challenge cognitive and emotional security.
Also:
- Early attachment experiences form the basis for how we relate to others and see relationships.
- Attachment behavior includes “feeling safe to explore”…a ”secure base.”
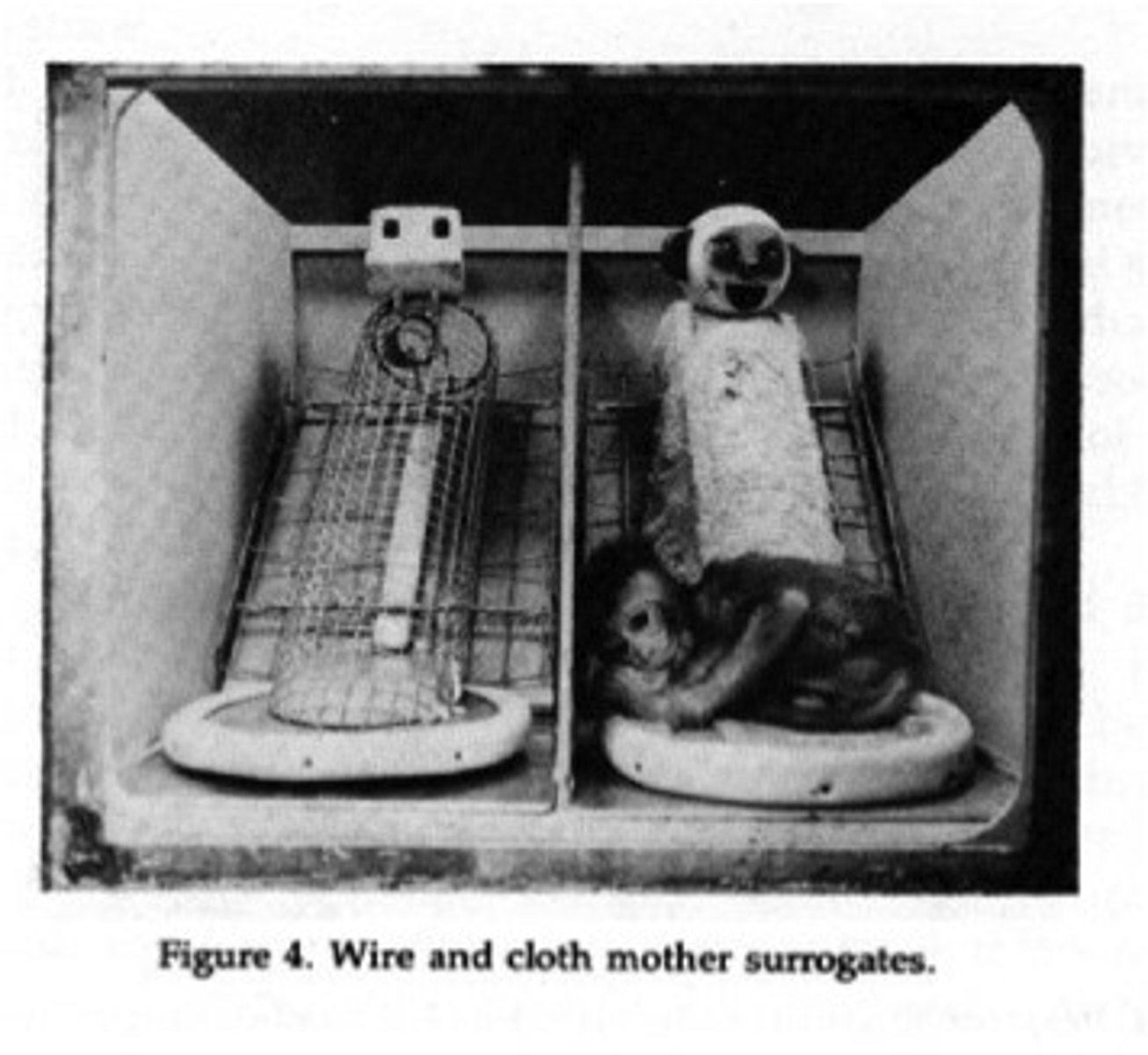
Harry Harlow's attachment research
- developmental psychologist Harry Harlow studied infant attachment using monkeys
- used wire frame and cloth-covered "mothers" to study the impact of nurturing touch, warmth, and food on infant monkey attachment
- demonstrated that attachment was based more on contact comfort (felt security; social contact) than hunger needs
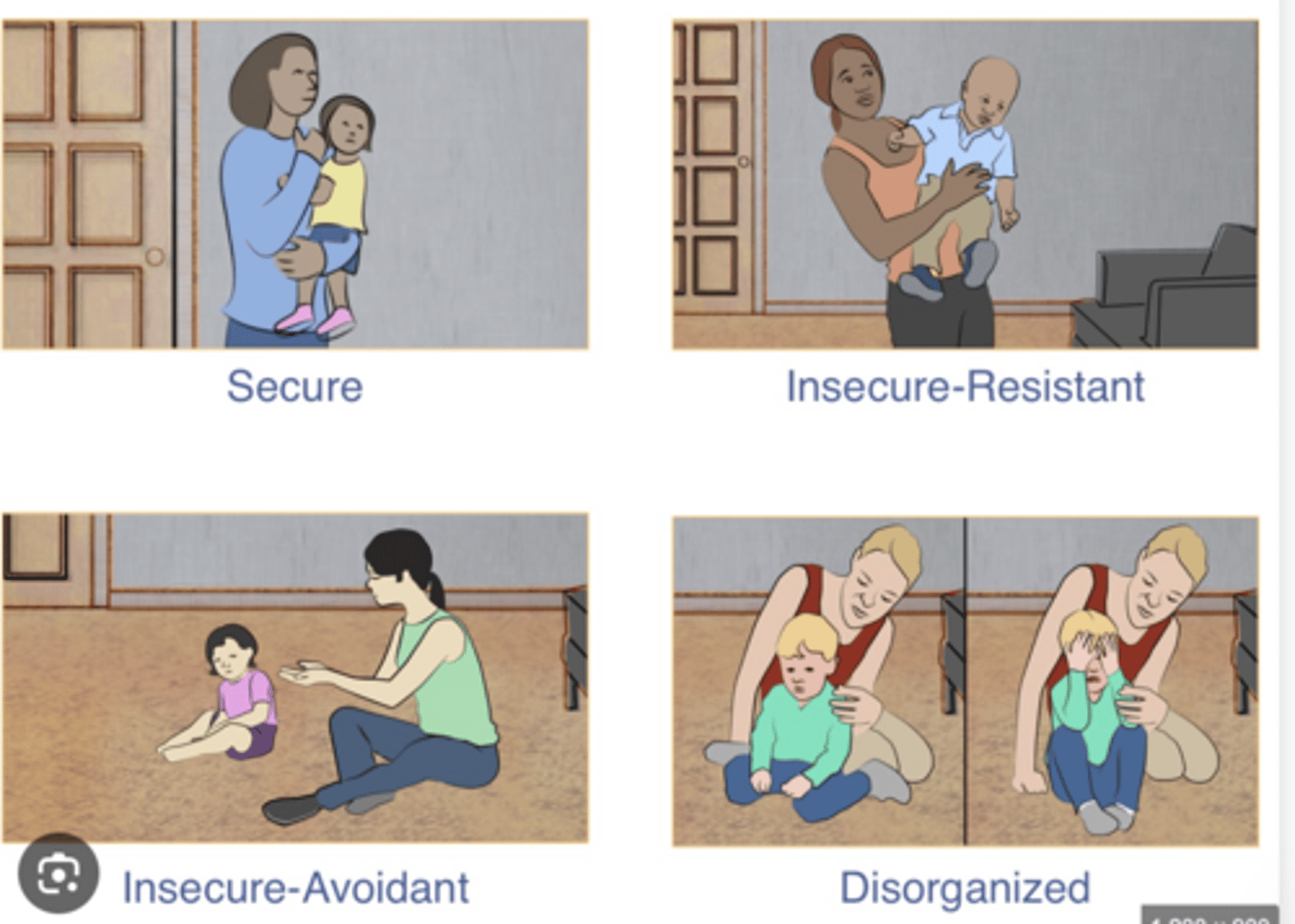
Attachment classifications as produced by Ainsworth's Strange Situation Procedure (SSP)
Place the infant in a “strange” place; activate separation distress by having the caregiver leave the room:
1. Secure (B):
- Parental sensitivity
2. Insecure (A&C):
- Parental insensitivity
1. Rejection of physical closeness, emotionally unavailable → avoidant (A babies / insecure-avoidant)
2. Inconsistent sensitivity ⇢ ambivalent/resistant (C babies / insecure-resistant)
3. Disorganized (D):
- Caregiver source of threat/fear
- Infant cannot maintain a coherent strategy → breakdown or lack of strategy → bizarre, contradictory behaviors (approach-withdrawal).
- Freezing, dazed, signs of fear, confusion, odd behaviors, rocking, head banging, etc.
What can the SSP supposedly tell us about a child's early relationships?
Classifications represent a coherent strategy the child has learned to use to get their security needs met, which are based on the historical patterns of interaction with their caregiver
Individuals’ attachment style tends to be stable across time:
– Secure children likely = secure adults (Odds Ratio 3.6)
– Insecure children are likely = insecure adults (O.R. 2.2)
– Disorganized children are likely = “unresolved” (O.R. 4.0)
Continuity of attachment (SECURE)
SECURE:
- Childhood: distress when mom leaves; greets when she returns.
- Adulthood: comfortable in relationships; seeks support from partner.

Continuity of attachment (INSECURE A)
INSECURE (A):
- Childhood: does not seek mom when she returns; focuses on envrionment.
- Adulthood: greater sense of autonomy; cut themselves off emotionally from partner.

Continuity of attachment (INSECURE C)
INSECURE (C):
- Childhood: very upset when mom leaves; explores very little.
- Adulthood: fears rejection from partner; strong desire to maintain closeness.

Continuity of attachment (DISORGANIZED)
DISORGANIZED:
- Childhood: breakdown of strategies to get comfort.
- Adulthood: relationships are a source of concern/fear.

Working models of relationships **optional
Early attachment experiences form the basis for how we relate to others and see relationships.
The paradox of aging **optional
Positive mental health among older adults who would normally be considered vulnerable.
Describe the timing and nature of what psychological characteristics decline with age **optional
- Declines in fluid intelligence
- Stability or improvement in crystallized intelligence
Socioemotional Selectivity Theory **optional
As people grow older, they view time as limited and shift their focus to meaningful events, experiences, and goals (often ignore negative info.).
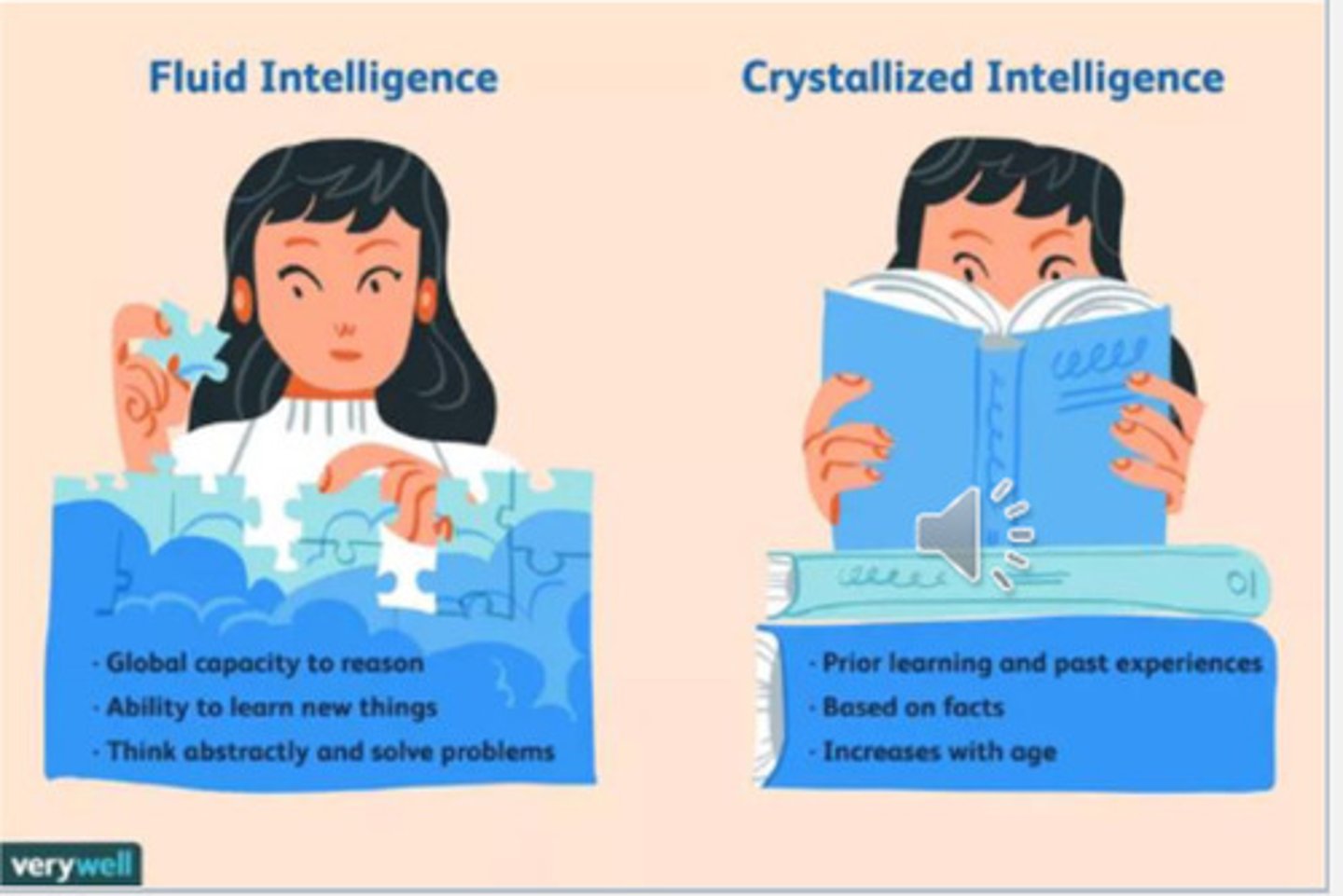
Crystallized vs. Fluid intelligence
Crystallized: specific knowledge of facts and information
- EX: using your existing knowledge of formulas and symbols to solve a math problem.
- increases as you age and gain more life experience; slows in adulthood, but can either stabilize or continue to increase.
Fluid: ability to think in terms of abstract concepts and symbolic relationships
- EX: thinking of a strategy to solve a complicated math problem.
- increases until adolescence, then gradually declines
Psychopathology
Psychological and behavioral dysfunction that occurs because of mental illness or social disorganization.
Nearly all forms of psychopathology have no definitive diagnostic test.
How many adults will have a diagnosable mental illness in their lifetime?
1 in 2 adults
Average age of onset across all disorders: ~ 24.4 years
MODELS OF PSYCHOPATHOLOGY
Two Primary Models:
1. Dimensional/Continuum Model:
- In psychology, psychopathology is conceptualized on a continuum, from fewer to more symptoms.
2. Disease/Disorder Model:
- Most commonly used within psychiatry, where pathology refers to disease processes or a disorder, present or not. This is a medicalized model of psychopathology.
HOW DO WE DETERMINE WHEN SOMETHING IS PSYCHOPATHOLOGY?
• Personal suffering: subjective distress
• Social Norms: violates normal standards of conduct
• Impairment/disability: harmful dysfunction
• Statistical approach: abnormal if rare
• Diagnosable: behavior conforms to specified patterns suggestive of deviance, distress, dysfunction, and/or danger
Medical model of psychopathology
- Most current diagnostic system
- Assumes we can distinguish normal from abnormal
- Views mental disorders as illnesses or diseases with biological causes (genetic, neurological, or chemical).
- Emphasizes diagnosis via frameworks like the DSM-5, standardized treatment, and potential cures
- Can overlook environmental, social, or psychological factors
DSM-5 Clusters
1. Odd/eccentric
- Paranoid
- Schizoid
- Schizotypical
2. Dramatic/erratic
- Borderline
- Narcissistic
- Histrionic
3. Anxious/fearful
- Avoidant
- Dependent
- OPPD
- OCPD
DSM Strengths/Weaknesses
STRENGTHS:
▪ Common language for the identification and treatment of mental health problems
▪ Can improve differential diagnosis
▪ Improve treatment development and selection
WEAKNESSES:
▪ Often does not fit real-world patients
▪ Comorbidity is common, but DSM treats different disorders that often co-occur as distinct
▪ Many terms in DSM are based on subjective judgments
▪ Culturally insensitive
▪ A particularly challenging system with developing children
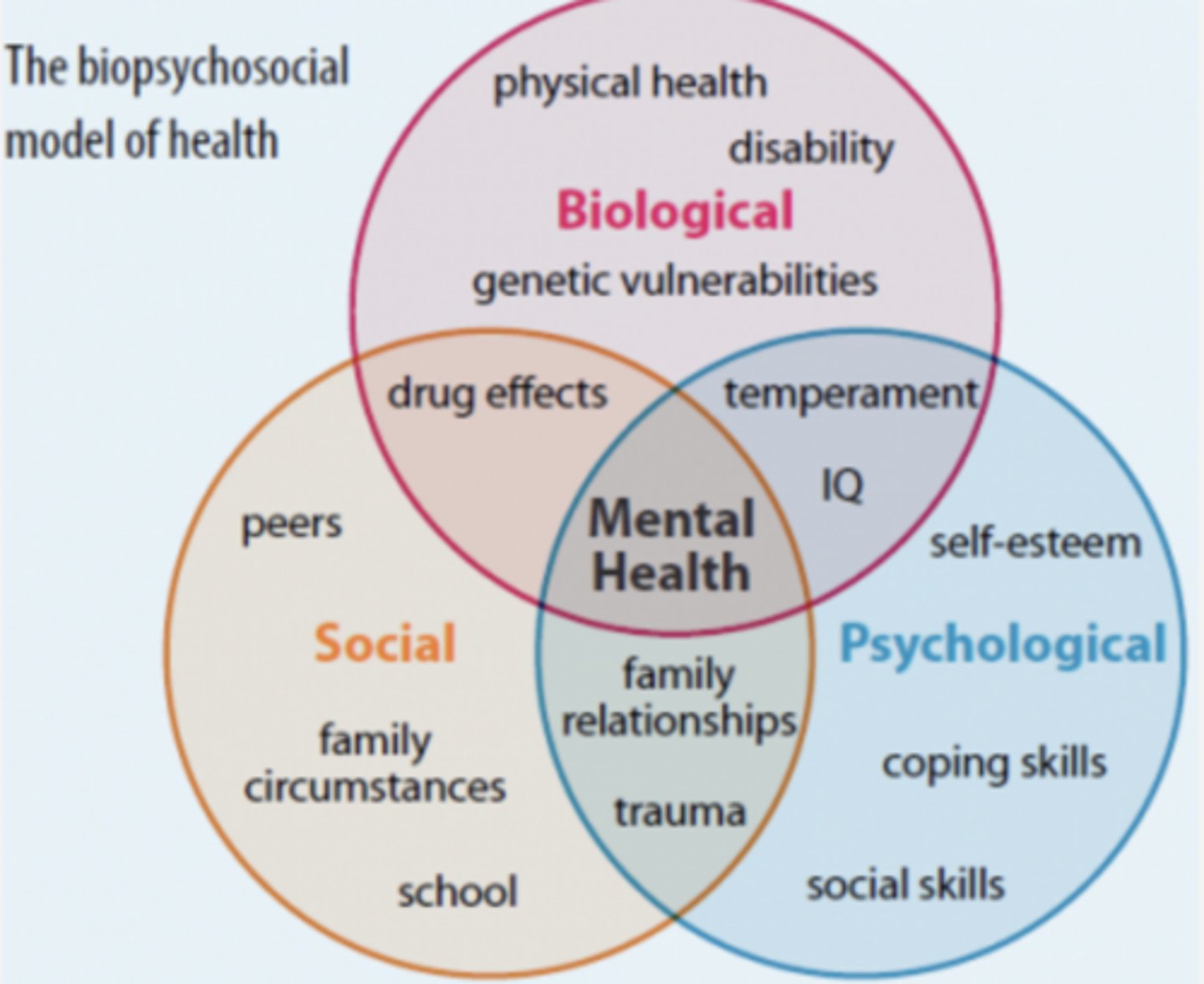
Psychological model of psychopathology
Provides theoretical frameworks for understanding the origin, development, and maintenance of mental disorders; The biopsychosocial model most widely accepted approach.
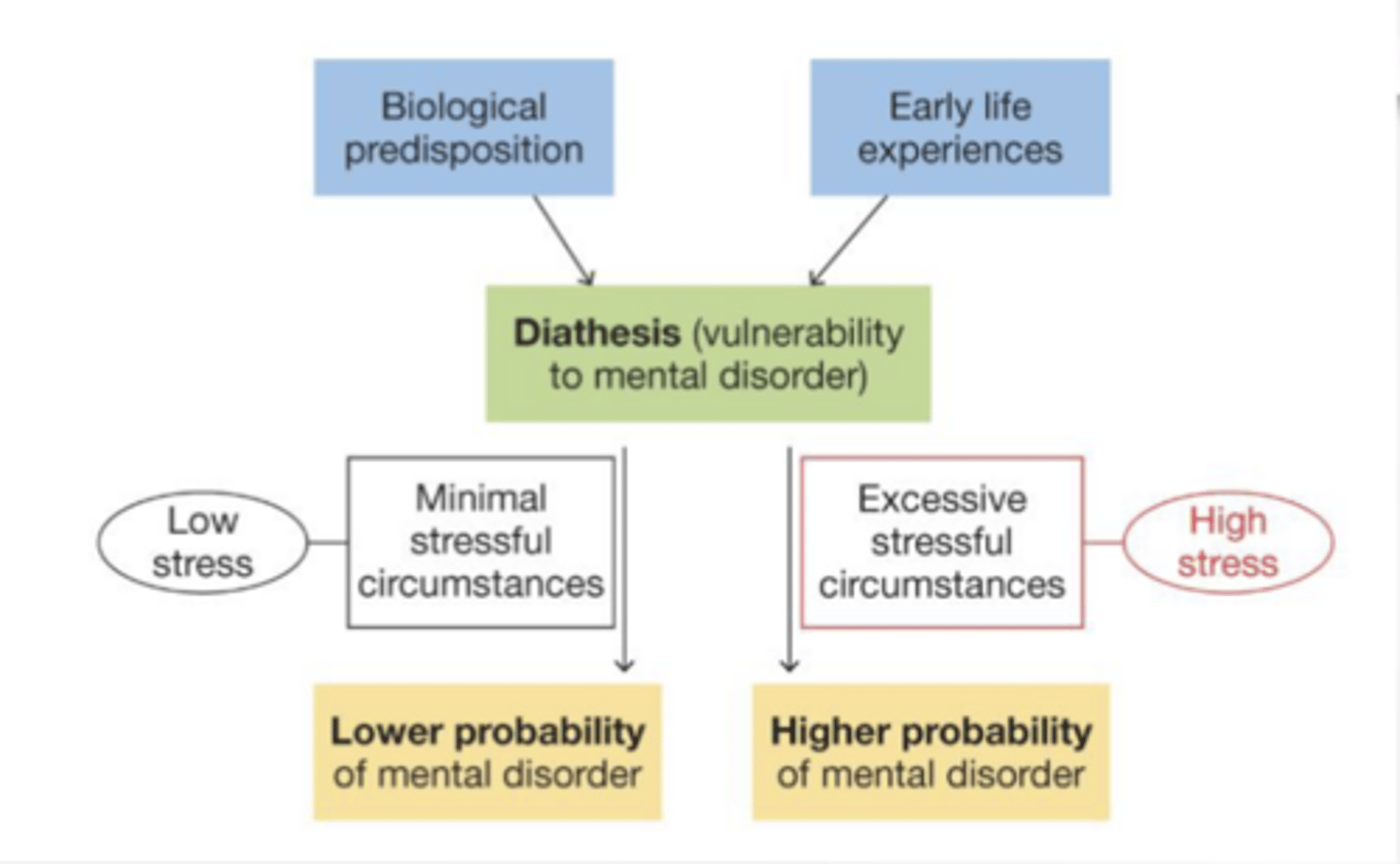
Diathesis-stress theory of psychopathology
- Combines biology & environment to explain causal processes
- Biological predispositions interact with early experience to create vulnerabilities (aka “Diathesis”) to psychopathology
- When in contact with stress→ increased odds of psychopathology
- Diathesis can include: Genotype; Neurochemistry;
Physiology/temperament; Cognitive styles; Personality dimensions; Emotion/emotion-regulation style; Harmful relations; Harmful contexts; Etc.
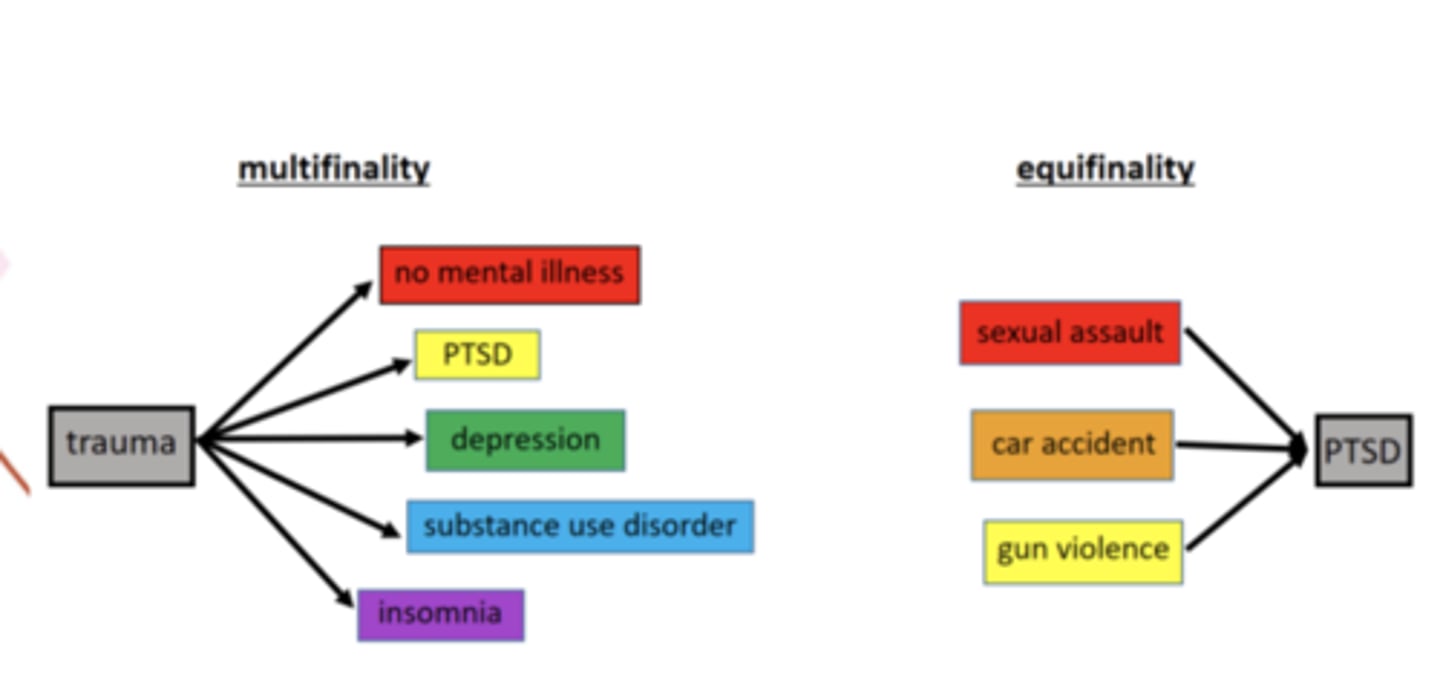
Multifinality vs. Equifinality
Multifinality - various outcomes may stem from similar beginnings
Equifinality - similar outcomes may follow from different early experiences
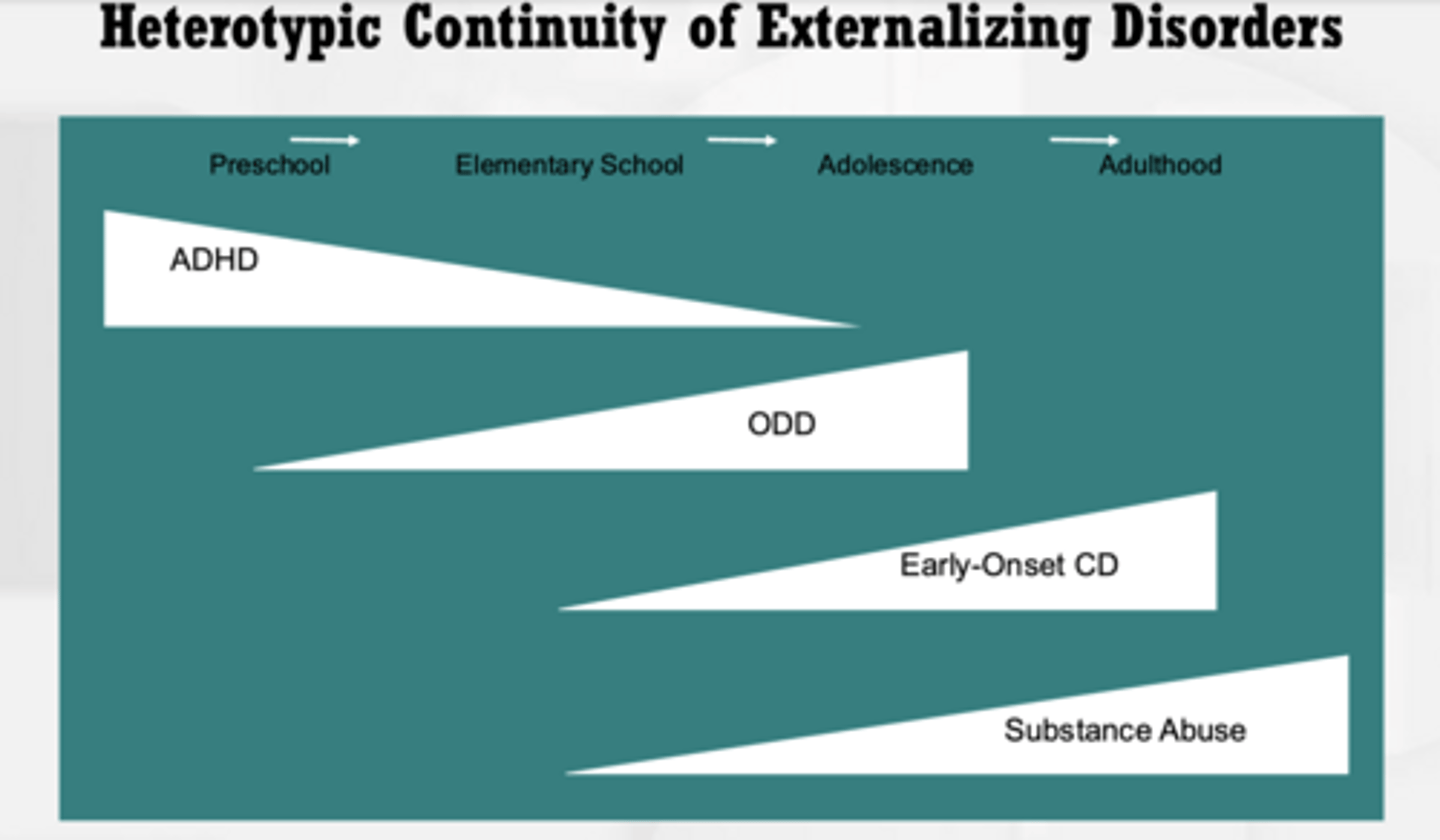
Heterotypic continuity
An earlier disorder gives way to and/or makes other disorders more likely (Ex. ADHD).
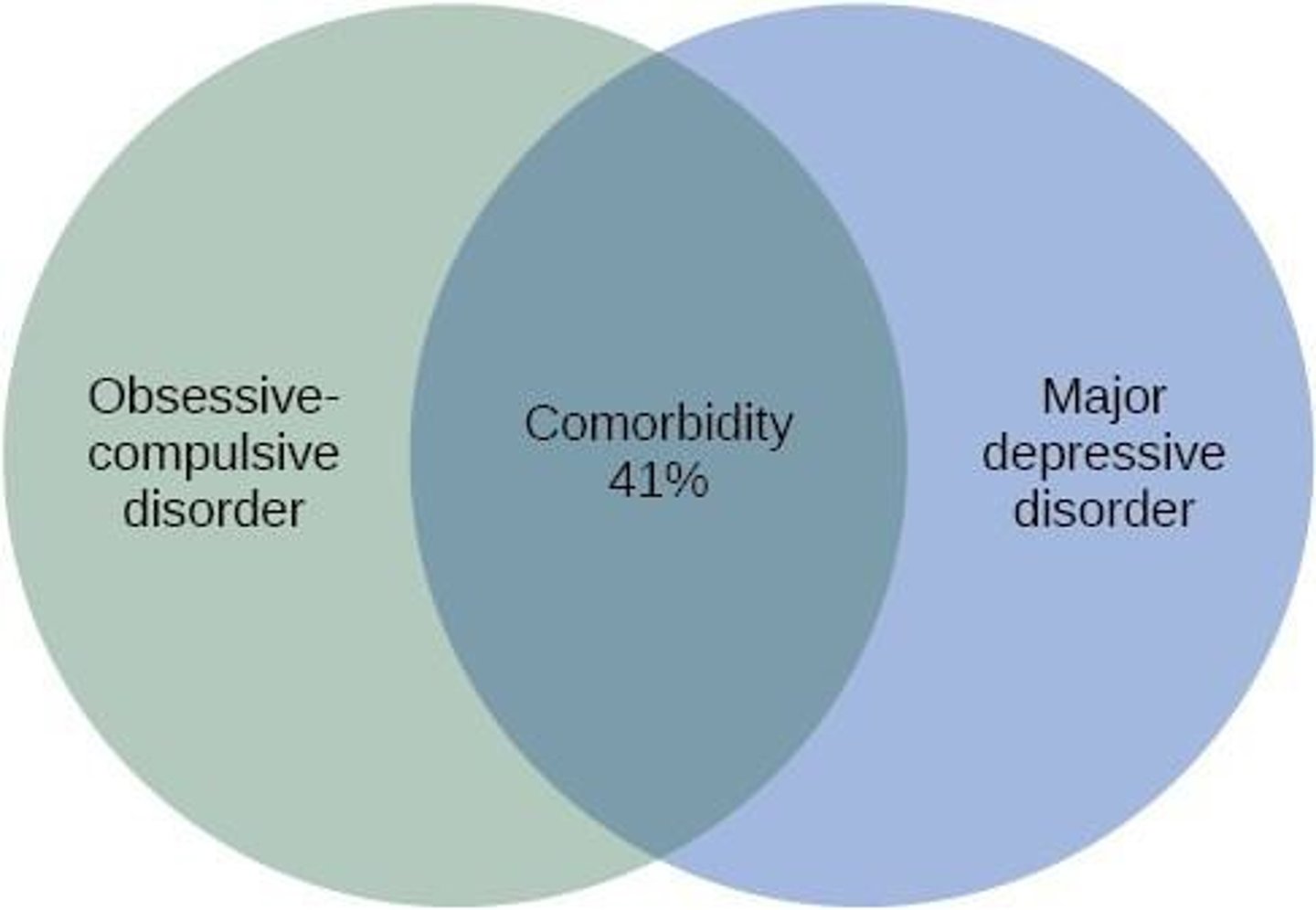
Co-morbidity
The simultaneous presence of two chronic diseases or conditions in a patient.
Epidemiology vs Etiology
Etiology: deals with individual mechanisms.
Epidemiology: deals with population-level patterns.
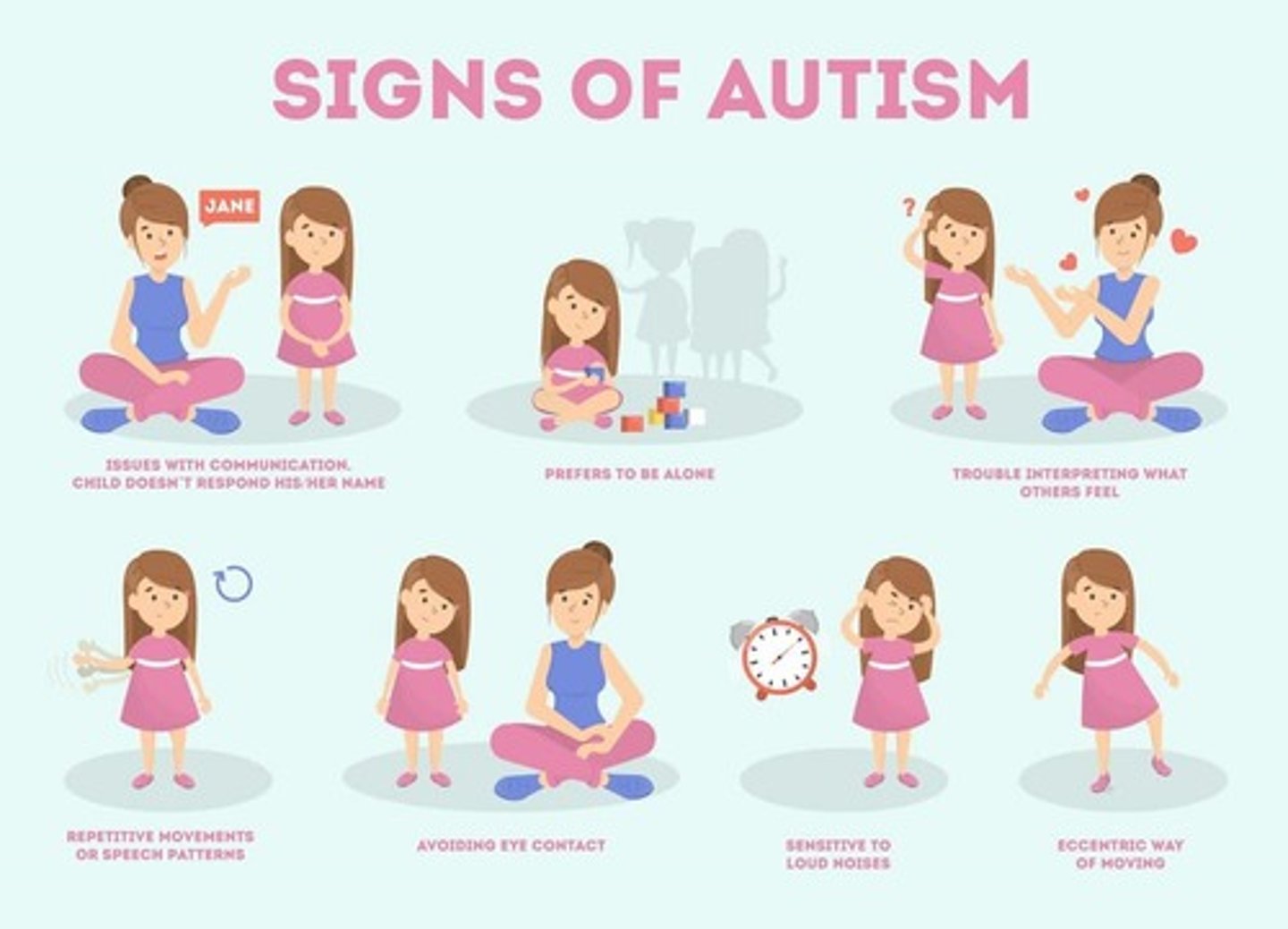
Autism Spectrum Disorder
(neurodev. disorder)
Symptomatology:
Social Communication and Interaction Deficits:
~ Reduced Social Reciprocity
~ Nonverbal Communication Challenges:
~ Relationship Challenges
Restrictive, repetitive behaviors and/or interests:
~ Stereotyped Movements or Speech
~ Inflexible Adherence to Routines
~ Highly Restricted Interests
~ Sensory Processing Differences
Epidemiology:
~ Occurs in boys vs. girls at a rate close to 4.5:1; however, more severe in girls.
Risk factors/likely causes (etiology):
~ ASD is fundamentally a condition of early brain dev.
~ Biological - Genetics
Risk modifiers, not sole causes:
~ Maternal health factors
~ Pregnancy and birth complications
Ongoing research for possible environmental causes:
~ air pollution
~ heavy metals
~ endocrine-disrupting chemicals
ADHD PRESENTATION TYPES
1. Predominantly Inattentive Presentation (ADHD-I): If inattention symptoms are met, but not hyperactivity-impulsivity.
2. Predominantly Hyperactive-Impulsive Presentation (ADHD-HI): If hyperactivity- impulsivity symptoms are met but not inattention.
3. Combined Presentation (ADHD-C): If both inattention and hyperactivity-impulsivity criteria are met.
- ADHD-C is most common in children (50-70%)
- ADHD-I is most common in adults (and girls)
ADHD maintaining factors:
Psychosocial Factors (Secondary Factors) can influence the nature and course of ADHD:
~ Viewed negatively by others
~ Constant negative feedback
~ Peer rejection = isolation
~ Low self-esteem

ADHD (JUST ETIOLOGY)
Risk factors/likely causes (etiology):
Brain regions implicated:
~ Failure of activation of critical attention/control circuits.
~ Inactivity of the frontal cortex
Genetic risk factors:
~ .7 (70%) heritability
Brain Neurochemistry:
~ Dopamine transporter and receptor genes
~ Serotonin
Environmental risk factors:
~ Undetermined: inadequate schooling, family stress, fast-
paced society.
~ Prenatal teratogens (Alcohol, Pesticides, Lead)
ADHD (JUST SYMPTOMOLOGY + EPIDEMIOLOGY)
(neurodev. disorder)
Symptomatology:
~ Inattention
~ Hyperactivity and Impulsivity
Epidemiology:
~ Most common dx of childhood
~ Boys outnumber girls 4 to 1
~ Greatest in the United States
~ SIGNIFICANT COMORBIDITY: (Over 75% of children w/ ADHD Dx have 1 or more comorbidities)
Eating disorders (JUST SYMPTOMATOLOGY + EPIDEMIOLOGY) (check)
(neurodev. disorder)
Symptomatology:
~ Anorexia Nervosa (starving)
~ Bulimia Nervosa (binging+purging)
~ Binge Eating Disorder
~ ARFID (lack of interest in foods)
~ Pica (consuming non-foods)
~ OSFED (distress due to feeding, but don't meet other criteria).
Epidemiology:
~ 1-2% of women AN.
~ 2-5% of women BN.
~ 2-6% of women BED.
~ 4-14% of women OSFED.
=
~ 0.2% of men AN.
~ 1-2% of men BED.
~ 3-5% of men OSFED
=
ED's (JUST ETIOLOGY)
Risk factors/likely causes (etiology):
Family history of EDs
Biological basis of eating disorders:
~ serotonin and dopamine; reward functioning in AN; elevated activation of self-control circuitry in AN and BN.
Sociocultural risk factors:
~ Appearance ideals
Emotion regulation problems:
Depression (JUST ETIOLOGY)
Risk factors/likely causes (etiology):
Biological theories:
~ hormones; neurotr.
Psychological theories:
~ Rumination vs. distraction; body image; interpersonal orientation.
Environmental/social :
~ gender roles; more stress; childhood trauma/abuse.
Cognitive:
~ Negative triad/view of world
(self, situations, future)
~ Attributional style
Situational:
▪ Stressors
▪ Social isolation
Genetics:
~ Moderate heritability
(.20-.40).
Depression (JUST SYMPTOMATOLOGY + EPIDEMIOLOGY)
(mood dis.)
Symptomatology:
M.D.
~ Severe negative moods
~ Lack of interest
~ Sleeping/eating disturbances
~ Loss of energy
~ Feelings of hopelessness
P.D.
~ Less intense
~ Longer lasting
Epidemiology:
~ Twice as many women suffer.
Cross-cultural differences:
~ Manifest depression with physical complaints:
▪ EX. China: Neurasthenia
▪ EX. Disorder of the spirit
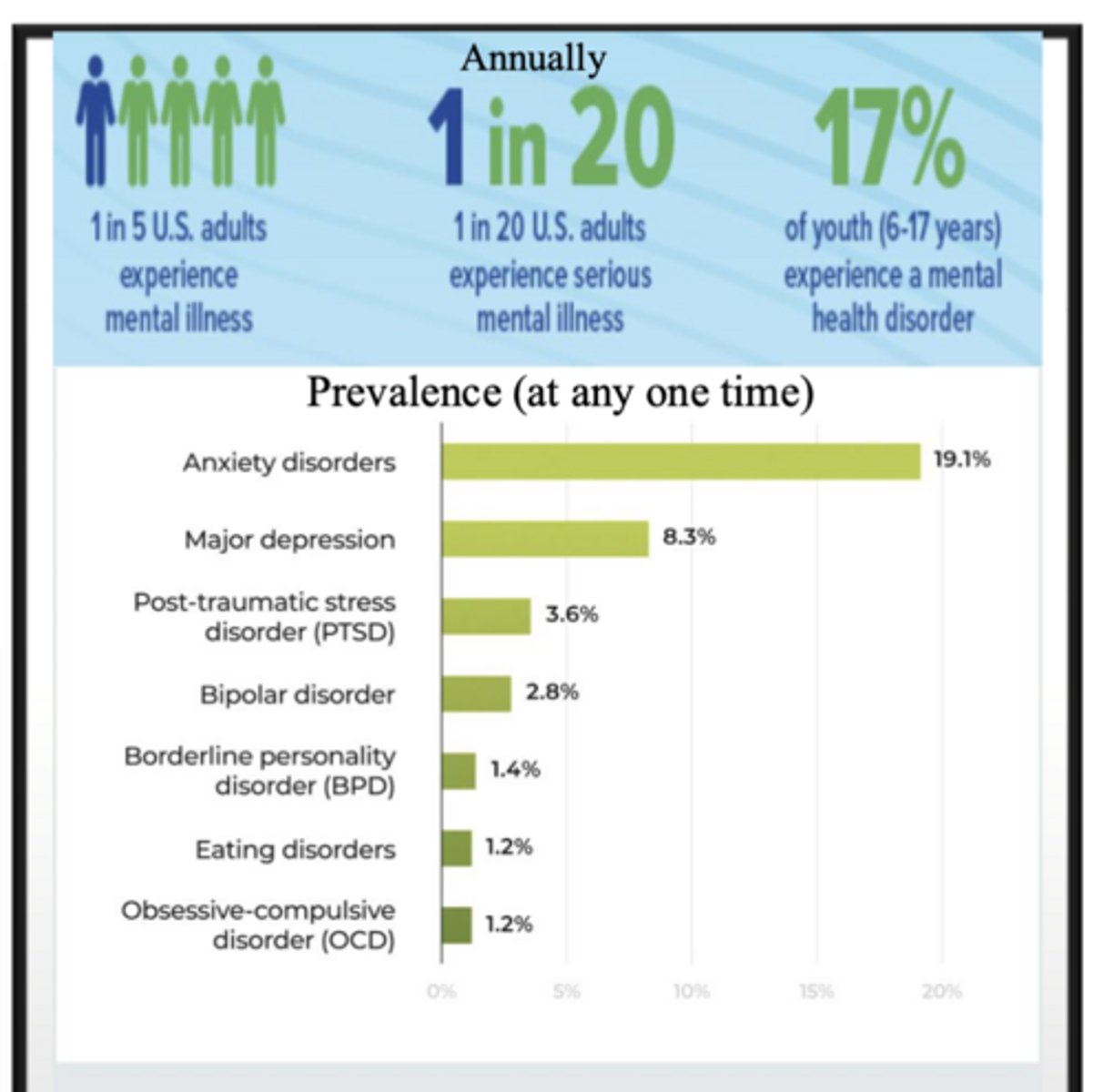
Anxiety (JUST SYMPTOMATOLOGY + EDPIDEMIOLOGY)
(anxiety dis.)
Symptomatology:
~ Characterized by intense and pervasive anxiety or fear in the absence of verifiable or immediate danger.
~ ALL include overactive threat detection + reduced regulation + reinforcement of fear state through avoidance.
Epidemiology:
~ Most people (approx. 62%) with one anxiety disorder also have another anxiety disorder.
~ see the "types" slides.
Anxiety (JUST ETIOLOGY)
Risk factors/likely causes (etiology):
Genetic:
~ Heritability: 30–50% depending on the specific disorder.
~ Polygenetic and operating through temperamental traits of neuroticism and behavioral inhibition
Neurobiological:
~ Amygdala hyperactivity
~ Conditioning (through experience)
~ Under-production of GABA neurotransmitter
~ Decreases neuron excitability
Cognitive:
~ Attentional bias toward threat
~ Perceive situations as more threatening
Environmental/Social:
~ Childhood adversity
~ Chronic stress
~ Peer/social threat
MAJOR Anxiety types + symptoms
▪ Generalized Anxiety Disorder:
~ Excessive anxiety and worry, difficulty in controlling the worry
~ Restlessness
~ Easily fatigued
~ Difficulty concentrating
~ Irritability
~ Muscle tension
~ Sleep disturbance
~ hypervigilance
▪ Obsessive-Compulsive Disorder:
~ Obsessions
~ Compulsions
▪ Panic Disorder
▪ Post Traumatic Stress Disorder:
~ Re-experiencing of the traumatic event
~ Emotional numbing and detachment
~ Hypervigilance and chronic arousal
~ Avoidance
▪ Social Phobia (Social Anxiety Disorder)
▪ Specific Phobias
MAJOR Bipolar Types
▪ Bipolar 1: depression and mania
▪ Bipolar 2: hypomania (milder) and depression

Bipolar Disorder (JUST SYMPTOMATOLOGY + EPIDEMIOLOGY)
(mood dis.)
Symptomatology:
~ Alternating periods of depression and mania.
~ Manic episodes – elevated mood, increased anxiety, diminished need for sleep, grandiose ideas, racing thoughts, extreme distractibility.
Epidemiology:
~ Significantly less common than depression (4% vs. 30% lifetime prevalence).
Bipolar Disorder (JUST ETIOLOGY)
Risk factors/likely causes (etiology):
Cognitive:
~ Negative triad/view of world
(self, situations, future)
~ Attributional style
Situational:
▪ Stressors
▪ Social isolation
Genetics:
~ High heritability (>.70).
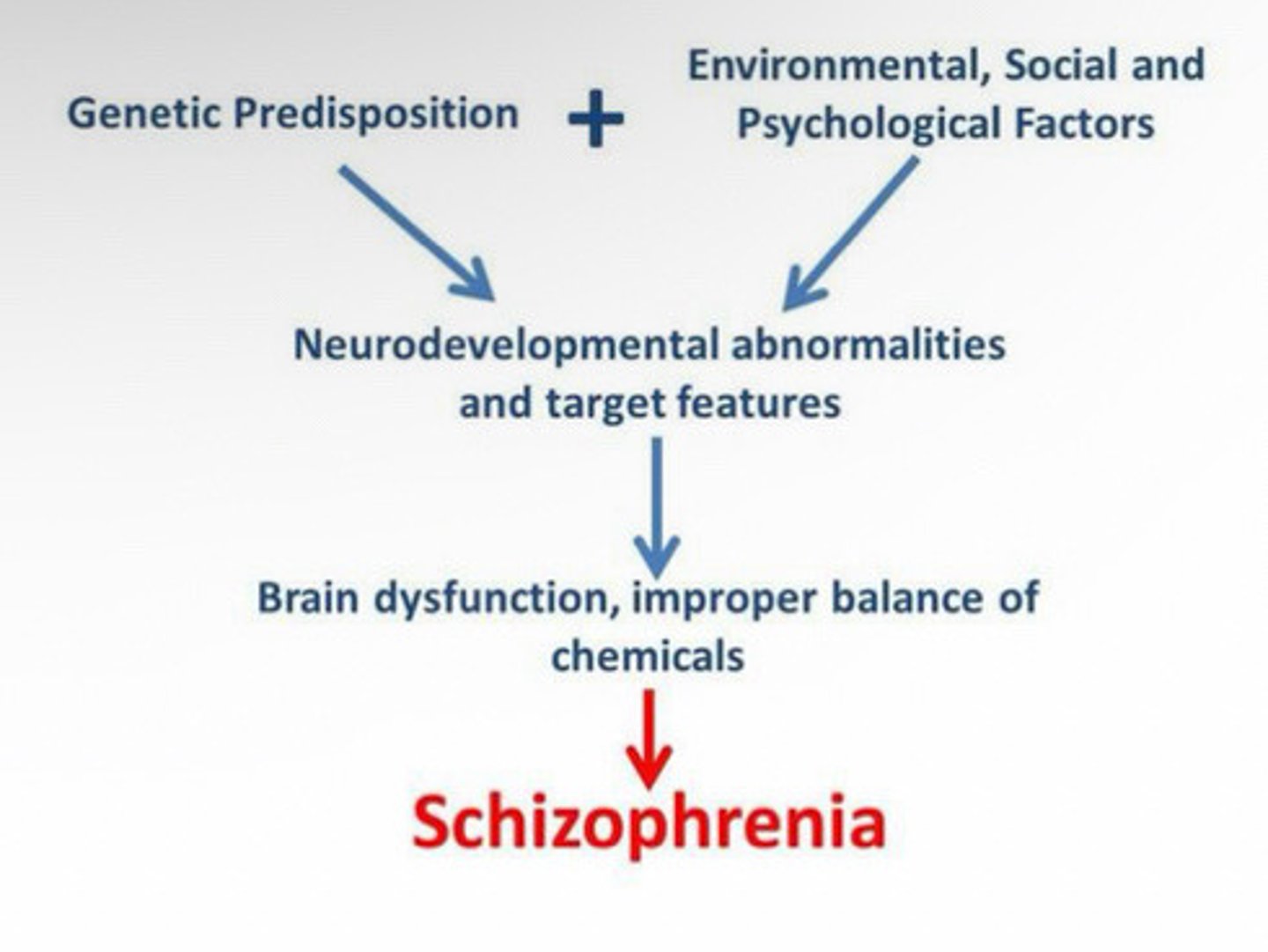
Schizophrenia (JUST ETIOLOGY)
Risk factors/likely causes (etiology):
~ A neurodevelopmental disorder largely caused by genetic vulnerabilities and environmental exposures.
Genetics:
~ Strongest single cause: Heritability 60-80%
~ Highly polygenetic: 100-1000 genetic variants, each contributing small effects.
Genes implicated in:
▪ Synaptic functioning
▪ Glutamate signaling
▪ Dopamine regulation
Neurodevelopmental Disruptions:
~ Abnormal brain development
~ Enlarged ventricles
~ Reduced gray matter
~ Altered white matter connectivity
~ Excessive or dysregulated synaptic pruning during adolescence
~ Disrupted cortical maturation
Neurochemistry:
~ Dopamine dysregulation is the most established neurochemical model
~ Both over-production and over-reception
~ Hyperdopaminergia in mesolimbic pathways
~ Hypodopaminergia in the prefrontal cortex
~ Glutamate dysfunction:
~ Excitotoxicity
Environment:
~ Maternal infection (influenza, toxoplasmosis)
▪ Severe maternal stress
▪ Obstetric complications
▪ Maternal malnutrition
~ Heavy cannabis use increases risk (especially high-THC
strains)1
~ Urban environments
~ Migration and minority status (likely via chronic social stress)
~ Childhood trauma
SCHIZOPHRENIA ETIOLOGY: why environment is important
▪ In the genetically vulnerable individual, schizophrenia
may be triggered by environmental stress, especially that
associated with urban settings:
▪ Urban environment: double the risk of schizophrenia DX
among individuals with a 1st degree relative (Torrey,
2009)
TWO THEORIES:
▪ The Intense World Theory:
~ Hyper-reactive to stimuli, leading to sensory overload, and social withdrawal as a coping mechanism.
▪ Social Drift Hypothesis:
~ Clear tendency for individuals with mental illness to drift to urban settings
Schizophrenia (JUST SYMPTOMATOLOGY + EPIDEMIOLOGY)
Symptomatology:
~ Symptoms of psychosis that profoundly alter the patient’s affect, thought, perceptions, or consciousness.
~ Psychosis: thoughts and emotions so impaired that contact is lost with external reality (“psychotic state”)
~ What the mind thinks, feels, and senses/perceives much stronger than actual reality in the moment.
~ Positive symptoms (delusions, hallucinations)
~ Negative symptoms (flat affect, slowed speech/movement)
~ Disorganization
~ Cognitive impairment
~ Mood symptoms
PRODROMAL PHASE: PERIOD BEFORE FULL PSYCHOSIS
- LASING 1-5 YEARS
- LATE TEENS TO EARLY ADULTHOOD
Epidemiology:
~ Average age of onset: 20s
~ .32 to 1.1% of population; 24 million worldwide suffer
~ 1 in 300
~ 112,000 US citizens will be Dx’d this year
Gender rates:
~ Roughly equal rates
~ Males have 1st psychotic episode earlier (late teens/early 20s) and females: 20s
~ Male schizophrenia is often more severe
~ Primarily an “adult” disorder
Iatrogenic Effects
Certain therapies have unintended consequences (e.g., drug side-effects; misdiagnosis, peer deviance training; harmful relationship with provider) called iatrogenic effects.
Biological models
◼ Reflect medical approaches to illness/disease
◼ Mental illness is a physiological malfunction
◼ Pharmacotherapy (medication) = common tx
◼ Modulate neurochemistry/brain function
Genetics, Neurochemistry, Brain Structure and Function
Cognitive models
◼ Aimed at changing patterns of thought and/or behavior.
◼ Thoughts, beliefs, information processing
◼ Dysfunctional thinking causes distress
◼ Cognitive Behavioral Therapy (CBT) = common tx
◼ Restructure schemas and cognitive distortions
Styles:
◼ Individual/Dyadic:
~Adult, Child, Couples
◼ Non-dyadic:
~ Family therapy/Group therapy
INCLUDES:
~ CBT
~ BA
~ DBT
~ ACT
~ Mindfulness & MBSR
Mindfulness & MBSR
◼ Mindfulness:
~ The practice of purposely focusing your attention on the present moment—and accepting it without judgment
◼ Mindfulness:
~ Based Stress Reduction (MBSR) therapy is used to cultivate mindfulness skills to reduce stress, alleviate suffering, and promote overall well-being.
◼ Works to weaken the effects of stressors that interact with diathesis.
◼ MBSR is a structured multi-week program that combines mindfulness meditation, body awareness, and yoga, etc.
~ ALSO, improved immune functioning!

Acceptance and Commitment Therapy (ACT)
◼ Theory:
~ Painful thoughts and emotions are inevitable.
~ Flexibility, not symptom elimination.
~ Effective for treating a wide variety of conditions that extend beyond traditional DSM clinical disorders.
◼ Core features/goals of ACT Tx:
~ Acceptance: emphasizes “willingness” to have unwanted
thoughts/feelings/experiences (“make room”).
~ Learning to see thoughts as mental events, not literal truths.
~ Being Present (mindfulness exercises).
Dialectical behavior therapy (DBT)
- Originally developed for Borderline Personality Disorder
- Focuses on 4 skill modules: Mindfulness (being present), Distress Tolerance (surviving crises), Emotion Regulation (managing feelings), and Interpersonal Effectiveness (navigating relationships).
- Promising treatment for borderline personality disorder -(involves exposing the client to stressors + helping the client regulate emotions/cope with stressors that might trigger suicidal behavior.
Behavioral Activation Tx (BA)
Mental health problems often involve:
◼ reduced activity
◼ avoidance behaviors
◼ loss of reinforcement
DBT reverses this by:
◼ increasing engagement in meaningful activities
◼ restoring environmental reward
◼ breaking avoidance cycles
Cognitive-Behavioral Therapy (CBT)
Theory:
~ Maladaptive thoughts and feelings play a fundamental role in shaping behavior, which further shapes emotion and thought.
Therapeutic objective:
~ Identify and change destructive or disturbing thought patterns that have a
negative influence on feelings and behavior
~ Activate behaviors that will directly challenge
maladaptive thoughts.
CBT is used to treat a variety of disorders, especially mood, anxiety disorders, and eating disorders!
Psychotherapy vs. Pharmacotherapy??
◼ Psychotherapies
- Regularly produce modestly stronger positive outcomes.
- yield better long-term outcomes
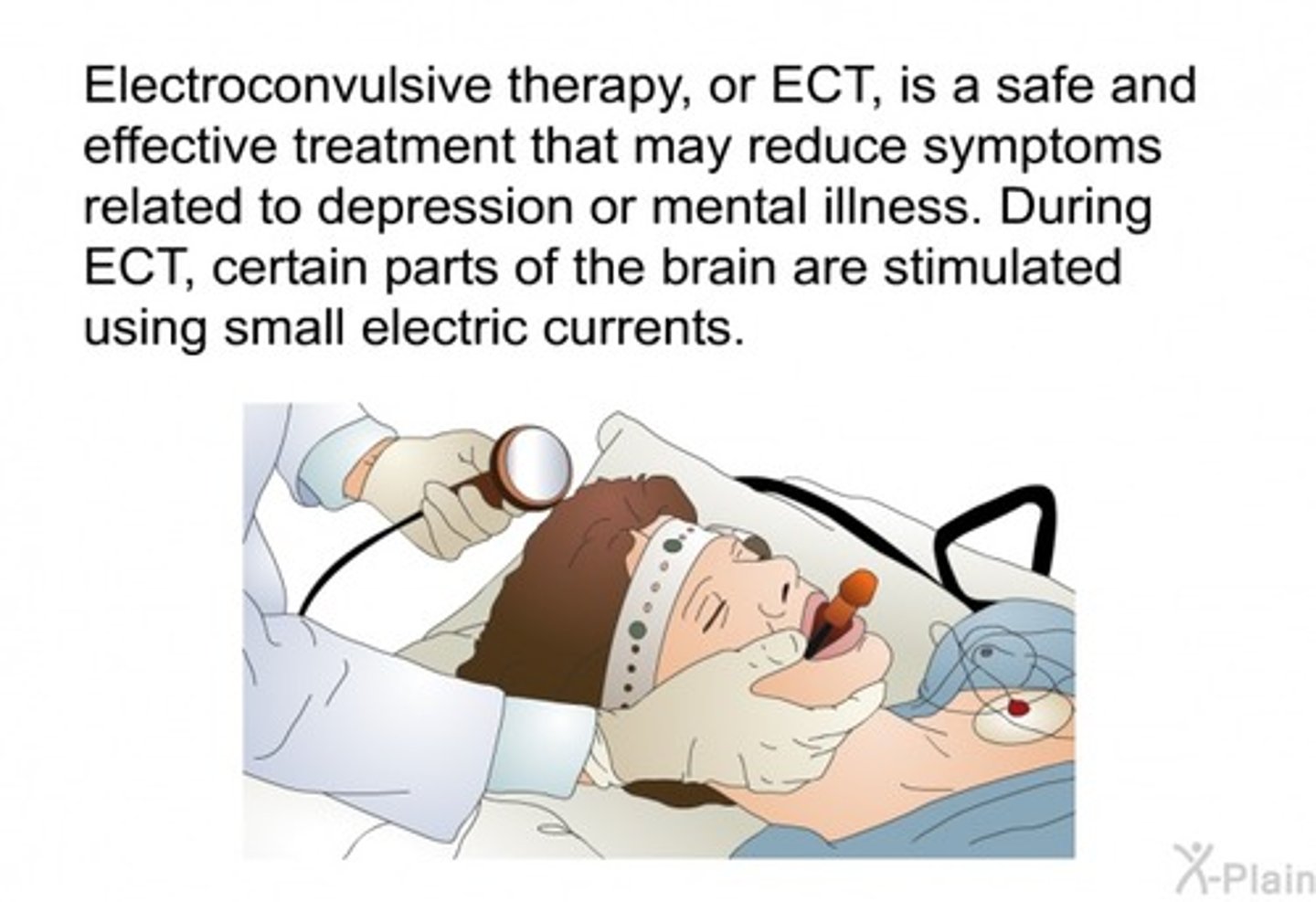
Electroconvulsive Therapy (ECT)
◼ ECT is a medical treatment most commonly used in patients with severe major depression or bipolar disorder who have not responded to other treatments.
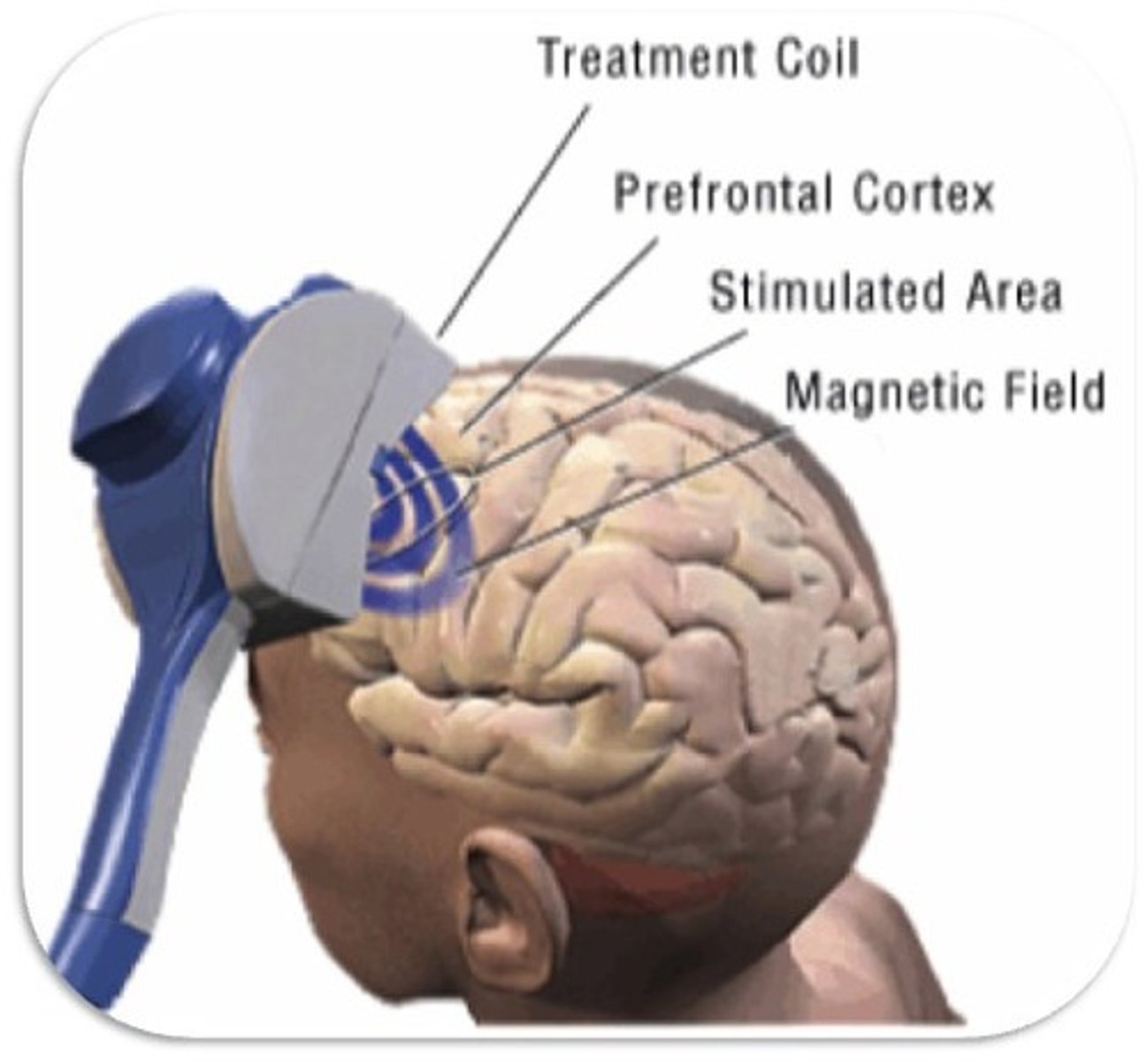
Transcranial Magnetic Stimulation
◼ Single-pulse TMS: Disruption of brain activity occurs only during the brief period of stimulation.
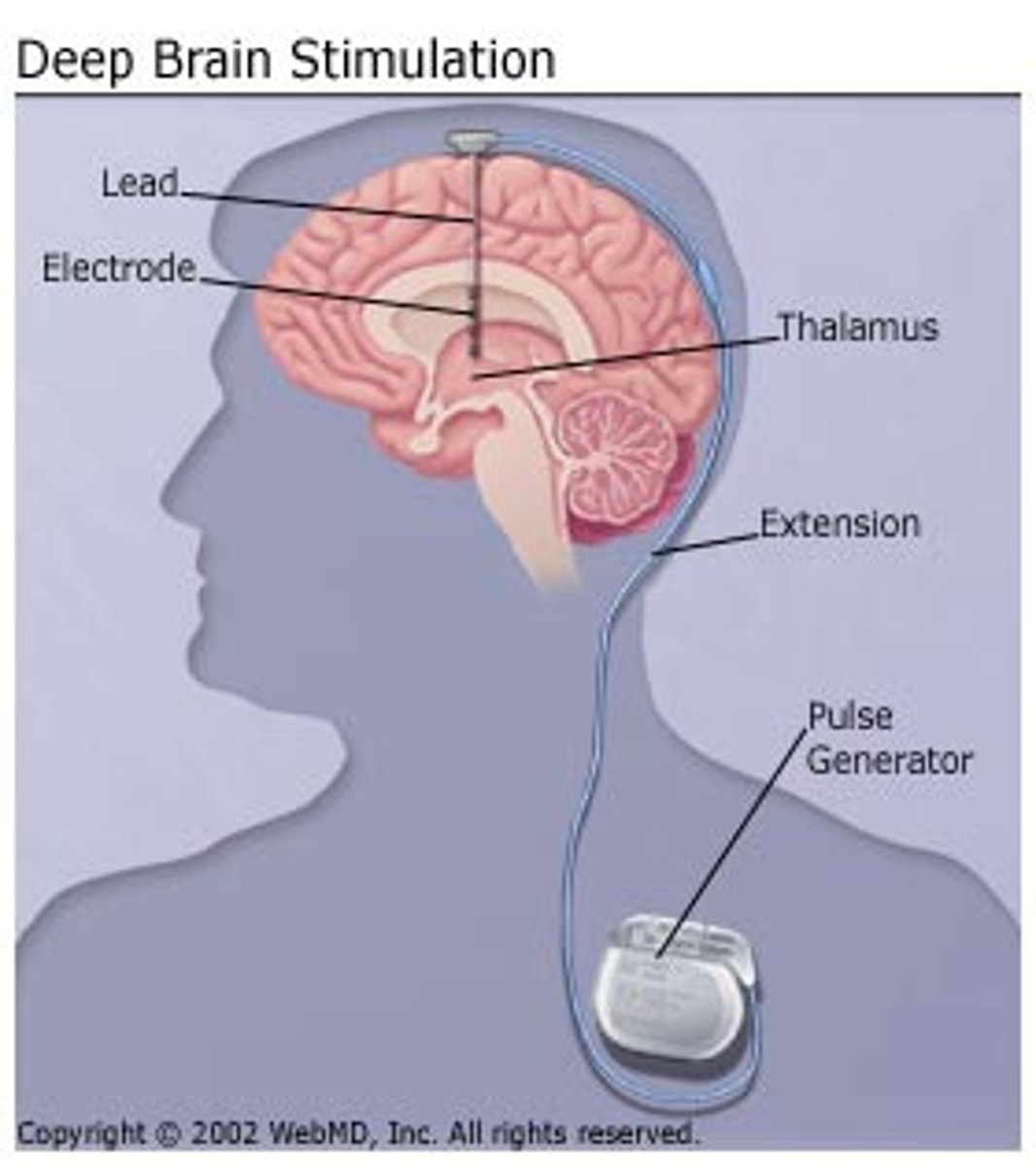
Deep Brain Stimulation (DBS)
◼ Surgical implanting of electrodes that administer electrical pulses to stimulate the brain
Environmental models (check)
Explain the development and course of psychopathology (check)
Developmental psychopathology
▪ Focuses on how maladaptive and adaptive processes unfold across development from infancy to adulthood.
▪ Central question: How do patterns of risk and resilience lead to or away from psychopathology? How do we prevent maladaptation and promote adaptation?
▪ Emphasizes timing (sensitive periods):
~ Continuity and change, and cascading effects across development; longitudinal.
Psychiatry/Clinical psychology
▪ Focus on assessment, description, diagnosis, and treatment of m. dis. when problems present at any point in the lifespan.
▪ Central question: How do we identify and treat psychological disorders in individuals?
▪ Largely present-focused:
~ Not focused on prevention, but focused on relapse prevention.
Relationship between Psychiatry/Clinical psychology & Developmental psychopathology:
Psychiatry/Clinical psychology provides:
▪ Diagnostic frameworks
▪ Treatment outcome data
▪ Clinical populations that shape developmental theory
Developmental psychopathology informs clinical psychology by identifying:
▪ Early markers of risk (e.g., childhood adversity; poverty)
▪ Sensitive developmental periods
▪ Mechanisms underlying the disorder
▪ Targets for prevention and early intervention
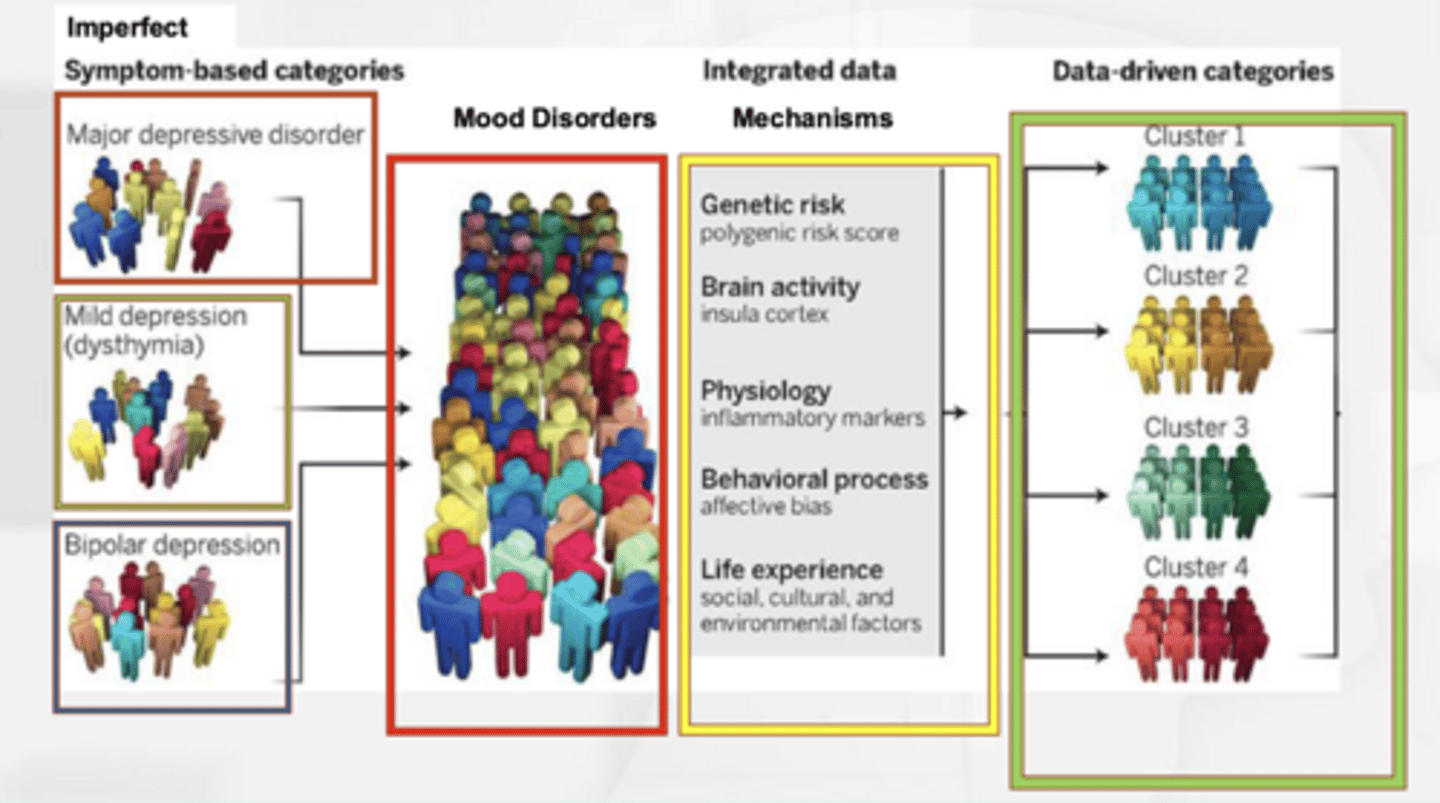
RDOC system and search for and use of "mechanisms."
Attempts to move away from the categorical psychopathology of DSM in favor of a dimensional approach based on research.
Looks at basic domains of human functioning at multiple levels of analysis to identify mechanisms that give rise to
disordered thoughts, emotions, and behaviors.
"Underlying all forms of psychopathology are 'problems' aka the 'domains' we should be studying - let's create a diagnostic system to understand all these things and not just symptoms."
Evidence-Based Treatments (EBTs)
Evidence-Based Treatment: Clearly specified treatments shown to be effective in controlled research with specific populations
What are the various levels of EBTs
1. Experimental Treatments
~ Being developed – not yet fully tested
2. Possibly Efficacious
~ Just one study, but no conflicting evidence
3. Probably Efficacious
~Same as Well-Established, but with “semi” control group
4. Well-Established:
➢ Two or more independent randomized control trials (RCTs)
➢ Treatment manual
➢ Clearly defined population
➢ Reliable and valid outcome measures
Gold Standard Treatments and how are they used to evaluate treatments?
Randomized Clinical Trials (RCT)
- (particularly the double-blind, placebo-controlled variety)
- By randomly assigning participants to treatment or control groups, researchers eliminate bias and confounding variables, allowing them to isolate the treatment's direct effect.
Medication Essential
Schizophrenia
Bipolar disorder
ADHD
Medication Helpful
Depression
Anxiety disorders
OCD
Medication Secondary
Personality disorders
Insomnia
PTSD (after therapy)
Stigma: what it is; how it affects treatment; theories of what contributes to mental health stigma
Today, it is one of the leading causes of delayed treatment seeking (8-10 years).
- Ableism
- Social Identity Theory
- Labeling Theory
- Structural Stigma Theory
- Evolutionary Psychology Theory